Subscribe to RSS
DOI: 10.1055/s-0038-1633484
Contralateral Transmaxillary Corridor: Surgical Planning and Pathway Analytics
Publication History
Publication Date:
02 February 2018 (online)
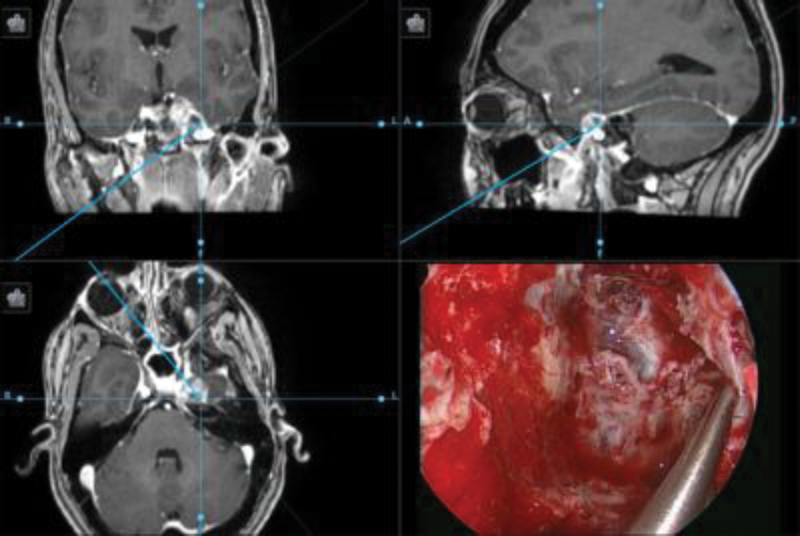
Background The contralateral transmaxillary (CTM) corridor was recently reported as a contralateral endoscopic approach to the petrous apex (see Fig. 1). This pathway was designed to improve access to lesions of the petrous apex that are lateral to the paraclival internal carotid artery (ICA) that would otherwise require lateralization of the paraclival ICA or a transpterygoid infrapetrous approach. The purpose of this study was to perform detailed analytics of the CTM pathway as originally described, including geometry, volume, angle of target approach, and surface area of the pathway–target interface (instrumentation space). The described analytics would then be studied relative to actual instrument pathways that were used in the treatment of petrous apex pathology through the CTM approach to confirm clinical efficacy and safety.
Methods This was a multi-institutional study. The CTM approach was performed virtually using software developed by the Surgical Engineering Division of the BioRobotics Laboratory at the University of (X) on six preoperative craniofacial CT scans to indicate potential anatomic boundary dimensions of the dissection as described in the original paper. The same analytics were then applied to the actual pathways that were used in the surgical procedure, demonstrated on the postoperative CT scans of the same six patients operated on at the University of (Y) by the surgeons who originally described the procedure. Comparisons were then made between planned and actual pathways used including completeness of resection metrics.
Results Computer pathway analytics performed on the preoperative images demonstrated excellent pathway characteristics for lesion manipulation as described earlier (XXX). The pathway volumes were greater than the required 3 mL, with excellent approach and manipulation angles. Decreased need for manipulation of the ICA was demonstrated, as hypothesized. Comparison of the postoperative scans with the planning analytics demonstrated that all actual pathways were less than the theoretical maximal pathway volume, and that all lesions were completely resected within the planned domains.
Conclusion Computer analytics of the CTM approach demonstrate that the pathway characteristics are highly favorable for completeness of resection metrics, including favorable pathway volume, angle of approach, and room for target instrumentation. Actual instrument travel in clinical cases was within the bounds of the original anatomic description, confirming the safety of the approach. The analytics illustrated in this article confirm the safety of the approach, and will assist in understanding and planning this approach in clinical use.