Keywords
intradural spinal arteriovenous fistula - embolization - microsurgical technique
Palavras-chave
fístula arteriovenosa espinhal intradural - embolização - técnica microcirúrgica
Background and Importance
Although rare, arteriovenous fistulas (AVFs) are the most common spinal vascular malformations,
and are mainly located in the thoracic region. Neurogenic claudication is the most
common clinical presentation, and it is often mistaken for lumbar stenosis. Magnetic
resonance imaging (MRI) complements the diagnosis, but the gold-standard procedure
is arteriography. Through arteriography, one can identify the AVF and treat it with
embolization, or the procedure can guide the microsurgical treatment. While in the
literature we can find information corroborating the endovascular first approach,[1] in the present article we demonstrate the efficacy of the microsurgical treatment.
Clinical Presentation
A 61-year-old woman presented at the outpatient clinic complaining of low back pain
and gait disturbance. The clinical presentation had been progressing for ∼ 6 months
with paresis and sensory loss in the limbs, in addition to urinary dysfunction. She
did not have diabetes, arterial nor trauma due to tumble.
A physical examination revealed slow gait, grade 4 paraparesis, exalted patellar and
Achilles reflexes, and normal plantar cutaneous reflexes. Tactile hypoesthesia with
a sensitive level in L2 was associated. The first treatment was conservative; we considered
the hypothesis of lumbar stenosis until the complementary exams.
The MRI ([Fig. 1]) demonstrated a normal spinal canal, but with a medullary hypersignal in the lumbar
up to the cone regions associated with serpiginous vessels near the dorsal medullary
region as flow-voids. Later, the hypothesis of dorsal intradural AVF was confirmed
by arteriography.
 Fig. 1 Magnetic resonance imaging with medullary hypersignal in the cone region (1), and serpiginous vessels near the dorsal medullary region as flow-voids (2).
Fig. 1 Magnetic resonance imaging with medullary hypersignal in the cone region (1), and serpiginous vessels near the dorsal medullary region as flow-voids (2).
The fistula embolization was attempted during the arteriography, but without success
(see preoperative arteriography with elements of embolization near the fistula region,
[Fig. 2]). The patient presented aggravation in her limb movements and grade 2 paraparesis.
She was referred to neurosurgery, and the microsurgical treatment was performed.
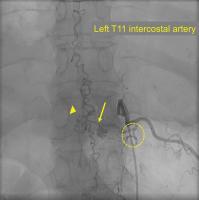 Fig. 2 Arteriography in which the left T11 intercostal thoracic artery was catheterized,
above the Adamkiewicz artery, and identification of the fistula (arrow), the venous ectasia (arrow head), and the elements of the previous embolization (circle).
Fig. 2 Arteriography in which the left T11 intercostal thoracic artery was catheterized,
above the Adamkiewicz artery, and identification of the fistula (arrow), the venous ectasia (arrow head), and the elements of the previous embolization (circle).
The team determined the fistula's topography with intraoperative fluoroscopy during
the surgery. We used information from the interventionist team on the site of the
fistula: to the left, at the level of T11. Then, we proceeded to the laminotomy from
T10 to T12. The dural opening was made with a number 15 blade and Metzembaum scissors.
We spotted the engorged veins under the subarachnoid space.
By means of microsurgical technique, the fistulous path was identified at the level
of the 10th left thoracic root ([Fig. 3]). Sensitive and motor roots were also identified at the drainage vein in the neural
root entry, and preserved during surgery ([Fig. 4]). The drainage vein was compressed with a bipolar forceps under electrophysiological
monitoring, and, as we did not observe any decrease in motor potentials, we proceeded
to the final bipolar coagulation, and cut with microsurgery scissors ([Fig. 5A], [B] and [C]).
 Fig. 3 (A) Identification of the intradural fistula, as well as the venous ectasia, over the
medullary region. (B) Identification of the extradural face of the neural root at the level of the fistula.
Fig. 3 (A) Identification of the intradural fistula, as well as the venous ectasia, over the
medullary region. (B) Identification of the extradural face of the neural root at the level of the fistula.
 Fig. 4 (A) Identification of the venous ectasia together with the fistula (1); the dorsal sensitive root, (2); and the ventral motor root, (3). (B) Compression of the fistula with a bipolar forceps while the neurologist performs
the electromonitoring.
Fig. 4 (A) Identification of the venous ectasia together with the fistula (1); the dorsal sensitive root, (2); and the ventral motor root, (3). (B) Compression of the fistula with a bipolar forceps while the neurologist performs
the electromonitoring.
 Fig. 5 (A) Coagulation of the fistula with a bipolar forceps; (B) Cutting of the fistula with microsurgical scissors; (C) The ecstasiated veins were identified after the obliteration of the fistula; (D) The treatment was complemented performing the extradural root coagulation with a
bipolar forceps.
Fig. 5 (A) Coagulation of the fistula with a bipolar forceps; (B) Cutting of the fistula with microsurgical scissors; (C) The ecstasiated veins were identified after the obliteration of the fistula; (D) The treatment was complemented performing the extradural root coagulation with a
bipolar forceps.
As we performed the dural eversion, enlarged vessels were observed in the extradural
face of the neural root. Therefore, these vessels were also submitted to cauterization
([Fig. 5D]). We closed the dura mater using 4–0 polydioxanone sutures (PDS), and the laminotomy
using mini-plates.
Discussion
There are many types of spinal vascular malformations.[2] However, the classification made by Spetzler et al, which was based on a case series,[5] is the most used. It has been divided into two main groups: AVFs and arteriovenous
malformations.[3] The AVF with intradural drainage is the most common, and it usually occurs in the
thoracic region,[4] as we exemplified in the present clinical case.
The artery of Adamkiewicz is the main medullary nutrition source in the thoracolumbar
region; it is located between T9-T12 in the left side. Identifying this artery is
important because it enables the embolization of root branches in this spinal topography,
if the artery of Adamkiewicz is not involved.[3]
Spinal AVFs occur in the dura-mater of the roots, leading to arterialization of the
venous plexus, venous hypertension and medullary ischemic myelopathy.[3]
[5]
With probable acquired cause, AVFs have progressive clinical manifestation and initially
present sensitive deficits (in 80% of the cases), paresis (70%) and sphincter dysfunction
(62.5%).[1] Neurogenic claudication is often mistaken for lumbar stenosis, which leads to a
delay in the diagnosis.[1] With time, motor deficits and gait disturbances progress.[3]
The diagnosis is suggested in the MRI exam when there is medullary hypersignal, as
well as serpiginous perimedullary vessels seen as flow-voids in the dorsal surface.[3]
The arteriography is the gold-standard examination, and specific protocols determine
the artery of Adamkiewicz level and venous stasis, suggesting the AVF site. During
the arteriography, the level of AVF is identified by the vertebral body and side.[5]
Arteriovenous fistulas should be treated as soon as diagnosed to prevent the progression
to severe and irreversible deficits that occur if the time between diagnosis and therapy
reaches 3 years.[5]
[6] Thus, the goal of the treatment is to stop the progression of the myelopathy, or
even to reverse the deficits by restoring spinal perfusion.[3]
Studies demonstrate that there are no differences in the obliteration rates between
the endovascular and microsurgical treatments, enabling the migration from embolization
to surgery, either due to the impossibility of embolization, or due to inadequate
occlusion.[7]
Some services suggest that the initial attempt of embolization at the moment of the
diagnostic arteriography is feasible; however, it has failure rates of 50%,[4]
[7] unlike the surgical treatment, which is definitive in all cases.[4]
For proper embolization, it should be possible to navigate with the microcatheter
to the fistulous point where the liquid emboligenic agent is injected,[3] which is not always possible, as in the present case.
During surgery, the site of the fistulous point should be identified at the exit of
the nerve root, enabling the clipping, or clotting and cutting of the fistulous connection.[3] Multimodal intraoperative monitoring increases the safety of the procedure,[3] so we performed it with the patient described. Venus compression with bipolar forceps
is one possibility, clipping the vein under electromonitoring before definitive occlusion
is the other.
The extradural inspection of the nerve root after cutting the fistulous point reveals
the vascularized pedicle; however, arterial nutrition is not always visible, since
the fistula occurs between the dural layers.[5] Thus, part of the surgical technique involves extradural coagulation at the height
of the involved nerve root.
Measures of epidural venous pressure reveal a drop from 40 mmHg before the treatment
to 23mmHg after obliteration of the fistula with subsequent reduction of the venous
flow.[5]
The patient was submitted to a successful surgical treatment, with the AVF being identified
intraoperatively; then, the AVF was submitted to coagulation and cutting, which were
complemented with extradural coagulation in the nerve root. The deficits were maintained
in the immediate postoperative period, and after the discharge from the hospital,
no new complications were identified.
Conclusion
Arteriovenous fistulas have progressive clinical manifestation, and should be treated
as soon as diagnosed to prevent the progression to severe and irreversible deficits.
Thus, the goal of the treatment is to stop the progression of the myelopathy. The
initial attempt of embolization at the moment of diagnostic arteriography is possible,
but it has failure rates of 50%, unlike the surgical treatment, which is definitive
in all cases. The patient was submitted to a successful surgical treatment, and physical
therapy rehabilitation was indicated.






