

RSS-Feed abonnieren
DOI: 10.1055/s-0042-1756638
The Relative Lymphocyte Count is Lower when the Etiological Agent in Pott Disease is Successfully Isolated[*]
Artikel in mehreren Sprachen: português | EnglishAutor*innen

Abstract
Objective To describe the clinico-epidemiological, laboratory, and radiological characteristics of tuberculous spondylodiscitis in the Brazilian population, and to assess whether there are differences between patients in whom the etiological agent in Pott disease was isolated or not.
Methods Patients diagnosed with tuberculosis (TB) of the spine (Pott disease) underwent follow-up between 2009 and 2019 at a quaternary hospital and were divided into 2 groups: successful isolation (SI) of the etiological agent (through bacilloscopy, culture, or positive molecular rapid test) and unsuccessful isolation (UI) of the etiological agent.
Results From a total of 26 patients diagnosed with TB of the spine, 21 (80.7%) were male, with a mean age of 40 ± 22.5 years. The average lymphocyte counts were higher in the UI group (25.35 ± 13.08; p = 0.025) compared to the SI group (14.18 ± 7.48). Moreover, the monocyte/lymphocyte ratio was lower in the UI group (0.39 ± 0.22; p = 0.009) than in the SI group (0.89 ± 0.65). Relative lymphocyte counts higher than or equal to 16.7 had a sensitivity of 76.9% and specificity of 62.5% in the UI group. Values higher than or equal to 0.58 for the monocyte/lymphocyte ratio showed a sensitivity of 84.6% and specificity of 75.0% in the UI group.
Conclusion No differences were observed regarding the clinico-epidemiological and radiological characteristics of the two experimental groups. However, the UI group had higher lymphocyte counts and a lower monocyte/lymphocyte ratio.
Introduction
Tuberculosis (TB) is one of the oldest infectious diseases that affect humans. About 10.4 million new cases a year are estimated worldwide, but only 1.3 million are diagnosed, and 2% are in the spine.[1] [2] It is one of the top ten global causes of death.[3]
Nonspecific symptoms and insidious onset characterize the clinical picture of the disease. The time from the onset of symptoms to the diagnosis can vary from 4 to 11 months.[4] [5] Axial pain is the most usual symptom, but patients may experience fever, constitutional symptoms, respiratory symptoms, and neurological deficit.[1] [4] The diagnosis consists of the clinical picture associated with specific aspects in the imaging exams and isolation of the microbiological agent and/or compatible anatomopathological exam, and/or a positive therapeutic test.[6] [7]
Tuberculosis patients have lymphocytopenia due to a decrease in CD4 T-lymphocytes. There is no change, however, in CD8 T-lymphocytes. This clinical picture is reversible and normalizes after recovery.[8] The patients manifest immunological abnormalities such as a failure in the proliferation of CD4 T-lymphocytes and interferon-gamma production in response to mycobacterial antigens.[9]
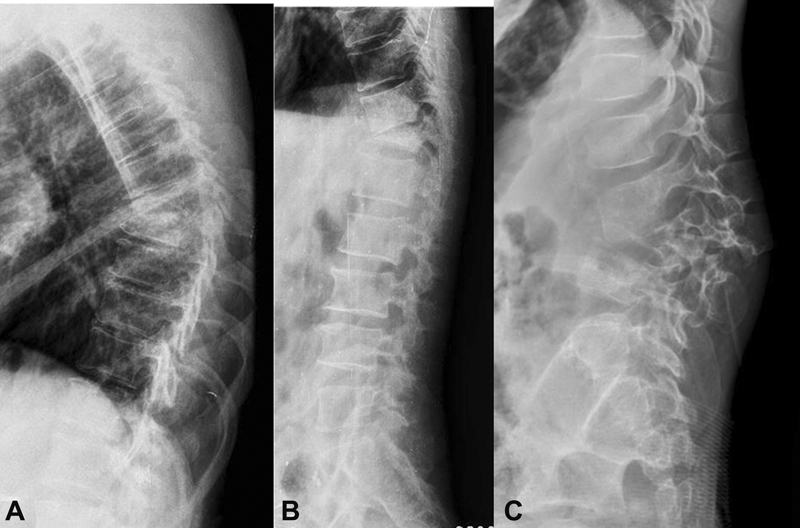
The radiographs of Pott disease initially show radiolucency, loss of definition and erosion of end plates, destruction of the vertebral body, and loss of disc height[10] ([Fig. 1]). Computed tomography (CT) improves the evaluation of the radiographic findings and of the extent of the lesion ([Fig. 2]). However, magnetic resonance imaging (MRI) is the most sensitive and specific imaging exam. The signal strength decreases in vertebral bodies in the T1-weighted sequences and increases in T2-weighted and short tau inversion recovery (STIR)-weighted images. The use of contrast, such as gadolinium, differentiates the infected from the uninfected areas[11] [12] ([Fig. 3]). The anatomopathological examination reveals granuloma with giant cells and caseous necrosis ([Fig. 4]). Isolation of the agent is possible through a specific culture for mycobacteria, a bacilloscopy to identify acid-fast bacilli (AFB), or a rapid molecular test for TB (RMT-TB).[2] [6] The treatment involves multiple medications and lasts at least 12 months, and may be extended due to resistant cases or adverse events. Surgery is indicated in patients with instability, neurological deficit, deformity, and large abscesses.[4] [6]



The patients present a characteristic clinico-radiographic picture; however, delay in establishing the diagnosis is usual. The diagnosis involves a positive therapeutic test. In an extensive series of 967 patients,[13] isolation of the etiologic agent occurred in only 16.6% of the cases. This shows that some patients meet the diagnostic criteria and respond to treatment until they are cured, but do not have the etiologic agent isolated.[2]
The objectives of the present study are to describe the clinic- epidemiological, radiological, and laboratory characteristics of tuberculous spondylodiscitis in a sample of the Brazilian population, and to assess if there are differences among patients in whom isolation of the etiologic agent occurred or not.
Materials and Methods
The present is a cross-sectional study involving a non-probabilistic sample of all patients who underwent outpatient follow-up between 2009 and 2019 in a quaternary hospital. The data were extracted from medical records, laboratory tests, and imaging exams. Patients diagnosed with TB of the spine, regardless of the age group and gender, were included. We excluded patients with incomplete data, any other type of infection, or previous spinal surgery. The institutional Ethics Committee approved the study (under CAAE 92596718.2.0000.5479).
The diagnosis of TB of the spine was established through the typical clinical characteristics and specific imaging tests, as well as the presence of at least one of the following criteria: isolation of the etiological agent, compatible anatomopathological examination, or positive therapeutic test.[6] The clinical criteria considered the presence of at least two of the following symptoms: back pain, pain on local palpation, night sweats, weight loss (at least 10% of body weight in the previous 6 months), fatigue, malaise, or fever (temperature greater than or equal to 37.8° Celsius).[6] The radiological criteria were established considering radiographs of the spine on the posteroanterior and lateral views, with the presence of at least four of the following findings: radiolucency, loss of definition and/or erosion of the vertebral plateaus, loss of height of the intervertebral disc space, vertebral geodes, bone sequestration, sclerosis, anterior wedging, and destruction of the vertebral body.[11] The criteria also included CT scans with at least one of the following findings: paravertebral masses and abscesses, calcifications, and involvement of posterior elements.[11] The MRI criteria were hyposignal of the affected vertebral body on T1-weighted images and hypersignal on T2- and STIR-weighted images, decreased intervertebral disc space, and loss of definition of disc boundaries, and hypersignal of the intervertebral disc on T2-weighted images.[11] [14]
Magnetic resonance images were obtained using a 1.5-Tesla device (Magnetom Symphony, Siemens Healthineers AG, Erlangen, Germany) with T1-, T2-, STIR-weighted cuts and with contrast added. The images were analyzed by an orthopedist and a radiologist who was a spine specialist with at least five years of experience.
The isolation of the etiological agent involved the presence of AFB by the Ziehl-Neelsen method, the RMT-TB, and mycobacteria culture (Löwenstein- Jensen or Ogawa-Kudoh).[6]
The anatomopathological examination was considered compatible in the case of the proliferation of epithelioid cells with the formation of confluent granulomas and Langhans giant cells with central foci of caseous necrosis around lymphocytic infiltrate upon staining with hematoxylin and eosin (H&E).[15] The therapeutic test was considered positive in cases in which the clinical and radiological findings were suggestive of TB, but the anatomopathological examination was not compatible with the disease and isolation of the etiological agent was not possible.[15] The cured cases were considered positive, and were defined through clinical improvement after the treatment for TB (absence or significant improvement in pain, sweating, and fever), and through the normalization of the inflammatory tests, of the erythrocyte sedimentation rate (ESR), and of the levels of C-reactive protein (CRP). All of the cured cases should remain stable for at least one month of observation.[16]
Variables Studied
The demographic and epidemiological variables analyzed were age, gender, presence of diabetes mellitus, chronic kidney disease or neoplasia, chronic use of corticosteroids for at least six months at an immunosuppressive dose in the last twelve months, HIV infection, pulmonary and/or extrapulmonary TB (except for spine TB) and type of household (urban, rural or free area).
The clinical characteristics from symptom onset to diagnosis were pain, score on the Visual Analogue Scale for Pain (VAS, from 0 to 10), respiratory symptoms (cough and dyspnea), constitutional symptoms (weight loss of at least 10% in the last 6 months, fatigue, malaise), fever (temperature greater than or equal to 37.8° Celsius), and neurological status at baseline and after 6 months (measured through the American Spinal Cord Injury Association [ASIA] impairment scale).
The laboratory variables at the time of diagnosis were hemoglobin level, leukocyte count, lymphocyte count, monocyte count, monocyte/lymphocyte ratio, ESR, and the levels of CRP, lactic dehydrogenase (DHL), creatinine, total proteins, and albumin. The biopsy was percutaneous, open, or guided by CT. The microbiological aspects studied were reactive tuberculin skin test (induration greater than or equal to 5 mm with the Mantoux technique),[17] bacilloscopy (presence of AFB using the Ziehl-Neelsen stain), compatible anatomopathological examination, culture (Lowenstein-Jensen medium), and RMT-TB with an evaluation of resistance to rifampcin (GeneXpert MTB/RIF, Cepheid, Sunnyvale, CA, United States).
Through MRI scans, we established the location of the Pott disease (cervical, thoracic, thoracolumbar transition, and lumbosacral), the number of levels affected, the presence of disease in multiple levels (3 or more), involvement of more than 2 vertebrae at adjacent levels, presence of collection within a vertebra or in adjacent paravertebral tissues, subligamentous spread, destruction of the vertebral body with a decrease in height greater than 50%, involvement of non-contiguous levels in different regions of the spine, hypointensity on T1 and hyperintensity on T2, irregularity of the margins of the end plates of the vertebral bodies on T2- and STIR-weighted sequences, and invasion of the epidural space by caseation or granulation tissue.[12]
The treatment variables included type (non-surgical or surgical), duration (months), drug and period of use (months), resistance to any drug in the treatment regimen for TB, presence of monoresistance or multidrug resistance (resistance to at least isoniazid and rifampcin), and the presence of complications (surgical site infection, neurological deficit, chronic pain after cure, and death).[6]
The patients were divided into two groups: those in whom the etiologic agent was successfully isolated (SI) or those with unsuccessful isolation (UI) through bacilloscopy and/or negative culture and/or RMT-TB. All cases in the study met the cure criteria.
Statistical Analyses
The categorical variables were expressed as frequencies (numbers and percentages), and the quantitative variables, as summary measures (mean, standard deviation, minimum and maximum values). The receiver operating characteristic (ROC) curve was used for the variables with a statistically significant difference regarding the assessment of the sensitivity and specificity, using as the gold standard the distribution of the values of that variable in the UI group. The data obtained were submitted to a statistical evaluation, using the Statistical Package for the Social Sciences (SPSS for Windows, SPSS Inc., Chicago, IL, United States) software, version 13.0. The level of statistical significance adopted was values of p lower than or equal to 0.05.
Results
The study included a total of 26 patients with TB of the spine, with 21 (80.7%) male subjects, and a mean age of 40 ± 22.5 years ([Table 1]). Axial pain was the most prevalent symptom (84.6%), with a mean VAS score of 6.6 ± 2.6. The mean time from symptom onset to diagnosis was of 23.8 ± 24.8 weeks. The mean score on the ASIA scale ranged from 172.0 in the first assessment to 202.0 after 6 months.0. Biopsy was performed in all patients: 11 were open, 10 were percutaneous, and 5 were guided by CT.
|
N |
SI |
% |
UI |
% |
p-value |
|
|---|---|---|---|---|---|---|
|
N |
26 |
9 |
34.6 |
17 |
65.4 |
|
|
Age (mean and standard deviation in years) |
40 ± 22.5 |
42 |
− |
40 |
− |
0.578** |
|
Gender |
26 |
9 |
34.6 |
17 |
65.4 |
1.000* |
|
Male |
21 |
8 |
38.1 |
13 |
61.9 |
|
|
Female |
5 |
1 |
20.0 |
4 |
80.0 |
|
|
Diabetes mellitus |
4 |
1 |
25.0 |
3 |
75.0 |
1.000* |
|
Chronic kidney disease |
1 |
0 |
0.0 |
1 |
100.0 |
1.000* |
|
Neoplasia |
2 |
0 |
0.0 |
2 |
100.0 |
1.000* |
|
Duration of the corticotherapy (months) |
1 |
0 |
0.0 |
1 |
100.0 |
1.000* |
|
Type of Household |
26 |
9 |
34.6 |
17 |
65.4 |
0.216** |
|
Urban |
12 |
2 |
16.7 |
10 |
83.3 |
|
|
Rural |
14 |
6 |
42,9 |
8 |
57.1 |
|
|
Treatment |
26 |
9 |
34.62 |
17 |
65.38 |
0.078* |
|
Non-surgical |
17 |
4 |
44.44 |
13 |
76.47 |
|
|
Surgical |
9 |
5 |
55.56 |
4 |
23.53 |
|
|
Time until cure (months) |
14.2 |
11.25 |
14.24 |
0.613** |
||
|
Location |
1.000* |
|||||
|
Thoracic |
13 |
5 |
38.5 |
8 |
61.5 |
|
|
Lumbar |
13 |
4 |
30.8 |
9 |
69.2 |
|
|
Levels |
0.316*** |
|||||
|
1 |
21 |
7 |
33.3 |
14 |
66.7 |
|
|
2 |
2 |
1 |
50.0 |
1 |
50.0 |
|
|
3 |
2 |
− |
− |
2 |
100.0 |
|
|
4 |
1 |
1 |
− |
− |
− |
|
|
Multiple-level disease |
3 |
1 |
33.3 |
2 |
66.7 |
1.000* |
|
Complications |
10 |
5 |
50 |
5 |
50 |
0.16*** |
|
Death |
1 |
0 |
0 |
1 |
100 |
|
|
Neurological deficit |
8 |
4 |
50 |
4 |
50 |
|
|
Chronic pain |
1 |
1 |
100 |
0 |
0 |
|
|
Postoperative infection |
0 |
0 |
0 |
0 |
0 |
|
|
None |
16 |
4 |
25 |
12 |
75 |
The etiologic agent was isolated (through culture and/or sputum-smear bacilloscopy and/or positive RMT-TB) in 9 cases. In the remaining 17 patients, isolation was not possible, and the diagnosis was established through a positive therapeutic test in 11 cases and through an anatomopathological examination compatible with TB in 6 cases ([Table 2]).
|
n |
% |
|
|---|---|---|
|
Isolation of the etiologic agent |
9 |
34.62 |
|
Pathology |
6 |
23.08 |
|
Therapeutic testing |
11 |
42.31 |
Regarding the tests that led to the diagnosis, 5 (19.23%) were bacilloscopies, 11 (42.31%) were anatomopathological tests, 5 (19.23%) were cultures, and 7 (26.92%) were RMT-TBs. It is important to note that, in the cases in which the agent was isolated, , if one of these tests were positive, one of the other two or both were also positive.
We identified the exclusive form of TB of the spine (Pott disease) in 14 patients, and it was associated with pulmonary TB in 7 cases. The disseminated form (2 or more extrapulmonary sites affected) was identified in 5 patients: compromise of the spine and lymph node (2), of the spine and knee (2), and of the spine and pleura (1).[18]
Moreover, the lumbar region was affected in half of the cases, and the thoracic region was affected in the other half ([Table 1]). The disease occurred in 1 level in 21 (80.8%) cases, and in 2, 3 and 4 levels in 2, 2, and 1 cases respectively. Only 9 (34.62%) cases required surgery ([Table 1]). The of average time from the beginning of the treatment until the cure was 14.2 months. All patients underwent the basic TB regimen, which consists of the administration of rifampicin, isoniazid, pyrazinamide, and ethambutol (RIPE), and only 1 patient presented TB that was resistant to isoniazid and ethambutol, which were replaced by levofloxacin and streptomycin. A smal part of the cases evolved with complications: 1 death and 8 cases of persistent neurological deficit ([Table 1]).
Results of the Groups
Significant differences were observed regarding the relative lymphocyte count (p = 0.025) and the monocyte/lymphocyte ratio (p = 0.009). The lymphocyte count was higher in the UI group (25.35 ± 13.08) compared to the SI (14.18 ± 7.48) group, while the monocyte/lymphocyte ratio presented a lower mean value in the UI (0,39 ± 0.22) group compared to the SI group (0.89 ± 0.65; [Table 3]). We analyzed the results of the ROC curve, using as a reference for the relative lymphocyte count the value of 16.7, that is, values greater than or equal to 16.7% in relation to the total leukocytes. We found a sensitivity of 76.9% and a specificity of 62.5%, and the area under the ROC curve was of 0.798, and the 95% confidence interval (95%CI) was of 0.60 to 0.98. As for the monocyte/lymphocyte ratio, values greater than or equal to 0.58 presented a sensitivity of 84.6% and a specificity of 75%. The area under the curve was of 0.846, and the 95%CI was of 0.67 to 1.01 ([Figs. 5] and [6]).


|
N |
SD/% |
SI |
SD/% |
UI |
SD/% |
p-value |
|
|---|---|---|---|---|---|---|---|
|
Hemoglobin (g/dL) |
12.1 |
2.1 |
12.1 |
2.71 |
12.15 |
1.61 |
0.678** |
|
Leukocytes (mil/μL) |
8.1 |
2.3 |
7.45 |
2.47 |
8.6 |
2.08 |
0.148** |
|
Lymphocytes (%) |
21.1 |
12.4 |
14.18 |
7.48 |
25.35 |
13.08 |
0.025** |
|
Monocytes (%) |
8.5 |
2.4 |
9.65 |
3.04 |
7.86 |
1.79 |
0.110** |
|
Monocyte/Lymphocyte Ratio |
0.6 |
0.5 |
0.89 |
0.65 |
0.39 |
0.22 |
0.009** |
|
CRP (mg/dL) |
7.0 |
6.7 |
7.25 |
3.18 |
6.83 |
8.51 |
0.195** |
|
ESR (mm) |
83.3 |
27.0 |
97.5 |
18.81 |
77.6 |
28.48 |
0.179** |
|
LDH (mg/dL) |
550.8 |
437.5 |
775.3 |
735.77 |
438.5 |
210.6 |
0.606** |
|
Creatinine (mg/dL) |
0.8 |
0.8 |
0.6 |
0.23 |
0.95 |
0.98 |
0.683** |
|
Total proteins (g/dL) |
6.8 |
0.6 |
7.23 |
0.68 |
6.5 |
0.47 |
0.131** |
|
Albumin (g/dL) |
3.2 |
0.5 |
2.9 |
0.53 |
3.37 |
0.51 |
0.157** |
|
Positive reactive tuberculin skin test |
4 |
15.38 |
3 |
33.33 |
1 |
5.88 |
1.000* |
|
Bacilloscopy |
5 |
19.23 |
5 |
55.56 |
0 |
0.00 |
0.001* |
|
Pathology |
11 |
42.31 |
5 |
55.56 |
6 |
35.29 |
0.637* |
|
Culture |
5 |
19.23 |
5 |
55.56 |
0 |
0.00 |
0.001* |
|
Rapid molecular test |
7 |
26.92 |
7 |
77.78 |
0 |
0.00 |
0.0001* |
When studying only the 11 cases in which the anatomopathological examination was compatible with the disease and dividing these cases according to the bacilloscopy (AFB positive = bacillus observed in the granuloma), the percentage of lymphocytes among patients with positive AFB (n: 5; mean: 12.54) and negative AFB (n: 6; mean: 33.18) presented a significant difference (p = 0.004; [Table 4]).
|
n |
Mean |
p-value** |
|
|---|---|---|---|
|
Positive anatomopathological examination |
11 |
||
|
Positive sputum-smear |
5 |
12.54 |
0.004 |
|
Negative sputum-smear |
6 |
33.18 |
We observed that the presence of collection within a vertebra or in adjacent paravertebral tissues, subligamentous spread, and irregularity of the edges of the end plates of vertebral bodies on T2- and STIR-weighted sequences presented 100% of sensitivity for the diagnosis of patients in the SI group ([Table 5]). These values refer to the variables in which the etiologic agent was isolated.
|
Sensitivity (%) |
Specificity (%) |
PPV (%) |
NVP (%) |
Accuracy (%) |
|
|---|---|---|---|---|---|
|
Involvement of more than 2 vertebrae in adjacent levels |
50.0 |
66.7 |
57.1 |
66.7 |
58.8 |
|
Presence of collection within a vertebra or in adjacent paravertebral tissues |
100.0 |
10.0 |
47.1 |
10.0 |
50.0 |
|
Subligamentous spread |
100.0 |
20.0 |
42.9 |
20.0 |
50.0 |
|
Destruction of the vertebral body with a decrease in the height of more than 50% |
85.7 |
30.0 |
46.2 |
30.0 |
52.9 |
|
Involvement of non-contiguous levels in different regions of the spine |
0.0 |
90.0 |
0.0 |
90.0 |
52.9 |
|
Alteration of the disk morphology with CSF-like isosignal, hypointense on T1, and hyperintense on T2 |
71.4 |
30.0 |
41.7 |
30.0 |
47.1 |
|
Irregularity of the end plates' margins of the vertebral bodies in T2- and STIR-weighted sequences |
100.0 |
0.0 |
41.2 |
0.0 |
41.2 |
|
Invasion of the epidural space by bone or granulation tissue |
71.4 |
50.0 |
50.0 |
50.0 |
58.8 |
Discussion
Patients in the UI group had a higher mean lymphocyte count and a lower monocyte/lymphocyte ratio. One possible explanation could be the depletion of T lymphocytes in the SI group due to the higher bacillary load. O'Shea et al.[19] (2018) compared patients with active TB, latent TB, and controls regarding the bacillary load and the lymphocyte count. Patients with a higher bacillary load (active form) had lower a lymphocyte count compared to those with a lower bacillary load, that is, those with the latent disease (p = 0.017) and the controls (p = 0.003) respectively.
To date, studies on lymphocyte count and the monocyte/lymphocyte ratio have only been conducted in groups with extravertebral TB.[20] [21] [22] Bashir et al.[20] (2014) and Wang et al.[23] (2015) observed that lymphocyte count is lower in patients with TB compared to the general population. La Manna et al.[24] (2017) found that a ratio higher than 0.28 could predict the incidence of TB with a sensitivity of 91.04% and a specificity of 93.55% (p < 0.001). Moreover, Liana et al.[21] (2019) observed that a monocyte/lymphocyte ratio higher than 0.476 had a sensitivity of 95.1% and a specificity of 70% for the diagnosis of TB (p < 0.001). The differences among the studies are probably related to the characteristics of the study subjects. La Manna et al.[24] compared healthy patients and TB patients, while Liana et al.[21] compared patients with chronic cough and positive and negative bacterial cultures.
Elevated lymphocyte counts are controversial in patients without mycobacterial isolation, and they indicate a better immune response against infection, resulting in larger granulomas with fewer bacilli, thus affecting mycobacterial isolation.[25] [26] [27] [28] Another possible complication involved in mycobacterial isolation are the limitations of the diagnostic tests. Although the culture growth requires up to 8 weeks, the RMT has a detection limit of at least 116 colony-forming units per milliliter (CFU/mL), while the culture requires 1 to 10 CFU/mL.
Assessing the possible limitations of this study, we could observe that some variables were not significantly different between the groups, probably due to the small sample size.
The diagnosis of Pott disease must involve a combination of criteria, because unsuccessful isolation of the etiological agent does not exclude the presence of the disease. Therefore, unsuccessful mycobacterial isolation in the presence of other diagnostic criteria should not delay the beginning of the treatment. T-cell response should always be considered.
Conclusion
We did not observe differences regarding the clinico-epidemiological and radiological characteristics between the groups in whom the etiological agent was isolated or not. Higher lymphocyte count and lower monocyte/lymphocyte ratio were observed in the UI group.
Conflito de Interesses
Os autores não têm conflito de interesses a declarar.
Financial Support
There was no financial support from public, commercial, or non-profit sources.
* Work developed at the Spinal Disorders Team, Departament of Orthopedics and Traumatology, Santa Casa de Misericórida de São Paulo, São Paulo, SP, Brazil.
-
Referências
- 1 Qian J, Rijiepu A, Zhu B, Tian D, Chen L, Jing J. Outcomes of radical debridement versus no debridement for the treatment of thoracic and lumbar spinal tuberculosis. Int Orthop 2016; 40 (10) 2081-2088
- 2 Wang G, Dong W, Lan T. et al. Diagnostic accuracy evaluation of the conventional and molecular tests for Spinal Tuberculosis in a cohort, head-to-head study. Emerg Microbes Infect 2018; 7 (01) 109
- 3 Dean A, Zyck S, Toshkezi G, Galgano M, Marawar S. Challenges in the Diagnosis and Management of Spinal Tuberculosis: Case Series. Cureus 2019; 11 (01) e3855
- 4 Dunn RN, Ben Husien M. Spinal tuberculosis: review of current management. Bone Joint J 2018; 100-B (04) 425-431
- 5 Chen CH, Chen YM, Lee CW, Chang YJ, Cheng CY, Hung JK. Early diagnosis of spinal tuberculosis. J Formos Med Assoc 2016; 115 (10) 825-836
- 6 BRASIL Ministério da Saúde. Manual de recomendações para o controle da Tuberculose no Brasil. 2019 ;(61). Disponível em: http://bvsms.saude.gov.br/bvs/publicacoes/manual_recomendacoes_controle_tuberculose_brasil.pdf
- 7 Kilborn T, Janse van Rensburg P, Candy S. Pediatric and adult spinal tuberculosis: imaging and pathophysiology. Neuroimaging Clin N Am 2015; 25 (02) 209-231
- 8 Uppal SS, Tewari SC, Verma S, Dhot PS. Comparison of CD4 and CD8 lymphocyte counts in HIV-negative pulmonary TB patients with those in normal blood donors and the effect of antitubercular treatment: hospital-based flow cytometric study. Cytometry B Clin Cytom 2004; 61 (01) 20-26
- 9 Jones BE, Oo MM, Taikwel EK. et al. CD4 cell counts in human immunodeficiency virus-negative patients with tuberculosis. Clin Infect Dis 1997; 24 (05) 988-991
- 10 Couto BB, Umeta RSG, Caffaro MFS, Meves R, Landim E, Avanzi O. Análise radiológica comparativa entre espondilodiscite tuberculosa e inespecífica. Coluna/Columna 2010; 9 (04) 394-400
- 11 Rivas-Garcia A, Sarria-Estrada S, Torrents-Odin C, Casas-Gomila L, Franquet E. Imaging findings of Pott's disease. Eur Spine J 2013; 22 (Suppl. 04) 567-578
- 12 Kanna RM, Babu N, Kannan M, Shetty AP, Rajasekaran S. Diagnostic accuracy of whole spine magnetic resonance imaging in spinal tuberculosis validated through tissue studies. Eur Spine J 2019; 28 (12) 3003-3010
- 13 Shi T, Zhang Z, Dai F. et al. Retrospective Study of 967 Patients With Spinal Tuberculosis. Orthopedics 2016; 39 (05) e838-e843
- 14 Lee KY. Comparison of pyogenic spondylitis and tuberculous spondylitis. Asian Spine J 2014; 8 (02) 216-223
- 15 Durovni B, Saraceni V, van den Hof S. et al. Impact of replacing smear microscopy with Xpert MTB/RIF for diagnosing tuberculosis in Brazil: a stepped-wedge cluster-randomized trial. PLoS Med 2014; 11 (12) e1001766
- 16 Batirel A, Erdem H, Sengoz G. et al. The course of spinal tuberculosis (Pott disease): results of the multinational, multicentre Backbone-2 study. Clin Microbiol Infect 2015; 21 (11) 1008.e9-1008.e18
- 17 Nayak S, Acharjya B. VDRL test and its interpretation. Indian J Dermatol 2012; 57 (01) 3-8
- 18 Rama Krishna M, Gottam US, Mahendra N. Disseminated tuberculosis with severe immune thrombocytopenia. Respir Med Case Rep 2019; 27: 100812
- 19 O'Shea MK, Tanner R, Müller J. et al. Immunological correlates of mycobacterial growth inhibition describe a spectrum of tuberculosis infection. Sci Rep 2018; 8 (01) 14480
- 20 Bashir AB, Abufatima AS, Mohamedani AA. Impact of pulmonary tuberculosis on total and differential peripheral blood leukocytes count. Int J Trop Med 2014; 9 (03) 33-37
- 21 Liana P, Brestilova B, Yakub Rahadiyanto K. The ratio of monocytes to lymphocytes accuracy as tuberculosis predictor. J Phys Conf Ser 2019; 1246: 012024
- 22 Djordjevic D, Rondovic G, Surbatovic M. et al. Neutrophil-to-Lymphocyte Ratio, Monocyte-to-Lymphocyte Ratio, Platelet-to-Lymphocyte Ratio, and Mean Platelet Volume-to-Platelet Count Ratio as Biomarkers in Critically Ill and Injured Patients: Which Ratio to Choose to Predict Outcome and Nature of Bacteremia?. Mediators Inflamm 2018; 2018: 3758068
- 23 Wang J, Yin Y, Wang X. et al. Ratio of monocytes to lymphocytes in peripheral blood in patients diagnosed with active tuberculosis. Braz J Infect Dis 2015; 19 (02) 125-131
- 24 La Manna MP, Orlando V, Dieli F. et al. Quantitative and qualitative profiles of circulating monocytes may help identifying tuberculosis infection and disease stages. PLoS One 2017; 12 (02) e0171358
- 25 Roy Chowdhury R, Vallania F, Yang Q. et al. A multi-cohort study of the immune factors associated with M. tuberculosis infection outcomes. Nature 2018; 560 (7720): 644-648
- 26 Jasenosky LD, Scriba TJ, Hanekom WA, Goldfeld AE. T cells and adaptive immunity to Mycobacterium tuberculosis in humans. Immunol Rev 2015; 264 (01) 74-87
- 27 Cooper AM. Cell-mediated immune responses in tuberculosis. Annu Rev Immunol 2009; 27: 393-422
- 28 Monina L, Khadera SA. Chemokines in tuberculosis: The good, the bad and the ugly. Semin Immunol 2008; 23 (01) 1-7
Endereço para correspondência
Publikationsverlauf
Eingereicht: 26. Oktober 2021
Angenommen: 18. Juli 2022
Artikel online veröffentlicht:
24. März 2023
© 2023. Sociedade Brasileira de Ortopedia e Traumatologia. This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commecial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/)
Thieme Revinter Publicações Ltda.
Rua do Matoso 170, Rio de Janeiro, RJ, CEP 20270-135, Brazil
-
Referências
- 1 Qian J, Rijiepu A, Zhu B, Tian D, Chen L, Jing J. Outcomes of radical debridement versus no debridement for the treatment of thoracic and lumbar spinal tuberculosis. Int Orthop 2016; 40 (10) 2081-2088
- 2 Wang G, Dong W, Lan T. et al. Diagnostic accuracy evaluation of the conventional and molecular tests for Spinal Tuberculosis in a cohort, head-to-head study. Emerg Microbes Infect 2018; 7 (01) 109
- 3 Dean A, Zyck S, Toshkezi G, Galgano M, Marawar S. Challenges in the Diagnosis and Management of Spinal Tuberculosis: Case Series. Cureus 2019; 11 (01) e3855
- 4 Dunn RN, Ben Husien M. Spinal tuberculosis: review of current management. Bone Joint J 2018; 100-B (04) 425-431
- 5 Chen CH, Chen YM, Lee CW, Chang YJ, Cheng CY, Hung JK. Early diagnosis of spinal tuberculosis. J Formos Med Assoc 2016; 115 (10) 825-836
- 6 BRASIL Ministério da Saúde. Manual de recomendações para o controle da Tuberculose no Brasil. 2019 ;(61). Disponível em: http://bvsms.saude.gov.br/bvs/publicacoes/manual_recomendacoes_controle_tuberculose_brasil.pdf
- 7 Kilborn T, Janse van Rensburg P, Candy S. Pediatric and adult spinal tuberculosis: imaging and pathophysiology. Neuroimaging Clin N Am 2015; 25 (02) 209-231
- 8 Uppal SS, Tewari SC, Verma S, Dhot PS. Comparison of CD4 and CD8 lymphocyte counts in HIV-negative pulmonary TB patients with those in normal blood donors and the effect of antitubercular treatment: hospital-based flow cytometric study. Cytometry B Clin Cytom 2004; 61 (01) 20-26
- 9 Jones BE, Oo MM, Taikwel EK. et al. CD4 cell counts in human immunodeficiency virus-negative patients with tuberculosis. Clin Infect Dis 1997; 24 (05) 988-991
- 10 Couto BB, Umeta RSG, Caffaro MFS, Meves R, Landim E, Avanzi O. Análise radiológica comparativa entre espondilodiscite tuberculosa e inespecífica. Coluna/Columna 2010; 9 (04) 394-400
- 11 Rivas-Garcia A, Sarria-Estrada S, Torrents-Odin C, Casas-Gomila L, Franquet E. Imaging findings of Pott's disease. Eur Spine J 2013; 22 (Suppl. 04) 567-578
- 12 Kanna RM, Babu N, Kannan M, Shetty AP, Rajasekaran S. Diagnostic accuracy of whole spine magnetic resonance imaging in spinal tuberculosis validated through tissue studies. Eur Spine J 2019; 28 (12) 3003-3010
- 13 Shi T, Zhang Z, Dai F. et al. Retrospective Study of 967 Patients With Spinal Tuberculosis. Orthopedics 2016; 39 (05) e838-e843
- 14 Lee KY. Comparison of pyogenic spondylitis and tuberculous spondylitis. Asian Spine J 2014; 8 (02) 216-223
- 15 Durovni B, Saraceni V, van den Hof S. et al. Impact of replacing smear microscopy with Xpert MTB/RIF for diagnosing tuberculosis in Brazil: a stepped-wedge cluster-randomized trial. PLoS Med 2014; 11 (12) e1001766
- 16 Batirel A, Erdem H, Sengoz G. et al. The course of spinal tuberculosis (Pott disease): results of the multinational, multicentre Backbone-2 study. Clin Microbiol Infect 2015; 21 (11) 1008.e9-1008.e18
- 17 Nayak S, Acharjya B. VDRL test and its interpretation. Indian J Dermatol 2012; 57 (01) 3-8
- 18 Rama Krishna M, Gottam US, Mahendra N. Disseminated tuberculosis with severe immune thrombocytopenia. Respir Med Case Rep 2019; 27: 100812
- 19 O'Shea MK, Tanner R, Müller J. et al. Immunological correlates of mycobacterial growth inhibition describe a spectrum of tuberculosis infection. Sci Rep 2018; 8 (01) 14480
- 20 Bashir AB, Abufatima AS, Mohamedani AA. Impact of pulmonary tuberculosis on total and differential peripheral blood leukocytes count. Int J Trop Med 2014; 9 (03) 33-37
- 21 Liana P, Brestilova B, Yakub Rahadiyanto K. The ratio of monocytes to lymphocytes accuracy as tuberculosis predictor. J Phys Conf Ser 2019; 1246: 012024
- 22 Djordjevic D, Rondovic G, Surbatovic M. et al. Neutrophil-to-Lymphocyte Ratio, Monocyte-to-Lymphocyte Ratio, Platelet-to-Lymphocyte Ratio, and Mean Platelet Volume-to-Platelet Count Ratio as Biomarkers in Critically Ill and Injured Patients: Which Ratio to Choose to Predict Outcome and Nature of Bacteremia?. Mediators Inflamm 2018; 2018: 3758068
- 23 Wang J, Yin Y, Wang X. et al. Ratio of monocytes to lymphocytes in peripheral blood in patients diagnosed with active tuberculosis. Braz J Infect Dis 2015; 19 (02) 125-131
- 24 La Manna MP, Orlando V, Dieli F. et al. Quantitative and qualitative profiles of circulating monocytes may help identifying tuberculosis infection and disease stages. PLoS One 2017; 12 (02) e0171358
- 25 Roy Chowdhury R, Vallania F, Yang Q. et al. A multi-cohort study of the immune factors associated with M. tuberculosis infection outcomes. Nature 2018; 560 (7720): 644-648
- 26 Jasenosky LD, Scriba TJ, Hanekom WA, Goldfeld AE. T cells and adaptive immunity to Mycobacterium tuberculosis in humans. Immunol Rev 2015; 264 (01) 74-87
- 27 Cooper AM. Cell-mediated immune responses in tuberculosis. Annu Rev Immunol 2009; 27: 393-422
- 28 Monina L, Khadera SA. Chemokines in tuberculosis: The good, the bad and the ugly. Semin Immunol 2008; 23 (01) 1-7





