A 50-year-old man with oropharynx cancer (T3N0M0) underwent upper gastrointestinal
endoscopy to search for synchronous lesions. Endoscopic examination identified two
synchronous extensive flat lesions (T0-IIb) in the esophagus: lesion A – a 5-cm lesion,
occupying 75 % of the circumference, located between 16 and 21 cm from the incisors;
lesion B – a 5-cm circumferential lesion, located between 26 and 31 cm from the incisors.
The intrapapillary capillary loop classification was suggestive of type V3. Endoscopic
ultrasound revealed neither submucosal invasion nor locoregional lymphadenopathies.
Following multidisciplinary evaluation, endoscopic submucosal dissection (ESD) was
planned ([Video 1]).
Video 1 Endoscopic submucosal tunnel dissection for the treatment of synchronous esophageal
neoplasms.
On account of the distance between the lesions, separate circumferential excision
assisted by endoscopic submucosal tunnel dissection (ESTD) was performed using a FlushKnife
(Fujifilm Corp., Tokyo, Japan). Circular incisions were completed at the anal and
oral margins, and ESTD was accomplished from the oral to the anal side creating two
submucosal tunnels in the proximal lesion and three submucosal tunnels in the distal
lesion (larger esophageal lumen) ([Fig. 1]). Submucosal dissection was completed and separate en bloc resections were achieved
([Fig. 2], [Fig. 3]).
 Fig. 1 Submucosal tunnels were created covering the whole esophageal lumen.
Fig. 1 Submucosal tunnels were created covering the whole esophageal lumen.
 Fig. 2 Ulcers were reassessed without muscular injury or bleeding.
Fig. 2 Ulcers were reassessed without muscular injury or bleeding.
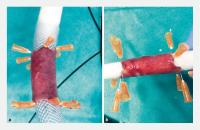 Fig. 3 Complete circumferential en bloc resection of esophageal lesions. a The distal lesion. b The proximal lesion.
Fig. 3 Complete circumferential en bloc resection of esophageal lesions. a The distal lesion. b The proximal lesion.
The procedure took 270 minutes and the patient was discharged 48 hours after the procedure
under oral prednisolone. Pathological analysis revealed a well-differentiated squamous
cell neoplasia (SCC), without lymphovascular invasion; the tumor was intramucosal
and resection was complete in lesion A but submucosal invasion with positive vertical
margins were present in lesion B. After multidisciplinary evaluation, chemoradiotherapy
for both esophageal and oropharyngeal neoplasms was performed. Three months later,
the patient refused endoscopic re-evaluation but there was no unequivocal dysphagia.
ESD is a well-established treatment for superficial esophageal SCC. However, for large
circumferential lesions, ESTD has a more rapid dissection speed and higher R0 resection
rate compared with conventional ESD [1]
[2]. Although widely performed in Asia, only a few cases have been described at Western
centers [3]
[4]. To the best of our knowledge, this is the first report of ESTD for two synchronous
circumferential SCCs in a Western center.
Endoscopy_UCTN_Code_TTT_1AO_2AG
Endoscopy E-Videos is a free access online section, reporting on interesting cases and new techniques
in gastroenterological endoscopy. All papers include a high quality video and all
contributions are freely accessible online.
This section has its own submission website at https://mc.manuscriptcentral.com/e-videos





