

Subscribe to RSS
DOI: 10.1055/s-0033-1361940
Development of a Tool to Identify Patients' Preference for Vitamin K Antagonist or Direct Oral Anticoagulant Therapy
Authors
Abstract
Direct oral anticoagulants (DOACs) were developed for the treatment of thromboembolic diseases to overcome limitations of vitamin K antagonists (VKA). International guidelines on atrial fibrillation acknowledge patients' for antiembolic therapy with VKA or DOAC as relevant decision criteria. The objective assessment of patients' preference social interactions and psychological factors are hard to measure albeit representing important contributors. After a series of structured interviews and pilot studies assessing the preparedness to use DOAC as an anticoagulant and the motivation of patients to participate in clinical studies with DOAC, seven items were identified from several questionnaires by regression analysis. Those items were seen the best to describe the willingness to change anticoagulation from VKA to DOAC. By their use, we aim to develop a tool for the objective identification of the patients' preferences for VKA or for DOAC to increase adherence to therapy and to reduce anticoagulant undertreatment. German-speaking patients were asked to fill out a questionnaire consisting of biographic data and the seven selected items, and 180 patients completed the questionnaire so far. Of these, 90 patients were on treatment with VKA (group 1), 57 patients changed anticoagulation from VKA to DOAC (group 2), 29 patients were DOAC naive patients (group 3), and 4 patients changed from DOAC to VKA (group 4). Overall, 94 patients received VKA, 29 patients received dabigatran, 50 patients received rivaroxaban, and 7 patients received apixaban as an anticoagulant. Eight patients were younger than 40 years, 35 patients were aged between 40 and 59 years, 53 patients were aged between 60 and 70 years, and 84 patients were aged older than 70 years. Indication for anticoagulation were atrial fibrillation (n = 106), pulmonary embolism (n = 24), deep vein thrombosis (n = 40), artificial heart valve replacement (n = 8), or other diseases (n = 2). Based on the results of the analysis, a score will be suggested to identify the preference of patients for anticoagulation with VKA or DOAC. This tool may be useful for practitioners and health-care professionals to support patient adherence to therapy, and thereby increase treatment effectiveness.
Keywords
anticoagulation - preference - adherence - warfarin - dabigatran - rivaroxaban - apixaban - atrial fibrillationPatients with nonvalvular atrial fibrillation (AF) are exposed to an increased risk for ischemic stroke and systemic embolism. Morbidity and mortality following stroke associated with AF are higher than in patients who suffer thromboembolic strokes in the absence of AF.[1] [2] [3] Therefore, AF is one of the most frequent reasons for therapeutic oral anticoagulant therapy with vitamin K antagonists (VKAs) in everyday practice. For decades, VKA used to be the state-of-the-art anticoagulant to prevent thromboembolic events in patients with AF and additional risk factors.[4] The major adverse effects are severe bleeding complications including intracranial hemorrhage.[5] [6] VKA usage requires frequent dose adjustments according to the international normalized ratio (INR) values between 2 and 3 to optimize the time in therapeutic range.[7] Other downsides of VKA are interactions with food and many drugs, severe bleeding complications (intracranial and extracranial), and other severe adverse effects such as coumarin-induced hepatitis. The slow onset and offset of action of VKAs necessitates the overlapping administration of heparins and low-molecular-weight heparins during the induction of anticoagulation as well as during surgical interventions.[8] Because of the limitations of therapy with VKA, patients are at risk for bleeding complications or for other reasons may not be treated with VKA or receive less effective medications, such as aspirin or even no prophylaxis.[9]
New anticoagulants (direct oral anticoagulants [DOAC]) were developed to overcome these drawbacks of conventional anticoagulant therapy and thereby help improve patient care. Advantages of novel synthetic DOACs inhibiting specifically only one activated coagulation factor include rapid onset and offset of action, lack of need for routine monitoring and dose adjustment, lack or infrequent food and drug interactions, and overall better efficacy and safety than the conventional anticoagulants when used appropriately. The rapid onset and offset of action may eliminate the need of bridging with subcutaneous heparins as is required during anticoagulation with VKA.[10] [11] [12]
For over 50 years of anticoagulation with VKA, patients did not have any choice for a different effective oral anticoagulant. This has now changed because of the development of DOAC, and now patients have the option to choose between VKA and DOAC. To qualify for this important decision-making process, patients and practitioners have to be well informed about advantages and limitations of available oral anticoagulants. Up to now, practitioners have largely acted as peers for patients which drug to choose for treatment.[13] [14] [15] Preferences of patients for therapy with conventional VKA or for a DOAC may become increasingly important and this is mentioned in the guidelines of the American College of Cardiology Foundation (ACCF), American Heart Association (AHA), Heart Rhythm Society (HRS),[16] European Society of Cardiology (ESC),[17] and American College of Chest Physicians (ACCP).[18] The understanding of the complex differences between oral anticoagulants by patients as laypersons is limited for many reasons, and seems similarly restricted as in patients with insulin-dependent diabetes.[14] Some investigations have addressed this and correlated the patients' preferences with the willingness to pay for DOAC,[19] the preparedness of patients to use DOAC instead of VKA for anticoagulation,[20] [21] and the motivation of patients to participate in clinical studies with DOAC[22] using questionnaires that were developed according to published techniques.[23] The patient preferences regarding treatment of human immunodeficiency virus (HIV)/AIDS identified a high impact of quality of life on patients' preferences for the selection of treatments was identified.[24] Furthermore, a tool was described to improve the adherence to HIV treatment based on psychological and environmental factors.[25] Involving patients in discussions about their treatment could lead to improved health through better adherence to chosen options, reduced practice variation about preference-sensitive options, and improved care in general.[26] So far, the willingness to change anticoagulation from VKA to dabigatran[21] has been reported so far but not the preference of patients to choose between VKA and other DOAC. As a consequence, no tool is available to scientifically describe the preference.[18] [27] [28] Earlier publications address the impact of patients' view on therapeutic options in anticoagulation in the pre-DOAC era or represent a personal view in the new era.[29] [30] [31] On this background, we aim to develop a tool to identify the preference of patients for a VKA or DOAC thereby improving patient's adherence to therapy as an essential prerequisite for success.
Development of the Questionnaire
Phase 1: Focus Groups for Concept Elicitation and Item Generation
The goal of this phase of development of the questionnaire was to elicit patients' experiences with oral anticoagulation for the treatment of AF and venous thromboembolism (VTE).[23] This phase was performed in a German focus group of patients on treatment with VKA using a structured discussion guide. Patients were recruited from the 4th Department of Medicine of the Medical Faculty Mannheim. The inclusion and exclusion criteria, ethics and informed consent procedure are described in the section “Study Design.” Patients were invited to share their recollections, opinions, and wishes for anticoagulation, followed by discussions aimed at patients undergoing treatment with oral anticoagulation.
A set of items was developed that reflected the anticoagulation-related concerns of the patient. All major areas of comments that had been identified by patients were represented in the initial set of questions. A self-developed questionnaire was thus developed. It was then reviewed by an expert psychiatrist (L.F.) and modified accordingly. The questionnaire was divided into two modules: a biographic module and an anticoagulation module. The latter investigates the personal experience of patients with anticoagulation and wishes for an optimal anticoagulant drug.[32]
In addition, patients' personality traits, fears related to a new medication, and self-assessment of the general health status were investigated by the validated personality inventory questionnaire Freiburger Persönlichkeitsinventar (FPI-R, Hogrefe-Verlag GmbH & Co.KG, Goettingen, 2001, Germany),[33] State-Trait Anxiety Inventory (STAI, Consulting Psychologists Press. Inc., Palo Alto, Calif., Beltz Test GmbH, Goettingen, Germany; 1970),[34] [35] [36] [37] and a 12-item short-form health survey questionnaire (SF-12; Hogrefe-Verlag GmbH & Co. KG Goettingen, Germany; 1998), summarizing two scales describing mental and physical well-being components.[38] [39] [40]
Phase 2: Applicability and Acceptability of the Questionnaire
A total of 110 patients, on stable treatment with VKA for at least 3 months, completed the four questionnaires (FPI-R, STAI, SF-12, and the self-developed questionnaire).[32] Patients replied to all questions indicating an adequate applicability and acceptability. Thus, rephrasing of the questions of our self-developed questionnaire was not required for further investigations.[23] [41]
Phase 3: Regression Analysis and Reduction of Items
In the meantime, DOACs were approved for prevention of embolism in nonvalvular atrial fibrillation. The wishes and fears for anticoagulation were discussed in this context with another focus group of patients in a structured interview under the guidance of an expert (J.H.). It is important to note that the price for DOACs is covered by health insurance companies in German-speaking countries. In this phase of development of the questionnaire, patients were investigated as to their disposition to change anticoagulant therapy from VKA to DOAC. Logistic regression analysis identified “extraversion” on the FPI-R being positively related to the willingness to change the medication. In addition, the following items of the self-developed questionnaire were identified: past thoughts regarding alternatives for anticoagulation, hope for a better quality of life, difficulty to adjust therapy based on the prothrombin time, lack of need for monitoring for dose adjustment of the anticoagulant drug, importance of the opinion of the practitioner on which anticoagulant to use, and skepticism to change drug for therapy.[20]
Phase 4: Reliability of the Seven Items
To analyze the reliability of the results, 85 of 110 patients replied for a second time to the seven items. The receiver-operative curve (ROC) confirmed the reliability of the seven items with a probability of 98%.[20] This high reliability supported the use of these seven items together with biographic data in patients' transition from VKA to DOAC ([Table 1]).
Abbreviations: DOAC, direct oral anticoagulant; VKA, vitamin K antagonist.
Study Design
This is a prospective, controlled, multicenter, case-control study in patients with an indication for anticoagulant therapy. The Ethics Committee II of the Medical Faculty Mannheim, Heidelberg University approved the study protocol. For the paper version, patients had to give written informed consent. In the online version patients accepted participation by clicking the button “participate” implying to have read and accepted the informed consent in an accessible PDF document.
Patients: Four groups of patients are included in the study: patients on treatment with VKA (group 1), patients who switched anticoagulant therapy from VKA to DOAC (group 2), DOAC naive patients without personal experience with therapy of VKA (group 3), and patients who changed therapy from DOAC to VKA (group 4).
Inclusion criteria: The inclusion criteria were confirmed diagnosis of AF, deep vein thrombosis, pulmonary embolism or artificial heart valve replacement, oral anticoagulant therapy, aged 18 years and older, and the ability to understand German language.
Exclusion criteria: The exclusion criteria included severe diseases with impairment of cognitive function and age < 18 years.
Project overview: Patients undergoing treatment with VKA or DOAC can participate in the study. The projected inclusion period was until the end of 2013. The questionnaire was divided into part one, referring to biographic data, and part two, referring to the seven questions ([Table 1]). The aim of the project is to support a structured and justifiable decision on whether a patient prefers to continue with the current anticoagulant or to switch to the other group of anticoagulants based on the results of the seven items ([Fig. 1]).

Methods
Generation, Documentation, and Processing of Data
Network
A network was organized for inclusion of patients into the project. A flyer was designed for distribution and publication in scientific and other journals. General practitioners, specialized hospital and outpatients care units, and blood coagulation centers agreed to participate. Advertisements were made at presentations on congresses, published in local and regional German newspapers in print, or on Internet forms and homepages of Gesellschaft für Thrombose und Haemostaseforschung with a link to www.blutverduennung.uni-hd.de.[42]
Construction of the Questionnaire
The targets for appropriate construction of questions consist of (1) easy understanding, (2) simple feasibility, (3) short-time solution, (4) low material and paper consumption, (5) easy readability, and (6) low frequency of random solutions.[43] For the answers to the seven items, we evaluated different scale formats in preliminary experiments (not shown) and finally chose a Likert scale for each of the items. Patients have to decide by agreeing or disagreeing with the statements of the items by choosing an integer between 0 and 10. This scale can be easily understood, offers graduated response choices depending on the intensity of agreement, and is readily interpretable.[44] [45] The time to answer to the whole questionnaire including biographic data ranges from 5 to 10 minutes.
Processing of Data
The questionnaire on Internet was created using the Web-based software evaluation system (EvaSys, Electric Paper Evaluationssysteme GmbH, Lueneburg, Germany). EvaSys is an Internet technology-based system that can be used in particular scientific evaluations of educational events and seminars. The evaluation process with EvaSys is visualized in five successive phases. First, the design of the questionnaire is created. Second, the type of answers from various formats as single or multiple choice, open question, or scale is selected. The scales can be classified as nominal scale, ordinal scale, interval scale, and ratio scale ([Table 2]). EvaSys generates a PDF file or an HTML file including patients' data and simple corresponding statistical measures such as frequencies or mean values. To ensure that only qualifying persons use the questionnaire, EvaSys individual transaction numbers (TANs) have to be created. On agreement of a person to participate in questionnaire, the TANs will be sent with a link from the homepage to the e-mail address of the participant. In the third phase, the data of the completed questionnaires are collected by EvaSys and automatically transferred into an Excel database spreadsheet (Microsoft, Redmond, WA). In the fourth phase, the raw data are exported for analysis in statistical programs such as SPSS (IBM Corporation, Armonk, NY), SAS (SAS Institute Inc., Cary, NC), or SPHINX (Sphinx Technology, Inc., Brooklyn, NY). The data analysis in our study will be performed with SAS statistical software release 9.3. Documented data in Excel fundamentally simplify the work for SAS programmers because it can import the data into SAS for evaluation. The fifth phase allows a quality management and process optimization of the system.
Statistical Analysis
Each question will be analyzed with a different statistical test depending on its special form. To compare the four groups regarding binary data (i.e., patients' gender or diseases), the Chi-square test or Fisher exact tests will be used, as appropriate. For quantitative data, which are approximately normally distributed (i.e., patients' age), one-way ANOVA (analysis of variance) will be performed. The Kruskal–Wallis test will be applied for ordinally scaled (i.e., the seven items) or skewed data. Comparisons between the two groups will be done by the two sample t-test or Mann-Whitney U test. Furthermore, for each patient, a multiple logistic regression analysis model will be performed to assess patient's preference expressed by the probability to perform anticoagulation with VKA or DOAC. This has already been done in a previous study.[20]
Preliminary Results
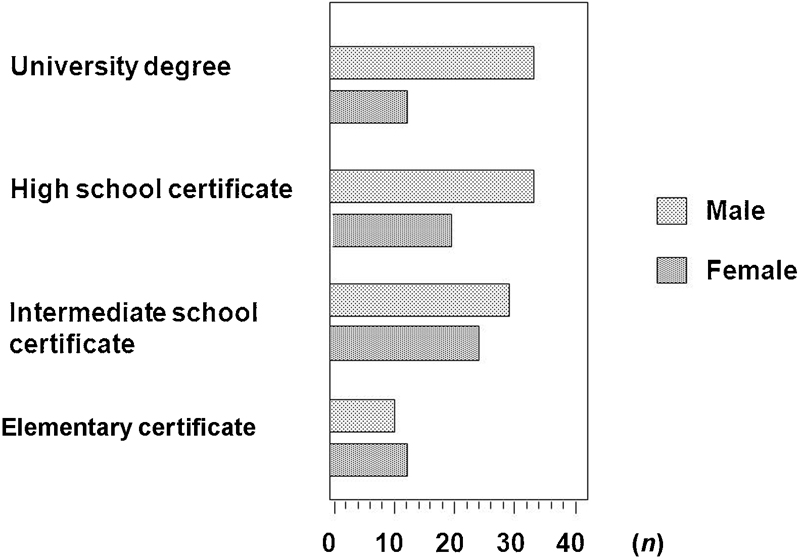
From February 1, 2013, to August 1, 2013, a total of 180 patients (109 males, age [mean ± standard deviation or SD]: 66.9 ± 10.9 y; 71 females, age [mean ± SD]: 63.2 ± 15.3 y) participated in the study and completed the questionnaire. The distribution of age in decades and according to gender is shown in [Fig. 2]. A total of 60 patients have answered the questions on paper format and 120 patients on the online format. The school degree of education of patients is shown in [Fig. 3]. Overall, 54 patients have elementary school certificates, 55 patients have intermediate school certificate, 24 patients have high school certificates, and 47 patients have university degrees. The indication for anticoagulation was mainly AF, followed by deep vein thrombosis, pulmonary embolism, and artificial heart valve replacement ([Fig. 4]).


A total of 90 patients were on treatment with VKA (group 1), 57 patients changed anticoagulation from VKA to one of the DOAC (group 2), 29 patients were DOAC naive patients and placed straight onto DOAC (group 3), and 4 patients changed therapy from DOAC to VKA (group 4) ([Fig. 5]). Patients of group 4 switched from DOAC to VKA due to fear of adverse effects on DOAC (n = 3) and one patient reported hair loss after 9 months of treatment. Of the 94 patients of group 1 and 4, 37 performed self-management of anticoagulation and 57 performed INR determinations at the general practitioner. Differences between genders cannot be identified ([Fig. 6]). The distribution of the DOAC dabigatran (all doses), rivaroxaban (all doses), and apixaban (2 × 5 mg twice daily) for anticoagulation is given in [Fig. 7].



Discussion
The aim of the present, still ongoing study is to develop a tool for practitioners to identify the preference of patients for a VKA or a DOAC as anticoagulant to improve adherence of patients to therapy. Many studies reported that the quality of clinical communication is related to positive health outcomes. Communication between patient and physician helps improve and resolve the problem of choosing the type of anticoagulant therapy.[46] In particular lack of physicians' time may be one of many reasons why the patients' preferences for a specific anticoagulant are currently being overlooked. With this study, we aim to find a tool for the physician and the health-care system that helps patients to choose the preferred type of oral anticoagulant.
The proportion of patients using VKA as an anticoagulant due to a specific reason such as fear of increased bleeding risk with a DOAC may influence the patients' preference. If a patient would prefer DOAC based on the results of the questionnaire, the practitioner may decide in favor of DOAC for a plausible reason justifying the higher price. On the contrary, patients may prefer anticoagulation with a VKA based on the results of the questionnaire facilitating the choice of this type of the anticoagulant for an individual patient.
Currently the ACCF/AHA/HRS,[16] ESC,[17] and ACCP guidelines[18] include the preferences of patients in their recommendations to choose VKA or DOAC for oral anticoagulation of patients with AF. Several reports are available on how to improve the adherence of a patient to anticoagulant therapy in patients with AF. It was recently reported if physicians' and patients' perspectives can be identified by answering several questions: “Do patients' and clinicians preferences explain the utilization of warfarin to prevent strokes associated with AF?,” “To what extent do patients' and clinicians' treatment preferences differ?,” and “What factors explain any differences that exist in treatment preferences between patients and clinicians?[47] Some questionnaires were developed without using results of structured interviews with patients regarding the price patients would be willing to pay for the treatment with a DOAC.[19] [48] In this report, a questionnaire was developed using published methodologies based on structured interview with focus groups with the treatment in question.[32] Thus, we have developed a set of approximately 28 questions related to therapy with VKA. In addition, standardized questionnaires regarding personality traits, anxiety, and self-assessment of health status were included. Logistic regression analysis identified seven items out of over 200 items regarding the willingness to switch anticoagulation from VKA to DOAC.[20] With this study, we want to identify the validity of seven items for patients who have really changed anticoagulation from VKA to DOAC. Thereby, the preference of patients for a specific type of an oral anticoagulant could be identified analyzing the differences between the four groups of patients.
An overview summarized 16 studies focused on patients with AF regarding the burden of antithrombotic treatment using different scales to identify the acceptance of thrombotic or bleeding risk on VKA.[18] Around 20% were willing to accept 35 additional bleeds on VKA for 3% absolute risk reduction of stroke. For these 20%, the disutility associated with one stroke was equal to the disutility associated with 11 bleeding episodes.[47] Patients with AF placed more value on the avoidance of stroke and less value on the occurrence of bleeding in contrast to physicians who placed more value on the occurrence of bleeding during treatment with warfarin.[13] This may relate to the concept of loss aversion, which refers to the tendency for individuals to prefer avoiding loss in favor of gaining benefits.[49]
Methods used to convey information about risks and benefits of therapy may significantly affect patient-reported preferences.[50] Also, previous exposure to a therapy was associated with a preference for continuing the same treatment.[51] [52] Cognitive dissonance occurs when participants tend to collect additional information to ensure that it is consistent with their previous decision.[53] To reduce cognitive dissonance, participants may be inclined to continue their treatment, despite new information suggesting a suboptimal choice. Patients who do not want to believe that they have been taking the worse treatment may interpret the evidence presented in a way that it is consistent with their previous choice.[18] These considerations can be translated to prefer anticoagulation with a VKA or a DOAC. This study should help overcome such cognitive dissonances for patients as well as practitioners.
Some limitations of the study should be considered. At present the investigations can be performed only with German-speaking persons. Translation to other languages encounters cross-cultural differences. International guidelines were developed to adapt questionnaires to other countries and cultures.[54] The opinion of a patient about acceptable risks for a thromboembolic or a bleeding event and economical aspects are not included in the questionnaire. In preliminary studies, these aspects were included and logistic regression analysis did not rank the results high enough to be included into the final present questionnaire.[32] The higher daily costs for DOACs compared with warfarin are not included into the questionnaire because in Germany they are covered by the insurance companies. This is different in many other countries and has to be respected when the questionnaire will be implemented in other countries. Patients unwilling to participate in the study may prefer more frequently a conventional over a new DOAC. The noninclusion of these patients may cause a bias. Convincing as many patients as possible to take part in our study may counteract this. However, the problem of not participating is inherent in most studies and cannot be eliminated completely.
In conclusion, this investigation is undertaken to develop a tool for the health-care system to maximize the adherence of patients to anticoagulant therapy by identification of their preference for a specific type of an oral anticoagulant. Using this tool, patients will be actively involved in the decision to perform anticoagulation with VKA or DOAC. As a consequence of implementing the tool into patient care, undertreatment in anticoagulation should be reduced.
Conflict of Interest
The authors do not declare any conflict of interest for the present investigation or preparation of the article.
Acknowledgments
The authors gratefully acknowledge the cooperation of Drs. Philip Wild, Jürgen Prochaska, Jan Beyer-Westerndorf, Jürgen Koscielny, Heinz Völler, Mrs. Antje Hagedorn, and Inge Träger.
-
References
- 1 Roskell NS, Lip GY, Noack H, Clemens A, Plumb JM. Treatments for stroke prevention in atrial fibrillation: a network meta-analysis and indirect comparisons versus dabigatran etexilate. Thromb Haemost 2010; 104 (6) 1106-1115
- 2 Lip GY. Stroke in atrial fibrillation: epidemiology and thromboprophylaxis. J Thromb Haemost 2011; 9 (Suppl. 01) 344-351
- 3 Falck-Ytter Y, Francis CW, Johanson NA , et al; American College of Chest Physicians. Prevention of VTE in orthopedic surgery patients: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines. Chest 2012; 141 (2, Suppl) e278S-e325S
- 4 Moser M, Bode C. [Anticoagulation in atrial fibrillation: a new era has begun]. Hamostaseologie 2012; 32 (1) 37-39
- 5 Schulman S, Beyth RJ, Kearon C, Levine MN ; American College of Chest Physicians. Hemorrhagic complications of anticoagulant and thrombolytic treatment: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines (8th Edition). Chest 2008; 133 (6, Suppl) 257S-298S
- 6 Lip GY, Andreotti F, Fauchier L , et al; European Heart Rhythm Association. Bleeding risk assessment and management in atrial fibrillation patients. Executive Summary of a Position Document from the European Heart Rhythm Association [EHRA], endorsed by the European Society of Cardiology [ESC] Working Group on Thrombosis. Thromb Haemost 2011; 106 (6) 997-1011
- 7 Ansell J, Hirsh J, Hylek E, Jacobson A, Crowther M, Palareti G ; American College of Chest Physicians. Pharmacology and management of the vitamin K antagonists: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines (8th Edition). Chest 2008; 133 (6, Suppl) 160S-198S
- 8 Harenberg J, Marx S, Krejczy M, Wehling M. New anticoagulants - promising and failed developments. Br J Pharmacol 2012; 165 (2) 363-372
- 9 Ogilvie IM, Newton N, Welner SA, Cowell W, Lip GY. Underuse of oral anticoagulants in atrial fibrillation: a systematic review. Am J Med 2010; 123 (7) 638-645 e4
- 10 Bates SM, Greer IA, Middeldorp S, Veenstra DL, Prabulos AM, Vandvik PO ; American College of Chest Physicians. VTE, thrombophilia, antithrombotic therapy, and pregnancy: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines. Chest 2012; 141 (2, Suppl) e691S-e736S
- 11 Hirsh J, O'Donnell M, Eikelboom JW. Beyond unfractionated heparin and warfarin: current and future advances. Circulation 2007; 116 (5) 552-560
- 12 Eikelboom JW, Weitz JI. A replacement for warfarin: the search continues. Circulation 2007; 116 (2) 131-133
- 13 Devereaux PJ, Anderson DR, Gardner MJ , et al. Differences between perspectives of physicians and patients on anticoagulation in patients with atrial fibrillation: observational study. BMJ 2001; 323 (7323) 1218-1222
- 14 Mühlbacher AC, Stoll M, Mahlich J, Nübling M. Patient preferences for HIV/AIDS therapy - a discrete choice experiment. Health Econ Rev 2013; 3 (1) 14
- 15 Holbrook A, Schulman S, Witt DM , et al; American College of Chest Physicians. Evidence-based management of anticoagulant therapy: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines. Chest 2012; 141 (2, Suppl) e152S-e184S
- 16 Anderson JL, Halperin JL, Albert NM , et al. Management of patients with atrial fibrillation (compilation of 2006 ACCF/AHA/ESC and 2011 ACCF/AHA/HRS recommendations): a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol 2013; 61 (18) 1935-1944
- 17 Camm AJ, Lip GY, De Caterina R , et al; ESC Committee for Practice Guidelines-CPG; Document Reviewers. 2012 focused update of the ESC Guidelines for the management of atrial fibrillation: an update of the 2010 ESC Guidelines for the management of atrial fibrillation—developed with the special contribution of the European Heart Rhythm Association. Europace 2012; 14 (10) 1385-1413
- 18 MacLean S, Mulla S, Akl EA , et al; American College of Chest Physicians. Patient values and preferences in decision making for antithrombotic therapy: a systematic review: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines. Chest 2012; 141 (2, Suppl) e1S-e23S
- 19 Moia M, Mantovani LG, Carpenedo M , et al. Patient preferences and willingness to pay for different options of anticoagulant therapy. Intern Emerg Med 2013; 8 (3) 237-243
- 20 Harenberg J, Marx S, Abou-Ayash N , et al. Which patients would be willing to change anticoagulation from vitamin-K antagonists to a new oral anticoagulant?. Haemostaseologie 2012; 33 (1) ED10-4
- 21 Elewa HF, Deremer CE, Keller K, Gujral J, Joshua TV. Patients satisfaction with warfarin and willingness to switch to dabigatran: a patient survey. J Thromb Thrombolysis 2013;
- 22 Zolfaghari S, Harenberg J, Knäble H , et al. Investigation on motivation of patients to participate in clinical studies with new oral anticoagulants. Haemostaseologie 2013; 34 (1) P5-19
- 23 Crawford B, Stanford RH, Wong AY, Dalal AA, Bayliss MS. Development of a questionnaire to assess experience and preference of intranasal corticosteroids in patients with allergic rhinitis. Patient Relat Outcome Meas 2011; 2: 119-126
- 24 Klausmann G, Hramiak I, Qvist M, Mikkelsen KH, Guo X. Evaluation of preference for a novel durable insulin pen with memory function among patients with diabetes and health care professionals. Patient Prefer Adherence 2013; 7: 285-292
- 25 Nelsen A, Gupta S, Trautner BW , et al. Intention to adhere to HIV treatment: a patient-centred predictor of antiretroviral adherence. HIV Med 2013; 14 (8) 472-480
- 26 Politi MC, Wolin KY, Légaré F. Implementing clinical practice guidelines about health promotion and disease prevention through shared decision making. J Gen Intern Med 2013; 28 (6) 838-844
- 27 Sudlow M, Thomson R, Kenny RA, Rodgers H. A community survey of patients with atrial fibrillation: associated disabilities and treatment preferences. Br J Gen Pract 1998; 48 (436) 1775-1778
- 28 Thomson R, Parkin D, Eccles M, Sudlow M, Robinson A. Decision analysis and guidelines for anticoagulant therapy to prevent stroke in patients with atrial fibrillation. Lancet 2000; 355 (9208) 956-962
- 29 Protheroe J, Fahey T, Montgomery AA, Peters TJ. The impact of patients' preferences on the treatment of atrial fibrillation: observational study of patient based decision analysis. BMJ 2000; 320 (7246) 1380-1384
- 30 Man-Son-Hing M, Laupacis A, O'Connor AM, Coyle D, Berquist R, McAlister F. Patient preference-based treatment thresholds and recommendations: a comparison of decision-analytic modeling with the probability-tradeoff technique. Med Decis Making 2000; 20 (4) 394-403
- 31 Schulman S, Crowther MA. How I treat with anticoagulants in 2012: new and old anticoagulants, and when and how to switch. Blood 2012; 119 (13) 3016-3023
- 32 Harenberg J, Felten M, Weiss C, Frölich L. The stability of the INR, the fear of thrombotic and bleeding complications are influenced by personality traits of patients on stable oral anticoagulant therapy. Haemostaseologie 2010; 30 (1) P02-P10
- 33 Franke GH. Possibilities of computer-assisted administration of the revised Freiburg Personality Inventory. 2 experimental studies[in German]. Z Exp Psychol 1997; 44 (2) 332-356
- 34 Forgays DG, Forgays DK, Spielberger CD. Factor structure of the State-Trait Anger Expression Inventory. J Pers Assess 1997; 69 (3) 497-507
- 35 Fisher PL, Durham RC. Recovery rates in generalized anxiety disorder following psychological therapy: an analysis of clinically significant change in the STAI-T across outcome studies since 1990. Psychol Med 1999; 29 (6) 1425-1434
- 36 Sanderson K, Andrews G. The SF-12 in the Australian population: cross-validation of item selection. Aust N Z J Public Health 2002; 26 (4) 343-345
- 37 Verkuil B, Brosschot JF, Thayer JF. Capturing worry in daily life: are trait questionnaires sufficient?. Behav Res Ther 2007; 45 (8) 1835-1844
- 38 Ware Jr J, Kosinski M, Keller SD. A 12-Item Short-Form Health Survey: construction of scales and preliminary tests of reliability and validity. Med Care 1996; 34 (3) 220-233
- 39 Svirtlih N, Pavic S, Terzic D , et al. Reduced quality of life in patients with chronic viral liver disease as assessed by SF12 questionnaire. J Gastrointestin Liver Dis 2008; 17 (4) 405-409
- 40 Völler H, Taborski U, Dovifat C , et al. ProTime self-management yielding improvement of fluency and quality of life. Thromb Haemost 2007; 98 (4) 889-895
- 41 Crawford B, Stanford RH, Wong AY, Dalal AA, Bayliss MS. Psychometric validation of the experience with allergic rhinitis nasal spray questionnaire. Patient Relat Outcome Meas 2011; 2: 127-133
- 42 Smetana GW, Davis RB, Phillips RS. Factors that influence patient response to requests to change to a unified restrictive formulary. J Gen Intern Med 2004; 19 (12) 1212-1219
- 43 Mussbrugger H, Kelava A. Testtheorie und Fragebogenkonstruktion. Berlin, Heidelberg. New York, NY: Springer Verlag; 2008: 409
- 44 Rogers MP, Orav J, Black PM. The use of a simple Likert scale to measure quality of life in brain tumor patients. J Neurooncol 2001; 55 (2) 121-131
- 45 Makowski CT, Jennings DL, Nemerovski CW, Szandzik EG, Kalus JS. The impact of pharmacist-directed patient education and anticoagulant care coordination on patient satisfaction. Ann Pharmacother 2013; 47 (6) 805-810
- 46 Casula M, Tragni E, Catapano AL. Adherence to lipid-lowering treatment: the patient perspective. Patient Prefer Adherence 2012; 6: 805-814
- 47 Alonso-Coello P, Montori VM, Solà I , et al. Values and preferences in oral anticoagulation in patients with atrial fibrillation, physicians' and patients' perspectives: protocol for a two-phase study. BMC Health Serv Res 2008; 8: 221
- 48 González-Rojas N, Giménez E, Fernández MA , et al. Preferences for oral anticoagulant treatment in the medium and long term prevention of stroke in non valvular atrial fibrillation [in Spanish]. Rev Neurol 2012; 55 (1) 11-19
- 49 Tversky A, Kahneman D. The framing of decisions and the psychology of choice. Science 1981; 211 (4481) 453-458
- 50 Bergus GR, Levin IP, Elstein AS. Presenting risks and benefits to patients. J Gen Intern Med 2002; 17 (8) 612-617
- 51 Maxwell GL, Synan I, Hayes RP, Clarke-Pearson DL. Preference and compliance in postoperative thromboembolism prophylaxis among gynecologic oncology patients. Obstet Gynecol 2002; 100 (3) 451-455
- 52 Man-Son-Hing M, Laupacis A, O'Connor AM , et al. A patient decision aid regarding antithrombotic therapy for stroke prevention in atrial fibrillation: a randomized controlled trial. JAMA 1999; 282 (8) 737-743
- 53 Draycott S, Dabbs A. Cognitive dissonance. 1: An overview of the literature and its integration into theory and practice in clinical psychology. Br J Clin Psychol 1998; 37 (Pt 3) 341-353
- 54 Beaton DE, Bombardier C, Guillemin F, Ferraz MB. Guidelines for the process of cross-cultural adaptation of self-report measures. Spine 2000; 25 (24) 3186-3191
Address for correspondence
-
References
- 1 Roskell NS, Lip GY, Noack H, Clemens A, Plumb JM. Treatments for stroke prevention in atrial fibrillation: a network meta-analysis and indirect comparisons versus dabigatran etexilate. Thromb Haemost 2010; 104 (6) 1106-1115
- 2 Lip GY. Stroke in atrial fibrillation: epidemiology and thromboprophylaxis. J Thromb Haemost 2011; 9 (Suppl. 01) 344-351
- 3 Falck-Ytter Y, Francis CW, Johanson NA , et al; American College of Chest Physicians. Prevention of VTE in orthopedic surgery patients: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines. Chest 2012; 141 (2, Suppl) e278S-e325S
- 4 Moser M, Bode C. [Anticoagulation in atrial fibrillation: a new era has begun]. Hamostaseologie 2012; 32 (1) 37-39
- 5 Schulman S, Beyth RJ, Kearon C, Levine MN ; American College of Chest Physicians. Hemorrhagic complications of anticoagulant and thrombolytic treatment: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines (8th Edition). Chest 2008; 133 (6, Suppl) 257S-298S
- 6 Lip GY, Andreotti F, Fauchier L , et al; European Heart Rhythm Association. Bleeding risk assessment and management in atrial fibrillation patients. Executive Summary of a Position Document from the European Heart Rhythm Association [EHRA], endorsed by the European Society of Cardiology [ESC] Working Group on Thrombosis. Thromb Haemost 2011; 106 (6) 997-1011
- 7 Ansell J, Hirsh J, Hylek E, Jacobson A, Crowther M, Palareti G ; American College of Chest Physicians. Pharmacology and management of the vitamin K antagonists: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines (8th Edition). Chest 2008; 133 (6, Suppl) 160S-198S
- 8 Harenberg J, Marx S, Krejczy M, Wehling M. New anticoagulants - promising and failed developments. Br J Pharmacol 2012; 165 (2) 363-372
- 9 Ogilvie IM, Newton N, Welner SA, Cowell W, Lip GY. Underuse of oral anticoagulants in atrial fibrillation: a systematic review. Am J Med 2010; 123 (7) 638-645 e4
- 10 Bates SM, Greer IA, Middeldorp S, Veenstra DL, Prabulos AM, Vandvik PO ; American College of Chest Physicians. VTE, thrombophilia, antithrombotic therapy, and pregnancy: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines. Chest 2012; 141 (2, Suppl) e691S-e736S
- 11 Hirsh J, O'Donnell M, Eikelboom JW. Beyond unfractionated heparin and warfarin: current and future advances. Circulation 2007; 116 (5) 552-560
- 12 Eikelboom JW, Weitz JI. A replacement for warfarin: the search continues. Circulation 2007; 116 (2) 131-133
- 13 Devereaux PJ, Anderson DR, Gardner MJ , et al. Differences between perspectives of physicians and patients on anticoagulation in patients with atrial fibrillation: observational study. BMJ 2001; 323 (7323) 1218-1222
- 14 Mühlbacher AC, Stoll M, Mahlich J, Nübling M. Patient preferences for HIV/AIDS therapy - a discrete choice experiment. Health Econ Rev 2013; 3 (1) 14
- 15 Holbrook A, Schulman S, Witt DM , et al; American College of Chest Physicians. Evidence-based management of anticoagulant therapy: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines. Chest 2012; 141 (2, Suppl) e152S-e184S
- 16 Anderson JL, Halperin JL, Albert NM , et al. Management of patients with atrial fibrillation (compilation of 2006 ACCF/AHA/ESC and 2011 ACCF/AHA/HRS recommendations): a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol 2013; 61 (18) 1935-1944
- 17 Camm AJ, Lip GY, De Caterina R , et al; ESC Committee for Practice Guidelines-CPG; Document Reviewers. 2012 focused update of the ESC Guidelines for the management of atrial fibrillation: an update of the 2010 ESC Guidelines for the management of atrial fibrillation—developed with the special contribution of the European Heart Rhythm Association. Europace 2012; 14 (10) 1385-1413
- 18 MacLean S, Mulla S, Akl EA , et al; American College of Chest Physicians. Patient values and preferences in decision making for antithrombotic therapy: a systematic review: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines. Chest 2012; 141 (2, Suppl) e1S-e23S
- 19 Moia M, Mantovani LG, Carpenedo M , et al. Patient preferences and willingness to pay for different options of anticoagulant therapy. Intern Emerg Med 2013; 8 (3) 237-243
- 20 Harenberg J, Marx S, Abou-Ayash N , et al. Which patients would be willing to change anticoagulation from vitamin-K antagonists to a new oral anticoagulant?. Haemostaseologie 2012; 33 (1) ED10-4
- 21 Elewa HF, Deremer CE, Keller K, Gujral J, Joshua TV. Patients satisfaction with warfarin and willingness to switch to dabigatran: a patient survey. J Thromb Thrombolysis 2013;
- 22 Zolfaghari S, Harenberg J, Knäble H , et al. Investigation on motivation of patients to participate in clinical studies with new oral anticoagulants. Haemostaseologie 2013; 34 (1) P5-19
- 23 Crawford B, Stanford RH, Wong AY, Dalal AA, Bayliss MS. Development of a questionnaire to assess experience and preference of intranasal corticosteroids in patients with allergic rhinitis. Patient Relat Outcome Meas 2011; 2: 119-126
- 24 Klausmann G, Hramiak I, Qvist M, Mikkelsen KH, Guo X. Evaluation of preference for a novel durable insulin pen with memory function among patients with diabetes and health care professionals. Patient Prefer Adherence 2013; 7: 285-292
- 25 Nelsen A, Gupta S, Trautner BW , et al. Intention to adhere to HIV treatment: a patient-centred predictor of antiretroviral adherence. HIV Med 2013; 14 (8) 472-480
- 26 Politi MC, Wolin KY, Légaré F. Implementing clinical practice guidelines about health promotion and disease prevention through shared decision making. J Gen Intern Med 2013; 28 (6) 838-844
- 27 Sudlow M, Thomson R, Kenny RA, Rodgers H. A community survey of patients with atrial fibrillation: associated disabilities and treatment preferences. Br J Gen Pract 1998; 48 (436) 1775-1778
- 28 Thomson R, Parkin D, Eccles M, Sudlow M, Robinson A. Decision analysis and guidelines for anticoagulant therapy to prevent stroke in patients with atrial fibrillation. Lancet 2000; 355 (9208) 956-962
- 29 Protheroe J, Fahey T, Montgomery AA, Peters TJ. The impact of patients' preferences on the treatment of atrial fibrillation: observational study of patient based decision analysis. BMJ 2000; 320 (7246) 1380-1384
- 30 Man-Son-Hing M, Laupacis A, O'Connor AM, Coyle D, Berquist R, McAlister F. Patient preference-based treatment thresholds and recommendations: a comparison of decision-analytic modeling with the probability-tradeoff technique. Med Decis Making 2000; 20 (4) 394-403
- 31 Schulman S, Crowther MA. How I treat with anticoagulants in 2012: new and old anticoagulants, and when and how to switch. Blood 2012; 119 (13) 3016-3023
- 32 Harenberg J, Felten M, Weiss C, Frölich L. The stability of the INR, the fear of thrombotic and bleeding complications are influenced by personality traits of patients on stable oral anticoagulant therapy. Haemostaseologie 2010; 30 (1) P02-P10
- 33 Franke GH. Possibilities of computer-assisted administration of the revised Freiburg Personality Inventory. 2 experimental studies[in German]. Z Exp Psychol 1997; 44 (2) 332-356
- 34 Forgays DG, Forgays DK, Spielberger CD. Factor structure of the State-Trait Anger Expression Inventory. J Pers Assess 1997; 69 (3) 497-507
- 35 Fisher PL, Durham RC. Recovery rates in generalized anxiety disorder following psychological therapy: an analysis of clinically significant change in the STAI-T across outcome studies since 1990. Psychol Med 1999; 29 (6) 1425-1434
- 36 Sanderson K, Andrews G. The SF-12 in the Australian population: cross-validation of item selection. Aust N Z J Public Health 2002; 26 (4) 343-345
- 37 Verkuil B, Brosschot JF, Thayer JF. Capturing worry in daily life: are trait questionnaires sufficient?. Behav Res Ther 2007; 45 (8) 1835-1844
- 38 Ware Jr J, Kosinski M, Keller SD. A 12-Item Short-Form Health Survey: construction of scales and preliminary tests of reliability and validity. Med Care 1996; 34 (3) 220-233
- 39 Svirtlih N, Pavic S, Terzic D , et al. Reduced quality of life in patients with chronic viral liver disease as assessed by SF12 questionnaire. J Gastrointestin Liver Dis 2008; 17 (4) 405-409
- 40 Völler H, Taborski U, Dovifat C , et al. ProTime self-management yielding improvement of fluency and quality of life. Thromb Haemost 2007; 98 (4) 889-895
- 41 Crawford B, Stanford RH, Wong AY, Dalal AA, Bayliss MS. Psychometric validation of the experience with allergic rhinitis nasal spray questionnaire. Patient Relat Outcome Meas 2011; 2: 127-133
- 42 Smetana GW, Davis RB, Phillips RS. Factors that influence patient response to requests to change to a unified restrictive formulary. J Gen Intern Med 2004; 19 (12) 1212-1219
- 43 Mussbrugger H, Kelava A. Testtheorie und Fragebogenkonstruktion. Berlin, Heidelberg. New York, NY: Springer Verlag; 2008: 409
- 44 Rogers MP, Orav J, Black PM. The use of a simple Likert scale to measure quality of life in brain tumor patients. J Neurooncol 2001; 55 (2) 121-131
- 45 Makowski CT, Jennings DL, Nemerovski CW, Szandzik EG, Kalus JS. The impact of pharmacist-directed patient education and anticoagulant care coordination on patient satisfaction. Ann Pharmacother 2013; 47 (6) 805-810
- 46 Casula M, Tragni E, Catapano AL. Adherence to lipid-lowering treatment: the patient perspective. Patient Prefer Adherence 2012; 6: 805-814
- 47 Alonso-Coello P, Montori VM, Solà I , et al. Values and preferences in oral anticoagulation in patients with atrial fibrillation, physicians' and patients' perspectives: protocol for a two-phase study. BMC Health Serv Res 2008; 8: 221
- 48 González-Rojas N, Giménez E, Fernández MA , et al. Preferences for oral anticoagulant treatment in the medium and long term prevention of stroke in non valvular atrial fibrillation [in Spanish]. Rev Neurol 2012; 55 (1) 11-19
- 49 Tversky A, Kahneman D. The framing of decisions and the psychology of choice. Science 1981; 211 (4481) 453-458
- 50 Bergus GR, Levin IP, Elstein AS. Presenting risks and benefits to patients. J Gen Intern Med 2002; 17 (8) 612-617
- 51 Maxwell GL, Synan I, Hayes RP, Clarke-Pearson DL. Preference and compliance in postoperative thromboembolism prophylaxis among gynecologic oncology patients. Obstet Gynecol 2002; 100 (3) 451-455
- 52 Man-Son-Hing M, Laupacis A, O'Connor AM , et al. A patient decision aid regarding antithrombotic therapy for stroke prevention in atrial fibrillation: a randomized controlled trial. JAMA 1999; 282 (8) 737-743
- 53 Draycott S, Dabbs A. Cognitive dissonance. 1: An overview of the literature and its integration into theory and practice in clinical psychology. Br J Clin Psychol 1998; 37 (Pt 3) 341-353
- 54 Beaton DE, Bombardier C, Guillemin F, Ferraz MB. Guidelines for the process of cross-cultural adaptation of self-report measures. Spine 2000; 25 (24) 3186-3191