Preoperative Evaluation
Clinical conference before surgery is very important for the patient and the doctors.
All of medical staffs, not only gynecologists but also radiologists and pathologists
if possible, should gather and discuss the precise diagnosis and the operative procedure.[1] In case of uterine fibroids, the preoperative assessment is especially important,
because the clinical diagnosis is not pathological but just presumable. In fact, 5%
of the cases diagnosed preoperatively as benign are pathologically not usual leiomyoma
but tumors of other histology such as cellular leiomyoma, dissecting leiomyoma, intravenous
leiomyomatosis, endometrial stromal sarcoma, smooth muscle tumor of uncertain malignant
potential, and leiomyosarcoma.
Thus, it is very important to confirm again the current case as benign leiomyoma using
magnetic resonance imaging (MRI) findings.[2] If MRI image shows that the tumor has uniform low-intensity in T2-weighted image
and well demarcated, it is absolutely benign leiomyoma ([Fig. 1]). Low-intensity with several furrow-like high-intensity strings also indicates benign
([Fig. 2]). In MRI, however, T2-weighted image with heterogeneous high-intensity and fine
granular shadow represents higher cellularity of tumor cells. High-intensity in T1-weighted
image suggests the presence of intratumoral bleeding. Defect in contrast-enhanced
image indicates the necrosis in the tumor. These MRI findings strongly suggest that
this tumor is not usual leiomyoma but may be leiomyosarcoma ([Fig. 3]). When considering the possibility of sarcoma, the attitude of surgeon must change
at hysterectomy. Especially, in case planning myomectomy or planning laparoscopic
surgery, it is much more serious for both careful explanation to the patient and careful
surgery with “non-touch” technique for the tumor.
 Fig. 1 Magnetic resonance imaging (MRI) findings of typical benign leiomyomas. If MRI image
shows that the tumor has uniform low-intensity in T2-weighted image and well demarcated,
it is absolutely benign leiomyoma. (A) T1-weighted image. (B) T2-weighted image. (C) Hysterectomy specimen of multiple benign leiomyomas.
Fig. 1 Magnetic resonance imaging (MRI) findings of typical benign leiomyomas. If MRI image
shows that the tumor has uniform low-intensity in T2-weighted image and well demarcated,
it is absolutely benign leiomyoma. (A) T1-weighted image. (B) T2-weighted image. (C) Hysterectomy specimen of multiple benign leiomyomas.
 Fig. 2 Magnetic resonance imaging findings of usual benign leiomyoma. Low-intensity in T2
with several furrow-like high-intensity strings also indicates benign leiomyoma. (A)
T1-weighted image. (B) T2-weighted image. (C) Cut section of typical benign leiomyoma.
Fig. 2 Magnetic resonance imaging findings of usual benign leiomyoma. Low-intensity in T2
with several furrow-like high-intensity strings also indicates benign leiomyoma. (A)
T1-weighted image. (B) T2-weighted image. (C) Cut section of typical benign leiomyoma.
 Fig. 3 Magnetic resonance imaging (MRI) findings of leiomyosarcoma. T2-weighted image with
heterogeneous high-intensity and fine granular shadow represents higher cellularity
of tumor cells. High-intensity in T1-weighted image suggests the presence of intratumoral
bleeding. These MRI findings strongly suggest that this tumor is not usual leiomyoma
but leiomyosarcoma. (A) T1-weighted image. (B) T2-weighted image. (C) Cut section
of typical leiomyosarcoma.
Fig. 3 Magnetic resonance imaging (MRI) findings of leiomyosarcoma. T2-weighted image with
heterogeneous high-intensity and fine granular shadow represents higher cellularity
of tumor cells. High-intensity in T1-weighted image suggests the presence of intratumoral
bleeding. These MRI findings strongly suggest that this tumor is not usual leiomyoma
but leiomyosarcoma. (A) T1-weighted image. (B) T2-weighted image. (C) Cut section
of typical leiomyosarcoma.
In addition, the direction of myoma growing is extremely various, such as submucosal,
subserosal, pedunculated, and retroperitoneal. This variation strongly influences
the operative procedure. In case of huge cervical myoma, the risk of ureteral injury
increases significantly. Therefore, preoperative planning of the surgery along with
looking at MRI findings is essential for the safe and reliable operation for the patient.
Surgical Steps
-
Opening Abdomen and Exploration
↓
-
Round Ligament and Peritoneum
↓
-
Infundibulopelvic Ligament and Adnexa
↓
-
Mobilization of Bladder
↓
-
Cardinal Ligament
↓
-
Amputation and Closure of Vagina
↓
-
Closing Abdomen
Explanation of Procedures
Abdominal hysterectomy has been indicated frequently for uterine fibroids. Due to
great variation in size and shape of the uterus due to the various development of
leiomyomata, the surgical procedure often deviates from the standard. However, gynecologic
surgeon should have some standard plan, and then modify it according to the anatomical
variation. Here, a standard operation technique is presented.
Opening Abdomen and Exploration
Patient is laid in the supine position and urethral catheter is inserted for continuous
bladder drainage. Keeping the bladder empty is very important for safe operation.
Trendelenburg position is not adopted in the standard. The vaginal cavity is prepared
by povidone-iodine before starting surgery.
Usually, the primary operator stands on the left side of patient. The assistant or
supervisor stands on the right side and in front of the operator, and plays an important
role both in appropriate traction of the uterus and in showing clearly the operative
field.
The operator incises the abdominal wall longitudinally from the pubis toward the umbilicus,
then the fascia, and the peritoneum. The midline and longitudinal incision is the
golden standard for pelvic surgery to facilitate the surgical procedure and to avoid
injury to vital structures, even in the modern era of laparoscopic surgery. Only if
the uterus is not so large, transverse incision is preferred.
The intestines are softly put upward and maintained with large gauze/sponge, and an
appropriate operative field is obtained by the self-retaining retractor.
Before starting surgery, the operator should examine the uterus, adnexae, and the
surrounding organs, and check whether unexpected abnormalities and/or adhesions exist
or not. If present, restoration of pelvic anatomy by release of adhesions is mandatory
for safer operation, except in the surgery for malignancy where the cancer cells exist
within the adhesion. If needed, the ascetic fluid is presented to pathology laboratory
for cytological examination.
Throughout the surgical procedure, the uterus is always maintained in the appropriate
traction by the assistant. Usually so that, a pair of long and straight Kocher clamps
are placed between the uterus and the adnexa. The tip of clamp should be at the avascular
and transparent space of anterior and posterior of broad ligaments, and should not
reach to the uterine vessels below. In the figures of this chapter, however, the clamp
was not used and the uterus was treated directly by the hand of assistant.
Round Ligament and Peritoneum
Since gynecologic surgery is essentially the operation in the retroperitoneum, it
is necessary for the operator to enter and explore the retroperitoneal cavity. To
do so, the operator must identify the entrance most easy to access, that is, the round
ligament. Even in case with distorted anatomy, round ligament can be identified easily.
Therefore, hysterectomy usually begins with the round ligament.
The operator grasps and lifts the right-sided round ligament using the forceps, finds
the transparent area beneath the ligament, and inserts twice the needle with No. 1–0
absorbable sutures. Then, tie and cut between the ligations with the Cooper scissors.
When cutting the ligaments or vessels, it is usually important to put the scissors
vertically to the ligament ([Fig. 4]) After the cut, air will enter into the retroperitoneal cavity, the loose connective
tissues fall down, and the cavity can be seen.
 Fig. 4 Ligation and cut of round ligament. (Reproduced with permission from Konishi I. Basic
procedure 2. In: Hiramatsu Y, Konishi I, Sakuragi N, Takeda S, eds. Mastering the
Essential Surgical Procedures OGS NOW, No.2 Total Abdominal Hysterectomy (Japanese).
Tokyo: Medical View; 2010:56–73. Copyright © Medical View).
Fig. 4 Ligation and cut of round ligament. (Reproduced with permission from Konishi I. Basic
procedure 2. In: Hiramatsu Y, Konishi I, Sakuragi N, Takeda S, eds. Mastering the
Essential Surgical Procedures OGS NOW, No.2 Total Abdominal Hysterectomy (Japanese).
Tokyo: Medical View; 2010:56–73. Copyright © Medical View).
Tips and Warnings
There are two kinds of surgical procedure for the treatment of ligament. The standard
is the clamp/cut first and then ligate, and another is suture/ligation first and then
cut. For treatment of the round and infundibulopelvic ligaments, the latter method
is usually employed due to its simplicity. In this case, however, the operator should
note that the suture tends to be loosen so that double ligation is needed.
Then, the operator incises the anterior leaf of broad ligament. Before incision, it
is important to identify the target endpoint for the incision, because erroneous and
deep dissection toward bladder induces bleeding. To identify the point, the operator
lifts the broad ligament of vesicouterine pouch, and identify the transitional and
freely movable area between the uterine and bladder serosa. Usually the target is
1 cm downward from the lower end of uterine serosa ([Fig. 5]). The incision line is concave-shaped from the round ligament to vesicouterine fossa.
Concave-shape is important to avoid unnecessary blood loss from the uterine vessels.
Before incision, the broad ligament is lifted with the forceps, and all of the subperitoneal
connective tissues are detached with Cooper scissors. This is very important to minimize
the bleeding. Then, the thin and transparent peritoneum is incised until the target.
 Fig. 5 Incision of anterior leaf of broad ligament. (Reproduced with permission from Konishi
I. Basic procedure 2. In: Hiramatsu Y, Konishi I, Sakuragi N, Takeda S, eds. Mastering
the Essential Surgical Procedures OGS NOW, No.2 Total Abdominal Hysterectomy (Japanese).
Tokyo: Medical View; 2010:56–73. Copyright © Medical View).
Fig. 5 Incision of anterior leaf of broad ligament. (Reproduced with permission from Konishi
I. Basic procedure 2. In: Hiramatsu Y, Konishi I, Sakuragi N, Takeda S, eds. Mastering
the Essential Surgical Procedures OGS NOW, No.2 Total Abdominal Hysterectomy (Japanese).
Tokyo: Medical View; 2010:56–73. Copyright © Medical View).
Next step is the incision of middle leaf of broad ligament toward upward. The same
dissection of loose connective tissues and incision toward the infundibulopelvic ligament
is performed.
Tips and Warnings
For a right-handed gynecologic surgeon, grasp ability of the left hand is essential
for handling forceps and treatment of ligaments. Therefore, it is important for young
students and residents to strengthen the grasping power of the left hand in the daily
practice and exercise.
Tips and Warnings
For peritoneal incision, the operator should tract the peritoneum intensively and
then attach the scissors almost vertically to the peritoneum, push slightly, and scrape
down all of the connective tissues beneath the peritoneum. Only a thin and transparent
peritoneum remains and can be incised without bleeding (O [good]). If the connective
tissues are incompletely detached, the veins and capillaries remain in the peritoneal
side, and so the incision results in bleeding (X [bad]). Such procedure is also important
in case of detachment of ureter, bladder, and rectum from the neighboring tissues
([Fig. 6]).
 Fig. 6 Incision of peritoneum. (Reproduced with permission from Konishi I. Basic procedure
2. In: Hiramatsu Y, Konishi I, Sakuragi N, Takeda S, eds. Mastering the Essential
Surgical Procedures OGS NOW, No.2 Total Abdominal Hysterectomy (Japanese). Tokyo:
Medical View; 2010:56–73. Copyright © Medical View).
Fig. 6 Incision of peritoneum. (Reproduced with permission from Konishi I. Basic procedure
2. In: Hiramatsu Y, Konishi I, Sakuragi N, Takeda S, eds. Mastering the Essential
Surgical Procedures OGS NOW, No.2 Total Abdominal Hysterectomy (Japanese). Tokyo:
Medical View; 2010:56–73. Copyright © Medical View).
Tips and Warnings
For identification of the right ureter, the operator should use the left hand, first
insert the index finger in the retroperitoneal side, and attach the thumb to the peritoneal
side of the posterior leaf of broad ligament. When touch the ureter by these fingers,
the operator feels the “snapping” sensation, being characteristic to ureter ([Fig. 7]). The operator should palpate the posterior leaf of broad ligament using his fingers,
and confirm the ureter running 2 to 4 cm apart from the ovarian artery and vein. Then,
insert the suture needle apart from the ureter ([Fig. 8]).
 Fig. 7 Identification of the right ureter. (Reproduced with permission from Konishi I. Basic
procedure 2. In: Hiramatsu Y, Konishi I, Sakuragi N, Takeda S, eds. Mastering the
Essential Surgical Procedures OGS NOW, No.2 Total Abdominal Hysterectomy (Japanese).
Tokyo: Medical View; 2010:56–73. Copyright © Medical View).
Fig. 7 Identification of the right ureter. (Reproduced with permission from Konishi I. Basic
procedure 2. In: Hiramatsu Y, Konishi I, Sakuragi N, Takeda S, eds. Mastering the
Essential Surgical Procedures OGS NOW, No.2 Total Abdominal Hysterectomy (Japanese).
Tokyo: Medical View; 2010:56–73. Copyright © Medical View).
 Fig. 8 Ligation and cut of infundibulopelvic ligament. (Reproduced with permission from
Konishi I. Basic procedure 2. In: Hiramatsu Y, Konishi I, Sakuragi N, Takeda S, eds.
Mastering the Essential Surgical Procedures OGS NOW, No.2 Total Abdominal Hysterectomy
(Japanese). Tokyo: Medical View; 2010:56–73. Copyright © Medical View).
Fig. 8 Ligation and cut of infundibulopelvic ligament. (Reproduced with permission from
Konishi I. Basic procedure 2. In: Hiramatsu Y, Konishi I, Sakuragi N, Takeda S, eds.
Mastering the Essential Surgical Procedures OGS NOW, No.2 Total Abdominal Hysterectomy
(Japanese). Tokyo: Medical View; 2010:56–73. Copyright © Medical View).
Infundibulopelvic Ligament and Adnexa
If the hysterectomy will be done along with salpingo-oophorectomy, the infundibulopelvic
ligament shall be cut. Here is the first important point to identify the running of
ureter to prevent the ureteral injury. The operator should palpate the posterior leaf
of broad ligament using his fingers, and confirm the ureter running 2 to 4 cm apart
from the ovarian artery and vein. The ligament is ligated using 1–0 absorbable sutures,
and is cut with Cooper scissors. Then, the upper stump of the ligament should be again
ligated for safety. To prevent postoperative bleeding, double ligation of the infundibulopelvic
ligament is always necessary in all gynecologic surgeries.
Tips and Warnings
For identification of the right ureter, the operator should use the left hand, first
insert the index finger in the retroperitoneal side, and attach the thumb to the peritoneal
side of the posterior leaf of broad ligament. When touch the ureter by these fingers,
the operator feels the “snapping” sensation, being characteristic to ureter. Thus,
the operator can identify the ureter running, and confirm the insertion point of the
suture needle is apart from the ureter.
If the adnexal organs are to be conserved, both the ovarian ligament and the tube
are clamped with the two forceps, cut, and then ligated with the 8-figure sutures.
Double ligation is also needed here, since the first suture tends to slide off from
the stump of ligament. Recently, only salpingectomy is frequently performed considering
the possible tubal origin of ovarian cancer. In this case, mesosalpinx is clamped
several times, cut, and ligated.
Then, the posterior part of broad ligament is incised. Here, it is also important
to determine the target endpoint of incision, that is the uterine origin of sacrouterine
ligament. The operator should tract the peritoneum intensively and then attach the
scissors almost vertically to the peritoneum, push slightly, and scrape down all of
the connective tissues beneath the peritoneum. Sometimes, the operator can see here
the running of the ureter ([Fig. 9]).
 Fig. 9 Incision of posterior leaf of broad ligament. (Reproduced with permission from Konishi
I. Basic procedure 2. In: Hiramatsu Y, Konishi I, Sakuragi N, Takeda S, eds. Mastering
the Essential Surgical Procedures OGS NOW, No.2 Total Abdominal Hysterectomy (Japanese).
Tokyo: Medical View;2010:56–73. Copyright © Medical View).
Fig. 9 Incision of posterior leaf of broad ligament. (Reproduced with permission from Konishi
I. Basic procedure 2. In: Hiramatsu Y, Konishi I, Sakuragi N, Takeda S, eds. Mastering
the Essential Surgical Procedures OGS NOW, No.2 Total Abdominal Hysterectomy (Japanese).
Tokyo: Medical View;2010:56–73. Copyright © Medical View).
Tips and Warnings
While incising the peritoneum, the operator should tract it intensively and then attach
the scissors almost vertically to the peritoneum, push slightly, and scrape down all
of the connective tissues beneath the peritoneum. Only a thin and transparent peritoneum
remains and can be incised without bleeding. If the connective tissues are incompletely
detached, the veins and capillaries remain in the peritoneal side, and so the incision
results in bleeding. Such procedure is also important in case of detachment of ureter,
bladder, and rectum from the neighboring tissues.
All of the above procedures are done for the left-sided round ligament, broad ligament,
and infundibulopelvic ligament or adnexa. Now, all of the peritoneal surface except
the cul-de-sac peritoneum are incised, and the uterus is now almost free from the
serosa. From now, the surgical procedures in the retroperitoneal space start.
Mobilization of Bladder
It is important to start the bladder mobilization at the midline of cervix, to prevent
bleeding from the lateral-sided vesicouterine ligaments. Before the start of mobilization
of bladder, therefore, the operator should palpate the cervix from both anterior and
posterior sides of uterus to confirm the position of the cervix. This is because the
cervix frequently deviates laterally due to fibroids or adhesion ([Fig. 10]). Palpation is also essential to assess the height of lower end of cervix or vaginal
fornix.
 Fig. 10 Palpation of uterine cervix. (Reproduced with permission from Konishi I. Basic procedure
2. In: Hiramatsu Y, Konishi I, Sakuragi N, Takeda S, eds. Mastering the Essential
Surgical Procedures OGS NOW, No.2 Total Abdominal Hysterectomy (Japanese). Tokyo:
Medical View; 2010:56–73. Copyright © Medical View).
Fig. 10 Palpation of uterine cervix. (Reproduced with permission from Konishi I. Basic procedure
2. In: Hiramatsu Y, Konishi I, Sakuragi N, Takeda S, eds. Mastering the Essential
Surgical Procedures OGS NOW, No.2 Total Abdominal Hysterectomy (Japanese). Tokyo:
Medical View; 2010:56–73. Copyright © Medical View).
When the operator lifts the cut-end of anterior leaf of broad ligament, the connective
tissues in the vesicouterine pouch spontaneously sink, where the first incision should
be made in the center of cervix. Pushing the Cooper scissors vertically to cervix
and cutting the connective tissues will disclose the surface of cervix, which is white,
smooth, and shining. Then, the connective tissues and the bladder are dissected downward
using the scissors from the cervix completely until the portion of lower end of cervix
([Fig. 11]). Then, the operator will treat the lateral vesicouterine ligaments. Loose connective
tissues on the surface of ligaments are carefully removed. Since it is rich in vasculature,
the dissection should not be done deeply to avoid bleeding. The bladder is now mobilized
to the appropriate level of height, ∼1 cm below the vaginal fornix.
 Fig. 11 Mobilization of bladder. To prevent bleeding from the lateral vesicouterine ligaments,
it is important to start the dissection at the midline of cervix. When lifting the
anterior leaf of broad ligament in the center, the connective tissues in the vesicouterine
pouch sink. Pushing the Cooper scissors vertically to cervix and cutting the sinking
tissues will disclose the surface of cervix. Then, the connective tissues and the
bladder are dissected downward using the scissors. (Reproduced with permission from
Konishi I. Basic procedure 2. In: Hiramatsu Y, Konishi I, Sakuragi N, Takeda S, eds.
Mastering the Essential Surgical Procedures OGS NOW, No.2 Total Abdominal Hysterectomy
(Japanese). Tokyo: Medical View; 2010:56–73. Copyright © Medical View).
Fig. 11 Mobilization of bladder. To prevent bleeding from the lateral vesicouterine ligaments,
it is important to start the dissection at the midline of cervix. When lifting the
anterior leaf of broad ligament in the center, the connective tissues in the vesicouterine
pouch sink. Pushing the Cooper scissors vertically to cervix and cutting the sinking
tissues will disclose the surface of cervix. Then, the connective tissues and the
bladder are dissected downward using the scissors. (Reproduced with permission from
Konishi I. Basic procedure 2. In: Hiramatsu Y, Konishi I, Sakuragi N, Takeda S, eds.
Mastering the Essential Surgical Procedures OGS NOW, No.2 Total Abdominal Hysterectomy
(Japanese). Tokyo: Medical View; 2010:56–73. Copyright © Medical View).
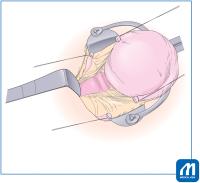 Fig. 12 Application of L-shaped retractor. (Reproduced with permission from Konishi I. Basic
procedure 2. In: Hiramatsu Y, Konishi I, Sakuragi N, Takeda S, eds. Mastering the
Essential Surgical Procedures OGS NOW, No.2 Total Abdominal Hysterectomy (Japanese).
Tokyo: Medical View; 2010:56–73. Copyright © Medical View).
Fig. 12 Application of L-shaped retractor. (Reproduced with permission from Konishi I. Basic
procedure 2. In: Hiramatsu Y, Konishi I, Sakuragi N, Takeda S, eds. Mastering the
Essential Surgical Procedures OGS NOW, No.2 Total Abdominal Hysterectomy (Japanese).
Tokyo: Medical View; 2010:56–73. Copyright © Medical View).
The L-shaped retractor is placed at the detached portion, pushing the bladder downward
([Fig. 12]).
Usually, mobilization of rectum from the uterus is not necessary, because the operator
can directly approach the posterior wall of vagina through the cul-de-sac peritoneum.
In the case complicated with endometriosis, however, the cul-de-sac is closed and
the rectum is adhered to the vagina and cervix. In such case, the dissection of the
rectum from the cervix is needed. Before this procedure, the operator should identify
the sacrouterine ligament for anatomical understanding, and the ligaments are cut
and ligated before hysterectomy. Cutting the sacrouterine ligament will always facilitate
the movability of uterus for easier hysterectomy.
Cardinal Ligament
Now, it is the time for clamping and cutting the uterine vessels of cardinal ligament.
Before that, it is necessary to carefully dissect and remove the loose connective
tissue on the uterine artery and vein. Removal of the connective tissues on the vesicouterine
ligament is also important for prevention of ureteral injury. Thus, the ascending
branch of the uterine artery and veins will be skeletonized ([Fig. 13]). To avoid the ureteral injury, it is very important, by the assistant, to keep
the uterus in the traction upward and to push the bladder downward using L-shaped
retractor. And then, the operator should palpate the ureter running along the posterior
leaf of broad ligament, to identify the level of ureter entering the cardinal ligament
1 to 3 cm lateral from the cervix and 2 to 4 cm below the uterine artery.
 Fig. 13 Dissection of connective tissues on cardinal ligament. (Reproduced with permission
from Konishi I. Basic procedure 2. In: Hiramatsu Y, Konishi I, Sakuragi N, Takeda
S, eds. Mastering the Essential Surgical Procedures OGS NOW, No.2 Total Abdominal
Hysterectomy (Japanese). Tokyo: Medical View; 2010:56–73. Copyright © Medical View).
Fig. 13 Dissection of connective tissues on cardinal ligament. (Reproduced with permission
from Konishi I. Basic procedure 2. In: Hiramatsu Y, Konishi I, Sakuragi N, Takeda
S, eds. Mastering the Essential Surgical Procedures OGS NOW, No.2 Total Abdominal
Hysterectomy (Japanese). Tokyo: Medical View; 2010:56–73. Copyright © Medical View).
In general, the cardinal ligament including uterine artery and veins will be cut two
times until reaching the vaginal fornix (two-steps clamping for cardinal ligament).
The first clamp is placed at an angle of 45° for the upper half of the cervix, so
that the tip of clamp reaching 1 cm below the height of internal os of the uterus.
At clamping, it is desirable to have the clamp slide off the surface of the cervix,
to all of vessels be completely clamped ([Fig. 14]). When the first clamp is placed, the operator is asked to palpate again the ureter,
and will confirm the distance between the tip of clamp and the ureter, that is usually
2 to 3 cm apart. Another upper clamp is then placed to prevent backflow bleeding from
the uterus. Then, the upper half of ligament is cut with Cooper scissors, needled,
and ligated with 1–0 absorbable suture. The cut-end of uterine artery needs double
ligation ([Fig. 15]).
 Fig. 14 Cut and ligation of cardinal ligament. Cardinal ligament including uterine artery
and veins is cut two times until reaching the vaginal fornix (two-step clamping).
First, the operator should palpate the ureter running. Then, the first clamp is placed
at an angle of 45° for the upper half of the cervix, so that the tip of clamp reaches
1 cm below the height of internal os of uterus. At clamping, it is desirable to have
the clamp slide off the surface of the cervix, to all of vessels be completely clamped.
Another upper clamp is placed to prevent backflow bleeding from the uterus. The operator
is asked to palpate again the ureter, and confirm the distance between the tip of
clamp and the ureter, that is usually 2 to 3 cm apart. Then, the upper half of ligament
is cut with Cooper scissors. (Reproduced with permission from Konishi I. Basic procedure
2. In: Hiramatsu Y, Konishi I, Sakuragi N, Takeda S, eds. Mastering the Essential
Surgical Procedures OGS NOW, No.2 Total Abdominal Hysterectomy (Japanese). Tokyo:
Medical View; 2010:56–73. Copyright © Medical View).
Fig. 14 Cut and ligation of cardinal ligament. Cardinal ligament including uterine artery
and veins is cut two times until reaching the vaginal fornix (two-step clamping).
First, the operator should palpate the ureter running. Then, the first clamp is placed
at an angle of 45° for the upper half of the cervix, so that the tip of clamp reaches
1 cm below the height of internal os of uterus. At clamping, it is desirable to have
the clamp slide off the surface of the cervix, to all of vessels be completely clamped.
Another upper clamp is placed to prevent backflow bleeding from the uterus. The operator
is asked to palpate again the ureter, and confirm the distance between the tip of
clamp and the ureter, that is usually 2 to 3 cm apart. Then, the upper half of ligament
is cut with Cooper scissors. (Reproduced with permission from Konishi I. Basic procedure
2. In: Hiramatsu Y, Konishi I, Sakuragi N, Takeda S, eds. Mastering the Essential
Surgical Procedures OGS NOW, No.2 Total Abdominal Hysterectomy (Japanese). Tokyo:
Medical View; 2010:56–73. Copyright © Medical View).
 Fig. 15 Cut and ligation of the first clamp for cardinal ligament. (Reproduced with permission
from Konishi I. Basic procedure 2. In: Hiramatsu Y, Konishi I, Sakuragi N, Takeda
S, eds. Mastering the Essential Surgical Procedures OGS NOW, No.2 Total Abdominal
Hysterectomy (Japanese). Tokyo: Medical View; 2010:56–73. Copyright © Medical View).
Fig. 15 Cut and ligation of the first clamp for cardinal ligament. (Reproduced with permission
from Konishi I. Basic procedure 2. In: Hiramatsu Y, Konishi I, Sakuragi N, Takeda
S, eds. Mastering the Essential Surgical Procedures OGS NOW, No.2 Total Abdominal
Hysterectomy (Japanese). Tokyo: Medical View; 2010:56–73. Copyright © Medical View).
Then the second clamp is placed along the cervix for hemostasis from small veins from
the ligament. The tip of clamp reaches the level of the vaginal fornix, and then the
lower half of cardinal ligament is cut and sutured ([Fig. 16]). During cutting the cardinal ligament here, the operator can recognize the plane
demarcating the cervix from the ligament. When entered this true plane, especially
near the sacrouterine ligament, the operator feels very easy and smooth for the cutting.
The cutting has finally reached the level of vaginal fornix. It is important to avoid
too deep cutting into the paracolpium, which results in the substantial amount of
bleeding.
 Fig. 16 Cut and ligation of the second clamp for cardinal ligament. (Reproduced with permission
from Konishi I. Basic procedure 2. In: Hiramatsu Y, Konishi I, Sakuragi N, Takeda
S, eds. Mastering the Essential Surgical Procedures OGS NOW, No.2 Total Abdominal
Hysterectomy (Japanese). Tokyo: Medical View; 2010:56–73. Copyright © Medical View).
Fig. 16 Cut and ligation of the second clamp for cardinal ligament. (Reproduced with permission
from Konishi I. Basic procedure 2. In: Hiramatsu Y, Konishi I, Sakuragi N, Takeda
S, eds. Mastering the Essential Surgical Procedures OGS NOW, No.2 Total Abdominal
Hysterectomy (Japanese). Tokyo: Medical View; 2010:56–73. Copyright © Medical View).
After the same procedure is done for the left side, it is the time to proceed the
final step for hysterectomy. Usually, it is not necessary to cut the sacrouterine
ligament, which will be cut simultaneously during the amputation of vagina.
Tips and Warnings
To avoid injury of the ureter during the ligation of cardinal ligament, such “two-steps
clamping” is essential. Each step eventually moves the ureter laterally apart from
the cervix and vagina, and so this is safer compared with one-step clamping. In case
of longer cervix, three-steps clamping shall be considered.
However, too many steps of clamp and ligation for cardinal ligament tend to produce
the bleeding between many cut-ends of ligament. Thus, two or three clamps might be
ideal for the treatment of cardinal ligament.
The operator can palpate the running ureter anytime during the surgical procedure,
and should confirm the distance between the ligation and the ureter.
When severe endometriosis or cervical myoma lifts the ureter running close to the
uterus, the operator should denude and isolate the ureter from the posterior leaf
of broad ligament, and mark it using yellow-colored tape.
Amputation and Closure of Vagina
A large gauze is placed in the Douglas pouch, and the transitional area between the
cervix and vagina is again palpated. Then, the sharp scalpel will be inserted vertically
into the uppermost portion of the anterior wall of vagina ([Fig. 17]). The portio and vagina are prepared by povidone-iodine, and a gauze is inserted
into the vaginal cavity. The long straight Kocher clamps are sequentially placed on
the cut-end of vaginal wall for hemostasis ([Fig. 18]). The sacrouterine ligament is simultaneously cut and clamped together with vaginal
wall. If the curved Kelly clamp is placed along the vaginal fornix as landmark, it
is easier to cut the vagina with the scalpel or scissors along the curve of clamp.
The vaginal vault is closed with Z-figure sutures ([Figs. 19] and [20]).
 Fig. 17 Incision of vaginal wall. (Reproduced with permission from Konishi I. Basic procedure
2. In: Hiramatsu Y, Konishi I, Sakuragi N, Takeda S, eds. Mastering the Essential
Surgical Procedures OGS NOW, No.2 Total Abdominal Hysterectomy (Japanese). Tokyo:
Medical View; 2010:56–73. Copyright © Medical View).
Fig. 17 Incision of vaginal wall. (Reproduced with permission from Konishi I. Basic procedure
2. In: Hiramatsu Y, Konishi I, Sakuragi N, Takeda S, eds. Mastering the Essential
Surgical Procedures OGS NOW, No.2 Total Abdominal Hysterectomy (Japanese). Tokyo:
Medical View; 2010:56–73. Copyright © Medical View).
 Fig. 18 Placing clamp along vaginal fornix. (Reproduced with permission from Konishi I. Basic
procedure 2. In: Hiramatsu Y, Konishi I, Sakuragi N, Takeda S, eds. Mastering the
Essential Surgical Procedures OGS NOW, No.2 Total Abdominal Hysterectomy (Japanese).
Tokyo: Medical View; 2010:56–73. Copyright © Medical View).
Fig. 18 Placing clamp along vaginal fornix. (Reproduced with permission from Konishi I. Basic
procedure 2. In: Hiramatsu Y, Konishi I, Sakuragi N, Takeda S, eds. Mastering the
Essential Surgical Procedures OGS NOW, No.2 Total Abdominal Hysterectomy (Japanese).
Tokyo: Medical View; 2010:56–73. Copyright © Medical View).
 Fig. 19 Suture of vaginal wall. The sacrouterine ligament is simultaneously cut and clamped
together with vaginal wall. Careful suture is important at the lateral end of vagina,
close to the stump of cardinal ligament. (Reproduced with permission from Konishi
I. Basic procedure 2. In: Hiramatsu Y, Konishi I, Sakuragi N, Takeda S, eds. Mastering
the Essential Surgical Procedures OGS NOW, No.2 Total Abdominal Hysterectomy (Japanese).
Tokyo: Medical View; 2010:56–73. Copyright © Medical View).
Fig. 19 Suture of vaginal wall. The sacrouterine ligament is simultaneously cut and clamped
together with vaginal wall. Careful suture is important at the lateral end of vagina,
close to the stump of cardinal ligament. (Reproduced with permission from Konishi
I. Basic procedure 2. In: Hiramatsu Y, Konishi I, Sakuragi N, Takeda S, eds. Mastering
the Essential Surgical Procedures OGS NOW, No.2 Total Abdominal Hysterectomy (Japanese).
Tokyo: Medical View; 2010:56–73. Copyright © Medical View).
 Fig. 20 Closure of vagina. The vaginal vault is closed with Z-figure sutures. (Reproduced
with permission from Konishi I. Basic procedure 2. In: Hiramatsu Y, Konishi I, Sakuragi
N, Takeda S, eds. Mastering the Essential Surgical Procedures OGS NOW, No.2 Total
Abdominal Hysterectomy (Japanese). Tokyo: Medical View; 2010:56–73. Copyright © Medical
View).
Fig. 20 Closure of vagina. The vaginal vault is closed with Z-figure sutures. (Reproduced
with permission from Konishi I. Basic procedure 2. In: Hiramatsu Y, Konishi I, Sakuragi
N, Takeda S, eds. Mastering the Essential Surgical Procedures OGS NOW, No.2 Total
Abdominal Hysterectomy (Japanese). Tokyo: Medical View; 2010:56–73. Copyright © Medical
View).
Tips and Warnings
The most frequent point with ureteral injury is during hemostasis against the bleeding
from surrounding the vaginal vault. Condition of traction for uterus has gone after
hysterectomy, and without traction, the vaginal vault has come very close to the ureter
running. Thus, hemostatic sutures without traction of the vaginal vault, near the
cut-ends of cardinal ligament, tend to involve the ureteral injury. Therefore, to
prevent the injury, the operator should restore the condition of traction; tract again
the vaginal vault upward and push the bladder downward. This procedure will move the
ureter laterally again. Then, the operator should identify the small point of bleeding
and place the superficial hemostatic suture. The operator should not suture deeply
into the ligament.
Closing Abdomen
The retroperitoneal space is washed by warm saline, and is confirmed for no bleedings
and no foreign bodies. Counting the number of gauze is completed. Pelvic peritoneum
is sutured with 2–0 continuous sutures, and completely closed. The cut-ends of ligaments
are placed retroperitoneally. Care must be taken not to injure the ureter during the
continuous suture.
The retractor and intraperitoneal sponge-gauze are removed, and the intestines are
restored to normal position. The abdomen is closed with each suture for the peritoneum,
fascia, and skin.
Tips and Warnings
The author always tells the students, “When bleeding occurs, do not immediately stop
the bleeding with panicking clamp or self-missing suture.” Prompt clamp or suture
tends to involve the neighboring organs, resulting in the postsurgical complications
such as injury or fistula of the urinary tract or the intestinal tract. Therefore,
first, push the gauze to the bleeding area, maintain transiently the hemostatic condition,
and wait a little bit. During the wait, the operator can escape from the panicking
time and will consider the most appropriate recovery. Small bleeding may stop and
only the major bleeding remains. Sometimes, further dissection of surrounding tissues
is needed along with keeping gauze pushing for the bleeding. Thus, the operator can
easily find the bleeding point or vessels, and can perform the proper hemostasis using
the pin-point clamp or suture without involving the neighboring organs. This is the
most important for gynecologic surgeons treating the pelvic organs having many dilated
vessels.





