

Subscribe to RSS
DOI: 10.1055/a-1751-3451
Kindergastroenterologische und hepatologische Versorgung in Deutschland: Ergebnisse einer deutschlandweiten Umfrage
Paediatric gastroenterological and hepatological care in Germany: results of a nationwide surveyAuthors
Supported by: Gesellschaft für Pädiatrische Gastroenterologie und Ernährung

Zusammenfassung
Einleitung Kinder und Jugendliche mit chronischen Magen-, Darm-, Pankreas-, und Lebererkrankungen benötigen eine altersgerechte und qualifizierte Behandlung. Anhand einer repräsentativen Umfrage wird die strukturelle und personelle ambulante und stationäre Versorgung von Kindern mit chronischen Magen-, Darm-, Pankreas- und Lebererkrankungen in Deutschland analysiert.
Methodik 319 Kliniken für Kinder- und Jugendmedizin sowie 50 kindergastroenterologische Praxen in Deutschland wurden eingeladen, an der anonymen Online-Umfrage über EFS Survey teilzunehmen. Es wurden die Struktur der Einrichtungen, Weiterbildungsbefugnisse, Kooperationen, Behandlungs- bzw. Betreuungsdaten und eine Einschätzung des Versorgungsbedarfs systematisch erfasst und deskriptiv ausgewertet.
Ergebnisse An der Umfrage haben 81 Kliniken und 10 Praxen teilgenommen. Fast zwei Drittel der Kliniken (n=52) erbringen ambulante kindergastroenterologische Leistungen. Meist bis zu 10 (25,4%) oder 20 Stunden/Woche (33,8%). Ein Viertel der Kliniken bietet keine Sprechstunden an. Der ambulante Versorgungsbedarf kann von zwei Dritteln der Institutionen nicht gedeckt werden. Die Hälfte aller Kliniken gab an, dass der stationäre kindergastroenterologische Versorgungsbedarf gedeckt werden kann. Ein Drittel kann diesen jedoch nicht abdecken und nur selten gibt es ungenutzte Kapazitäten. 35 Kliniken (43,2%) verfügen über eine Weiterbildungsbefugnis gemäß Landesärztekammer (n=33) und/oder sind Weiterbildungszentrum der Gesellschaft für pädiatrische Gastroenterologie und Ernährung (GPGE) (n=18).
Schlussfolgerung Es besteht sowohl ein ambulantes als auch stationäres Versorgungsdefizit in der Kinder- und Jugendgastroenterologie. Dieses resultiert unter anderem aus den ökonomischen Rahmenbedingungen und Personalmangel. Gut ausgebildete Fachärzt*innen mit Spezialisierung in Kinder- und Jugendgastroenterologie werden für eine flächendeckende qualifizierte Versorgung weiterhin benötigt. Zukünftige Studien sollten auch den kindergastroenterologischen Versorgungsbedarf aus Sicht anderer Gruppen einbeziehen, wie betroffener Patienten*innen, internistischer Gastroenterolog*innen und niedergelassener Kinder- und Jugendärzt*innen.
Abstract
Introduction Children and adolescents with chronic gastrointestinal, pancreatic and liver diseases need age-appropriate and qualified treatment. A representative survey is used to analyse the structural and personnel-related outpatient and inpatient care of children with chronic gastrointestinal, pancreatic and liver diseases in Germany.
Methodology 319 paediatric and adolescent medicine clinics and 50 paediatric gastroenterology practices in Germany were invited to participate in the anonymous online survey via EFS Survey. The structure of the facilities, further training authorisations, cooperations, treatment and care data and an assessment of the need for care were systematically recorded and descriptively evaluated.
Results 81 clinics and 10 practices participated in the survey. Almost two thirds of the clinics (n=52) provide outpatient paediatric gastroenterology services. Mostly up to 10 (25.4%) or 20 hours/week (33.8%). A quarter of the clinics do not offer consultation hours. Outpatient care needs cannot be met by two-thirds of the institutions. Half of all clinics stated that inpatient paediatric gastroenterology care needs can be met. However, one third cannot cover this and only rarely are there unused capacities. 35 clinics (43.2%) have a further training authorisation according to the state medical association (n=33) and/or are a further training centre of the Society for Paediatric Gastroenterology and Nutrition (GPGE) (n=18).
Conclusion There is a deficit in both outpatient and inpatient care in paediatric and adolescent gastroenterology. This results, among other things, from the economic framework conditions and a lack of personnel. Well-trained specialists with specialisation in paediatric and adolescent gastroenterology are still needed to provide qualified care throughout the country. Future studies should also include the need for paediatric gastroenterological care from the perspective of other groups, such as affected patients, internal gastroenterologists and paediatricians in private practice.
Schlüsselwörter
Versorgungsstruktur - Kinder- und Jugendmedizin - Kindergastroenterologie - KinderhepatologieKeywords
Care structure - paediatric and adolescent medicine - paediatric gastroenterology - paediatric hepatologyEinleitung
Die Kinder- und Jugendgastroenterologie ist eine der umfassendsten Subdisziplinen der Kinder- und Jugendmedizin, da sie sowohl angeborene als auch erworbene Erkrankungen des Gastrointestinaltraktes, der Bauchspeicheldrüse, der Leber und Gallenwege sowie Ernährungsstörungen vom Neugeborenen bis zum Adoleszenten einschließt, in vielfältigem interdisziplinären Austausch steht und Expertise in zahlreichen Untersuchungsmethoden erfordert [1]. Das Spektrum der Erkrankungen sowie die Untersuchungs- und Behandlungsmethoden im Kindes- und Jugendalter unterscheiden sich in vielen Bereichen erheblich von denen im Erwachsenalter [1], weshalb in aktuellen Leitlinien der Arbeitsgemeinschaft medizinischer Fachgesellschaften (AWMF) e.V. Pädiatrie-spezifische Aspekte in S3-Leitlinien der Deutschen Gesellschaft für Gastroenterologie, Verdauungs- und Stoffwechselerkrankungen (DGVS) e.V. (z.B. Morbus Crohn, Colitis Ulzerosa, Helicobacter pylori, Zöliakie, Gastroösophageale Refluxkrankheit, Reizdarmsyndrom, Autoimmune Lebererkrankungen oder Hepatitis B und C) berücksichtigt werden bzw. altersspezifische Krankheitsbilder in S2k-Leitlinien der Gesellschaft für pädiatrische Gastroenterologie und Ernährung (GPGE) e.V. (Cholestase im Neugeborenenalter, Obstipation und Stuhlinkontinenz, akute infektiöse Gastroenteritis im Säuglings-, Kindes- und Jugendalter) dargestellt werden [2] [3]. Zusätzlich bestehen für zahlreiche Medikamente in diesem Bereich keine Zulassung für das Kindes- und Jugendalter und es fehlen kindgerechte Darreichungen und Dosierungen [4]. Dies erfordert eine qualifizierte altersgerechte medizinische Versorgung durch Kinder- und Jugendgastroenterolog*innen [1].
Als Subdisziplin entwickelte sich die pädiatrische Gastroenterologie ab den 1960er Jahren rapide und mündete u.a. in der Gründung der European Society of Pediatric Gastroenterology (ESPG) im Jahr 1968 [5]. In den folgenden Jahren wurden die Bereiche Ernährungsmedizin und Hepatologie in das Fachgebiet eingeschlossen. 1974 fand die erste Sitzung der Mitteleuropäischen Arbeitsgemeinschaft für pädiatrische Gastroenterologie und Ernährung statt und 11 Jahre später wurde 1985 die deutschsprachige gemeinnützige „Gesellschaft für pädiatrische Gastroenterologie und Ernährung“ (GPGE) in Ising gegründet [6]. 2003 beschloss der 106. Deutsche Ärztetag schließlich, die Zusatzbezeichnung Kindergastroenterologie für Fachärzte der Kinder- und Jugendmedizin einzuführen – knapp 80 Jahre nach der Anerkennung des Facharztes für Magen-, Darm- und Stoffwechselerkrankungen im Jahr 1924 auf dem 43. Deutschen Ärztetag. Seitdem wurden die (Muster-) Weiterbildungsordnung in den Landesärztekammern eingeführt und Ärzt*innen in diesem Spezialgebiet ausgebildet. Die Weiterbildungsinhalte orientierten sich dabei an dem damaligen europäischen Ausbildungscurriculum für pädiatrische Gastroenterologie, Hepatologie und Ernährung [5]. Hierdurch sollten vor allem die Defizite in der flächendeckenden Versorgung chronisch kranker Kinder und Jugendlicher mit Magen-, Darm-, Leber- und Pankreaserkrankungen beseitigt werden und eine altersgerechte und qualifizierte Behandlung sichergestellt werden. Fast 20 Jahre nach Einführung der Zusatzweiterbildung in Deutschland ist eine systematische Analyse der qualitativen und strukturellen Versorgungssituation in diesem Versorgungsbereich als Grundlage weiterer Bedarfsplanungen notwendig.
Material und Methodik
Im Auftrag der Gesellschaft für pädiatrische Gastroenterologie und Ernährung (GPGE) e.V. erfolgte eine kontrollierte, strukturierte und anonyme Online-Umfrage in Deutschland mit dem Onlineportal EEF Survey. Hierzu wurden insgesamt 50 Arztpraxen mit kindergastroenterologischem Schwerpunkt aus dem Mitgliederverzeichnis der GPGE e.V. und 319 Kinderkliniken aus dem Verzeichnis der Deutschen Gesellschaft für Kinder- und Jugendmedizin (DGKJ) e.V. um ihre Teilnahme gebeten [7]. Eine Internetrecherche mit den Suchbegriffen „Klinik“, „Kindergastroenterologie“ und „(Bundesland)“ ergab 120 Treffer in Deutschland, welche sich alle auch im Klinikverzeichnis der DGKJ fanden.
Im Umfragezeitraum von August bis Oktober 2020 antworteten 10 Arztpraxen (20% Rücklaufquote) und 81 Kliniken (25% Rücklaufquote) aller Versorgungsstufen aus fast allen Bundesländern (bis auf das Saarland und Mecklenburg-Vorpommern). Insgesamt 54 Teilnehmende haben die Umfrage vollständig online abgeschlossen, 20 haben diese abgebrochen und wurden bei der Auswertung nicht berücksichtigt. Weitere 37 Kliniken oder Praxen haben den Fragebogen ausgedruckt und per Post oder E-Mail zugeschickt. Insgesamt bestand der Fragebogen für die Kliniken aus 17 Fragen und der Fragebogen für die Arztpraxen enthielt 12 Fragen (Supplement). Die ersten 10 Fragen des Fragebogens für die Kliniken und die ersten 7 des Fragebogens für die Arztpraxen befassten sich mit Strukturmerkmalen. Die Fragen 11 und 12 des Fragebogens für Kliniken und Frage 8 des Fragebogens für die Praxen erfragten die Weiterbildungssituation der Fachärzt*innen in der Kindergastroenterologie. Auskunft über Kooperationspartner konnten in den Fragen 13 (Klinik) und Frage 9 (Praxis) gegeben werden. Die Fragen 14 und 15 im Klinikfragebogen sowie Frage 10 und 11 im Praxisfragebogen evaluierten die Anzahlen der ambulanten und stationären kindergastroenterologischen Betreuungen bzw. Behandlungen 2019 für Darm-, Leber- und Gallenerkrankungen, parenterale Langzeiternährung, Patient*innen mit seltenen Erkrankungen und allgemeine Patient*innen der Kindergastroenterologie, sowie die Anzahl der technischen Untersuchungen für das Jahr 2019. Eine subjektive Einschätzung des kindergastroenterologischen Versorgungsbedarfs erfolgte für die Kliniken mit den letzten Fragen (15–17), und für die Praxis mit der Frage 12. Durch eine Vorabinformation über die während des Surveys abgefragten Daten sollte die Abbruchquote geringgehalten werden.
Die Daten wurden anonym in einer Access-Datenbank (Microsoft) erfasst und in IBM SPSS 2.6 sowie teilweise auch mit GraphPad Prism 9 (GraphPad Software LCC) statistisch ausgewertet. Neben deskriptiver Statistik wurden zweiseitige ungepaarte t-Tests für Gruppenvergleiche durchgeführt.
Die Ethikkommission Ulm wurde zu Beginn über das Forschungsprojekt informiert. Aufgrund des Studiendesigns, das keine Untersuchung von Patient*innen vorsieht, war kein formaler Ethikantrag erforderlich.
Ergebnisse
An der Umfrage nahmen 81 Kinderkliniken aus allen Versorgungsstufen teil. Hauptsächlich waren dies n=36 (45,7%) akademische Lehrkrankenhäuser (AKLKH), n=14 (17,3%) Krankenhäuser (KH) mit Schwerpunkt- und n=15 (18,5%) mit Maximal- oder Zentralversorgung (große städtische Kliniken und Universitätskliniken). Ein Drittel der Kinderkliniken (26 von 78) hatten 50 bis 100 Betten und ein Fünftel (19,2%) mehr als 100 Betten. Weniger als 50 Betten hatten Kliniken der Grund- (n=2; [2,6%]) und Regel- (n=11 [14,1%]), Schwerpunkt- (n=9) und Maximalversorgung (n=2) sowie AKLKH (n=12) und eine Rehaklinik angegeben.
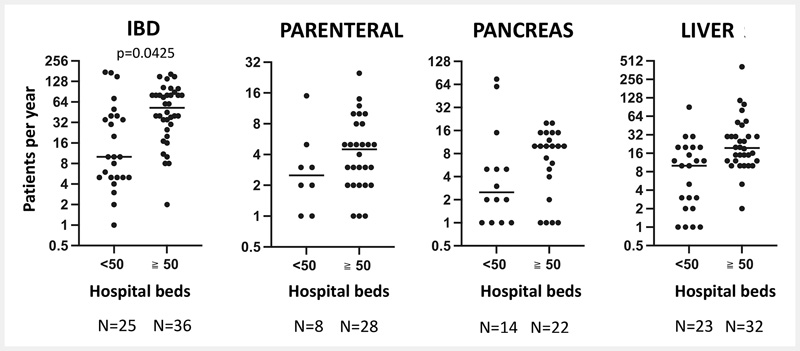
Die jährlichen stationären fachspezifischen Behandlungen im Jahr 2019 lagen von 71 Kliniken vor. Durchschnittlich wurden jährlich 981 Patient*innen behandelt (von 15 bis 10.850, Std.-Abw. 1545). Eine kontinuierliche ambulante oder stationäre Versorgung erfolgte bei durchschnittlich 49 Patient*innen mit chronisch-entzündlichen Darmerkrankungen, 27 mit Leber- und Gallenwegserkrankungen, 6 mit langzeitparenteraler Ernährung, 10 mit Pankreaserkrankungen, 12 Patienten mit seltenen Erkrankungen und 493 Patienten mit anderen gastroenterologischen Erkrankungen. Der Hauptanteil dieser Patienten wird in Kliniken mit ≥ 50 Betten betreut ([Abb. 1]). Knapp ein Drittel (n=26, 32%) der Kliniken verfügt über eine Tagesklinik, in denen Patient*innen zur Endoskopie (n= 25; 96%), Biologikatherapie (n=20, 77%) oder anderen diagnostischen oder therapeutischen Maßnahmen (n=18, 72%) versorgt werden. Kliniken der Grund- und Regelversorgung haben keine tagesklinischen Einrichtungen.

71 Kliniken machten Angaben zum wöchentlichen Sprechstundenangebot. Mehr als ein Viertel dieser Kliniken (n=19, 26,8%) gaben an, keine ambulante gastroenterologische Sprechstunden anzubieten. Häufig wurden bis zu 10 (n=18, 25,4%) oder 20 Stunden/Woche (n= 24, 33,8%) angegeben und nur 10 Kliniken (14,1%) liegen mit ihrer Sprechstundenzeit darüber (Mittelwert 16,2; SD 13.1; 0,5–80). Eine ambulante kindergastroenterologische Leistungsabrechnung erfolgt bei der Hälfte aller teilnehmenden Kliniken (n=41). Diese wird häufig über persönliche Ermächtigungen (n=27, 66%) sowie §120 SGB V (n=21, 51%) erstellt, wobei in 14 Fällen beide Abrechnungsverfahren zur Anwendung kommen. Der Anteil der Kliniken mit Leistungserbringung als Hochschulambulanz nach §117 SGB V (n=6, 15%) oder über ambulante spezialärztliche Versorgung §116b SGB V (n=3, 7%) ist gering, wovon hier von 2 Kliniken beide Leistungen abgerechnet werden können.
Sonografien werden an allen teilnehmenden Kliniken durchgeführt. Häufig werden diese in der eigenen pädiatrischen Sonografie (n=53, 65,4%) oder der Kinderradiologie (n=23, 28,4%) durchgeführt. Darüber hinaus haben viele (n=37; 45,7%) angegeben, diese auch selbst in der Kindergastroenterologie durchzuführen.
Endoskopien bei Kindern und Jugendlichen wurden an 79 der 81 teilnehmenden Kliniken durchgeführt. Häufig erfolgen diese allein durch die internistische Endoskopie (n=29, 36,7%), räumlich oder personell interdisziplinär (n=21, 26,6%) oder rein kindergastroenterologisch (n= 16, 20,3%). Die Sedierung wird in der internistischen Endoskopie in knapp der Hälfte der Fälle durch Anästhesist*innen (41%) und Pädiater*innen mit intensivmedizinischer Erfahrung (7%) durchgeführt, während diese bei rein kindergastroenterologischem Setting überwiegend durch die Kinderanästhesie (31%), Pädiater*innen mit intensivmedizinischer Erfahrung und Fachärzt*innen für Kinder- und Jugendmedizin (31%), pädiatrische Intensivmediziner*innen (19%) und Pädiater*innen mit intensivmedizinischer Erfahrung und Fachärzt*innen für Anästhesie (19%) erfolgen.
Das kindergastroenterologische Untersuchungsangebot und die Zahlen für Endoskopien, Leberbiopsien, 24-h (Impedanz)-pH und Atemtestdiagnostik sind in [Tab. 1] dargestellt. Signifikant mehr Untersuchungen pro Klinik für obere Endoskopien, Koloskopien, Gastrostoma-Anlagen und Leberbiopsien erfolgten an Kinderkliniken mit ≥ 50 Betten und in GPGE-Weiterbildungszentren ([Abb. 2] und [Abb. 3]).


Zwei Drittel (n=55, 67,6%) der Kliniken, insbesondere mit Maximal- und Zentralversorgung (13 von 15 entsprechend 86,7%), verfügen über einen kindergastroenterologischen Rufdienst. Dieser wird meist durch mehrere Fachabteilungen abgedeckt. Die internistische Endoskopie ist hierbei sehr häufig (n=41, 74,5%) und die Kinderchirurgie in 9 (16,3%) Krankenhäusern beteiligt.
Fachspezifisch pädiatrisch qualifiziertes Personal wurde an 68 der teilnehmenden Kliniken (84%) beschäftigt. Insgesamt waren 2019 an 42 Kliniken zertifizierte Kindergastroenterolog*innen (61,8%), an 59 Kliniken Ernährungsberater*innen, an 52 Kliniken Mitarbeiter*innen aus dem psychologischen Bereich, an 47 Kliniken Endoskopie- bzw. Funktionspersonal, an 13 Kliniken Logopäd*innen, an 6 Kliniken Physiotherapeut*innen und an 14 Kliniken weitere qualifizierte Berufsgruppen (klinische Linguist*innen, Schmerztherapeut*innen, Urotherapeut*innen und Kontinenztrainer*innen etc.) im Bereich der Kindergastroenterologie spezifisch tätig. Insgesamt waren 81 Ärzt*innen nach Landesärztekammer (LÄK) zertifizierte Kindergastroenterolog*innen mit einem Beschäftigungsumfang von 56,15 Vollzeitstellen an 42 Kliniken angestellt (Tabelle Supplement). Das sind durchschnittlich 1,9 zertifizierte Kindergastroenterolog*innen (Variationsbreite von 1 bis 5) auf 1,6 Vollzeitstellen (Variationsbreite von 0,1 bis 4). Eine Zertifizierung durch die Gesellschaft für pädiatrische Gastroenterologie und Ernährung (GPGE) e.V. lag bei 61 Ärzt*innen vor.
Eine Weiterbildungsbefugnis bestand an 35 (43,2%) Kliniken. An 32 Kliniken bestand eine volle Weiterbildungsbefugnis der Landesärztekammer (LÄK), 18 Kliniken waren durch die Gesellschaft für pädiatrische Gastroenterologie und Ernährung (GPGE) als Weiterbildungszentren (WBZ) zertifiziert. An fast allen (17 der 18) WBZ der GPGE bestand gleichzeitig eine Weiterbildungsbefugnis der LÄK. Es befanden sich insgesamt 59 Ärzt*innen für Kinder- und Jugendgastroenterologie an 29 Kliniken in der Weiterbildung.
Die Hälfte der Kliniken (n=43, 53%) gaben an, dass der stationäre kindergastroenterologische Versorgungsbedarf gedeckt werden kann. Etwas mehr als ein Drittel (n=31, 38%) kann diesen jedoch nicht abdecken und nur selten (n=7, 8,6%) wird von ungenutzten Kapazitäten berichtet ([Abb. 4]). Insbesondere teilnehmende Kliniken der Zentral- und Maximalversorgung geben zu zwei Dritteln an, dass die stationären Ressourcen nicht ausreichen. Hierfür werden Personalmangel (ärztlich und pflegerisch) und beschränkte Ressourcen (limitierte Bettenkapazitäten, Konflikt mit Akutversorgung, Engpässe in der Endoskopie) verantwortlich gemacht ([Abb. 5]). Der ambulante Versorgungsbedarf kann sogar von zwei Dritteln (n=55, 67,9%) der Institutionen nicht gedeckt werden ([Abb. 4]). Hierfür werden von 28 Kliniken (13 AKLKHs und 8 KHs mit Maximal- oder Zentralversorgung sowie 7 KHs der Schwerpunktversorgung) ökonomische Rahmenbedingungen als Grund angegeben ([Abb. 5]). Zusätzlich wurden von 36 Kliniken andere Ursachen angegeben, wie z.B. Mangel an qualifiziertem Personal (ärztlich und pflegerisch, insbesondere keine verfügbaren Kindergastroenterolog*innen), unzureichende Vergütung von Leistungen, Beschränkungen in der Leistungserbringung oder Entzug der Ermächtigung für ambulante Leistungserbringung, fehlendes Interesse des Einrichtungsträgers bzw. der Klinikleitung an Etablierung dieser Subdisziplin sowie eingeschränkte Ressourcen (räumliche Limitationen für Sprechstunde oder Sonografie, Konkurrenz mit allgemeinpädiatrischem Versorgungsauftrag, regionale kindergastroenterologische Unterversorgung v.a. im ländlichen Bereich) und lange Wartezeiten für die Erstvorstellung in der Spezialambulanz beklagt.


Insgesamt nahmen auch 10 von 50 angefragten niedergelassenen Kolleg*innen an der Umfrage teil, davon betreiben 7 eine kindergastroenterologische Schwerpunktpraxis und ein Kollege eine kindergastroenterologische Facharztpraxis. Im Durchschnitt wurden 700 kindergastroenterologische Behandlungen im Jahr 2019 durchgeführt (maximal 2560/Jahr). Das Sprechstundenangebot lag bei durchschnittlich 12,2 Stunden pro Woche und reichte von 0 (n=1), über ≤ 10 Stunden/Woche (n=5), ≤ 20 (n=2) und 24 (n=1), bis auf 40 (n=1). In 2 Praxen wurden auch Endoskopien durchgeführt. Angaben zu ambulanten Leberbiopsien, Gastrostoma-Anlagen oder 24h-(Impedanz-) pH-Metrien wurden keine gemacht. Die kindergastroenterologische Facharztpraxis führt auch Gastrostoma-Anlagen und Impedanz-pH-Metrien in einem stationären Setting durch, für 2 weitere Praxen trifft das für die Impedanz-pH-Metrie zu. In der kindergastroenterologischen Facharztpraxis besteht auch eine eingeschränkte Weiterbildungsmöglichkeit für Kindergastroenterologie nach LÄK. 5 der teilnehmenden Praxen sind auch Mitglieder in der Arbeitsgemeinschaft niedergelassener Kindergastroenterologen (ANGKE) der GPGE.
Diskussion
Diese Umfrage mit einer repräsentativen Stichprobe von Kinderkliniken aller Versorgungsstufen in Deutschland gewährt erstmals tiefere Einblicke in die strukturelle und personelle Versorgungssituation in der Kinder- und Jugendgastroenterologie.
Entsprechend der Kinderrechts-Konvention der Vereinten Nationen aus dem Jahr 1989 haben Kinder gemäß §24 das Recht auf den höchstmöglichen Gesundheitsstandard und auf Zugang zu einer entsprechenden Versorgung und Behandlung ihrer Erkrankungen [8].
Im Gegensatz zur Erwachsenenmedizin mit 951 ambulant tätigen Gastroenterolog*innen existiert neben der wohnortnahen hausärztlichen Versorgung durch Kinder- und Jugendärzt*innen keine flächendeckende ambulante spezialärztliche Versorgung durch kindergastroenterologische und hepatologische Schwerpunktpraxen bei niedergelassenen Kinder- und Jugendärzt*innen [9] [10]. Diese Umfrage zeigt, dass die ambulante kindergastroenterologische Versorgung im Wesentlichen in Spezialambulanzen der Kinderkliniken an Krankenhäusern der Schwerpunktversorgung, Akademischen Lehrkrankenhäusern und Kliniken der Maximal- und Zentralversorgung stattfindet. Insgesamt 120 Kinderkliniken in Deutschland weisen den Bereich Kindergastroenterologie gesondert auf ihrer Homepage aus. Dies wird auch durch Angaben der Bundesärztekammer aus dem Jahr 2019 gestützt, die insgesamt 278 Kindergastroenterolog*innen verzeichnet haben, von denen 203 dem stationären sowie 70 dem ambulanten Sektor zugeordnet und 5 ohne Zuordnung aufgeführt werden. Insgesamt 59 Kindergastroenterolog*innen (21%) sind in der Niederlassung tätig, aber nur eine an der Umfrage teilnehmende Praxis hat sich als alleinige kindergastroenterologische Facharztpraxis etabliert. Ursächlich hierfür ist die nicht kostendeckende Finanzierung kindergastroenterologischer Leistungen im ambulanten Bereich, sodass niedergelassene Ärzte mit der Zusatzbezeichnung Kindergastroenterologie aus wirtschaftlichen Gründen gezwungen sind, ihr Portfolio in der Patientenversorgung einzuschränken. Die geringe Teilnahme an der Befragung und die angegebenen verhältnismäßig geringen Patientenzahlen und Sprechstundenzeiten bestätigen dies eindrücklich. Die fehlende Refinanzierung der sprechenden Medizin ist ein generelles Problem der Gastroenterologie, da im EBM nur die endoskopischen Leistungen einigermaßen kostendeckend abgebildet sind [10]. Gerade in Zeiten begrenzter Versorgungskapazitäten an den Kliniken ließe sich die spezialärztliche Versorgung auch durch die niedergelassenen Ärzte in der Fläche gewährleisten und durch Kooperation mit spezialisierten Kinderkliniken und niedergelassenen Gastroenterologen die Versorgungsqualität verbessern.
Seit der Einführung der Zusatzbezeichnung Kinder- und Jugendgastroenterologie ist die Anzahl der anerkannten Kinder- und Jugendgastroenterologen in Deutschland stetig gestiegen – 2010 hatten nur 75 Ärzt*innen eine Zusatzbezeichnung der LÄK [11]. Trotz der Steigerung sind weiterhin nur an knapp zwei Dritteln der teilnehmenden Kliniken Kindergastroenterolog*innen beschäftigt, obwohl dort Kinder mit Darm-, Leber, oder Pankreas-Erkrankungen behandelt werden. Darüber hinaus sind zertifizierte Kindergastroenterolog*innen häufig in Teilzeit beschäftigt oder mit anderen ärztlichen Tätigkeiten beauftragt, sowie einige vorübergehend (z.B. Elternzeit) oder längerfristig nicht mehr in diesem Bereich aktiv tätig (z.B. durch anderen Tätigkeitsschwerpunkt, Wechsel ins Ausland). Sie stehen somit nicht vollumfänglich für die kindergastroenterologische und -hepatologische Versorgung zur Verfügung und die berechnete Anzahl von 20,3 Ärztekammer-zertifizierten Kindergastroenterolog*innen pro 1 Million Kinder und Jugendliche unter 18 Jahre in 2019 müsste entsprechend korrigiert werden. Unsere Umfrage zeigt, dass diese Zahl bereits aufgrund der Teilzeittätigkeit um 30% auf 14,2 pro 1 Million gekürzt werden müsste. Aktuelle Kennzahlen zum Vergleich aus anderen Ländern liegen nicht vor [12] [13]. In den USA waren 2004 ca. 9 Ärzt*innen pro 1 Million Kinder exklusiv in der pädiatrischen Gastroenterologie, Hepatologie und Ernährung tätig und wurden von einem zunehmenden Anteil an technischer und pflegerischer Assistenz unterstützt, um dem Mangel entgegenzuwirken [12]. Aber auch im Bereich des Assistenzpersonals wird in der Umfrage über Mangelsituationen berichtet, die in der Pädiatrie bereits allgegenwärtig sind [14]. Ebenso bestätigt der hohe Anteil an Kooperationen mit anderen Kinderkliniken mit Kindergastroenterologien den Mangel an spezialisierten Kinder- und Jugendgastroenterolog*innen, der in dieser Umfrage von einigen Teilnehmern beklagt wurde. Andererseits können gute standortübergreifende Kooperationen sowohl die spezialärztliche Versorgung als auch ein hohes Maß an Qualität sicherstellen.
An den meisten Kinderkliniken, die Kindergastroenterolog*innen beschäftigen, besteht bereits eine volle Weiterbildungsbefugnis der LÄK (32 von 42; 76%). Die Mindestanforderung nach §11 der neuen Musterweiterbildungsordnung (MWBO 2018) für die Zusatzweiterbildung Kinder- und Jugendgastroenterologie ist die Facharztanerkennung für Kinder- und Jugendmedizin und zusätzlich 24 Monate (18 Monate nach alter MWBO 2003) Weiterbildung in der Kinder- und Jugendgastroenterologie an einer befugten Weiterbildungsstätte [15]. Die GPGE bietet ihren Mitgliedern eine individuelle Zertifizierung als GPGE-Gastroenterolog*in an, die alle 5 Jahre erneuert werden muss. Im Jahr 2019 gab es insgesamt 219 von der GPGE zertifizierte Kindergastroenterolog*innen. Von den aktuell insgesamt 36 deutschen GPGE-Weiterbildungszentren nahm die Hälfte (n=18) an der Befragung teil [16]. Erfreulich ist, dass an fast allen Kliniken mit Weiterbildungsbefugnis auch tatsächlich eine Weiterbildung erfolgt und sich dort 2019 durchschnittlich jeweils 2 Ärzt*innen in der Weiterbildung befanden. An den Weiterbildungszentren werden auch signifikant mehr Untersuchungen durchgeführt, sodass an fast allen Standorten eine gute praktische Ausbildung der Weiterbildungsassistent*innen gewährleistet werden kann. Insgesamt kann man die strukturelle Weiterbildungssituation in der Kinder- und Jugendgastroenterologie in Deutschland als gut bezeichnen. Gut strukturierte praxisnahe Fort- und Weiterbildungsangebote für Ärzte und Pflegende zu versorgungsrelevanten Themen können zusätzlich zu einer guten Versorgungsqualität beitragen.
Weiterhin zeigt die Umfrage, dass an zahlreichen Kliniken auch dank der Integration von nicht ärztlichem, ausgebildetem und erfahrenem Personal innerhalb der Klinik sowie durch Kooperationen mit anderen Fachabteilungen die geforderte Strukturqualität sowie ein pädiatrisch-ganzheitliches Behandlungsspektrum erreicht wird [17]. An vielen Standorten sind multiprofessionelle Teams mit zum Beispiel Funktionspersonal, Ernährungsberater*innen und Psycholog*innen verfügbar. Insbesondere an Kliniken der Zentral- und Maximalversorgung ist ein kindergastroenterologischer Rufdienst verfügbar. In Kooperation mit der internistischen Endoskopie wird meist die Notfallendoskopie abgesichert, da in der Regel aufgrund der unzureichenden Ausstattung mit qualifiziertem Personal kein 24/7 Ruf- oder Bereitschaftsdienst abgedeckt werden kann.
Ein Drittel aller teilnehmenden Kinderkliniken (31 von 81) und zwei Drittel der Kliniken mit Maximal- und Zentralversorgung (10 von 15) geben an, den stationären Versorgungsbedarf im Bereich Kinder- und Jugendgastroenterologie nicht decken zu können. Dieser geäußerte Mangel erfordert eine genauere Analyse der Versorgungskapazitäten. Als Grund wird neben dem Mangel an qualifiziertem Personal vor allem die nicht ausreichende Bettenkapazität genannt. Deutschlandweit ist seit Jahren die Anzahl der Kinderkliniken und Bettenkapazität an Planbetten stark rückläufig. Allein im Zeitraum von 2004 bis 2017 wurde die Bettenkapazität um 2356 Betten bzw. 11,3% von 20.935 auf 18.579 kontinuierlich abgebaut, das entspricht 22,5 Betten pro 100.000 Einwohner im Jahr 2017 [18] [19]. Dies widerspricht der aktuellen demografischen Entwicklung, die eine stetige Zunahme der Kinder unter 18 Jahren seit 2013 mit 13,075 Mio. auf 13,74 Mio. in 2020 zeigt [20]. Außerdem sollten bei der Analyse der Versorgungsrealität, wie von der Deutschen Gesellschaft für Kinder- und Jugendmedizin (DGKJ) e.V. gefordert, nicht die Anzahl der Planbetten, sondern die tatsächlich betreibbaren Betten zugrunde gelegt werden [21]. Dies bestätigt auch das Ergebnis unserer Umfrage und steht im Widerspruch zur Einschätzung der Bundesregierung, dass keine strukturelle Unterversorgung in der Pädiatrie besteht [22].
In einem Positionspapier des Berufsverbandes Kinder- und Jugendärzte (BvKJ) e.V., des PädNetzS, des Paednet Südbaden e.V., des Verbandes leitender Kinder- und Jugendärzte und Kinderchirurgen Deutschlands (VLKKD) und der Landesärztekammer Baden-Württemberg wird vor einer existentiellen Gefährdung der Qualität der gegenwärtigen vorgehaltenen Strukturen gewarnt [23]. Weiterhin ist aber auch die flächendeckende ambulante pädiatrische Grundversorgung aus Sicht des BvKJ in Gefahr [9]. Die aktuelle epidemiologische Entwicklung und die Zunahme von Kindern und Jugendlichen mit chronischen Erkrankungen aus dem Bereich der pädiatrischen Hepatologie und Gastroenterologie, wie zum Beispiel Adipositas mit Fettleberhepatitis, chronischen rezidivierenden Bauchschmerzen, Nahrungsmittelallergien, Zöliakie oder auch chronisch-entzündlichen Darmerkrankungen, führt zu unzureichenden spezialärztlichen Versorgungskapazitäten mit langen Wartezeiten. Das Kindernetzwerk kritisiert bereits seit einigen Jahren eine Unterversorgung von chronisch kranken Kindern und Jugendlichen [24]. Die Kapazitäten der Spezialambulanzen werden u.a. aus Kostengründen wegen unzureichender Re-Finanzierung von den Trägern der Einrichtungen weiter reduziert. Diese Entwicklung wird für die Kinder- und Jugendgastroenterologie in unserer Umfrage bestätigt. Durch den Verlust der Kinderkrankenpflege als eigenständige Ausbildung ist zu befürchten, dass die Versorgungssituation in der ambulanten und stationären Kinderkrankenpflege in Zukunft noch prekärer wird [14]. Hieraus ergibt sich für Kinder- und Jugendliche mit chronischen Darm-, Leber- und Pankreaserkrankungen, dass der Anspruch auf eine dem Alter entsprechende medizinische und fachärztliche Versorgung nicht garantiert werden kann. Eine flächendeckende ambulante und stationäre Versorgungsstruktur, wie sie in der Erwachsenenmedizin vorgehalten wird, kann für die Kinder- und Jugendgastroenterologie als nicht realistisch angesehen werden [17]. Eine ambulante gastroenterologische Grundversorgung mit Abklärung und Behandlung von beispielsweise Bauchschmerzen und Obstipation kann bereits durch niedergelassene Kinder- und Jugendärzte erfolgen, hierfür wird zunächst noch keine spezialärztliche Konsultation benötigt. Dennoch erfordern die epidemiologische Entwicklung und die Fortschritte in der Diagnostik und Therapie der Erkrankungen für die schweren, chronischen oder seltenen Erkrankungen ein fachärztliches kindergastroenterologisches Versorgungsangebot. Hierfür wird eine entsprechende spezialärztliche Bedarfsplanung benötigt. Im Hinblick auf die Versorgung der Patient*innen und die Ausbildung des ärztlichen Nachwuchses wird u.a. von der DGKJ gefordert, Sprechstunden als Institutsambulanzen führen zu dürfen, einen Sicherstellungszuschlag Kinder- und Jugendmedizin einzuführen, um die flächendeckende Versorgung zu sichern und einen Maximalversorger-Zuschlag für die Versorgung von komplexen und chronisch kranken Kindern zu gewähren [14].
Diese Umfrage beinhaltet Limitationen aufgrund ihres Designs bezüglich Antwortrate und Erreichbarkeit der Teilnehmenden für Rückfragen [25]. Die Umfrage erfasst mit 81 teilnehmenden Kliniken 25% aller angefragten Kinderkliniken. Es ist anzunehmen, dass viele der 199 Kliniken ohne Kindergastroenterologie nicht an der Umfrage teilgenommen haben und sich die Teilnehmenden hauptsächlich aus den 120 Kliniken mit eigener Kindergastroenterologie rekrutieren. Diese Annahme lässt sich aufgrund des Rücklaufes und der Anonymität der Umfrage nicht klären, sollte aber als Selektions-Bias bei der Interpretation der Daten berücksichtigt werden. Das würde bedeuten, dass sich die Gesamtsituation auf alle Kinderkliniken übertragen noch deutlich schlechter darstellt. Im niedergelassenen Bereich konnten wir nur 40 der 59 laut Bundesärztekammer tätigen niedergelassenen Kindergastroenterolog*innen über das Mitgliederverzeichnis der GPGE identifizieren. Davon haben insgesamt 10 (entsprechend 20% bzw. 17%) teilgenommen.
Unser Fragebogen erfasst die Strukturqualität anhand einer anonymen Selbstauskunft und ist nicht überprüfbar. Die Anonymität der Umfrage erleichtert möglicherweise auch kritische Antworten zur Versorgungssituation der eigenen Institution. Dies könnte sich insbesondere für die Erhebung der Bedarfsdeckung vorteilhaft auswirken. Eine nicht anonyme Umfrage hätte jedoch einige Vorteile in Bezug auf die Möglichkeiten einer Verbesserung der Rücklaufquote und Datenanalyse geboten. Für eine umfassende Bedarfsanalyse sollten zukünftig weitere relevante Gruppen, wie betroffene Patientengruppen bzw. Patientenvereinigungen und die niedergelassenen Kinder- und Jugendärzte und internistische Gastroenterologen einbezogen werden.
Schlussfolgerung
Diese Umfrage zeigt, dass die Subdisziplin der Kinder- und Jugendgastroenterologie deutschlandweit an den Kinderkliniken etabliert wurde und es ausreichend Weiterbildungszentren gibt. Dennoch besteht häufig ein ambulantes und stationäres Versorgungsdefizit. Hierfür werden hauptsächlich die ökonomischen Rahmenbedingungen sowie nicht ausreichende räumliche und personelle Ressourcen als Ursachen genannt. Die insbesondere im ambulanten Bereich identifizierten Versorgungslücken machen deutlich, dass eine kostendeckende spezialärztliche ambulante Leistungsvergütung dringend erforderlich ist. Außerdem werden für eine qualifizierte Versorgung noch mehr gut ausgebildete Fachärzt*innen mit Spezialisierung in der Kinder- und Jugendgastroenterologie benötigt. Zukünftige Studien sollten auch die Sicht anderer relevanter Gruppen auf den kindergastroenterologischen und -hepatologischen Versorgungsbedarf einbeziehen. Etwa die Perspektive betroffener Patient*innen, internistischer Gastroenterolog*innen oder niedergelassener Kinder- und Jugendärzt*innen.
Beitrag der Autoren
Die Autoren haben wie folgt zum Manuskript beigetragen: Konzeption der Umfrage (MZ, CP, MC, SD, SB, SS, RM, AK), Erstellung der Online-Umfrage (MZ), Durchführung der Umfrage (MZ, CP, SH), Sammlung und Auswertung der Daten sowie deren Interpretation (MZ, CP), Erstellung des Manuskriptes (CP) und kritische Revision (alle Autoren).
Introduction
Paediatric and adolescent gastroenterology is one of the most comprehensive subdisciplines of paediatric and adolescent medicine, as it includes both congenital and acquired diseases of the gastrointestinal tract, pancreas, liver and bile ducts, as well as nutritional disorders from the newborn to adolescence and is involved in diverse interdisciplinary exchanges and requires expertise in numerous examination methods [1]. The spectrum of diseases as well as the examination and treatment methods in childhood and adolescence differ considerably in many areas from those in adulthood [1], which is why current guidelines of the Association of Medical Societies (AWMF) e. V. include paediatrics-specific aspects in S3 guidelines of the German Society of Gastroenterology, Digestive and Metabolic Diseases (DGVS) e. V. (e. g. Crohn's disease, ulcerative colitis, Helicobacter pylori, coeliac disease, gastro-oesophageal reflux disease, irritable bowel syndrome, autoimmune liver diseases or hepatitis B and C), or age-specific clinical pictures are presented in S2k guidelines of the German-speaking Society of Paediatric Gastroenterology and Nutrition (GPGE) e. V. (cholestasis in neonates, constipation and faecal incontinence, acute infectious gastroenteritis in infants, children and adolescents) [2] [3]. In addition, many drugs in this area are not approved for use in children and adolescents, and there is a lack of child-friendly presentations and dosages [4]. This requires qualified age-appropriate medical care by paediatric and adolescent gastroenterologists [1].
As a sub-discipline, paediatric gastroenterology developed rapidly from the 1960 s onwards, culminating, among other things, in the foundation of the European Society of Pediatric Gastroenterology (ESPG) in 1968 [5]. In the following years, nutritional medicine and hepatology were included in the specialty. In 1974, the first meeting of the Central European Working Group for Paediatric Gastroenterology and Nutrition took place and 11 years later, the German-speaking non-profit "Society of Paediatric Gastroenterology and Nutrition" (GPGE) was founded in Ising in 1985 [6]. In 2003, the 106th German Medical Congress finally decided to introduce the additional title of paediatric gastroenterology for specialists in paediatric and adolescent medicine - almost 80 years after the recognition of the specialist in gastrointestinal and metabolic diseases in 1924 at the 43 rd German Medical Congress. Since then, the (model) further training regulations have been introduced in the state medical associations and doctors have been trained in this speciality. The content of further training was based on the European training curriculum for paediatric gastroenterology, hepatology and nutrition [5]. The main aim was to eliminate the deficits in the comprehensive care of chronically ill children and adolescents with gastrointestinal, liver and pancreatic diseases and to ensure age-appropriate and qualified treatment. Almost 20 years after the introduction of additional training in Germany, a systematic analysis of the qualitative and structural care situation in this care area is necessary as a basis for further demand planning.
Material and methodology
On behalf of the German-speaking Society of Paediatric Gastroenterology and Nutrition (GPGE) e. V., a controlled, structured and anonymous online survey was conducted in Germany using the online portal EEF Survey. For this purpose, a total of 50 medical practices with a focus on paediatric gastroenterology from the GPGE e. V. member directory and 319 paediatric clinics from the directory of the German Society for Paediatric and Adolescent Medicine (DGKJ) e. V. were asked to participate [7]. An internet search using the search terms "clinic", "paediatric gastroenterology" and "(federal state)" resulted in 120 hits in Germany, all of which were also found in the DGKJ clinic directory.
In the survey period from August to October 2020, 10 medical practices (20 % response rate) and 81 clinics (25 % response rate) of all care levels from almost all federal states (except for Saarland and Mecklenburg-Western Pomerania) responded. A total of 54 participants completed the survey in full online, 20 dropped out and were not included in the evaluation. A further 37 clinics or practices printed out the questionnaire and sent it by post or e-mail. In total, the questionnaire for the clinics consisted of 17 questions and the questionnaire for the medical practices contained 12 questions. The first ten questions of the questionnaire for the clinics and the first seven of the questionnaire for the medical practices dealt with structural characteristics. Questions 11 and 12 of the questionnaire for clinics and question 8 of the questionnaire for practices asked about the further training situation of the specialists in paediatric gastroenterology. Information about cooperation partners could be provided in questions 13 (clinic) and 9 (practice). Questions 14 and 15 in the clinic questionnaire and questions 10 and 11 in the practice questionnaire evaluated the number of outpatient and inpatient paediatric gastroenterology services and treatments in 2019 for intestinal, liver and biliary diseases, long-term parenteral nutrition, patients with rare diseases and general paediatric gastroenterology patients, as well as the number of technical examinations for 2019. A subjective assessment of the need for paediatric gastroenterology care was made for the clinics with the last questions (15–17), and for the practice with question 12. The dropout rate was to be kept low by providing advance information about the data requested during the survey.
The data were recorded anonymously in an Access database (Microsoft) and statistically analysed in IBM SPSS 2.6, and partly also with GraphPad Prism 9 (GraphPad Software LCC). In addition to descriptive statistics, two-sided unpaired t-tests were conducted for group comparisons.
The Ethics Committee Ulm was informed about the research project at the beginning. Due to the study design, which does not include an examination of patients, no formal ethics application was required.
Results
81 paediatric hospitals from all levels of care participated in the survey. Mainly these were n = 36 (45.7 %) academic teaching hospitals (AKLKH), n = 14 (17.3 %) hospitals with focus and n = 15 (18.5 %) with maximum or central care (large municipal hospitals and university hospitals). One third of the paediatric hospitals (26 out of 78) had 50 to 100 beds and one fifth (19.2 %) had more than 100 beds. Less than 50 beds were reported by primary (n = 2; (2.6 %)) and regular (n = 11 (14.1 %)), specialised (n = 9) and maximum care (n = 2) hospitals, as well as AKLKH (n = 12) and one rehabilitation hospital.
The annual inpatient specialist treatments in 2019 were available from 71 clinics. On average, 981 patients were treated annually (from 15 to 10,850, SD 1545). Continuous outpatient or inpatient care was provided to an average of 49 patients* with inflammatory bowel disease, 27 with liver and biliary tract disease, 6 with long-term parenteral nutrition, 10 with pancreatic disease, 12 patients with rare diseases and 493 patients with other gastroenterological diseases. The majority of these patients are cared for in clinics with ≥ 50 beds ([Abb. 6]) ). Almost one third (n = 26, 32 %) of the clinics have a day clinic in which patients are treated for endoscopy (n = 25; 96 %), biological therapy (n = 20, 77 %) or other diagnostic or therapeutic measures (n = 18, 72 %). Primary and general care hospitals do not have day-care facilities.
Seventy-one clinics provided information on weekly consultation hours. More than a quarter of these clinics (n = 19, 26.8 %) stated that they did not offer any outpatient gastroenterology consultations. Often up to 10 (n = 18, 25.4 %) or 20 hours/week (n = 24, 33.8 %) were given and only 10 clinics (14.1 %) exceeded this with their consultation hours (mean 16.2; SD 13.1; 0.5–80). Outpatient paediatric gastroenterology services are billed at half of all participating hospitals (n = 41). This is often done via personal authorisations by the Association of Statutory Health Insurance Physicians (n = 27, 66 %) as well as § 120 of the German Social Code (SGB) V (n = 21, 51 %), whereby both billing procedures are used in 14 cases. The proportion of clinics providing services as university outpatient clinics according to § 117 SGB V (n = 6, 15 %) or via outpatient specialist care § 116b SGB V (n = 3, 7 %) is low, of which two clinics can bill for both services.
Sonographies are performed at all participating hospitals. Frequently, these are performed in the in-house paediatric sonography (n = 53, 65.4 %) or paediatric radiology (n = 23, 28.4 %). In addition, many (n = 37; 45.7 %) stated that they also perform them themselves in paediatric gastroenterology.
Endoscopies in children and adolescents were performed at 79 of the 81 participating hospitals. These are often performed by internal endoscopy alone (n = 29, 36.7 %), spatially or personnel interdisciplinary (n = 21, 26.6 %) or purely paediatric gastroenterology units (n = 16, 20.3 %). In internal endoscopy, sedation is performed in almost half of the cases by anaesthetists (41 %) and paediatricians with experience in intensive care (7 %), while in a purely paediatric gastroenterological setting it is predominantly performed by paediatric anaesthetists (31 %), paediatricians with intensive care experience and specialists in paediatrics and adolescent medicine (31 %), paediatric intensive care specialists (19 %) and paediatricians with intensive care experience and specialists in anaesthesia (19 %).
The range of paediatric gastroenterology examinations and the figures for endoscopies, liver biopsies, 24-h (impedance) pH and breath test diagnostics are shown in [Tab. 2]. Significantly more examinations per clinic for gastrointestinal (GI), colonoscopies, gastrostomy sites and liver biopsies were performed at paediatric hospitals with ≥ 50 beds and in GPGE training centres ([Abb. 7] and [Abb. 8]).


Two thirds (n = 55, 67.6 %) of the hospitals, especially those with maximum and central care (13 out of 15, corresponding to 86.7 %), have a paediatric gastroenterology on-call service. This is usually covered by several specialist departments. Internal endoscopy is very frequently involved (n = 41, 74.5 %) and paediatric surgery in nine (16.3 %) hospitals.
Specialised paediatric qualified staff were employed at 68 of the participating clinics (84 %). In 2019, 42 hospitals employed certified paediatric gastroenterologists (61.8 %), 59 hospitals employed dieticians, 52 hospitals employed psychological staff, 47 hospitals employed endoscopy and functional staff, 13 hospitals employed speech therapists, 6 hospitals employed physiotherapists and 14 hospitals employed other qualified professional groups (clinical linguists, pain therapists, urotherapists and continence trainers, etc.) in the field of paediatric gastroenterology. A total of 81 doctors certified by the State Medical Association (LÄK) were employed as paediatric gastroenterologists at 42 hospitals with a total of 56.15 full-time positions (Table Supplement). This is an average of 1.9 certified paediatric gastroenterologists (range of variation from 1 to 5) per 1.6 full-time positions (range of variation from 0.1 to 4). Certification by the Society for Paediatric Gastroenterology and Nutrition (GPGE) e. V. was available for 61 doctors.
Further training authorisation existed at 35 (43.2 %) clinics. 32 hospitals were fully authorised by the State Medical Association (LÄK) to provide further training, 18 hospitals were certified by the Society for Paediatric Gastroenterology and Nutrition (GPGE) as further training centres (TC). At almost all (17 of the 18) of the GPGE's TC’s, there was also a further training authorisation from the LÄK. A total of 59 doctors for paediatric and adolescent gastroenterology were undergoing further training at 29 clinics.
Half of the hospitals (n = 43, 53 %) stated that the inpatient paediatric gastroenterology care demand can be met. However, slightly more than a third (n = 31, 38 %) cannot cover this and only rarely (n = 7, 8.6 %) is unused capacity reported ([Abb. 9]). In particular, two-thirds of participating hospitals in central and maximum care report that inpatient resources are insufficient. Staff shortages (medical and nursing) and limited resources (limited bed capacities, conflict with acute care, bottlenecks in endoscopy) are held responsible for this ([Abb. 10]). The need for outpatient care cannot even be met by two thirds (n = 55, 67.9 %) of the institutions ([Abb. 9]). Economic conditions were cited as the reason for this by 28 hospitals (13 AKLKHs and eight hospitals with maximum or centralised care as well as seven hospitals providing specialised care) ([Abb. 10]). In addition, other reasons were given by 36 hospitals, such as a lack of qualified staff (medical and nursing, in particular no available paediatric gastroenterology specialists), insufficient remuneration for services, restrictions in the provision of services or withdrawal of authorisation for outpatient service provision, lack of interest on the part of the facility owner or the hospital management in establishing these services. The complaints also included limited resources (spatial limitations for consultation hours or sonography, competition with general paediatric care, regional underuse of paediatric gastroenterology, especially in rural areas) and long waiting times for the first presentation at the special outpatient clinic.


A total of 10 out of 50 colleagues in private practice also took part in the survey, seven of whom run a paediatric gastroenterology practice and one a paediatric gastroenterology specialist practice. On average, 700 paediatric gastroenterology treatments were carried out in 2019 (maximum 2560/year). Consultation hours averaged 12.2 hours per week and ranged from 0 (n = 1), to ≤ 10 hours/week (n = 5), ≤ 20 (n = 2) and 24 (n = 1), to 40 (n = 1). Endoscopies were also performed in two practices. No data on outpatient liver biopsies, gastrostomy placements or 24 h (impedance) pH metry were provided. The paediatric gastroenterology practice also performs gastrostomy placement and impedance pH measurements in an inpatient setting, for two other practices this applies to impedance pH measurements. In the paediatric gastroenterology specialist practice, there is also a limited opportunity for further training in paediatric gastroenterology according to the LÄK. Five of the participating practices are also members of the GPGE working group of paediatric gastroenterologists in private practice (ANGKE).
Discussion
This survey with a representative sample of paediatric hospitals of all care levels in Germany provides for the first time deeper insights into the structural and personnel care situation in paediatric and adolescent gastroenterology.
According to the United Nations Convention on the Rights of the Child of 1989, children have the right to the highest attainable standard of health and to access to appropriate care and treatment for their medical conditions [8].
In contrast to adult medicine with 951 physicians in gastroenterology practice, there is no comprehensive outpatient specialised medical care by pediatric gastroenterologists in addition to the general practitioners' care close to home [9] [10]. This survey shows that outpatient paediatric gastroenterological care mainly takes place in special outpatient departments of paediatric clinics at academic teaching hospitals, and specialised, maximum and central care hospitals. A total of 120 children's hospitals in Germany show the subspeciality of paediatric gastroenterology separately on their homepage. This is also supported by data from the German Medical Association from 2019, which recorded a total of 278 paediatric gastroenterologists, of whom 203 are assigned to the inpatient sector and 70 to the outpatient sector, and five are listed without assignment. A total of 59 paediatric gastroenterologists (21 %) are in private practice, but only one of the practices participating in the survey has established itself as a sole paediatric gastroenterology specialist practice. The reason for this is that the financing of paediatric gastroenterology services in the outpatient sector does not cover costs, so that physicians in private practice with the additional title of paediatric gastroenterology are forced to limit their portfolio in patient care for economic reasons. The low participation in the survey and the reported relatively low patient numbers and consultation hours confirm this impressively. The lack of refinancing of talking medicine is a general problem in gastroenterology, as only endoscopic services are covered to some extent in the assessment factor for billing (EBM) [10]. Particularly in times of limited care capacities at the hospitals, specialised medical care could also be guaranteed by the physicians in private practice in the area and the quality of care could be improved through cooperation with specialised paediatric clinics and gastroenterologists in private practice.
Since the introduction of the additional title of paediatric and adolescent gastroenterology, the number of recognised paediatric and adolescent gastroenterologists in Germany has risen steadily - in 2010, only 75 doctors had an additional title from the LÄK [11] . Despite the increase, paediatric gastroenterologists are still only employed at just under two thirds of the participating hospitals, although children with intestinal, liver or pancreatic diseases are treated there. In addition, certified paediatric gastroenterologists are often employed on a part-time basis or commissioned with other medical activities, and some are temporarily (e. g. parental leave) or long-term no longer actively working in this field (e. g. due to a different focus of activity, move abroad). They are therefore not fully available for paediatric gastroenterology and paediatric hepatology care and the calculated number of 20.3 medical association-certified paediatric gastroenterologists per 1 million children and adolescents under 18 years of age in 2019 would have to be corrected accordingly. Our survey shows that this number would already have to be reduced by 30 % to 14.2 per 1 million due to part-time work. Current figures for comparison from other countries are not available [12] [13]. In the USA in 2004, about nine physicians per million children worked exclusively in paediatric gastroenterology, hepatology and nutrition and were supported by an increasing proportion of technical and nursing assistants to counteract the shortage [12] . However, the survey also reports shortages in the area of assistant staff, which are already ubiquitous in paediatrics [14]. Likewise, the high proportion of cooperations with other paediatric hospitals with paediatric gastroenterologies confirms the shortage of specialised paediatric and adolescent gastroenterologists, which was lamented by some participants in this survey. On the other hand, good inter-site cooperation can ensure both specialised care and a high level of quality.
Most paediatric hospitals that employ paediatric gastroenterologists are already fully authorised by the LÄK to provide further training (32 out of 42; 76 %). The minimum requirement according to § 11 of the new model further training regulations (MWBO 2018) for additional further training in paediatric and adolescent gastroenterology is a specialist qualification in paediatric and adolescent medicine and an additional 24 months (18 months according to the old MWBO 2003) of further training in paediatric and adolescent gastroenterology at an authorised further training institution [15]. The GPGE offers its members individual certification as a GPGE gastroenterologist, which must be renewed every 5 years. In 2019, there were a total of 219 paediatric gastroenterologists certified by the GPGE. Of the current total of 36 German GPGE training centres, half (n = 18) participated in the survey [16]. It is pleasing to note that further training is actually taking place at almost all clinics with further training authorisation, and an average of two doctors were undergoing further training there in 2019. Significantly more examinations are also carried out at the training centres, so that good practical training of the training assistants can be guaranteed at almost all locations. Overall, the structural situation for further training in paediatric and adolescent gastroenterology in Germany can be described as good. Well-structured, practice-oriented training and continuing education programmes for doctors and nurses on topics relevant to care can also contribute to a good quality of care.
Furthermore, the survey shows that at many clinics the required structural quality and a paediatric holistic treatment spectrum are also achieved thanks to the integration of non-medical, trained and experienced staff within the clinic as well as through cooperation with other specialist departments [17]. At many locations, multiprofessional teams are available with, for example, functional staff, nutritionists and psychologists. A paediatric gastroenterology on-call service is available in particular at central and maximum care hospitals. In cooperation with the internal endoscopy unit, emergency endoscopy is usually provided, as it is usually not possible to cover a 7/24 on-call or stand-by service due to the insufficient number of qualified staff.
One third of all participating paediatric hospitals (31 out of 81) and two thirds of hospitals with maximum and central care (10 out of 15) state that they are unable to meet the inpatient care demand in the field of paediatric and adolescent gastroenterology. This expressed shortage requires a more detailed analysis of the care capacities. In addition to the lack of qualified staff, the main reason given is the insufficient bed capacity. Throughout Germany, the number of paediatric clinics and bed capacity in terms of planned beds has been declining sharply for years. In the period from 2004 to 2017 alone, bed capacity was continuously reduced by 2356 beds or 11.3 % from 20,935 to 18,579, which corresponds to 22.5 beds per 100,000 inhabitants in 2017 [18] [19]. This contradicts the current demographic trend, which shows a steady increase in the number of children under 18 years of age from 13.075 million in 2013 to 13.74 million in 2020 [20]. Furthermore, as demanded by the German Society for Paediatrics and Adolescent Medicine (DGKJ) e. V., the analysis of care reality should not be based on the number of planned beds but on the beds that can actually be operated [21]. This also confirms the result of our survey and contradicts the Federal Government's assessment that there is no structural underuse in paediatrics [22].
In a position paper of the Professional Association of Paediatricians (BvKJ), the PaedNetzS, the Paednet Südbaden e. V., the Association of Head Paediatricians and Paediatric Surgeons in Germany (VLKKD) and the State Medical Association of Baden-Württemberg, there is a warning of an existential threat to the quality of the current structures [23]. Furthermore, from the BvKJ's point of view, comprehensive outpatient paediatric primary care is also in danger [9]. The current epidemiological development and the increase in children and adolescents with chronic diseases from the field of paediatric hepatology and gastroenterology, such as obesity with fatty liver hepatitis, chronic recurrent abdominal pain, food allergies, coeliac disease or also chronic inflammatory bowel diseases, leads to insufficient specialist care capacities with long waiting times. The German Children's Network has been criticising the underuse of care for chronically ill children and adolescents for several years [24]. The capacities of the special outpatient clinics are being further reduced by the providers of the facilities for cost reasons, among others, due to insufficient re-financing. This development is confirmed for paediatric and adolescent gastroenterology in our survey. Due to the loss of paediatric nursing as an independent training, it is to be feared that the supply situation in outpatient and inpatient paediatric nursing will become even more precarious in the future [14] . This means that children and adolescents with chronic intestinal, liver and pancreatic diseases will not be guaranteed the right to medical and specialist care appropriate to their age. A comprehensive outpatient and inpatient care structure, as is provided in adult medicine, cannot be considered realistic for paediatric and adolescent gastroenterology [17]. Basic outpatient gastroenterological care with clarification and treatment of abdominal pain and constipation, for example, can already be provided by paediatricians in private practice, for which a specialist consultation is not yet required. Nevertheless, the epidemiological development and the progress in the diagnosis and therapy of the diseases require specialist paediatric gastroenterological care for severe, chronic or rare diseases. For this purpose, a corresponding specialist demand planning is required. With regard to the care of patients and the training of young doctors, the DGKJ demands, among other things, that consultation hours be allowed to be run as outpatient clinics, that a guarantee supplement for paediatric and adolescent medicine be introduced to ensure comprehensive care and that a maximum care supplement be granted for the care of complex and chronically ill children [14].
This survey has limitations due to its design in terms of response rate and accessibility of participants for queries [25] . With 81 participating hospitals, the survey covers 25 % of all requested paediatric hospitals. It can be assumed that many of the 199 hospitals without paediatric gastroenterology did not take part in the survey and that the participants were mainly recruited from the 120 hospitals providing paediatric gastroenterology subspeciality. This assumption cannot be clarified due to the response rate and the anonymity of the survey, but should be considered as a selection bias when interpreting the data. This would mean that the overall situation, transferred to all paediatric clinics, is still significantly worse. In the private practice sector, we were only able to identify 40 of the 59 paediatric gastroenterologists working in private practice according to the German Medical Association via the GPGE membership directory. Of these, a total of 10 (corresponding to 20 % or 17 %) participated.
Our questionnaire records structural quality on the basis of an anonymous self-report and is not verifiable. The anonymity of the survey may also facilitate critical responses to the care situation of one's own institution. This could be particularly beneficial for the survey on the coverage of needs. However, a non-anonymous survey would have offered some advantages in terms of the possibilities of improving the response rate and data analysis. For a comprehensive needs analysis, other relevant groups should be included in the future, such as affected patient groups or patient associations and the paediatricians and internal gastroenterologists in private practice.
Conclusion
This survey shows that the sub-discipline of paediatric and adolescent gastroenterology has been established at paediatric hospitals throughout Germany and that there are sufficient further training centres. Nevertheless, there is often a deficit in outpatient and inpatient care. The main reasons cited for this are the economic framework conditions and insufficient spatial and personnel resources. The gaps in care identified in the outpatient sector in particular make it clear that cost-covering reimbursement for specialised outpatient services is urgently needed. In addition, more well-trained specialists with specialisation in paediatric and adolescent gastroenterology are needed for qualified care. Future studies should also include the perspective of other relevant groups on the need for paediatric gastroenterological and hepatological care. For example, the perspective of affected patients, internal gastroenterologists or paediatricians in private practice.
Authors contribution
The authors contributed to the manuscript as follows: conception of the survey (MZ, CP, MC, SD, SB, SS, RM, AK), preparation of the online survey (MZ), implementation of the survey (MZ, CP, SH), collection and analysis of the data as well as their interpretation (MZ, CP), preparation of the manuscript (CP) and critical revision (all authors).
Interessenkonflikt
Die Autoren geben an, dass keine finanziellen Interessenkonflikte bestehen. AK, SB, RM, SS, SD, MC und CP sind Mitglieder der Gesellschaft für Pädiatrische Gastroenterologie und Ernährung (GPGE) e.V.; AK, SB, SS, SD, MC und CP waren zum Zeitpunkt der Umfrage im Vorstand und Beirat der GPGE ehrenamtlich tätig; SH ist bei der GPGE angestellt. CP ist Mitglied der Deutschen Gesellschaft für Gastroenterologie, Verdauungs- und Stoffwechselkrankeiten (DGVS) und RM beim Bund niedergelassener Gastroenterologen (BNG).
-
Literatur
- 1 Day AS. Pediatric Gastroenterology-challenges great and small. Frontiers in pediatrics 2013; 1: 2
- 2 Posovszky C, Backendorf V, Buderus S. et al. S2k-Leitlinie „Akute infektiöse Gastroenteritis im Säuglings-, Kindes- und Jugendalter“ – AWMF Registernummer 068–003. Zeitschrift fur Gastroenterologie 2019; 57: 1077-1118
- 3 Gesellschaft für pädiatrische Gastroenterologie und Ernährung (GPGE) e.V.. 2021 https://www.gpge.eu/leitlinien
- 4 Karesh A, Tomaino J, Mulberg AE. Off-label use of medicine in pediatrics: focus on gastrointestinal diseases. Current opinion in pediatrics 2013; 25: 612-617
- 5 Milla PJ. The European training syllabus in pediatric gastroenterology, hepatology, and nutrition. Journal of pediatric gastroenterology and nutrition 2002; 34: 111-115
- 6 Behrens R, Buderus S, Bufler P. et al. 30 Jahre Gesellschaft für pädiatrische Gastroenterologie und Ernährung. In: Gesellschaft für pädiatrische Gastroenterologie und Ernährung e.V.. 2015
- 7 Deutsche Gesellschaft für Kinder- und Jugendmedizin (DGKJ) e.V. https://www.dgkj.de/veroeffentlichungen/kinderkliniken
- 8 United Nations. Convention on the Rights of the Child. 1989
- 9 Fischbach T, Fehr F, Fegeler U. Flächendeckende ambulante pädiatrische Versorgung in Deutschland. Monatsschrift Kinderheilkunde 2018; 166: 108-115
- 10 Bokemeyer B. Gastroenterologie in der Niederlassung in Weissbuch Gastroenterologie 2020/2021. Berlin/Boston: De Gryuter; 2019
- 11 Rodeck B. Gibt es genug pädiatrische Gastroenterologen?. DCCV Bauchredner 2010; 3: 64-67
- 12 Crandall WV, Barnard JA, Cohen MB. et al. Pediatric gastroenterology workforce survey, 2003–2004 – A report of the North American Society for Pediatric Gastroenterology, Hepatology and Nutrition. Journal of pediatric gastroenterology and nutrition 2005; 40: 397-405
- 13 Morinville V, Drouin E, Levesque D. et al. Canadian pediatric gastroenterology workforce: current status, concerns and future projections. Can J Gastroenterol 2007; 21: 653-664
- 14 Deutsche Gesellschaft für Kinder- und Jugendmedizin e. V. (DGKJ). Medizinische Versorgung von Kindern und Jugendlichen stärken – Versorgungslücken schließen! Positionspapier der DGKJ. 2020
- 15 Bundesärztekammer, Arbeitsgemeinschaft der deutschen Ärztekammern. (Muster-)Weiterbildungsordnung. 2018
- 16 Gesellschaft für pädiatrische Gastroenterologie und Ernährung (GPGE) e.V. GPGE zertifizierte Weiterbildungszentren. https://www.google.com/maps/d/viewer?mid=19vS26xDM70c-jDZiDvGNaRcmT-o&ll=50.70082121148441%2C6.723562749999999&z=6
- 17 Zimmer K-P, Rodeck B. Qualitätssicherung in der Kindergastroenterologie. Pädiatrische Gastroenterologie, Hepatologie und Ernährung 2013; 801-804
- 18 Landesärztekammer Baden-Württemberg. Weiterbildungsordnung (WBO) der Landesärztekammer Baden-Württemberg vom 18. Mai 2020. 2020
- 19 Deutsche Akademie für Kinder- und Jugendmedizin. Thesen zur Analyse und Zukunftsszenario der flächendeckenden medizinischen Versorgung der Kinder und Jugendlichen in Deutschland. 2013 https://www.yumpu.com/de/document/read/19170747/thesen-zur-analyse-und-zukunftsszenario-der-dakj
- 20 Statistisches Bundesamt. 2021 https://www.destatis.de/DE/Themen/Gesellschaft-Umwelt/Bevoelkerung/Bevoelkerungsstand/Tabellen/liste-altersgruppen.html
- 21 Deutsche Gesellschaft für Kinder- und Jugendmedizin (DGKJ) e.V. Kommentar der DGKJ, der GKinD und des VLKKD auf die Antwort der Bundesregierung auf die Kleine Anfrage der Fraktion DIE LINKE (Bundestags-Drucksache 19/7270). https://www.dgkj.de/kommentar-kinderkliniken
- 22 Bundesegierung. Notstand in Kindekliniken. Deutscher Bundestag 19 Wahlperiode. 2019 https://dserver.bundestag.de/btd/19/072/1907270.pdf
- 23 Fessle R, Clever U, Gaukler RA. et al. Ressourcensicherung in Baden-Württemberg. 2018
- 24 Kindernetzwerk e.V. Ungeregelt:Versorgung chronisch kranker Kinder. https://www.kindernetzwerk.de/de/agenda/Politikportal/2018/Oekonomisierung/Ungeregelt.php
- 25 Jones TL, Baxter MA, Khanduja V. A quick guide to survey research. Annals of the Royal College of Surgeons of England 2013; 95: 5-7
Korrespondenzadresse
Publication History
Received: 25 August 2021
Accepted after revision: 07 November 2021
Article published online:
16 March 2022
© 2022. The Author(s). This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial-License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/).
Georg Thieme Verlag KG
Rüdigerstraße 14, 70469 Stuttgart, Germany
-
Literatur
- 1 Day AS. Pediatric Gastroenterology-challenges great and small. Frontiers in pediatrics 2013; 1: 2
- 2 Posovszky C, Backendorf V, Buderus S. et al. S2k-Leitlinie „Akute infektiöse Gastroenteritis im Säuglings-, Kindes- und Jugendalter“ – AWMF Registernummer 068–003. Zeitschrift fur Gastroenterologie 2019; 57: 1077-1118
- 3 Gesellschaft für pädiatrische Gastroenterologie und Ernährung (GPGE) e.V.. 2021 https://www.gpge.eu/leitlinien
- 4 Karesh A, Tomaino J, Mulberg AE. Off-label use of medicine in pediatrics: focus on gastrointestinal diseases. Current opinion in pediatrics 2013; 25: 612-617
- 5 Milla PJ. The European training syllabus in pediatric gastroenterology, hepatology, and nutrition. Journal of pediatric gastroenterology and nutrition 2002; 34: 111-115
- 6 Behrens R, Buderus S, Bufler P. et al. 30 Jahre Gesellschaft für pädiatrische Gastroenterologie und Ernährung. In: Gesellschaft für pädiatrische Gastroenterologie und Ernährung e.V.. 2015
- 7 Deutsche Gesellschaft für Kinder- und Jugendmedizin (DGKJ) e.V. https://www.dgkj.de/veroeffentlichungen/kinderkliniken
- 8 United Nations. Convention on the Rights of the Child. 1989
- 9 Fischbach T, Fehr F, Fegeler U. Flächendeckende ambulante pädiatrische Versorgung in Deutschland. Monatsschrift Kinderheilkunde 2018; 166: 108-115
- 10 Bokemeyer B. Gastroenterologie in der Niederlassung in Weissbuch Gastroenterologie 2020/2021. Berlin/Boston: De Gryuter; 2019
- 11 Rodeck B. Gibt es genug pädiatrische Gastroenterologen?. DCCV Bauchredner 2010; 3: 64-67
- 12 Crandall WV, Barnard JA, Cohen MB. et al. Pediatric gastroenterology workforce survey, 2003–2004 – A report of the North American Society for Pediatric Gastroenterology, Hepatology and Nutrition. Journal of pediatric gastroenterology and nutrition 2005; 40: 397-405
- 13 Morinville V, Drouin E, Levesque D. et al. Canadian pediatric gastroenterology workforce: current status, concerns and future projections. Can J Gastroenterol 2007; 21: 653-664
- 14 Deutsche Gesellschaft für Kinder- und Jugendmedizin e. V. (DGKJ). Medizinische Versorgung von Kindern und Jugendlichen stärken – Versorgungslücken schließen! Positionspapier der DGKJ. 2020
- 15 Bundesärztekammer, Arbeitsgemeinschaft der deutschen Ärztekammern. (Muster-)Weiterbildungsordnung. 2018
- 16 Gesellschaft für pädiatrische Gastroenterologie und Ernährung (GPGE) e.V. GPGE zertifizierte Weiterbildungszentren. https://www.google.com/maps/d/viewer?mid=19vS26xDM70c-jDZiDvGNaRcmT-o&ll=50.70082121148441%2C6.723562749999999&z=6
- 17 Zimmer K-P, Rodeck B. Qualitätssicherung in der Kindergastroenterologie. Pädiatrische Gastroenterologie, Hepatologie und Ernährung 2013; 801-804
- 18 Landesärztekammer Baden-Württemberg. Weiterbildungsordnung (WBO) der Landesärztekammer Baden-Württemberg vom 18. Mai 2020. 2020
- 19 Deutsche Akademie für Kinder- und Jugendmedizin. Thesen zur Analyse und Zukunftsszenario der flächendeckenden medizinischen Versorgung der Kinder und Jugendlichen in Deutschland. 2013 https://www.yumpu.com/de/document/read/19170747/thesen-zur-analyse-und-zukunftsszenario-der-dakj
- 20 Statistisches Bundesamt. 2021 https://www.destatis.de/DE/Themen/Gesellschaft-Umwelt/Bevoelkerung/Bevoelkerungsstand/Tabellen/liste-altersgruppen.html
- 21 Deutsche Gesellschaft für Kinder- und Jugendmedizin (DGKJ) e.V. Kommentar der DGKJ, der GKinD und des VLKKD auf die Antwort der Bundesregierung auf die Kleine Anfrage der Fraktion DIE LINKE (Bundestags-Drucksache 19/7270). https://www.dgkj.de/kommentar-kinderkliniken
- 22 Bundesegierung. Notstand in Kindekliniken. Deutscher Bundestag 19 Wahlperiode. 2019 https://dserver.bundestag.de/btd/19/072/1907270.pdf
- 23 Fessle R, Clever U, Gaukler RA. et al. Ressourcensicherung in Baden-Württemberg. 2018
- 24 Kindernetzwerk e.V. Ungeregelt:Versorgung chronisch kranker Kinder. https://www.kindernetzwerk.de/de/agenda/Politikportal/2018/Oekonomisierung/Ungeregelt.php
- 25 Jones TL, Baxter MA, Khanduja V. A quick guide to survey research. Annals of the Royal College of Surgeons of England 2013; 95: 5-7