
Subscribe to RSS
DOI: 10.1055/s-0034-1364950
Gastroscopic snare polypectomy for cystic duct adenoma: a rare occurrence
Publication History
Publication Date:
22 April 2014 (online)


Cystic duct adenoma is an uncommon disease. Appropriate therapeutic strategies have not been clearly defined. Surgical resection is often recommended [1] [2] [3] [4]. Recently, endoscopic procedures for biliary papillomatosis were reported, such as endoscopic papillary balloon dilation, argon plasma coagulation, photodynamic therapy, endoscopic retrograde biliary drainage, and intraluminal brachytherapy with iridium-192 [5] [6] [7] [8] [9]. However, it is difficult to achieve complete resection and the recurrence rate is high. We report on a patient diagnosed with cystic duct adenoma who presented with recurrent cholangitis and was treated with a snare polypectomy using a gastroscope.
A 61-year-old woman was admitted to our hospital with intermittent upper abdominal pain and fever. An abdominal computed tomography scan, magnetic resonance cholangiopancreatography, and endoscopic ultrasound showed a dilated intrahepatic biliary system and common biliary duct (CBD), with a hyperechoic mass floating at the upper CBD ([Fig. 1]). Endoscopic retrograde cholangiopancreatography showed a CBD diameter of 2.5 cm ([Fig. 2]) and excessive mucinous discharge from the papilla of Vater ([Fig. 3]). It is interesting that the duodenoscope could access the CBD easily via the papilla. Subsequent examination using a forward-viewing gastroscope (GIF-H260; Olympus, Tokyo, Japan) demonstrated a 2-cm adenomatous lesion in the cystic duct and protruding into the CBD ([Fig. 4]). Histological examination revealed biliary tubulovillous adenoma with moderate-grade dysplasia.



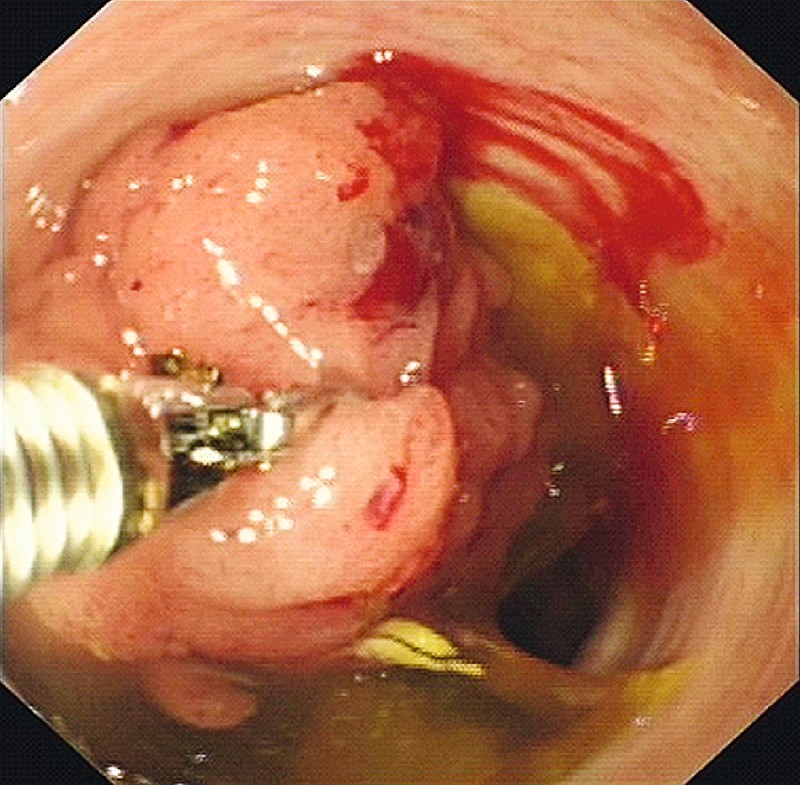
The case was discussed by the multidisciplinary team who decided that surgical removal should be performed due to the potential for malignancy. However, the patient refused surgery and requested noninvasive endoscopic treatment. Therefore, endoscopic polypectomy was performed after written informed consent had been obtained from the patient. Piecemeal intraductal snare polypectomy was performed under gastroscopic visualization and the adenoma was completely resected without any remnant ([Fig. 5], [Video 1]).

Quality:
After the procedure, the patient experienced no further abdominal pain or fever. During the 3-month follow-up period, the patient was asymptomatic with normal liver function test findings and no recurrent cholangitis.
Endoscopy_UCTN_Code_CCL_1AZ_2AC
* These authors contributed equally to this article.
-
References
- 1 Ariche A, Shelef I, Hilzenrat N et al. Villous adenoma of the common bile duct transforming into a cholangiocarcinoma. Isr Med Assoc J 2002; 4: 1149-1150
- 2 Kosemehmetoglu K, Akpinar E, Sokmensuer C et al. Papillary carcinoma with diffuse papillomatosis of gallbladder and cystic duct. Ann Diagn Pathol 2011; 15: 140-144
- 3 Jazrawi SF, Nguyen D, Barnett C et al. Novel application of intraductal argon plasma coagulation in biliary papillomatosis (with video). Gastrointest Endosc 2009; 69: 372-374
- 4 Forlano I, Fersini A, Tartaglia N et al. Biliary papillomatosis. Case report. Ann Ital Chir 2011; 82: 405-408
- 5 Tsuchida K, Yamagata M, Saifuku Y et al. Successful endoscopic procedures for intraductal papillary neoplasm of the bile duct: a case report. World J Gastroenterol 2010; 16: 909-913
- 6 Bechmann LP, Hilgard P, Frilling A et al. Successful photodynamic therapy for biliary papillomatosis: a case report. World J Gastroenterol 2008; 14: 4234-4237
- 7 Brauer BC, Fukami N, Chen YK. Direct cholangioscopy with narrow-band imaging, chromoendoscopy, and argon plasma coagulation of intraductal papillary mucinous neoplasm of the bile duct (with videos). Gastrointest Endosc 2008; 67: 574-576
- 8 Suffat LP, Fronda G, Maglione V et al. Cholangioscopic management of intrahepatic papillomatosis unsuitable for surgical treatment. Ann Ital Chir 2009; 80: 35-38
- 9 Rafiq E, Alaradi O, Bawany M et al. A combination of snare polypectomy and APC therapy for prolapsing common bile duct adenoma. J Interv Gastroenterol 2012; 2: 193-195