
RSS-Feed abonnieren
DOI: 10.1055/s-0036-1580737
Transsphenoidal Approach to Pituitary Adenomas: from the Microscope to the Endoscope
Acesso transesfenoidal aos adenomas hipofisários: do microscópio ao endoscópioAddress for correspondence
Publikationsverlauf
06. September 2015
24. Dezember 2015
Publikationsdatum:
29. März 2016 (online)
Abstract
Objective Report the transitioning from the usage of microscope to endoscope in the transsphenoidal approach to pituitary adenomas with a main focus on technical nuances and incorporation of new surgical instruments throughout several years.
Methods Between 1993 and 2015, the Skull Base team of Hospital das Clínicas of UFMG operated on 225 pituitary adenomas through a transsphenoidal approach. The study was divided into 3 groups: the first group (from 1993 to 2001) used the microscope only; the second group (from 2002 to 2004) used both the microscope and endoscope simultaneously, and the third group (from 2005 to 2015) used the endoscope only.
Results There were 120 functional adenomas and 98 non-functional pituitary tumors; 7 cases could not be classified. The first two groups consisted of 50 cases, as 175 cases were operated with the endoscope only. As the transseptal moved to the endonasal route, it allowed the procedure to be performed by three or four hands, better visualization of the lateral sella, approach to the cavernous sinus and treatment of CSF leaks with a vascularized graft from the septal mucosa. The surgical instruments were adapted as the microscopic approach was switched to the endoscopic technique.
Conclusion Despite the lack of literature data showing superior magnification or lighting when comparing the endoscope to the microscope, we believe the former provides greater comfort and safety in the transsphenoidal approach for the treatment of pituitary adenomas.
#
Resumo
Objetivo Relatar a transição do microscópio ao endoscópio no acesso transesfenoidal aos adenomas hipofisários, com ênfase nas nuances técnicas, conceitos e incorporações de instrumentos cirúrgicos ao longo dos anos.
Método No período de 1993 a 2015, foram operados 225 adenomas hipofisários por via transesfenoidal pelo grupo de cirurgia de base do crânio do Hospital das Clínicas da UFMG. O estudo foi dividido em três etapas, de acordo com o dispositivo usado para iluminação e magnificação do campo operatório: primeira etapa (1993 a 2001), uso do microscópio; segunda etapa (2002 a 2004), uso simultâneo do microscópio e do endoscópio; terceira etapa (2005 a 2015), uso exclusivo do endoscópio.
Resultados Adenomas funcionantes corresponderam a 120 casos, e os não funcionantes, a 98. Sete casos não puderam ser classificados. Cinquenta cirurgias corresponderam às duas primeiras etapas, e 175 foram realizadas exclusivamente com o endoscópio. O acesso migrou do transeptal para o endonasal, o que permitiu a cirurgia a três ou quatro mãos, melhor visualização das porções laterais da sela e abordagem do seio cavernoso, além de tratamento de fístulas com retalho pediculado de mucosa do septo. Os instrumentos cirúrgicos foram adaptados à medida que se trocou o microscópio pelo endoscópio.
Conclusão Apesar de a literatura não demonstrar que um tipo de equipamento de iluminação e magnificação seja superior ao outro, acreditamos que o endoscópio nos propiciou maior conforto e segurança no tratamento dos adenomas hipofisários por via transesfenoidal.
#
Introduction
The evolution of the transsphenoidal approach to the sellar region can be divided into three ages: Macroscopic, Microscopic, and Endoscopic. This division has as a main factor the development of lighting and magnification methods. The Macroscopic Age corresponds to approximately the first half of the 20th century, with Harvey Cushing as its main representative. It is characterized by naked eye surgeries and frontal lighting of the operative field or the use of lamps on the speculum tip. The Microscopic Age began in the 1960s, when Jules Hardy described the use of the surgical microscope, which had a huge impact on the quality of lighting and magnification of the operative field, allowing it to become wider and deeper. Hardy described details of the surgical technique and adapted specific instruments for this type of surgery. The bases for the transsphenoidal approach using microscopic vision introduced by Hardy are still used today, with few modifications. In the late ‘90s, groups of neurosurgeons and otorhinolaryngologists from different countries introduced the endoscope as a new piece of operative field lighting and magnification equipment, leading to changes in surgical instruments and approach specifics.[1] [2]
Despite the division of ages, the endoscopic technique does not supplant the microscopic technique, and various professionals that deal with pituitary tumors have had the opportunity to operate with one of these two lighting and magnification methods. According to Edward Laws, it is estimated that 50% of the neurosurgery services in the United States still use the microscope (personal communication).
In 2002, the neuroendoscope was introduced in the Hospital das Clínicas of the Federal University of Minas Gerais. Since then, the skull base surgery group progressively moved from microscope to endoscope use only in the transsphenoidal approach to the sellar region, going through a period when both types of equipment were employed. This study aims to relate our experience, with emphasis on technical nuances, on the modified concepts and incorporations of customized instruments throughout the past years. The authors intend, therefore, to aid surgeons desiring to move towards a similar path.
#
Methods
The skull base surgery group of the Hospital das Clínicas of the Federal University of Minas Gerais began their activities in 1993, in the association of neurosurgery and otorhinolaryngology teams. Since then, 255 pituitary adenoma surgeries were performed by the same neurosurgeon (author AVG).
Patients were selected for the transsphenoidal approach according to one of the following criteria: (1) microadenomas (tumors with a diameter < 10 mm); (2) macroadenomas extending to the floor of the third ventricle and possibly elevated; and (3) macroadenomas with an important intrasphenoidal component. The following criteria were not considered as contraindication for the transsphenoidal approach: (1) low aerated sphenoidal sinus; and (2) invasion of the cavernous sinus(es). Patients were submitted to the transcranial approach when the macroadenoma presented suprasellar extension up to the foramen of Monro and/or anterior expansion to the sphenoid plane, middle fossa, or descending the sellar back. According to these criteria, 30 (11.8%) of the surgeries were performed through a transcranial approach and 225 (88.2%) through a transsphenoidal approach. The latter approaches comprise the cases for the present study.
The functional classification of adenomas followed clinical and immunohistochemical criteria. Tumors were classified as: ACTH, GH, prolactin and TSH producers, and nonfunctional. In the case of co-producing tumors, only the hormone with the most significant clinical expression was considered.
The 23-year duration of this study was divided into three phases. From 1993 to 2001, the procedure was performed exclusively using the microscope. From 2002 to 2004, despite the microscope being the main equipment, at the end of each step of the approach and the global period, the endoscope was brought into the operative field for visualization and familiarization of the neurosurgeon with the equipment. From 2005 to 2015, the entire procedure was performed using only the endoscope.
In order to describe the evolution of the technique, the surgical procedure was divided into three surgical periods: (1) approach and opening of the sphenoid sinus; (2) opening of the sellar floor and tumor resection; and (3) closing. This evolution was influenced by personal learning and medical literature that accompanied the study period.
During the second phase (from 2002 to 2004), when the microscope and the 30-degree endoscope were simultaneously used, the image and magnification provided by each equipment type were compared.
#
Results
The 225 surgeries were performed in 92 male patients and 124 female patients (9 patients were re-operated through the same approach). Their ages varied from 14 to 81 years.
[Table 1] shows the distribution of the types of adenomas, according to the functional classification. The functioning tumors (GH, ACTH, prolactin, and TSH producers) corresponded to 120 cases, while the nonfunctioning corresponded to 98. In seven (previous) cases, it was impossible to identify the classification of the adenomas in medical records. Regarding size, 31% of the cases were classified as microadenomas and 69% as macroadenomas.
Twenty-nine cases were submitted to surgical treatment using only the microscope. In 21 cases, the microscope and the endoscope were used together. These 50 surgeries (22.2%) correspond to the two initial phases of the study during the first 12 years (from 1993 to 2004). During the last 11 years (from 2005 to 2015), 175 cases (77.8%) were operated exclusively using the endoscope ([Table 2]).
Positioning and Placement of the Surgical Team
Over the years, small changes have been made regarding patient positioning and anesthetic procedures. After receiving general anesthesia, orotracheal intubation, two peripheral venous accesses, invasive arterial monitoring, and an indwelling urinary catheter, the patient was positioned with his/her head resting on a slightly extended frame, above the chest. A cushion placed under the patient's knees eased the extension of the lower limbs, which were placed above the chest as well. Intravenous hydrocortisone at a dose of 100 mg was used in every case, regardless of presence or absence of adrenal insufficiency and even in cases of Cushing's disease. Antibiotic prophylaxis was administered during anesthetic induction and continued for 24 hours, although the nasal tamponade remained until the second or third postoperative day. At first, sulfamethoxazole and trimethoprim were used, but during the last 6 years, they were replaced by ceftriaxone and clindamycin, following a recommendation from the hospital infection control committee. Asepsis was performed using topical Povidine on the face, nasal cavity, and upper gum (only if sub-labial approach was performed). In cases in which fat or fascia lata extraction was predicted, the thigh was prepared with PVP degerming alcoholic Povidine. Operative fields were prepared, and only the nose and the upper lip remained uncovered. However, during the age of pure endoscopic surgery, the face and the nose were covered with sterile plastic, and two punctures were made as instrument passages. Nasal vasoconstrictor was dripped into each nostril before anesthetic induction. After operative fields were established, cottonoids with adrenaline solution were introduced into each nostril and kept for 3 to 5 min.
At the beginning of the surgical period, when the microscope was the equipment of choice for lighting and magnification, the patient's head was rotated to the right and tilted as if the left ear was ipsilaterally pointing to the shoulder. The surgeon (initially the otorhinolaryngologist and later the neurosurgeon) was placed at the right side of the patient as if facing him/her. The assistant was placed right in front of the surgeon, at the head of the operating table. The surgical instrument technician was placed at the left of the surgeon. The anesthetist was placed at the left of the patient, close to his/her feet. The procedure was initiated by naked eye, with frontal focus lighting until the speculum placement and approach to the sphenoidal rostrum. At this moment, the microscope was brought to the field and placed over the patient's head, where the assistant had been. The ocular lenses were flat, and the objective was a 400 mm lens.
During the second phase, from 2002 to 2004, when the endoscope was incorporated, the cabinet containing the monitor, the light source, and the camera was placed to the left of the patient, opposite to the surgeon's position. At that time, only the 30-degree endoscope was used.
During the third phase, from 2005 to 2015, when the whole procedure began to be performed exclusively using the endoscope, there was a major change in the positioning of the surgical team. During the approach and until the exposure of the sellar floor, the otorhinolaryngologist was to the right side of the patient and assisted by the neurosurgeon, who was on the left. Right after, the positions were inverted. Once the surgery started to be carried out by three or four hands, the patient's head was placed in a neutral position in order to allow both surgeons to have equal access to the nasal cavities. The cabinet containing the monitor, light source, and camera was placed over the patient's head, in order to allow both surgeons to view the image ahead of them. The instrument technician and the anesthetist remained in their original positioning.
At the beginning of our experience, radioscopy was used as a method of intraoperative localization, but it was quickly abandoned. During the last year, the neuronavigation system was acquired and placed at the upper left corner of the table's head, next to the video cabinet. For proper use, the patient's head was fixed using a three-point head frame (Mayfield type), and the three-sphere reference array was fixed to the Mayfield support, in order not to interfere in the endoscope instrument's entry into the nasal cavities.
#
Approach and Opening of the Sphenoid Sinus
The approach to the sphenoidal rostrum was transseptal in 71 cases (31.6%) and endonasal in 154 cases (68.4%). In the 50 surgeries in which the microscope was used, the approach was transseptal. At first, the incision was sub-labial, but shortly thereafter, incisions to the nasal mucosa close to the columella were adopted. A submucosal dissection was performed from the right of the nasal septum to the junction of the cartilage with the perpendicular plate of the vomer bone. In this posterior septal region, a bilateral dissection was performed, in order to preserve the cartilaginous portion still adhered to the left nasal cavity mucosa. Once the mucosa was dissected to the end of the septum, the sphenoidal rostrum was identified. The elevation of its mucosa to the lateral and cranial side allowed the identification of the sphenoid ostia. At this moment, the speculum was placed in order to hold the created tunnel open. This phase of the procedure was performed by naked eye and using frontal lighting. Under magnification and lighting from the microscope and in the first cases of pure endoscopy, the opening of the sphenoid was initiated through the sphenoid ostia using a 2 mm Kerrison gouge. The sphenoidotomy was extended inferiorly using a chisel and laterally using the Kerrison gouge. The sinus mucosa was moved away or partially resected, allowing the exposure of the sellar floor bone.
At the beginning of the use of pure endoscopic technique, the transseptal approach was maintained as described above. Then, in an attempt to follow the medical literature describing the endonasal approach, this method was adopted using both nostrils. The approach is initiated through the bilateral dislocation of the inferior and medium turbinates. At the bottom of the nasal cavity, sphenoid ostia are located about 1.5 cm above the choanae and a few millimeters laterally from the junction of the nasal septum with the sphenoidal rostrum. Sphenoidotomy is initiated by widening the ostia using the Kerrison gouge. Part of the mucosa that covers the rostrum is simultaneously removed. The inferior and thicker portion of the rostrum was previously removed using the chisel, but more recently, it has been removed using a motorized cutting drill. The most posterior portion of the nasal septum is removed, and the bone is saved for the sellar closing. This is the most commonly used endonasal approach, though it can present some variations. Its main recommendation has been for adenomas restricted to the sella or with superior projections to the optic chiasm. In cases where the suprasellar expansion is large (generally tumors with a height exceeding 2.5 cm), and therefore the chance of cerebrospinal fluid leak is greater, a nasal septal flap is prepared during the approach. In cases where there is an important septum deviation or spurs that complicate the instrument passage, a traditional treatment for the deviation can be performed during the same surgical act.
#
Sellar Opening and Tumor Resection
The method for sellar opening and tumor resection underwent little change during the replacement of the microscope by the endoscope. If the sellar floor was thin, its removal was performed only by using the Kerrison gouge. If it was preserved, a central opening was made using the chisel and enlarged in all directions using the Kerrison gouge. Recently, a motorized diamond drill has been used. The dural opening was cross-shaped initially; however, during the last 2 years it became “U” shaped with its base turned down.
The tumor resection is initiated with internal decompression using a ring curette, vacuum suction, and tumor and biopsy forceps. Then, it is removed with a curette from the posterior, lateral, and finally, the anterior directions of the sella. In few cases, it is possible to obtain a cleavage plane between the tumor and the normal gland, allowing the lesion's “extracapsular” dissection. Neoplasia has a soft and quite friable consistency in most patients. Such characteristic favors the “centripetal” dissection and identification of a firmer normal gland tissue, which is not easily removed using the curette. Intratumoral bleeding is quite variable. Rarely, the tumor was more consistent. With the use of the microscope, the lateral curettage towards the cavernous sinuses was blindly performed. However, the 30-degree endoscope allowed a better visualization of the sinus wall and the curettage procedure of this region.
#
Closing
The sellar reconstruction was performed in every case with bone fragments or cartilage from the nasal septum and covered with biological glue. In cases where intraoperative cerebrospinal fluid fistula was not observed or the arachnoid lesion was punctiform, the sellar interior was coated with Surgicel. In cases of greater magnitude of cerebrospinal fluid fistula, the sellar interior was filled with fat and glue before the floor reconstruction. When the microscope was used, and in the first years of the endoscopic technique, fat was placed in the sphenoid sinus. During the last 4 years, septum mucosa pedicle flaps were adopted in cases where cerebrospinal fluid fistula was significant. More recently, in cases of significant intraoperative cerebrospinal fluid fistula, fascia lata has been used for the sellar floor reconstruction using the gasket technique.[3]
Nasal tamponade was performed in every patient and maintained for 2 to 3 days.
In all cases of significant intraoperative cerebrospinal fluid fistula, an external lumbar drainage with a number 16 epidural catheter was installed. The cerebrospinal fluid drainage was performed every 12 hours. A syringe was attached to the catheter tip, followed by aspiration of 20 ml of cerebrospinal fluid or an inferior volume if the patient reported headaches. The drainage was maintained for 4 to 5 days, and the fluid was forwarded for analysis every 2 days. In cases of persistent cerebrospinal fluid rhinorrhea, drainage was maintained for up to 10 days before submitting the patient to a new fistula closure approach. Acetazolamide was not administered in order not to obscure a diabetes insipidus diagnosis, which may occur in this type of surgery.
#
#
Discussion
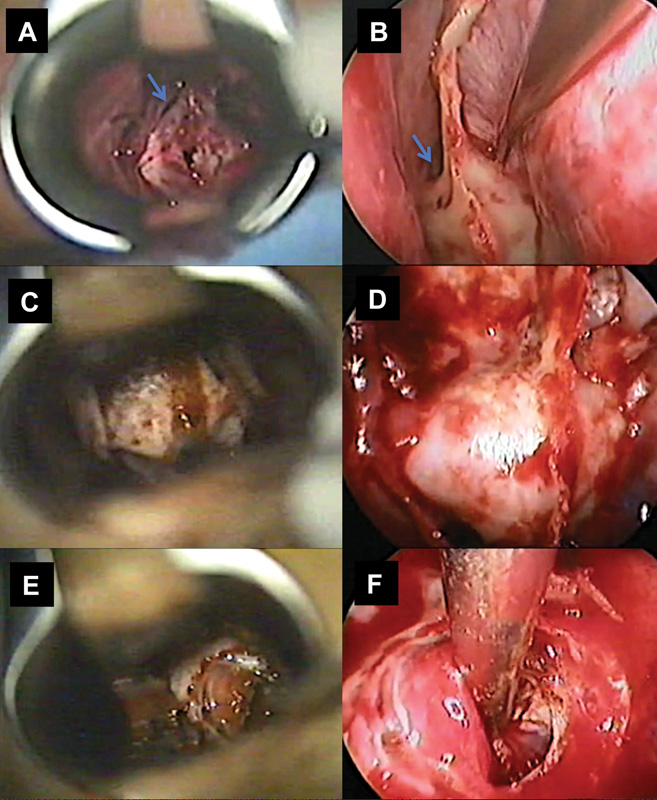
The major differences between the microscope and the endoscope are in lighting and magnification capabilities. The endoscope has better lighting capability for the operative field because it directs all the light towards it. The microscope remains apart from it, thus only part of the light is directed to the operative field, while the other part lightens the patient's face. For this reason, the use of speculum becomes mandatory and, the more opened it is, the better the lighting towards the sellar region. Regarding magnification, the image from the endoscope is larger than the view from the microscope. In addition, the straight view provided by the microscope reduces the field of view. The endoscope has a larger aperture, and the field of view can be enhanced using 30- and 45-degree lenses, allowing visualization behind anatomic barriers as well ([Fig. 1]). In our experience, these aspects provided more comfort and safety to the procedure, allowing a more “aggressive” attitude of the surgeon, in the sense of attempting more complete dissections throughout the years.
The endoscope presents the following disadvantages: two-dimensional view, frequent lens fogging, some conflict degree with the surgical instruments in the operative field, and ability of handling only one instrument at the time if one of the surgeon's hands is holding the lens. All of these inconveniences have been gradually overcome. The loss of the tri-dimensional view, which was provided by the microscope and is reported by literature[4] did not seem evident to us and did not present a restraint. Furthermore, various authors report that approaching and distancing movements of the endoscope allow quick adaptation and compensation.[4] Although fogging and darkening by blood once demanded removal and reinsertion of the lens, continually interrupting the surgery and extending its time, this inconvenience was solved by using an endoscope housing, which is coupled to an extension and a syringe containing saline solution. The lens cleaning is performed using manual irrigation of a few milliliters of saline solution. Furthermore, the evolution towards the three or four hands technique allowed the surgeon's hands to be free. Currently, we prefer that the assistant hold the camera and, eventually, the vacuum pump. The solution for the instrument conflicts were solved by training.
As reported above, the microscope demands the use of the speculum to keep the tunnel open for lighting and allow the instruments to reach the operative field. The larger the opening, the better the lighting and the lesser the chance of the instruments shadowing the surgeon's view. The transseptal approach is the best for this objective. If the incision is sub-labial, the opening must be even larger. In the first phase of our study, this incision was used especially when we needed to introduce the motorized drill in order to open a low aerated sphenoid sinus. However, we know that the greater the manipulation of nasal structures, the greater the sinonasal complications index, with complications such as septal perforation, crust formation, adhesions, and post-operative sinusitis. Therefore, the approach to the sphenoid sinus passing directly through the natural nasal cavity seems more logical and reduces the surgical time. Literature reports that the speculum can be inserted through one of the nostrils.[5] We did not use it this way, but at first it seemed that the speculum opening would be smaller, and the slightly angled approach presents a risk of hitting the cavernous contralateral sinus and obtaining a smaller ipsilateral sellar portion view. With this reasoning, we moved from the transseptal approach to the endonasal approach in the third phase of our study when we began to exclusively use the endoscope. The two-nostril approach allowed not only a three or four handed surgery, but also widened the angle of instrument insertion, allowing a greater access to the lateral portions of the sella and the cavernous sinus.
Moving from the microscope to the endoscope also demanded a change in the surgical instruments. While the speculum and its widener, designed by Hardy, were abandoned, various instruments long used by otorhinolaryngologists were incorporated, such as the Cottle septum elevator, septum suction elevator, turbinate scissors, Takahashi forceps, Struycken cutting forceps, Stammberger cutting forceps, Hartmann alligator forceps, and chisel. The microsurgical instruments remained the same, but their shapes changed. While microscopic surgery required a bayonet shape in order not to shadow the surgeon's view, with the endoscope this shape hits the camera when the instrument is rotated. Therefore, the instruments have been re-shaped to a rectilinear shape. For microscope surgeries there was a tunnel for instrument penetration, thus their width was not a problem. The ergonomic forceps handling, with the thumb opposing to the second and third fingers, allowed instruments such as micro scissors, tumor forceps, and bipolar forceps to be wide. In the endoscope approach, the path is narrow and the instruments are slim.[6] Initially, micro scissors, tumor forceps, and bipolar forceps were redesigned, with a slim and straight stem, and the grip received rings for finger insertion. Such design demanded training and adapting the neurosurgeon. Nevertheless, the gesture became less precise, a characteristic that microsurgery establishes. More recently, these instruments have been renovated, maintaining the slim and rectilinear stem demanded by endoscopy, but conserving the same forceps grip as the old instruments ([Fig. 2]).

Once the endoscope allowed the lateral and back visualization of the structures, it was important to suck, resect, and coagulate these regions. While the angulated curettes previously allowed only a blind removal in these spots, this procedure was now in view, offering more safety. Using the angulation principle for instrument tips, suction tips angled 30 degrees upside and downside and tumor forceps with equally angled tips were manufactured[7] ([Fig. 3]).

Due to the depth of the operative field, we designed an applicator for the biological glue, composed of two long and parallel cannulas, long used since the microscopic age ([Fig. 4]).

Since the beginning of our experiment, we observed that once the sphenoid ostia were identified, the sellar floor would be right behind. Therefore, we early abandoned fluoroscopy, which was restricted to rare cases of low aerated sinuses or to reoperations where the anatomy of the sellar floor could hardly be identified. Throughout all these years, we used the correlation between the anatomy observed in image exams (computed tomography scan and magnetic resonance imaging) and the intraoperative anatomy. We can say that this correlation has provided safety for the opening of the sellar floor in almost every case. More recently, with the incorporation of neuronavigation systems, we began to use it specifically for low aerated sphenoid sinuses cases, reoperation, or small lesions close to the cavernous sinus, or those that invade the medial and inferior portions of the sinus, where we believe that a resection is possible. In our opinion, these last locations were impossible to reach with the use of the microscope. Hardy still highlights the importance of fluoroscopy as the best way to document, in real time, the descent of the tumor.[ 2] We preferred not to use it because we believe that fluoroscopy is not so sensitive and demands the insertion of a lumbar catheter and an injection of air or contrast, which raises the cost and/or the risk. Although neuronavigation is based on pre-operative images, we thought that if the tip reached the superior limits of the lesion, a complete resection was likely. We do not have experience with intraoperative resonance; however, the literature reports that this procedure does not significantly raise the degree of radicality of the tumor removal. Furthermore, intraoperative resonance is quite expensive and requires three to four exams during the surgery, greatly increasing the surgery global time.[8] [9]
Theoretically, because endoscopy provides better lighting, magnifications, and view angle, it could lead to an increase of cure rate or remission of adenomas. However, in practice, this evidence was not observed.[10] [11] [12] It seems to be true for us, especially in cases of microadenomas, in which excellent results in a large series of microsurgery techniques maintained a similar success rate when performed by experienced endoscopists. In the second phase of our series, when the endoscope was used at the end of the microsurgery global time, despite the extraction of fragments of tumors that were not detected with the use of the microscope in few cases, it did not mandatorily lead to a total resection or biochemical cure. Intuitively, however, we believe that in some situations the endoscopic technique seems to provide better results. Currently, we dare to open the medial and/or inferior portions of the cavernous sinus, which was impossible during the microscope age. This advance was made possible mainly by the lateral view and magnification provided by the endoscope, although new hemostatic products and also the learning curve itself contributed in this sense.
Regarding the sella closing, we were always in favor of trying its reconstruction, in order to avoid fistula or for the possible necessity of reoperation because a new surgical procedure would become less difficult. We never used allografts such as Porex ® or titanium or ceramic plates. In all our cases, we used bone or cartilage extracted from the nasal septum. Our policy was to use the minimum possible fat, in order not to interfere in the interpretation of postoperative exams. In the microscopic era, in cases of large fistulas, we filled the sphenoid sinus with fat after the sellar reconstruction. Since the description of the nasal septum mucosa pedicle flaps,[ 13] we started to adopt them and practically no longer use fat in the sinus. This is an additional advantage of the endoscopic technique when compared to the microscopic technique.
#
#
-
References
- 1 Gandhi CD, Christiano LD, Eloy JA, Prestigiacomo CJ, Post KD. The historical evolution of transsphenoidal surgery: facilitation by technological advances. Neurosurg Focus 2009; 27 (3) E8
- 2 Hardy J. Reflections on the evolutions of pituitary tumor surgery with emphasis on the transsphenoidal approach. In: Laws E, Lanzino G, editors. Transsphenoidal surgery. Philadelphia: Saunders; 2010: 1-3
- 3 Leng LZ, Brown S, Anand VK, Schwartz TH. “Gasket-seal” watertight closure in minimal-access endoscopic cranial base surgery. Neurosurgery 2008; 62 (5) (Suppl. 02) E342-E343 , discussion E343
- 4 Cappabianca P, Cavallo LM, Esposito F, Stagno V, Notaris MG. Endoscopic transsphenoidal surgery: anatomy, instrumentation, technique. In: Laws E, Lanzino G, editors. Transsphenoidal surgery. Philadelphia: Saunders; 2010: 128-142
- 5 Rothon Jr AL. The sellar region. Neurosurgery 2002; 51 (4 Suppl): S335-S374
- 6 Cappabianca P, Alfieri A, Thermes S, Buonamassa S, de Divitiis E. Instruments for endoscopic endonasal transsphenoidal surgery. Neurosurgery 1999; 45 (2) 392-395 , discussion 395–396
- 7 Jho HD, Alfieri A. Endoscopic endonasal pituitary surgery: evolution of surgical technique and equipment in 150 operations. Minim Invasive Neurosurg 2001; 44 (1) 1-12
- 8 Bernays RL. Intraoperative imaging: current trends, technology and future directions. In: Laws E, Lanzino G, editors. Transsphenoidal surgery. Philadelphia: Saunders; 2010: 56-69
- 9 Buchfelder M, Schlaffer SM. Intraoperative magnetic resonance imaging during surgery for pituitary adenomas: pros and cons. Endocrine 2012; 42 (3) 483-495
- 10 Ammirati M, Wei L, Ciric I. Short-term outcome of endoscopic versus microscopic pituitary adenoma surgery: a systematic review and meta-analysis. J Neurol Neurosurg Psychiatry 2013; 84 (8) 843-849
- 11 Goudakos JK, Markou KD, Georgalas C. Endoscopic versus microscopic trans-sphenoidal pituitary surgery: a systematic review and meta-analysis. Clin Otolaryngol 2011; 36 (3) 212-220
- 12 Rotenberg B, Tam S, Ryu WH, Duggal N. Microscopic versus endoscopic pituitary surgery: a systematic review. Laryngoscope 2010; 120 (7) 1292-1297
- 13 Hadad G, Bassagasteguy L, Carrau RL , et al. A novel reconstructive technique after endoscopic expanded endonasal approaches: vascular pedicle nasoseptal flap. Laryngoscope 2006; 116 (10) 1882-1886
Address for correspondence
-
References
- 1 Gandhi CD, Christiano LD, Eloy JA, Prestigiacomo CJ, Post KD. The historical evolution of transsphenoidal surgery: facilitation by technological advances. Neurosurg Focus 2009; 27 (3) E8
- 2 Hardy J. Reflections on the evolutions of pituitary tumor surgery with emphasis on the transsphenoidal approach. In: Laws E, Lanzino G, editors. Transsphenoidal surgery. Philadelphia: Saunders; 2010: 1-3
- 3 Leng LZ, Brown S, Anand VK, Schwartz TH. “Gasket-seal” watertight closure in minimal-access endoscopic cranial base surgery. Neurosurgery 2008; 62 (5) (Suppl. 02) E342-E343 , discussion E343
- 4 Cappabianca P, Cavallo LM, Esposito F, Stagno V, Notaris MG. Endoscopic transsphenoidal surgery: anatomy, instrumentation, technique. In: Laws E, Lanzino G, editors. Transsphenoidal surgery. Philadelphia: Saunders; 2010: 128-142
- 5 Rothon Jr AL. The sellar region. Neurosurgery 2002; 51 (4 Suppl): S335-S374
- 6 Cappabianca P, Alfieri A, Thermes S, Buonamassa S, de Divitiis E. Instruments for endoscopic endonasal transsphenoidal surgery. Neurosurgery 1999; 45 (2) 392-395 , discussion 395–396
- 7 Jho HD, Alfieri A. Endoscopic endonasal pituitary surgery: evolution of surgical technique and equipment in 150 operations. Minim Invasive Neurosurg 2001; 44 (1) 1-12
- 8 Bernays RL. Intraoperative imaging: current trends, technology and future directions. In: Laws E, Lanzino G, editors. Transsphenoidal surgery. Philadelphia: Saunders; 2010: 56-69
- 9 Buchfelder M, Schlaffer SM. Intraoperative magnetic resonance imaging during surgery for pituitary adenomas: pros and cons. Endocrine 2012; 42 (3) 483-495
- 10 Ammirati M, Wei L, Ciric I. Short-term outcome of endoscopic versus microscopic pituitary adenoma surgery: a systematic review and meta-analysis. J Neurol Neurosurg Psychiatry 2013; 84 (8) 843-849
- 11 Goudakos JK, Markou KD, Georgalas C. Endoscopic versus microscopic trans-sphenoidal pituitary surgery: a systematic review and meta-analysis. Clin Otolaryngol 2011; 36 (3) 212-220
- 12 Rotenberg B, Tam S, Ryu WH, Duggal N. Microscopic versus endoscopic pituitary surgery: a systematic review. Laryngoscope 2010; 120 (7) 1292-1297
- 13 Hadad G, Bassagasteguy L, Carrau RL , et al. A novel reconstructive technique after endoscopic expanded endonasal approaches: vascular pedicle nasoseptal flap. Laryngoscope 2006; 116 (10) 1882-1886