Key words
heart - cardiac - MR functional imaging - MR angiography - ischemia/infarction - normal
variants
Introduction
As competitive athletes symbolize vitality and health, they have always been granted
a status of special appreciation and prestige. This may explain the sense of tragedy
that comes with sudden cardiac death (SCD) in athletes, caused by a diverse set of
cardiovascular diseases such as hypertrophic and dilated cardiomyopathy (HCM/DCM),
myocarditis, arrhythmogenic right ventricular disease (ARVD), coronary anomalies or
even coronary artery disease (CAD) [1]
[2]. An overall incidence of 2.1/100,000/year [2] has fuelled interest in pre-participation screening and the identification of the
risk factors commonly responsible for SCD in elite athletes [3]
[4]
[5]. Of note, morphological and functional adaptations of the cardiovascular system
related to endurance training [6]
[7]
[8]
[9]
[10] must be distinguished from pathological findings of the myocardium. Congenital or
acquired anomalies should be excluded in order to minimize the risk for cardiac events
during physical activity. Previous approaches to pre-participation testing included
personal and family history as well as physical examination [3]
[4]
[11]
[12]
[13]. Due to a high percentage of abnormal electrocardiographic (ECG) findings in HCM
[14] and ARVD [5]
[11]
[12], an additional 12-lead ECG is recommended [15] since it has the potential to increase the sensitivity of the screening progress
[5]
[15]
[16]
[17]. However, these tests and even performing an additional echocardiography may fail
to detect risk factors especially with regard to coronary anomalies and subtle ischemic
and non-ischemic myocardial fibrosis. In this context, CMR imaging has turned out
to be the method of choice using delayed enhancement and high-resolution 3 D imaging
techniques [18]
[19]
[20]
[21]. Furthermore, CMR imaging allows the assessment of ventricular chamber volumes and
functional parameters with good inter- and intraobserver reliability [21]
[22].
The purpose of this study was to quantify the prevalence of potential risk factors
and determine ventricular functional parameters using CMR in elite athletes with unremarkable
pre-participation screening.
Methods
Study population
The study protocol was approved by the institutional ethics committee and all participants
gave written informed consent prior to the study.
We prospectively enrolled 100 healthy athletes (mean age 35.2 ± 11.4 years, range
from 18 to 62 years; 77 males, mean age 37.4 ± 11.4 years, range from 19 to 62 years;
23 females, mean age 28.4 ± 8.5 years, range from 18 to 50 years). The athletes were
highly trained long-distance runners (n = 39), cyclists (n = 8), triathletes (n = 34),
handball players (n = 13) and one speed skater with a training history of at least
two years and a weekly training workload of 13.1 ± 4.2 hours (males: 13.1 ± 4.5 hours/week,
range from 5 to 30 hours/week; females: 12.8 ± 3 hours/week, range from 7 to 20 hours/week).
The physical characteristics of the athletes are given in detail in [Table 1].
Table 1
Physical characteristics.
Tab. 1 Körperliche Eigenschaften.
|
total
|
male
|
female
|
|
age [years]
|
35.2 ± 11.4
|
37.4 ± 11.4
|
28.4 ± 8.5
|
|
height [m]
|
1.78 ± 7.6
|
1.81 ± 6.1
|
1.7 ± 6.2
|
|
weight [kg]
|
71 ± 9.7
|
72.9 ± 8.4
|
65.2 ± 11.4
|
|
BSA [kg/m²]
|
1.87 ± 0.16
|
1.91 ± 0.13
|
1.7 ± 0.2
|
|
heart rate [bpm]
|
55 ± 6.9
|
53 ± 6.7
|
58 ± 7.3
|
|
VO2 max.[ml/min]
|
55.5 ± 7.9
|
57.3 ± 6.9
|
50.1 ± 8.7
|
|
training hours/week
|
13.1 ± 4.2
|
13.1 ± 4.5
|
12.8 ± 3
|
In standard pre-participation screening which was performed prior to the CMR examination,
none of the participants showed any pathologies prohibiting their sports activities.
The BNP values were within normal ranges (< 100 ng/l) in all athletes and none of
the participants reported previous cardiovascular disease. Furthermore, all athletes
denied taking prohibited substances.
Cardiac magnetic resonance imaging protocol
All examinations (n = 95) were performed on a 1.5 Tesla MR system (Magnetom Avanto,
Siemens Medical Solutions, Forchheim, Germany) using surface coils for signal reception.
In 5 cases no CMR imaging data sets could be generated because of the withdrawal of
informed consent. For the evaluation of wall motion abnormalities and myocardial hypertrophy,
2 D cine steady-state free precession (SSFP) sequences were acquired in a 4-chamber
view, left ventricular long axis view (ECG-retrogating, repetition time (TR) 39.75,
echo time (TE) 1.12 ms, angle of excitation (FA) 70°, field of view (FOV) adapted
to each athlete, pixel spacing 1.8 × 1.8, matrix 156 × 192, slice thickness (SL) 6 mm,
bandwidth (BW) 930 Hz/pixel) as well as in short axis angulation (ECG-retrogating,
TR 58.96 ms, TE 1.13 ms, FA 70°, pixel spacing 2.4 × 1.8, matrix 113 × 192, SL 5 mm,
BW 930 Hz/pixel).
For coronary MR angiography (MRA), an ECG-gated 3 D GRE/SSFP sequence was combined
with respiratory navigator gating and tracking. The respiratory navigator was localized
at the lung-liver interface of the right hemidiaphragm with a 2 mm gating window.
The acquisition window and TR were adapted to the duration of the end-diastolic period
of rest and an individual trigger delay was determined in order to minimize myocardial
motion artifacts during the acquisition interval. The following settings were used:
spatial resolution (voxel size) 1.0 × 1.0 × 1.1 mm, TE 1.75 ms, FA 90°, matrix 216 × 320,
BW 601 Hz/pixel.
Furthermore, delayed enhancement imaging was performed 10 minutes after administration
of 0.15 mmol/kg body weight Gadobutrol (Gadovist, Bayer Healthcare, Leverkusen, Germany)
at a flow rate of 2.0 ml/s using an inversion recovery [IR] turbo FLASH 2 D sequence
(TR 700 ms. TE 4.91 ms, FA 30°, matrix 154 × 256, pixel spacing 1.5 × 1.12 mm, SL
8 mm, BW 140 Hz/Pixel). Optimal inversion time (TI) was determined using a TI scout
sequence (TR 23.49 ms, TE 1.12 ms, FA 60°, pixel spacing 3.5 × 1.8 mm, matrix 78 × 192,
SL 8 mm, BW 965 Hz/Pixel) to minimize the signal intensity of normal myocardium.
Imaging analyses
Two experienced readers independently reviewed the image loops of each subject in
a random fashion. Readers were blinded for subject details including age and training
hours/week.
Quantitative analysis was performed off-line using dedicated software (Leonardo VD30B,
Siemens Medical Solutions). The left ventricular (LV) and right ventricular (RV) wall
mass and volumes were measured by tracing the endocardial and epicardial borders on
the short-axis views. At the base of the LV, the aorta was included in the LV volume
below the aortic valve. Blood volumes above the aortic valve, as well as volumes surrounded
by a thin myocardial wall on the mitral valve plane (left atrial blood volume), were
excluded from the LV volume and the basal slice was selected for the left ventricle
when at least 50 % of the blood volume was surrounded by myocardium in both end-diastole
and end-systole. By inspection of the cine loops, end-systole was defined as the frame
with the smallest ventricular cavity. Papillary muscles and trabeculae were included
in the ventricular volumes (and excluded from the wall mass) for efficiency and reproducibility.
Epicardial fat and the pericardium were excluded from the RV and LV mass [17]. End-diastolic volumes (EDV) and end-systolic volumes (ESV) of the LV and RV were
calculated according to a modified Simpson’s rule in short axis views [17]
[18]
[19] and were used to determine stroke volume (SV) and ejection fraction (EF). The LV
mass was determined by summation of EDVs within the epicardial and endocardial borders
of the short-axis slices and by multiplying the myocardial tissue volume by its specific
density of 1.05 g/cm3. Atrial sizes were assessed by planimetry of the maximum right
atrial (RA) and left atrial (LA) areas in a standard 4-chamber view just before the
opening of the mitral valve. Pulmonary veins were excluded from the LA area [18]. Additionally, all parameters were indexed to the body surface area (BSA) for comparative
analysis in order to minimize differences of cardiac parameters related to height
and weight. The LV remodeling index (MM/LV-EDV) was calculated to determine the pattern
of ventricular remodeling.
Delayed enhancement images, the MR coronary angiography and the Cine SSFP images were
evaluated visually regarding wall motion abnormalities, coronary anomalies and ischemic
or non-ischemic patterns of delayed myocardial enhancement. In the event of a deviation
between both readers, the images were re-evaluated by both radiologists in consensus.
Statistics
The data were statistically analyzed using SPSS software, version 11.5 (SPSS, Inc,
Chicago, USA). Continuous data are presented as mean ± standard deviation. Normality
was tested using the Kolmogorov-Smirnov test. The inter-reader agreement regarding
chamber volumes, functional parameters and MM were evaluated using the Cohen’s Kappa
test. Pearson correlation coefficients were calculated for selected variables. A p-value
of less than 0.05 was considered statistically significant.
Results
For cine SSFP and delayed enhancement images, diagnostic image quality was obtained
in all of the 95 MRI examinations. The mean total imaging time was 50:42 min ± 10:12 min
(range from 34 to 74 min) and the acquisition time of the MR coronary angiography
was 14:33 min ± 5:25 min (range from 6:34 to 44:42 min).
The results of the evaluation of the chamber volumes, atrial sizes and functional
parameters are given in detail in [Table 2] and [Fig. 1]. The quantitative analyses showed a simultaneous increase of left ventricular chamber
size and MM, called eccentric hypertrophy of the left ventricle (LV-EDV: male 106.5 ± 12.9 ml/m²,
female 92.7 ± 6.4 ml/m²; MM: male 78.9 ± 10.2 g/m², female 61.4 ± 5.4 g/m²; remodeling
index: male 0.75, female 0.665). Furthermore, an enlargement of the right chamber
volumes (RV-EDV: male 122.6 ± 19.0 ml/m², female 99.9 ± 7.2 ml/m²) and an increased
LV-SV (male: 64.7 ± 10.0 ml/m², female 56.5 ± 5.7 ml/m²) as well as RV-SV (male: 66.7 ± 10.4 ml/m²,
female 54.2 ± 7.1 ml/m²) were found. The evaluation of the chamber and stroke volumes
as well as the MM revealed significantly elevated values for male athletes in comparison
to the female study population ([Table 2]). The Cohen’s kappa test showed good results regarding the interobserver variability
(κ-values are also shown in [Table 2]). There was a significant correlation between weekly training volume and LV-EDV
(r² = 0.2375, p = 0.0430) and LV-ESV (r² = 0.2465, p = 0.0355) in male athletes whereas
in female athletes no significant correlations between chamber volumes and training
load were found.
Table 2
Results of the evaluation of the ventricular volumes and functional parameters. A
p-value of < 0.05 was regarded as statistically significant. к-value in parentheses.
[LV] left ventricular [RV] right ventricular [EDV] end-diastolic volume [ESV] end-systolic
volume [SV] stroke volume [EF] ejection fraction [MM] myocardial mass [LA] left atrium
[RA] right atrium.
Tab. 2 Ergebnisse der quantitativen Auswertung von Ventrikelvolumina und Funktionsparametern.
Ein p-Wert von < 0,05 wurde als statistisch signifikant erachtet. к-Werte in Klammern.
[LV] linker Ventrikel [RV] rechter Ventrikel [EDV] enddiastolisches Volumen [ESV]
endsystolisches Volumen [SV] Schlagvolumen [EF] Ejektionsfraktion [MM] Myokardmasse
[LA] linker Vorhof [RA] rechter Vorhof.
|
total
|
male
|
female
|
p-values
|
|
LV-EDV [ml/m²]
|
103.3 ± 13.1 (0.80)
|
106.5 ± 12.9
|
92.7 ± 6.4
|
< 0.001
|
|
LV-ESV [ml/m²]
|
40.4 ± 8.2 (0.78)
|
41.8 ± 8.5
|
36.3 ± 5.2
|
0.007
|
|
LV-SV [ml/m²]
|
62.9 ± 9.7 (0.81)
|
64.7 ± 10.0
|
56.4 ± 5.7
|
0.001
|
|
LV-EF [%]
|
60.8 ± 5.7 (0.75)
|
60.8 ± 6.0
|
60.9 ± 4.8
|
0.916
|
|
RV-EDV [ml/m²]
|
118.4 ± 19.7 (0.67)
|
126.6 ± 19.0
|
99.9 ± 7.2
|
< 0.001
|
|
RV-ESV [ml/m²]
|
56.1 ± 14.2 (0,65)
|
59.9 ± 14.5
|
45.7 ± 7.3
|
< 0.001
|
|
RV-SV [ml/m²]
|
62.3 ± 10.4
|
66.7 ± 10.4
|
54.2 ± 7.1
|
< 0.001
|
|
RV-EF[%]
|
56.2 ± 5.4 (0.60)
|
52.6 ± 6.4
|
54.7 ± 5.6
|
0.191
|
|
MM [g/m²]
|
74.8 ± 11.9 (0.78)
|
78.9 ± 10.2
|
61.4 ± 5.4
|
< 0.001
|
|
remodeling index
|
0.726
|
0.750
|
0.665
|
0.0001
|
|
LA [cm²]
|
23.7 ± 4.7
|
24.8 ± 4.6
|
20.3 ± 3.6
|
0.0001
|
|
RA [cm²]
|
27.8 ± 5.6
|
29.5 ± 4.9
|
22.6 ± 3.3
|
< 0.0001
|
 Fig. 1 Results of the quantitative analysis of chamber volumes and functional parameters.
Left ventricular [LV] end-diastolic volume [EDV], end-systolic volume [ESV], stroke
volume [SV], ejection fraction [EF], myocardial mass [MM] as well as the results of
the left atrial [LA] and right atrial [RA] planimetry of male athletes are shown in
a, b; c, d show the results of the evaluation of female athletes.
Fig. 1 Results of the quantitative analysis of chamber volumes and functional parameters.
Left ventricular [LV] end-diastolic volume [EDV], end-systolic volume [ESV], stroke
volume [SV], ejection fraction [EF], myocardial mass [MM] as well as the results of
the left atrial [LA] and right atrial [RA] planimetry of male athletes are shown in
a, b; c, d show the results of the evaluation of female athletes.
Abb. 1 Ergebnisse der quantitativen Auswertung der Ventrikelvolumina und funktionellen Parametern.
a, b zeigen das enddiastolisches und endsystolische Volumen [EDV, ESV], das Schlagvolumen
[SV], die Ejektionsfraktion [EF] und die Myokardmasse [MM] des linken Ventrikels sowie
die Ergebnisse der Planimetrie von linkem und rechtem Vorhof [LA, RA] in männlichen
Athleten, c, d die Ergebnisse der Athletinnen.
However, pathological findings were detected in 6 athletes (6.3 %).
Regarding the coronary anomalies, we found one case with the circumflex artery originating
from the right coronary sinus and course posterior to the ascending aorta ([Fig. 2]). Furthermore, one athlete showed an atypical, anterior origin of the right coronary
artery (RCA), formally not according to a coronary anomaly but which might cause symptoms
of ischemia during exercise due to the long-distance course between the ascending
aorta and pulmonary trunk ([Fig. 3]). In addition, one athlete was suffering from ectasia of the ascending aorta ([Fig. 4]) but had normal blood pressure values (120/80 mmHg) and in 2 athletes we found pathological
signal alterations in the delayed enhancement imaging without corresponding wall motion
abnormalities, due to the spot-shaped pattern consistent with a non-ischemic, postinflammatory
genesis ([Fig. 5]). In addition, one of the athletes showed pleural effusions and pericardial effusion,
but no wall motion abnormalities or delayed enhancement of the myocardium ([Fig. 6]). On presentation, the athlete previously experienced a feverish infection, which
turned out to be an Epstein-Barr virus infection. 6 weeks later the athlete underwent
a control MRI examination which showed complete recovery.
 Fig. 2 ECG-gated 3-D MR angiography of a 46-year-old male triathlete with a training load
of 18 hours per week. a Origin of the left anterior descending artery from the left sinus (short arrow) and
of the right coronary artery from the right sinus (long arrow). b+c show the left circumflex artery (LCX), also originating from the right sinus (dotted
arrow) and taking course dorsal to the ascending aorta (dotted arrow in d), which represents the most common but benign variant of coronary anomaly.
Fig. 2 ECG-gated 3-D MR angiography of a 46-year-old male triathlete with a training load
of 18 hours per week. a Origin of the left anterior descending artery from the left sinus (short arrow) and
of the right coronary artery from the right sinus (long arrow). b+c show the left circumflex artery (LCX), also originating from the right sinus (dotted
arrow) and taking course dorsal to the ascending aorta (dotted arrow in d), which represents the most common but benign variant of coronary anomaly.
Abb. 2 EKG-getriggerte 3-D-MR-Angiografie eines 46-Jahre alten, männlichen Triathleten mit
einem Trainingspensum von 18 Stunden pro Woche. a Abgang des Ramus interventricularis anterior aus dem links-koronaren Sinus (kurzer
Pfeil) und der rechten Koronararterie aus dem rechts-koronaren Sinus (langer Pfeil).
b+c zeigen den Ramus circumflexus, welcher ebenso dem rechts-koronaren Sinus entspringt
(gepunkteter Pfeil) und dorsal der aszendierenden Aorta (gepunkteter Pfeil in d) verläuft, was der häufigsten und als benigne einzustufenden Variante einer Koronaranomalie
entspricht.
 Fig. 3 ECG-gated 3-D MR angiography of a 39-year-old male marathon runner with a training
load of 10 hours per week reveals a right coronary artery [RCA] originating from the
left corner of the right sinus which is formally not considered as a coronary anomaly
but might cause recurrent ischemic alterations due to the long course of the RCA between
the aorta and pulmonary trunk.
Fig. 3 ECG-gated 3-D MR angiography of a 39-year-old male marathon runner with a training
load of 10 hours per week reveals a right coronary artery [RCA] originating from the
left corner of the right sinus which is formally not considered as a coronary anomaly
but might cause recurrent ischemic alterations due to the long course of the RCA between
the aorta and pulmonary trunk.
Abb. 3 EKG-getriggerte 3-D-MR-Angiografie eines 39 Jahre alten, männlichen Marathonläufers
mit einem Trainingspensum von 10 Stunden pro Woche. Hier entspringt die rechte Koronararterie
[RCA] weit links im Bereich des rechts-koronaren Sinus, was formal nicht als Koronaranomalie
erachtet wird, aufgrund des langstreckigen Verlaufs der RCA zwischen Aorta und Truncus
pulmonalis jedoch zu rezidivierenden ischämischen Ereignissen führen kann.
 Fig. 4 43-year-old marathon runner with a training load of 10 hours per week. HASTE sequenz
shows an ectasia of the ascending aorta of 4.2 cm. This athlete will be closely monitored.
Fig. 4 43-year-old marathon runner with a training load of 10 hours per week. HASTE sequenz
shows an ectasia of the ascending aorta of 4.2 cm. This athlete will be closely monitored.
Abb. 4 Die HASTE-Sequenz eines 43-jährigen Marathonläufers mit einem Trainingspensum von
10 Stunden pro Woche zeigte eine Ektasie der Aorta aszendens auf 4,2 cm. Dieser Befund
wird engmaschig verlaufskontrolliert.
 Fig. 5 Delayed enhancement imaging 10 minutes after application of contrast medium of a
47-year-old female cyclist (a, b) and a 50-year-old male cyclist (c, d), both with a training load of 15 hours per week. We found disseminated and intramural
myocardial hyperenhancement representative for a non-ischemic type pattern and therefore
indicative of a previous myocarditis, in both cases without any wall motion abnormalities.
Fig. 5 Delayed enhancement imaging 10 minutes after application of contrast medium of a
47-year-old female cyclist (a, b) and a 50-year-old male cyclist (c, d), both with a training load of 15 hours per week. We found disseminated and intramural
myocardial hyperenhancement representative for a non-ischemic type pattern and therefore
indicative of a previous myocarditis, in both cases without any wall motion abnormalities.
Abb. 5 Delayed-Enhancement-Bildgebung 10 Minuten nach der Injektion von Kontrastmittel,
in a, b von einer 47-jährigen Radfahrerin und in c, d von einem 50 Jahre alten, männlichen Radfahrer, jeweils mit einem Trainingspensum
von 15 Stunden pro Woche. Hier fanden sich in beiden Athleten disseminierte, intramyokardiale
Signalalterationen vom nicht-ischämischen Verteilungsmuster als Zeichen einer stattgehabten
Myokarditis, in beiden Fällen ohne Nachweis von entsprechenden regionalen Wandbewegungsstörungen.
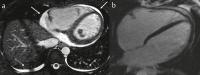 Fig. 6 a ECG-gated 3-D MR angiography of a 29-year-old triathlete reveals pericardial effusion
(arrows) and pleural effusions (dotted arrows), but no wall motion abnormalities or
b delayed enhancement of the myocardium. On presentation, the athlete previously experienced
a feverish infection, which turned out to be an Epstein-Barr virus infection. 6 weeks
later the athlete underwent a control MRI examination which showed complete recovery.
Fig. 6 a ECG-gated 3-D MR angiography of a 29-year-old triathlete reveals pericardial effusion
(arrows) and pleural effusions (dotted arrows), but no wall motion abnormalities or
b delayed enhancement of the myocardium. On presentation, the athlete previously experienced
a feverish infection, which turned out to be an Epstein-Barr virus infection. 6 weeks
later the athlete underwent a control MRI examination which showed complete recovery.
Abb. 6 a EKG-getriggerte 3-D-MR-Angiografie eines 29-jährigen Triathleten mit Nachweis eines
Perikardergusses (Pfeile) sowie von Pleuraergüsse (gepunktete Pfeile). Regionale Wandbewegungsstörungen
oder b pathologische Signalalterationen in der delayed enhancement-Bildgebung fanden sich
nicht. Anamnestisch gab dieser Athlet einen kürzlich durchgemachten, grippalen Infekt
an, welcher sich als Epstein-Barr-Virus Infektion erwies. Eine im Abstand von 6 Wochen
durchgeführte Verlaufskontrolle zeigte eine vollständige Rückläufigkeit der vorbeschriebenen
Befunde.
Discussion
In the last decades tragic reports of SCD in highly trained athletes have received
more and more attention. In most of the cases, cardiovascular diseases such as HCM,
myocarditis, ARVD, coronary anomalies and even coronary artery disease are either
retrospectively identified or have been ignored by doctors or the athletes [1]
[2]. This has evoked increasing interest in the determination of such acquired or congenital
cardiovascular diseases in athletes. In this context, the role of CMR examinations
in the screening process is increasingly discussed, especially since routine testing,
even in combination with echocardiography may fail in the detection of cardiovascular
diseases such as coronary anomalies and subtle myocardial fibrosis that can be found
in approximately 30 % of patients with DCM [23]. This is of major importance as the differentiation between “athlete’s heart” –
characterized by cavity dilatation and eccentric myocardial hypertrophy – and DCM
or mild forms of HCM can be difficult. In fact, MRI and especially delayed enhancement
imaging may be particularly helpful in making that distinction.
As expected, ventricular volumes and functional parameters as assessed in our cohort
are increased for the left and right ventricular EDV, ESV and SV as well as MM in
highly-trained athletes as opposed to a non-athlete population [6]
[7]
[8]
[24]
[25]
[26]. The remodeling indexes were within normal ranges [8], which is consistent with eccentric hypertrophy. Of note, the remodeling index is
reduced in cases of isolated cavity dilatation and increased in cases of concentric
LV hypertrophy, which is pathognomonic for HCM [19]. Furthermore, the thickness of the interventricular septum was within normal range
and there was no asymmetric thickening of the myocardial wall or typical delayed enhancement
pattern indicative of HCM [27]. This suggests that the enlargement of the ventricles and the eccentric hypertrophy
is a function of physiological changes caused by endurance training. In this context,
Petersen et al. [10] showed that physiological LV hypertrophy in athletes can reliably be distinguished
from pathological LV hypertrophy such as in HCM. However, the diagnosis of mild forms
of HCM is still challenging. Therefore, athletes with a positive family history of
HCM, which often shows an autosomal dominant inheritance, should be closely monitored.
The second most common cardiovascular cause of SCD in highly trained athletes is a
coronary anomaly [18]. In our study we were able to identify one athlete suffering from the most frequent
[28] but benign variant of coronary anomaly, notably a circumflex artery originating
from the right sinus ([Fig. 2]). Another athlete showed an RCA originating from the left corner of the right sinus
which is formally not considered as a coronary anomaly but might be affected during
exercise due to the long course of the RCA between the aorta and pulmonary trunk ([Fig. 3]). However, both athletes had no signs of myocardial ischemia during exercise testing.
Also a perfusion defect of the myocardium in an additionally performed adenosine-induced
stress perfusion MRI was ruled out in the athlete with the abnormal course of the
circumflex artery.
Myocarditis is known to be another common etiology for SCD in young athletes. We found
disseminated and intramural myocardial hyperenhancement in two cases. While both athletes
denied having a history of cardiovascular disease, this pattern is characteristic
of a non-ischemic type and indicates remote myocarditis [19] ([Fig. 5]).
As the typical patterns of hyperenhancement in acute myocarditis may decrease during
healing and can be almost invisible after recovery [19], false-negative examinations cannot be excluded. With this problem in mind, we identified
a restrained, non-ischemic enhancement in a further three athletes ([Fig. 7]). However, as these observations could not be confirmed in a second plane and none
of these athletes showed wall motion abnormalities, the findings were judged to be
non-significant. The follow-up MRI examinations performed in the athlete with Epstein-Barr
infection revealed complete recovery of the pericardial effusion and no ventricular
function impairment.
 Fig. 7 Delayed enhancement imaging of a 36-year-old runner with a training load of 20 hours
per week shows disseminated and intramural myocardial hyperenhancement of the lateral
wall (arrows). These findings could not be confirmed in a second plane and were therefore
judged to be non-significant.
Fig. 7 Delayed enhancement imaging of a 36-year-old runner with a training load of 20 hours
per week shows disseminated and intramural myocardial hyperenhancement of the lateral
wall (arrows). These findings could not be confirmed in a second plane and were therefore
judged to be non-significant.
Abb. 7 In der Delayed-Enhancement-Bildgebung eines 36-jährigen Läufers mit einem Trainingspensum
von 20 Stunden pro Woche fanden sich disseminierte, intramyokardiale Signalalterationen
im Bereich der lateralen Wandsegmente (Pfeile), welche sich jedoch nicht zuverlässig
in einer 2. Ebene bestätigen ließen und somit als nicht-signifikant eingestuft wurden.
Prognostic significance of abnormal MRI findings in athletes
Although the presence of delayed enhancement has prognostic significance in the context
of cardiomyopathy [29] and viral myocarditis [30], it remains unclear whether the concept may be transferred to asymptomatic athletes
with delayed enhancement of non-ischemic origin. More than two years after the MRI,
both athletes are still performing their activity (mountain biking) without any symptoms.
Holter-ECG was performed in one of these athletes twice (the other athlete refused
additional testing) and no relevant heart rhythm disorders could be detected.
The relevance of coronary anomalies in asymptomatic persons is still under debate.
Coronary anomalies are disproportionately common in young athletes suffering from
SCD. However, the athlete in our study was 46-years-old and had been performing high-intensity
training for several years. Whether this athlete has a higher risk for SCD even in
the absence of symptoms like fainting or proven myocardial ischemia remains to be
seen. Ultimately, none of the above-mentioned athletes was restricted from sports
competition.
Study Limitations
Certainly, this study has some major limitations. A control collective consistent
of non-athletes was not examined and the quantitative analyses of the RV were performed
using short axis slices. No additional axial slices were acquired. Moreover, a work-up
(adenosine-stress MRI, Holter-ECG, repeated MRI) was only performed in the case of
pathological findings. Thus, it remains unclear whether athletes with an initially
unremarkable MRI would present abnormal findings during further examinations.
Conclusion
Routine implementation of CMR imaging in the context of pre-participation screening
of highly-trained athletes revealed abnormal findings in more than 5 percent of all
athletes and is a useful tool in the detection of cardiovascular disease. However,
the prognostic significance of these findings remains unclear. Thus, cardiac MRI cannot
be recommended as a routine examination in the care of athletes.





