
Subscribe to RSS
DOI: 10.1055/s-0032-1310137
Cannulotome introduced via a percutaneous endoscopic gastrostomy (PEG) tube – new technique for release of a buried bumper
Corresponding author
Publication History
Publication Date:
11 January 2013 (online)

Buried bumper syndrome is a major complication of percutaneous endoscopic gastrostomy (PEG), in which the inner bumper of the PEG tube migrates to become embedded in the stomach wall. Several endoscopic strategies have been proposed for releasing the bumper, based on: external traction [1], endoscopic traction [2], external pressure [3] and dissection of the overgrowing tissue using a needle-knife [4], argon plasma coagulation, or a dilation balloon [5].
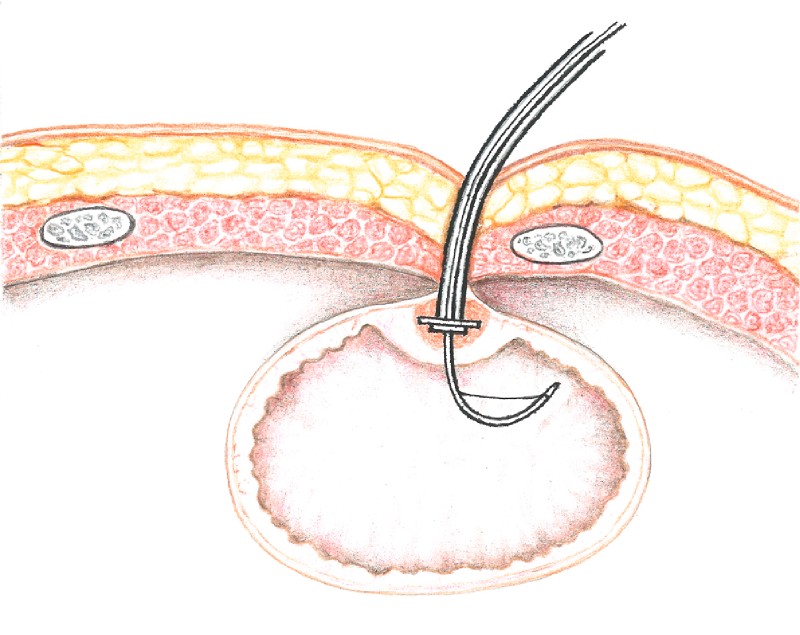
Between January 2000 and March 2012, 1226 PEG procedures were carried out in our endoscopy unit. A total of 35 cases of buried bumper syndrome (2.85 %) occurred in 32 patients during this period, 22 of which were suitable for endoscopic treatment. Based on this experience, we recommend the following treatment for buried bumper syndrome: insertion of a guide wire from the outside followed by dissection of the overgrowing tissue, and then pushing a PEG tube stiffened with a dilator into the stomach ([Fig. 1]) and retrieving the bumper with a snare.

Dissection of the overgrowing tissue seems to be crucial and there is a risk of complication. We usually use a needle-knife and argon plasma coagulator for this part of the procedure, but in five cases we used a novel technique in which we introduce a cannulotome via a PEG tube. That is, under endoscopic control provided by the first operator, the second operator inserts a cannulotome over the wire from the outside into the stomach through a shortened PEG tube. Leakage of air between the PEG tube and the cannulotome is sealed using a modified part of a dilator, which acts like a bushing ([Fig. 1]). While the cannulotome is bent and pulled slightly from the outside, the cutting wire dissects the tissue growing over the bumper ([Fig. 2] and [Fig. 3]; [Video 1]). Dissection proceeds from the centre of the buried bumper and traction is directed along the long axis of the cannula (which is not always perpendicular to the stomach wall); the length of the cuts should not exceed the radius of the bumper. Incisions should be carried out at the most prominent bulges, and three to five cuts are usually sufficient. With this technique, a buried PEG bumper can be released more rapidly and more safely compared with other currently used techniques.

Quality:
Endoscopy_UCTN_Code_TTT_1AO_2AK
#
Competing interests: None
Acknowledgment
This study was supported by research grant IGA NT/13414 from the Ministry of Health (Czech Republic).
-
References
- 1 Lee TH, Lin JT. Clinical manifestations and management of buried bumper syndrome in patients with percutaneous endoscopic gastrostomy. Gastrointest Endosc 2008; 68 (Suppl. 03) 580-584
- 2 Furlano RI, Sidler M, Haack H. The push-pull T technique: an easy and safe procedure in children with the buried bumper syndrome. Nutr Clin Pract 2009; 23 (Suppl. 06) 655-657
- 3 Binnebosel M, Klink CD, Otto J et al. A safe and simple method for removal and replacement of a percutaneous endoscopic gastrostomy tube after ‘buried bumper syndrome’. Endoscopy 2010; 42: E17-18
- 4 Ma MM, Semlacher EA, Fedorak RN et al. The buried gastrostomy bumper syndrome: prevention and endoscopic approaches to removal. Gastrointest Endosc 1995; 41 (Suppl. 05) 505-508
- 5 Strock P, Weber J. Buried bumper syndrome: endoscopic management using a balloon dilator. Endoscopy 2005; 37 (Suppl. 03) 279
Corresponding author
-
References
- 1 Lee TH, Lin JT. Clinical manifestations and management of buried bumper syndrome in patients with percutaneous endoscopic gastrostomy. Gastrointest Endosc 2008; 68 (Suppl. 03) 580-584
- 2 Furlano RI, Sidler M, Haack H. The push-pull T technique: an easy and safe procedure in children with the buried bumper syndrome. Nutr Clin Pract 2009; 23 (Suppl. 06) 655-657
- 3 Binnebosel M, Klink CD, Otto J et al. A safe and simple method for removal and replacement of a percutaneous endoscopic gastrostomy tube after ‘buried bumper syndrome’. Endoscopy 2010; 42: E17-18
- 4 Ma MM, Semlacher EA, Fedorak RN et al. The buried gastrostomy bumper syndrome: prevention and endoscopic approaches to removal. Gastrointest Endosc 1995; 41 (Suppl. 05) 505-508
- 5 Strock P, Weber J. Buried bumper syndrome: endoscopic management using a balloon dilator. Endoscopy 2005; 37 (Suppl. 03) 279