Keywords
gastrostomy - jejunostomy - advanced technique
In 1822, Alexis St. Martin suffered a gunshot wound to the left lower chest. Under
the care of William Beaumont, his injuries eventually developed into a gastrocutaneous
fistula which persisted for another 58 years, which established that a permanent opening
to the stomach could safely be created.[1] This famous case has been surmised to have inspired a military surgeon, Christian
Egeberg, to remark in 1841, “I cannot see why the indications should not be just as
great to open the intestinal canal to put nourishment in as to open it to take a foreign
body out.” The first completed surgical gastrostomy creation was subsequently performed
in 1846 by a French surgeon, Charles Sédillot.[2]
While there were many subsequent refinements in surgical technique in intervening
years, a major step in the evolution of gastrostomy tube placement was the description
of percutaneous endoscopic gastrostomy creation by Gauderer et al in 1980.[3] This was followed shortly thereafter by Preshaw describing fluoroscopically guided
gastrostomy creation in 1981[4]; percutaneous, rather than transoral, insertion techniques were described by several
authors in 1983.[5]
[6]
[7] Since then, radiologic percutaneous gastrostomy (RPG) placement has become widely
accepted, with high technical success rates and low rates of complications.[8]
[9]
[10]
In this article, we discuss the standard RPG technique and describe additional radiologic
techniques for challenging anatomic or physiologic cases.
Indications
The predominant indications for RPG are similar to those of other gastrostomy tubes:
nutritional support or gastrointestinal decompression. The need for nutritional support
can have many sources, including neurogenic dysphagia, head and neck malignancy with
obstruction or impaired swallowing, head or throat surgery, medical conditions causing
impaired absorption, or metabolically demanding states requiring high caloric intake
(e.g., burns). Decompression may be requested for palliation in cases of small bowel
obstruction as well as for diversion in the setting of enteric fistulae.[11] In cases of gastric outlet obstruction, lower esophageal sphincter incompetence
(leading to aspiration), or gastroparesis, placement of a gastrojejunostomy or jejunostomy
tube may be preferable.[12]
Contraindications
There are few absolute contraindications to RPG placement. These include uncorrected
coagulopathy, peritonitis, bowel ischemia, and portal hypertension with gastric varices.
Most of the relative contraindications are related to wound healing or technical feasibility.
Ascites, long-term steroid use or immunosuppression, the presence of a ventriculoperitoneal
shunt, open wounds, the presence of herniorrhaphy mesh, or hypoalbuminemia have been
associated with infection or impaired wound healing.
Ascites was previously considered an absolute contraindication due to the risk of
poor tract healing leading to bacterial peritonitis from gastric and skin flora. O'Keeffe
et al reported leakage of ascites in 24% of patients with ascites and tube displacement
into the peritoneum in 4% of patients. Of note, gastropexy was not used in these cases.[13] It has been suggested that paracentesis and gastropexy can reduce that risk,[14]
[15]
[16]
[17] although a recent study reported an ascites leakage rate of 14% in patients with
chronic ascites who underwent transabdominal gastrostomy creation.[18]
Steroids or immunosuppression, as with any invasive procedure, can impair wound healing,
with an attendant increased risk of peritubal leakage.[11] Gastrostomy tube placement increases the risk of ventriculoperitoneal shunt infection
and may also carry a risk of ascending meningitis.[19]
[20] Hypoalbuminemia has also been linked to higher complication rates, including increased
short-term mortality, although it is not clear if optimizing serum albumin after placement
could ameliorate this risk.[21]
[22]
[23]
[24]
[25]
[26]
Billroth partial gastrectomy, hiatal hernias, esophagectomy with gastric pull-through,
colonic interposition, and an elevated left hemidiaphragm can preclude a percutaneous
approach to the stomach. However, CT-guided gastric puncture, balloon dilation of
the stomach, balloon occlusion of the gastric outflow, infracolic placement (through
the transverse mesocolon), or percutaneous transesophageal gastrostomy (PTEG) can
make these challenging approaches technically feasible.[27]
[28]
Approaches
There are many variations on RPG placement. These are often performed under moderate
sedation, although in appropriate patients they can be placed with local anesthesia
alone. Other patients have comorbidities that require general anesthesia.
Prior to starting, the colon should be positively identified to prevent traversal
of the colonic lumen. In a 2007 review, Friedmann et al found 28 cases of transcolonic
placement in the literature. The most common symptoms were diarrhea and feculent leakage
around the tube. Many were asymptomatic, and 10 were treated conservatively, while
14 were treated with surgery. Subsequently, colonic perforation or obstruction has
been described.[29]
[30]
Oftentimes, barium is administered orally or via enteric tube prior to the procedure.
However, air within the colon is often sufficient to identify this structure; when
in doubt, a barium enema can also be performed.[31]
A nasal or oral gastric tube should be in place to insufflate the stomach. While there
are many commercial choices on the market, a 4- or 5-Fr angiographic catheter can
also be used, with or without a wire. When passing a tube is not technically feasible,
ultrasound- or CT-guided insertion of an 18- to 22-gauge needle into the gastric lumen
has been described to allow for insufflation. Once the gastrostomy tube has been placed,
the needle can be safely removed without risk of bleeding.[32]
[33]
[34]
[35]
[36]
Smooth muscle relaxants such as scopolamine butyl bromide or glucagon can be given
prior to insufflation to diminish peristalsis and spasm the pylorus. This allows for
insufflation of the stomach in isolation. Note that glucagon has a short half-life
(around 8 minutes) and can cause hyperglycemia in diabetics.[37]
Then, securement of the stomach to the abdominal wall is generally recommended because
it prevents intraperitoneal leakage of gastric contents during tract dilation, and
it allows safe recanalization of the tract and replacement of a tube if the gastrostomy
tube becomes inadvertently dislodged prior to tract maturation.[38] T-tacks are commonly used for gastropexy, although other devices exist. There is
no clear consensus on the number of T-tacks that should be used, although 2–3 is most
commonly used. Contrast can be injected through the delivery needles to confirm intraluminal
location prior to deployment.[39]
[40]
[41]
Through the middle of the gastropexy devices, an 18- or 19-gauge needle is inserted
into the gastric lumen. Contrast is injected to confirm intraluminal location, and
a stiff wire is inserted into the stomach. Over the stiff wire, the tract is dilated.
Multiple methods exist to do this; however, the most common are serial dilators with
a peel-away sheath, a telescoping dilator set with a peel-away sheath, or using an
angioplasty balloon.[42]
Either through the peel-away sheath or over the angioplasty balloon, the gastrostomy
tube is advanced into the gastric lumen. Confirmation of intraluminal location can
be confirmed via aspiration of air through the tube, watching the distended stomach
deflate fluoroscopically, injecting contrast to visualize rugae, and taking a lateral
view to see contrast fall into the stomach. A cone-beam CT can be performed if further
clarification is necessary ([Fig. 1]).
 Fig. 1 Standard radiologic percutaneous gastrostomy tube placement. Note the transverse
colon (*) and contrast opacifying gastric rugae (^), confirming direct placement into
the gastric lumen.
Fig. 1 Standard radiologic percutaneous gastrostomy tube placement. Note the transverse
colon (*) and contrast opacifying gastric rugae (^), confirming direct placement into
the gastric lumen.
Alternatively, a pull-through tube can be placed by navigating a wire through the
gastric lumen, into the esophagus, and out the oral cavity. Over the wire, a mushroom-retention
pull-through gastrostomy tube can then be advanced ([Fig. 2]).
 Fig. 2 Standard radiologic pull-through gastrostomy tube placement. (a) Retrograde catheterization of the esophagus and mouth from the gastric lumen allows
for advancement of the tube from the oral cavity. (b) Completion imaging demonstrating contrast opacifying gastric rugae (^).
Fig. 2 Standard radiologic pull-through gastrostomy tube placement. (a) Retrograde catheterization of the esophagus and mouth from the gastric lumen allows
for advancement of the tube from the oral cavity. (b) Completion imaging demonstrating contrast opacifying gastric rugae (^).
Case 1: Poor Percutaneous Access
Case 1: Poor Percutaneous Access
Colon, liver, or ribs can be interposed between the stomach and the anterior abdominal
wall, even with insufflation of the stomach. Caudal-cranial angulation is oftentimes
enough to create a window between these structures.
Infracolic placement can also be performed. This was first described by Mirich and
Gray in 1989.[27] While there is theoretical risk of omental infarction, mesenteric ischemia or hemorrhage,
or catheter malfunction from this approach, several retrospective studies report no
adverse outcomes with infracolic placement.[43]
[44]
Transhepatic gastrostomy tube placement has been described without significant adverse
effects, although this is limited by low numbers ([Fig. 3]).[35]
[45] However, there are case reports of delayed bleeding and intrahepatic abscess formation
associated with removal or exchange of the tube.[46]
[47]
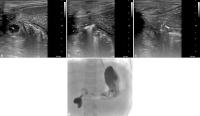 Fig. 3 Transhepatic gastrostomy tube placement. This patient was a 3-year-old with discontinuity
of his duodenum after trauma, requiring venting gastrostomy placement prior to staged
surgical repair. Due to extensive adhesions, particularly of his transverse colon
to the deep surface of the liver, surgical placement carried prohibitively high risk
of bowel perforation. (a) Sagittal ultrasound imaging demonstrating the liver (+), stomach (*), and transverse
colon (^). (b) Due to adhesions, their spatial relationship between the liver (+), stomach (*),
and transverse colon wall (^) persisted despite insufflation. (c) Ultrasound-guided needle puncture (x) through a small amount of liver parenchyma
and into the stomach. (d) Final gastrostomy image.
Fig. 3 Transhepatic gastrostomy tube placement. This patient was a 3-year-old with discontinuity
of his duodenum after trauma, requiring venting gastrostomy placement prior to staged
surgical repair. Due to extensive adhesions, particularly of his transverse colon
to the deep surface of the liver, surgical placement carried prohibitively high risk
of bowel perforation. (a) Sagittal ultrasound imaging demonstrating the liver (+), stomach (*), and transverse
colon (^). (b) Due to adhesions, their spatial relationship between the liver (+), stomach (*),
and transverse colon wall (^) persisted despite insufflation. (c) Ultrasound-guided needle puncture (x) through a small amount of liver parenchyma
and into the stomach. (d) Final gastrostomy image.
Case 2: No Pylorus
In the absence of a pylorus, insufflating the stomach becomes impossible—the immediate
escape of air to the small bowel prevents distension of the stomach and can also obscure
the fluoroscopic view sufficiently to preclude safely continuing with tube placement.
Some have described proceeding regardless, with CT-guided puncture of the stomach.[35]
[36] Additionally, balloon occlusion of the outflow tract can allow for insufflation
of the stomach; however, the smaller stomach size after partial gastrectomy can still
preclude safe gastrostomy tube placement[48] ([Fig. 4]).
 Fig. 4 Balloon occlusion of the outflow tract. This patient had a Billroth I distal gastrectomy
for peptic ulcer disease in 1983. He subsequently developed oropharyngeal cancer and
required enteric access prior to starting radiation; however, the gastric remnant
was small and high, and insufflation was not possible due to the lack of a pylorus.
(a) An occlusive balloon was advanced to the proximal alimentary limb over wire through
the nares and inflated. (b) The gastric remnant was then insufflated and, with steep caudal angulation, a window
between the costal margin (*) and colon (^) allowed for access to the stomach for
gastrostomy tube placement. (c) Final gastrostomy tube placement.
Fig. 4 Balloon occlusion of the outflow tract. This patient had a Billroth I distal gastrectomy
for peptic ulcer disease in 1983. He subsequently developed oropharyngeal cancer and
required enteric access prior to starting radiation; however, the gastric remnant
was small and high, and insufflation was not possible due to the lack of a pylorus.
(a) An occlusive balloon was advanced to the proximal alimentary limb over wire through
the nares and inflated. (b) The gastric remnant was then insufflated and, with steep caudal angulation, a window
between the costal margin (*) and colon (^) allowed for access to the stomach for
gastrostomy tube placement. (c) Final gastrostomy tube placement.
Case 3: Medical Contraindication for Gastrostomy Tube Placement
Case 3: Medical Contraindication for Gastrostomy Tube Placement
Some patients have such profound malnutrition that they may not be able to adequately
epithelialize the gastrostomy tract, leading to long-term risks of tube dislodgement
and peritonitis. Others have hostile sites for percutaneous access due to interposed
structures, wounds, enterocutaneous fistulae, herniorrhaphy mesh, prior radiation,
or peritoneal metastases with malignant ascites. In such cases, PTEG has been utilized
for gastric venting and feeding ([Fig. 5]).[28]
[49]
[50]
 Fig. 5 Transesophageal gastrostomy tube placement. This patient was a 44-year-old female
with anorexia nervosa presented with severe malnourishment and malnutrition. Due to
her inability to maintain adequate nutrition via oral and parenteral routes, gastrostomy
tube placement was requested for supplemental nutrition. Due to ascites and profound
hypoalbuminemia (1.2 g/dL at initial consultation), there was consensus between IR,
general surgery, and gastroenterology that she was at high risk for poor wound healing,
and that the risk of bacterial peritonitis could potentially be fatal in her case.
Therefore, the decision was made to place a percutaneous transesophageal gastrostomy
tube. (a) Transverse ultrasound image of the left neck showing the relationship between the
left internal jugular vein (V), left common carotid artery (A), thyroid gland (T),
trachea (*), and esophagus (E). (b) After hydrodissection of the space between the carotid artery (A) and thyroid gland
(T), a 16-mm angioplasty balloon was inflated in the cervical esophagus (E) to serve
as a target for percutaneous puncture. (c) The space between the carotid artery and thyroid gland was traversed with a 22-gauge
needle to the edge of the esophagus. Puncture of the balloon was performed with fluoroscopic
guidance. (d) The tract was dilated, and a 12-Fr MIC jejunostomy tube (*; Avanos Medical Devices,
Alpharetta, GA) was cut to length and placed with the distal end in the stomach and
the balloon retention at the esophagostomy.
Fig. 5 Transesophageal gastrostomy tube placement. This patient was a 44-year-old female
with anorexia nervosa presented with severe malnourishment and malnutrition. Due to
her inability to maintain adequate nutrition via oral and parenteral routes, gastrostomy
tube placement was requested for supplemental nutrition. Due to ascites and profound
hypoalbuminemia (1.2 g/dL at initial consultation), there was consensus between IR,
general surgery, and gastroenterology that she was at high risk for poor wound healing,
and that the risk of bacterial peritonitis could potentially be fatal in her case.
Therefore, the decision was made to place a percutaneous transesophageal gastrostomy
tube. (a) Transverse ultrasound image of the left neck showing the relationship between the
left internal jugular vein (V), left common carotid artery (A), thyroid gland (T),
trachea (*), and esophagus (E). (b) After hydrodissection of the space between the carotid artery (A) and thyroid gland
(T), a 16-mm angioplasty balloon was inflated in the cervical esophagus (E) to serve
as a target for percutaneous puncture. (c) The space between the carotid artery and thyroid gland was traversed with a 22-gauge
needle to the edge of the esophagus. Puncture of the balloon was performed with fluoroscopic
guidance. (d) The tract was dilated, and a 12-Fr MIC jejunostomy tube (*; Avanos Medical Devices,
Alpharetta, GA) was cut to length and placed with the distal end in the stomach and
the balloon retention at the esophagostomy.
These can be done under moderate sedation, which can allow for identification of aberrant
recurrent laryngeal nerve if the patient develops breathy dysphonia during infiltration
of the soft tissues with local anesthetic.
The most common adverse event after PTEG is displacement of the tube, which will often
present with recurrence of bowel obstruction symptoms and decreased tube output. Site
infection is uncommon.[51] Nausea and vomiting are reportedly lower when compared with decompressive nasogastric
tubes.[52]
Case 4: Jejunal Access
While the focus of this article has mainly been gastric access, jejunal access can
be necessary due to gastric outlet or duodenal obstruction, discontinuity between
the stomach and small bowel, or aspiration due to an incompetent lower esophageal
sphincter.[17]
Existing gastrostomy stomas can be converted to a gastrojejunostomy tube by manipulating
an angiographic catheter through the stoma, pylorus, and duodenum to the proximal
jejunum. Over a wire, the angiographic catheter can be exchanged for a balloon-retention
gastrojejunostomy tube. Alternatively, the catheterization of the jejunum can be performed
through the lumen of a pull-through gastrostomy tube; the angiographic catheter can
be exchanged over wire for a purpose-built jejunal extension.
Primary gastrojejunostomy tube placement can also be safely performed.[53] If using a pull-through gastrostomy tube, there is essentially no technical difference
in placement of the gastrostomy tube or jejunal extension. If placing a balloon-retention
gastrojejunostomy tube, catheterization of the jejunum is performed prior to tract
dilation. The use of a peel-away sheath may prevent strain on the gastropexy devices
caused by friction between the gastric wall and silicone of the gastrojejunostomy
tube during advancement.[17]
Primary percutaneous jejunostomy tube placement can also be performed with fluoroscopic,
CT, or ultrasound-guided approaches ([Figs. 6] and [7]). Due to the motility of the intestine, puncture-resistance of the intestinal wall,
and small size of the jejunal lumen, these can be very technically challenging, with
a reported technical success rate of 85 to 95% in the literature.[54]
[55]
[56]
 Fig. 6 Fluoroscopic jejunostomy tube placement. A 23-year-old female with cyclic vomiting
and SMA syndrome had recurrent reflux of gastrojejunostomy tubes into her stomach
and esophagus, requiring direct jejunal access for nutrition. (a) Through the existing gastrojejunal access, the small bowel was insufflated, and
a proximal anterior loop of jejunum was targeted fluoroscopically in a steep right
anterior oblique projection. Contrast was injected through the T-tack delivery needle
to confirm intraluminal placement. (b) After two T-tacks (^) were placed to secure the jejunum to the abdominal wall, the
jejunum was punctured with an 18-gauge needle. (c) Over a wire, the tract was dilated, and a 12-Fr MIC jejunostomy tube (*; Avanos
Medical Devices, Alpharetta, GA) was placed.
Fig. 6 Fluoroscopic jejunostomy tube placement. A 23-year-old female with cyclic vomiting
and SMA syndrome had recurrent reflux of gastrojejunostomy tubes into her stomach
and esophagus, requiring direct jejunal access for nutrition. (a) Through the existing gastrojejunal access, the small bowel was insufflated, and
a proximal anterior loop of jejunum was targeted fluoroscopically in a steep right
anterior oblique projection. Contrast was injected through the T-tack delivery needle
to confirm intraluminal placement. (b) After two T-tacks (^) were placed to secure the jejunum to the abdominal wall, the
jejunum was punctured with an 18-gauge needle. (c) Over a wire, the tract was dilated, and a 12-Fr MIC jejunostomy tube (*; Avanos
Medical Devices, Alpharetta, GA) was placed.
 Fig. 7 CT-guided jejunostomy tube placement. A 54-year-old female was transitioning to hospice
due to advanced ovarian cancer. She developed a closed-loop small bowel obstruction
related to metastases and surgical adhesions, and decompression was requested for
palliation. (a) Coronal post-contrast CT of the abdomen and pelvis showing the closed-loop obstruction
(*). Because the obstructed bowel was very superficially located at the left flank,
it appeared amenable to percutaneous drainage. (b) Two T-tacks (^) were placed with CT fluoroscopic guidance into the obstructed jejunum
(*). (c) The space between the T-tacks was punctured with an 18-gauge needle, which was exchanged
over wire for a 10-Fr pigtail drainage catheter. (d) Subsequent fluoroscopic image demonstrates decompression of the obstructed portions
of the duodenum and proximal jejunum. Note the mild distension of the duodenum (*)
proximal to the superior mesenteric artery (x).
Fig. 7 CT-guided jejunostomy tube placement. A 54-year-old female was transitioning to hospice
due to advanced ovarian cancer. She developed a closed-loop small bowel obstruction
related to metastases and surgical adhesions, and decompression was requested for
palliation. (a) Coronal post-contrast CT of the abdomen and pelvis showing the closed-loop obstruction
(*). Because the obstructed bowel was very superficially located at the left flank,
it appeared amenable to percutaneous drainage. (b) Two T-tacks (^) were placed with CT fluoroscopic guidance into the obstructed jejunum
(*). (c) The space between the T-tacks was punctured with an 18-gauge needle, which was exchanged
over wire for a 10-Fr pigtail drainage catheter. (d) Subsequent fluoroscopic image demonstrates decompression of the obstructed portions
of the duodenum and proximal jejunum. Note the mild distension of the duodenum (*)
proximal to the superior mesenteric artery (x).
Reestablishing a previous jejunostomy site has a higher technical success rate and
lower complication rate, because the jejunal wall is already surgically adherent to
the abdominal wall and thus no longer mobile.[56]
[57] The tract can often be seen under ultrasound ([Fig. 8]).
 Fig. 8 Ultrasound-guided jejunostomy tube placement. A 48-year-old female with previous
resection of a small bowel neuroendocrine tumor had a jejunostomy tube for nutritional
support after the resection. This was subsequently removed when the patient was able
to maintain nutritional goals via oral intake alone. Unfortunately, she again began
losing weight and required the jejunostomy tube. (a) Ultrasound of the site of the jejunostomy tube demonstrates a hypoechoic scar (^)
from the skin, through the abdominal wall, and into jejunum. This was punctured under
real-time ultrasound guidance with a 22-gauge needle (*). (b) The tract was dilated to allow for placement of a 10-Fr pigtail catheter, which
was subsequently exchanged for a balloon-retention jejunostomy tube 2 weeks later.
Fig. 8 Ultrasound-guided jejunostomy tube placement. A 48-year-old female with previous
resection of a small bowel neuroendocrine tumor had a jejunostomy tube for nutritional
support after the resection. This was subsequently removed when the patient was able
to maintain nutritional goals via oral intake alone. Unfortunately, she again began
losing weight and required the jejunostomy tube. (a) Ultrasound of the site of the jejunostomy tube demonstrates a hypoechoic scar (^)
from the skin, through the abdominal wall, and into jejunum. This was punctured under
real-time ultrasound guidance with a 22-gauge needle (*). (b) The tract was dilated to allow for placement of a 10-Fr pigtail catheter, which
was subsequently exchanged for a balloon-retention jejunostomy tube 2 weeks later.
In patients with malignant duodenal obstruction, palliative duodenal stent placement
may be performed percutaneously under minimal sedation[58] ([Fig. 9]).
 Fig. 9 Transgastric duodenal stent placement. A 92-year-old female presented with duodenal
obstruction due to pancreatic cancer. While her nutritional needs were met by a gastrojejunostomy
tube, she ultimately elected for hospice and requested a duodenal stent to allow for
oral intake. (a) Contrast injection from a 12-Fr sheath placed via gastrojejunostomy tract demonstrates
high-grade stenosis of the D3 portion of duodenum (^). Contrast was injected in the
D4 portion via 5-Fr angiographic catheter (*) to elucidate the extent of the stenosis.
(b) Through the sheath, a 22-mm WallFlex duodenal stent (Boston Scientific, Marlborough,
MA) was deployed across the stenotic portion of the duodenum. (c) After post-molding the stent with an angioplasty balloon, the duodenum was widely
patent, allowing ready transit from stomach to jejunum.
Fig. 9 Transgastric duodenal stent placement. A 92-year-old female presented with duodenal
obstruction due to pancreatic cancer. While her nutritional needs were met by a gastrojejunostomy
tube, she ultimately elected for hospice and requested a duodenal stent to allow for
oral intake. (a) Contrast injection from a 12-Fr sheath placed via gastrojejunostomy tract demonstrates
high-grade stenosis of the D3 portion of duodenum (^). Contrast was injected in the
D4 portion via 5-Fr angiographic catheter (*) to elucidate the extent of the stenosis.
(b) Through the sheath, a 22-mm WallFlex duodenal stent (Boston Scientific, Marlborough,
MA) was deployed across the stenotic portion of the duodenum. (c) After post-molding the stent with an angioplasty balloon, the duodenum was widely
patent, allowing ready transit from stomach to jejunum.
Conclusion
Enteric access is commonly required for venting or nutrition. Many of these patients
have complex medical or surgical history which precludes standard access techniques.
However, the imaging tools used by interventional radiology allow for obtaining access
in many of these challenging patients.





