

Subscribe to RSS
DOI: 10.1055/s-0044-1787772
Insights into Imaging of Pericardial and Cardiac Tuberculosis: A Comprehensive Review
Authors
Funding None.

Abstract
Pericardial and cardiac tuberculosis (TB) is an uncommon form of extrapulmonary TB that poses a considerable diagnostic challenge for clinicians due to its nonspecific and diverse presentation. Its presentation is so diverse and distinct that it necessitates advanced imaging with cardiac computed tomography (CT)/cardiac magnetic resonance (CMR) in addition to routine transthoracic echocardiography (TTE) for accurate diagnosis, myocardial involvement, management planning, and follow-up. This comprehensive review article highlights the highly valuable role of imaging modalities like echocardiography, cardiac CT, and CMR in the detailed evaluation of pericardial and cardiac TB, highlighting different forms of cardiac and pericardial involvement, their distinctive imaging features, and diagnostic challenges.
Introduction
Pericardial and cardiac involvement by tuberculosis (TB), though uncommon, is the second most common cause of TB-related deaths after cranial and spinal TB.[1] Tubercular involvement in the heart occur in the pericardium, myocardium, endocardium, or coronary arteries.[2] The diagnosis of isolated pericardial and cardiac TB is difficult since the clinical presentation is typically ambiguous, and traditional procedures, such as sputum smear microscopy, culture, and histology, have limited sensitivity and specificity. As a result, imaging techniques such as transthoracic echocardiography (TTE), cardiac computed tomography (CT), and cardiac magnetic resonance (CMR) play a critical role in the diagnosis, evaluation, its differentiation from other pathologies, in monitoring the therapeutic response, and for follow-up of pericardial and cardiac TB. In this review article, we will discuss the epidemiology, pathophysiology, clinical features, and imaging modalities for evaluation of pericardial and cardiac TB, and we will review the current evidence and recommendations on the use of echocardiography, cardiac CT, and CMR imaging for the diagnosis and management of these conditions.
Epidemiology
TB is a prevailing infectious, communicable illness caused by Mycobacterium bacillus, which is a significant cause of morbidity and mortality in the developing countries. The World Health Organization statistics for India 2022 gave an incidence of 210 per 100,000 people.[3] Further, approximately 40% of Indians are thought to have Mycobacterium bacillus infections, majority of whom have latent TB rather than an active illness.[4]
Pathophysiology
Mycobacterium bacillus is primarily a pulmonary pathogen but can affect all parts of the body, including the heart and pericardium. These bacteria can reach the pericardium and heart through:
-
Retrograde spread from hilar, peribronchial, subcarinal, and paratracheal lymph nodes
-
Direct spread from adjacent lungs and pleura
-
Hematogenous spread in miliary TB mainly in immunocompromised individuals who have high TB bacilli load
Cardiovascular involvement in TB has been found to be associated with relatively poor prognosis, like tubercular pericarditis has been found to be associated with mortality as high as 40%[5] ([Table 1]).[6] [7] [8]
|
Involvement type |
Incidence |
|---|---|
|
Pericardial involvement |
2–5%[7] |
|
Cardiac involvement |
0.14–2%[8] |
Pericardial Involvement in TB
Pericardial involvement is much more common than involvement of myocardial counterpart, and shows variable presentation which includes:
-
Acute pericarditis with or without pericardial effusion
-
Acute pericarditis with underlying myocardial involvement: myopericarditis
-
Constrictive pericarditis (CP): Effusive type or chronic calcific/fibrotic type[9]
These types of pericardial involvements show frequent overlap with each other and are not mutually exclusive. TB is a leading cause of chronic CP (CCP) in developing countries and accounts for 38 to 83% of all cases.[10] Pericardial TB is relatively common among Cardiovascular System (CVS) involvement, especially in immunocompromised individuals (acquired immunodeficiency syndrome) where tubercular effusion in pericardium reaches as high as 85%.[5]
On the other hand, TB accounts for less than 5% of cases in immunocompetent persons presenting with pericarditis[8] ([Table 1]). Ten percent of patients with TB-related pericarditis experience transient constriction, and 20 to 50% of patients proceed to overt CCP even after receiving anti-TB treatment.[11] It is possible for CP to last for several years, before symptomatic heart failure develops.[12]
Tuberculous pericarditis has four recognized pathological stages and different clinical presentation:
-
(1) Dry stage: This stage is characterized by fibrinous exudation, initial polymorphonuclear leukocytosis, and loose macrophage and T cell organization. The patient clinically presents with symptoms of acute pericarditis (chest discomfort, pericardial friction rub, and broad ST elevation without effusion).
-
(2) Effusive stage: There is pericardial effusion with predominant cellular infiltrate consisting of lymphocytes and monocytes; clinically, the patient presents with clinical features of heart failure or cardiac tamponade. Moderate to massive pericardial effusion is seen on imaging.
-
(3) Absorptive stage: There is pericardial fluid absorption and organization of exudates. Caseating granuloma formation and pericardial thickening are seen on imaging and the patient presents with clinical features of CP.
-
(4) Constrictive stage: In this stage, the clinical presentations and echocardiographic findings are consistent with CP. However, no significant fluid is seen in the pericardial cavity in this stage.
Imaging in Pericardial Tuberculosis
Echocardiography
TTE is first-line investigation of choice for pericardium evaluation owing to its easy availability, high sensitivity and specificity index, no radiation exposure, and relative cost effectiveness. TTE is routinely performed in suspected cases of myopericardial TB, for the evaluation of pericardial thickening, myocardial function, and structural and physiologic assessment ([Table 2]). However, TTE have limited diagnostic value in obese individuals, in patients with poor acoustic window, and allows limited evaluation of pericardium anterior to right ventricle (RV) and near atrioventricular (AV) groove, and is unable to identify localized effusions and characterize myocardial tissue.
Abbreviations: CT, computed tomography; f/u, follow-up; MR, magnetic resonance; RCMP, restrictive cardiomyopathy.
Echo Features of Constrictive Pericarditis
-
Pericardial thickening
-
Small tubular-shaped ventricles
-
Biatrial dilation and dilated systemic veins
-
Distorted ventricular septum (flattened/sigmoid)
-
Diastolic restriction of ventricles making it difficult to differentiate CP from restrictive cardiomyopathy (RCMP)
-
Atypical septal movement (septal bounce)
Chest X-Ray
Chest X-rays are not a routine part of evaluation of pericardial pathologies. However, they can provide an insight into the extracardiac focus of infection in lung parenchyma. Pericardial calcifications usually seen in CCP are visible on chest X-ray in roughly 50% of cases.[10] Tubercular pericardial calcification occurs specifically in the AV and interventricular grooves, as well as the inferior diaphragmatic surface of the pericardium that surrounds the ventricles (region of normal fatty areas). TB has been associated with two distinct pericardial calcification types: (1) linear and thin ([Fig. 1A, B]) which resembles eggshell calcification around the heart and was considered unique to tuberculous CP or (2) it can appear thick and shaggy.[13]

CT Scan
CT is reasonable whenever there is suspicion of loculated collection or localized pericardial thickening or TTE findings are nonconclusive for myopericardial TB[14] ([Table 2]). Further, attenuation values in CT can differentiate transudative (Hounsfield units [HU] values similar to water) from exudative effusion (higher HU values).[15] Exudative effusion is more consistent with pericardial effusion secondary to TB.
Another benefit of doing cardiac CT is its great sensitivity in detecting calcification in the pericardium ([Fig. 2]), which is usually seen in tubercular CP.

Cardiac CT features favoring CP:
-
Thickened (> 4 mm), enhancing pericardium
-
Localized adherent thickened pericardium
-
Pericardial calcification is very sensitive and strongly suggestive of tubercular etiology (lung, lymph node calcification)
-
Biatrial dilation with dilated systemic and hepatic veins (HVs)
-
Retrograde flow of contrast into inferior vena cava and HVs
-
Tubular configuration of ventricles
-
Septal bounce on retrospectively gated CT scan helps distinguish it from RCMP
-
Better evaluation of mediastinal lymph nodes and lung parenchyma to look for extracardiac focus of tubercular infection
-
Associated pericardial or pleural effusion
But because of the risk of radiation exposure, poor contrast resolution, limitation of CT in differentiating a small effusion from pericardial thickening,[13] and better CMR availability, CMR is preferred for evaluation of pericardial pathologies.
Magnetic Resonance Imaging
Magnetic resonance imaging (MRI) is the gold standard imaging modality for evaluating various pericardial diseases ([Table 2]). Its advantages include no radiation exposure, noninvasiveness, multiplanar imaging, potential for tissue characterization, large field of view, best depiction of pericardial thickness, and ability to differentiate small pericardial effusion from thickened pericardium. Disadvantages of CMR include its difficulty in identifying calcifications and the need for electrocardiogram gating (difficult to perform in patients with atrial/ventricular tachyarrhythmias).
Normal pericardium show linear hypointense signal on T1- and T2-weighted images around cardiac chamber with pericardial thickness ≤ 4 mm in normal individuals.
(1) Acute pericarditis: Cardiac MR is a gold standard imaging modality for assessment of pericardial inflammation and for therapeutic response monitoring.[16] CMR in acute pericarditis reveals thickened pericardium (> 4 mm), pericardial effusion, and can diagnose pericardial layer edema. T1 and T2 mapping values are being recently utilized to characterize pericardial effusion and assess pericardial inflammation. T1 values are significantly found to be lower in exudative pericardial effusion and a cutoff T1 value of 3013 millisecond is found to differentiate transudates from exudates acquired at 1.5T MRI[17] with a sensitivity of 94% and specificity of 79%.[18]
T1 values in inflamed pericardium are typically elevated, reflecting the presence of increased extracellular water and inflammatory cells. It has been reported that native T1 values > 1,730 millisecond had a sensitivity of 94% and specificity of 71% to diagnose moderate or greater pericardial delayed enhancement and can be used as a contrast-independent marker for detecting pericardial inflammation.[19]
A suitable method for identifying pericardial inflammation is pericardial enhancement, on gadolinium-enhanced CMR with fat-water late gadolinium enhancement (LGE) making pericardial inflammation more visible ([Fig. 3]). Other imaging features include linear enhancement of the surrounding fat and adjacent cardiac tissue, which indicates simultaneous myocardial involvement. Pericardial enhancement become more irregular in chronic pericarditis.[16]

(2) CCP: CCP is characterized by a thickened, fibrotic, rigid, and adherent pericardium which restricts diastolic filling and lead to diastolic dysfunction of ventricles and potential symptoms of right heart failure. MRI has a reported accuracy of 93% for differentiation between CP and RCMP on the basis of depiction of thickened pericardium (> 4 mm). The differentiation of CCP from RCMP is of utmost importance as CCP is managed by surgery and is usually curable whereas RCMP is treated medically and eventually require heart transplant. It is important to remember, however, that neither pericardial thickening nor calcification is diagnostic of CP unless the patient also has symptoms of physiologic constriction or restriction.
Tuberculous pericarditis causes pericardial thickness to vary in many areas (1–17 mm; mean, 4 mm) in patients with constrictive physiology (96%). However, it has been reported that up to 18 to 20% of patients with CP have a normal pericardial thickness.[20] [21]
Furthermore, CMR tagging techniques may be useful for accurately depicting fibrotic pericardial adhesions. Tag lines are usually displaced during the cardiac cycle in healthy people due to the pericardium's unrestricted mobility; however, in individuals with pericardial adhesions, these lines fail to break and appear stretched due to adhesion between pericardial layers. No pericardial enhancement is seen in fibrotic end stage of CP ([Table 3]).
|
Echocardiography |
CT |
MRI |
|
|---|---|---|---|
|
Pericardial thickening |
++ |
+ |
++ |
|
Pericardial enhancement |
− |
+ |
++ |
|
Pericardial effusion |
++ |
+ |
++ |
|
Myocardial involvement |
− |
− |
++ |
|
Pericardial calcification |
− |
++ |
– |
|
Functional evaluation |
+ |
− |
++ |
Abbreviations: CT, computed tomography; MR, magnetic resonance imaging.
Typical CMR features of CP include ([Fig. 4]):
-
Morphological: thickened pericardium (> 4 mm[22])
-
Better differentiation of pericardial fluid from pericardial thickening
-
Functional changes–cine MRI: septal flattening/septal bounce on 4 chamber and short axis cine images
-
Respiratory changes: on free deep breathing MR, accentuation of septal bounce is seen on inspiration with reversal of septal bounce on expiration
-
Right atrium (RA) and left atrium (LA) dilatation
-
If a good fat plane is seen between the pericardium and myocardium, an easier dissection during the surgery can be predicted
-
Tagging sequences: shows no distortion of grid lines at myopericardial interface suggestive of adhesion
-
Myocardial evaluation: myocardial atrophy/fibrosis, which carries a poorer prognosis even after pericardial resection
Disadvantage: Inability to identify pericardial calcification ([Table 3])[23]
Myocardial Involvement
First case of myocardial TB was reported by Maurocordat on autopsy in 1664.[16] Myocardial involvement in TB is rare, documented in up to 0.3% of individuals dying due to tuberculsosis,[24] often not diagnosed while they are alive.[25] The tuberculous myocarditis cases were predominantly seen with concomitant pulmonary infection (56%) and concomitant pericarditis (43%).[1]
Myocardial Tubercular Involvement[26]
-
Miliary tubercles of the heart, which are common in miliary TB patients, with the heart being one of several organs affected.[1]
-
Myocardial tuberculoma: Tuberculoma in heart varies from pea to egg size, with central caseation. They can involve atria, ventricles, and interventricular septum.[10]
-
Diffuse infiltrative type: Least common.
Spread
Myocardial involvement in TB can happen by:
-
Hematogenous spread from an extracardiac focus,
-
Direct spread from the adjacent lung or pericardium, or
-
Retrograde lymphatic spread from mediastinal lymph nodes.
Clinical Presentation
Myocardial tuberculomas are associated with infiltration of all myocardial layers and have variable presentation, and can remain asymptomatic or present as[27]:
-
Cardiac conduction abnormalities: Heart block, bradyarrhythmias, or tachyarrhythmias
-
Congestive heart failure
-
Acute fulminant myocarditis
-
Sudden cardiac death
-
Ventricular pseudoaneurysm, RV outflow obstruction, and coronaries involvement
-
Atrial and ventricular arrhythmia
-
Superior vena caval obstruction
-
Long QT syndrome
-
High-grade heart block
Imaging in Tubercular Myocarditis
TB is a rare cause of myocarditis which carries high mortality rate. TB myocarditis carries a low incidence rate, gradual onset, and slow progression[28] and is diagnosed mostly in postmortem study. Isolated cases of tuberculous myocarditis without involvement of any other organs are very rare with few case reports reported in literature. Tubercular myocarditis is uncommon, with reported rates of less than 2% in various case series, most of them being in immunocompromised individuals.[29]
Tuberculous myocarditis is mainly reported in “young” (< 45 years) individuals and males are more commonly affected than females (2:1).[30] Tubercular myocarditis involves most commonly the left ventricle (LV) (68%), followed by the RV (43%), RA (37%), and least LA involvement seen in 18% of the cases.[29]
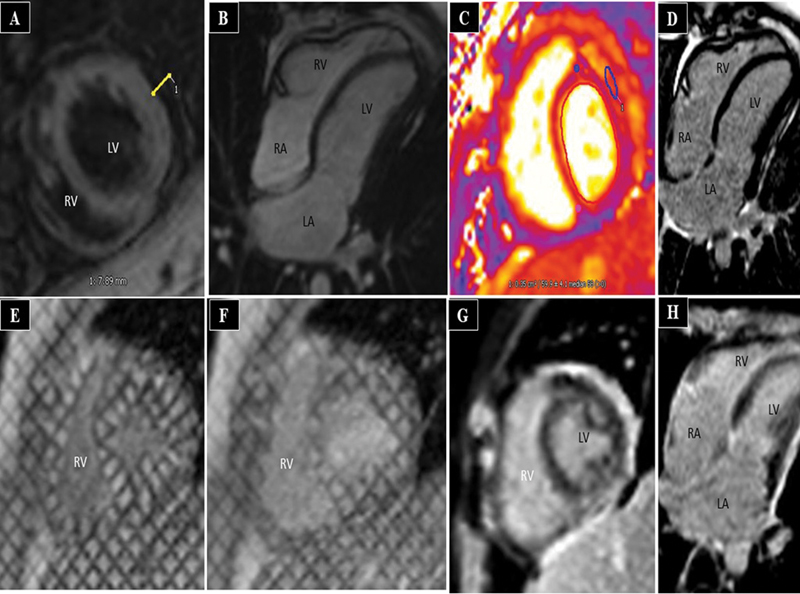
In acute phase, LV myocardium may appear hypertrophied and shows signal intensity, mapping values of myocarditis, that is, isointense to hypointense on T1- and hyperintense on T2-weighted sequences with elevated native T1 and T2 mapping values, and areas of LGE similar to CMR findings seen in other myocarditis. If cardiac TB is suspected, imaging of the thorax, head, and abdomen may indicate a primary focus, as the majority of myocardial TB cases are caused by dissemination from an extracardiac focus. Once detected, cardiac TB responds quite effectively to regular anti-TB treatment.[31]
Cardiac Tuberculoma
Myocardial tuberculomas are mass-like lesions in the heart. They are extremely rare and were found in just 19 of 13,658 postmortem cases (0.14%)[30] in an autopsy study. They commonly involve the right-sided chamber of the heart, namely, the RA wall, because of frequent involvement of the right-sided mediastinal lymph nodes or secondary to contiguous spread.
Echocardiography
TTE can accurately detect the mass, its location, and its hemodynamic impact and may reveal a hypoechoic or echogenic (calcified tuberculoma) immovable mass in the ventricular myocardium or atrial wall.
Cardiac MRI
TTE, being the first-line imaging modality, lacks specificity, and cardiac MR is the way to go for myocardial mass evaluation. Cardiac MRI provides additional advantage to TTE as it provides:
-
Better mass characterization
-
Precise location of the mass
-
Relationship to the cardiac chambers
-
Extension to the pericardium and surrounding mediastinal structures
-
Differentiate it from other cardiac masses
Typical MRI features of cardiac tuberculomas include:
-
Well-circumscribed, sharply demarcated mass from the surrounding myocardium/atrial wall[32]
-
Iso to hypo on T1- and T2-weighted images. Shortening of T2 can differentiate tuberculoma from other myocardial mass like secondary metastases or primary angiosarcoma, which appear bright on T2-weighted images
-
Classic appearance of myocardial tuberculoma is seen on T2-weighted images, that is, they typically show a central isointense core surrounded by hypointense rim and an outer thin hyperintense line. Central core correspond to caseation which are surrounded by fibrous capsule and outer infiltration by inflammatory cells
-
Post Gadolinium images: Variable enhancement is seen in post-Gd images ranging from heterogeneous LGE to ring enhancement around a central nonenhancing core with conglomeration at the periphery.
But these characteristic features of myocardial tuberculomas are rarely seen owing to rarity of disease and it can act as great masquerader of other cardiac mass.[1] In such cases, extracardiac focus of tuberculous infection may give a hint to the diagnosis. The treatment of myocardial tuberculomas primarily involves administration of antitubercular therapy (ATT) regimen. It has been reported that complete clinical and imaging disappearance of mass occurs after ATT initiation[33] ([Figs. 5] and [6]). MRI can be used for follow-up of these tuberculomas after treatment.


Papillary Muscle Involvement
Papillary muscle enlargement is a rare cardiovascular manifestation secondary to tubercular involvement which is rarely seen in clinical practice and is often an autopsy finding.[16]
Coronary Artery Disease
Studies have shown a higher association (1.75 to 2 times) of acute myocardial infarction as well as coronary atherosclerosis in TB patients in developing countries.[2] Several mechanisms are postulated behind this like:
-
Latent TB infection causes chronic inflammation and cell-mediated injuries of coronaries, eventually leading to coronary artery disease.
-
Immunological response to heat shock protein-65 (HSP65) from mycobacteria with resultant cross-reaction with human HSP65, which damages endothelium and promotes atherogenesis in coronaries.[2]
Conclusion
Pericardial and cardiac involvement in TB is an uncommon extrapulmonary manifestation of TB that can result in variable presentation ranging from heart failure, CP, or sudden cardiac death. Hence, early diagnosis of this form of extrapulmonary TB is critical to overall care. Although TTE is the screening modality for identifying pericardial and myocardial involvement in TB, advanced imaging modalities like cardiac CT and CMR give greater tissue characterization, which are usually necessary to help diagnose and differentiate it from the lesions mimicking them. Early diagnosis of cardiac TB, be it pericardial or myocardial, can help direct early institution of ATT besides deciding for and against surgical interventions in these patients. MRI remains the imaging tool of choice for deciding management and follow-up of these patients.
Conflict of Interest
None declared.
-
References
- 1 Singhal M, Kaur M, Singh H, Bahl A, Nahar U, Sharma A. Multimodality imaging of myocardial tuberculosis presenting as right ventricular cardiomyopathy: a case report. Asian Cardiovasc Thorac Ann 2023; 31 (06) 515-518
- 2 Diagnostics | Free Full-Text | Cardiovascular Involvement in Tuberculosis: From Pathophysiology to Diagnosis and Complications—A Narrative Review. Accessed January 21, 2024 At: https://www.mdpi.com/2075-4418/13/3/432
- 3 Global WHO, Report TB; 2022. Accessed January 20, 2024 at: https://pib.gov.in/pib.gov.in/Pressreleaseshare.aspx?PRID=1871626
- 4 Statistics India TB. TB Facts. Accessed December 9, 2023 at: https://tbfacts.org/tb-statistics-india/
- 5 Mayosi BM. Contemporary trends in the epidemiology and management of cardiomyopathy and pericarditis in sub-Saharan Africa. Heart 2007; 93 (10) 1176-1183
- 6 López-López JP, Posada-Martínez EL, Saldarriaga C. et al Neglected tropical diseases, other infectious diseases affecting the heart (the NET-heart Project). . Tuberculosis and the heart. J Am Heart Assoc 2021; 10 (07) e019435
- 7 Clinical characteristics and initial management of patients with tuberculous pericarditis in the HIV era: the Investigation of the Management of Pericarditis in Africa (IMPI Africa) registry | BMC Infectious Diseases | Full Text. Accessed January 21, 2024 at: https://bmcinfectdis.biomedcentral.com/articles/10.1186/1471-2334-6-2
- 8 Yang CC, Lee MH, Liu JW, Leu HS. Diagnosis of tuberculous pericarditis and treatment without corticosteroids at a tertiary teaching hospital in Taiwan: a 14-year experience. J Microbiol Immunol Infect 2005; 38 (01) 47-52
- 9 Mayosi BM, Burgess LJ, Doubell AF. Tuberculous pericarditis. Circulation. 2005; Dec 6; 112 (23) 3608-16
- 10 Fowler NO. Tuberculous pericarditis. JAMA 1991; 266 (01) 99-103
- 11 Tuberculosis and the Heart. Accessed December 9, 2023 at: https://www.ahajournals.org/doi/pdf/10.1161/JAHA.120.019435
- 12 Metaxas EI, Kotsifas K, Tatsis G, Simpsiris P, Ntanos I, Tsoukalas G. Tuberculous pericarditis: three cases and brief review. Monaldi Arch Chest Dis 2010; 73 (01) 44-50
- 13 Napolitano G, Pressacco J, Paquet E. Imaging features of constrictive pericarditis: beyond pericardial thickening. Can Assoc Radiol J 2009; 60 (01) 40-46
- 14 Cosyns B, Plein S, Nihoyanopoulos P. et al; European Association of Cardiovascular Imaging (EACVI), European Society of Cardiology Working Group (ESC WG) on Myocardial and Pericardial diseases. European Association of Cardiovascular Imaging (EACVI) position paper: multimodality imaging in pericardial disease. Eur Heart J Cardiovasc Imaging 2015; 16 (01) 12-31
- 15 Çetin MS, Özcan Çetin EH, Özdemir M. et al. Effectiveness of computed tomography attenuation values in characterization of pericardial effusion. Anatol J Cardiol 2017; 17 (04) 322-327
- 16 Das KM, Mansoori TA, Alattar YH. et al. Tuberculosis of the heart: a diagnostic challenge. Tomography 2022; 8 (04) 1649-1665
- 17 Rosmini S, Seraphim A, Captur G. et al. 247 characterisation of pleural and pericardial effusions with T1 mapping. Eur Heart J Cardiovasc Imaging 2019; 20 (Suppl. 02) jez120
- 18 Vidalakis E, Kolentinis M, Gawor M, Vasquez M, Nagel E. CMR in pericardial diseases - an update. Curr Cardiovasc Imaging Rep 2020; 13 (04) 14
- 19 Chetrit M, Chahine J, Ramchand J. et al. Abstract 13990: will native T1-mapping of the pericardium replace late gadolinium enhancement?. Circulation 2019; 140 (Suppl. 01) A13990
- 20 Masui T, Finck S, Higgins CB. Constrictive pericarditis and restrictive cardiomyopathy: evaluation with MR imaging. Radiology 1992; 182 (02) 369-373
- 21 Masui T, Finck S, Higgins CB. Constrictive pericarditis and restrictive cardiomyopathy: evaluation with MR imaging. Radiology 1992; 182 (02) 369-373
- 22 Nishimura RA. Constrictive pericarditis in the modern era: a diagnostic dilemma. Heart 2001; 86 (06) 619-623
- 23 Conte E, Revaiah PC, Tan TC. Pericardial diseases: the emerging role for cardiac magnetic resonance imaging in the diagnosis of pericardial diseases. Eur Heart J Case Rep 2022; 6 (04) ytac164
- 24 Dixit R, Chowdhury V, Singh S. Case report: myocardial tuberculosis-MRI. Indian J Radiol Imaging 2009; 19 (01) 57-59
- 25 Jeilan M, Schmitt M, McCann G, Davies J, Leverment J, Chin D. Images in cardiovascular medicine. Cardiac tuberculoma. Circulation 2008; 117 (07) 984-986
- 26 Desai N, Desai S, Chaddha U, Gable B. Tuberculous myopericarditis: a rare presentation in an immunocompetent host. BMJ Case Rep 2013; 2013 (01) bcr2012007749-bcr2012007749
- 27 Hamedanchi and Daliri - 2009 - A Vanishing Cardiac Mass.pdf. Accessed January 20, 2024 at: https://www.jto.org/article/S1556-0864(15)30966-7/pdf
- 28 Wren C, Stovin PG. Isolated interventricular septal tuberculoma causing complete heart block. Thorax 1982; 37 (02) 149-150
- 29 Michira BN, Alkizim FO, Matheka DM. Patterns and clinical manifestations of tuberculous myocarditis: a systematic review of cases. Pan Afr Med J 2015; 21: 118
- 30 Rose AG. Cardiac tuberculosis. A study of 19 patients. Arch Pathol Lab Med 1987; 111 (05) 422-426
- 31 Cantinotti M, De Gaudio M, de Martino M. et al. Intracardiac left atrial tuberculoma in an eleven-month-old infant: case report. BMC Infect Dis 2011; 11 (01) 359
- 32 Hashmani S, Tipoo Sultan FA, Masood MQ. Unusual presentation of a young man with disseminated tuberculosis and right ventricular mass. BMJ Case Rep 2016; 2016: bcr2016216964
- 33 Gulati GS, Kothari SS. Diffuse infiltrative cardiac tuberculosis. Ann Pediatr Cardiol 2011; 4 (01) 87-89
Address for correspondence
Publication History
Article published online:
02 August 2024
© 2024. Indographics. This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/)
Thieme Medical and Scientific Publishers Pvt. Ltd.
A-12, 2nd Floor, Sector 2, Noida-201301 UP, India
-
References
- 1 Singhal M, Kaur M, Singh H, Bahl A, Nahar U, Sharma A. Multimodality imaging of myocardial tuberculosis presenting as right ventricular cardiomyopathy: a case report. Asian Cardiovasc Thorac Ann 2023; 31 (06) 515-518
- 2 Diagnostics | Free Full-Text | Cardiovascular Involvement in Tuberculosis: From Pathophysiology to Diagnosis and Complications—A Narrative Review. Accessed January 21, 2024 At: https://www.mdpi.com/2075-4418/13/3/432
- 3 Global WHO, Report TB; 2022. Accessed January 20, 2024 at: https://pib.gov.in/pib.gov.in/Pressreleaseshare.aspx?PRID=1871626
- 4 Statistics India TB. TB Facts. Accessed December 9, 2023 at: https://tbfacts.org/tb-statistics-india/
- 5 Mayosi BM. Contemporary trends in the epidemiology and management of cardiomyopathy and pericarditis in sub-Saharan Africa. Heart 2007; 93 (10) 1176-1183
- 6 López-López JP, Posada-Martínez EL, Saldarriaga C. et al Neglected tropical diseases, other infectious diseases affecting the heart (the NET-heart Project). . Tuberculosis and the heart. J Am Heart Assoc 2021; 10 (07) e019435
- 7 Clinical characteristics and initial management of patients with tuberculous pericarditis in the HIV era: the Investigation of the Management of Pericarditis in Africa (IMPI Africa) registry | BMC Infectious Diseases | Full Text. Accessed January 21, 2024 at: https://bmcinfectdis.biomedcentral.com/articles/10.1186/1471-2334-6-2
- 8 Yang CC, Lee MH, Liu JW, Leu HS. Diagnosis of tuberculous pericarditis and treatment without corticosteroids at a tertiary teaching hospital in Taiwan: a 14-year experience. J Microbiol Immunol Infect 2005; 38 (01) 47-52
- 9 Mayosi BM, Burgess LJ, Doubell AF. Tuberculous pericarditis. Circulation. 2005; Dec 6; 112 (23) 3608-16
- 10 Fowler NO. Tuberculous pericarditis. JAMA 1991; 266 (01) 99-103
- 11 Tuberculosis and the Heart. Accessed December 9, 2023 at: https://www.ahajournals.org/doi/pdf/10.1161/JAHA.120.019435
- 12 Metaxas EI, Kotsifas K, Tatsis G, Simpsiris P, Ntanos I, Tsoukalas G. Tuberculous pericarditis: three cases and brief review. Monaldi Arch Chest Dis 2010; 73 (01) 44-50
- 13 Napolitano G, Pressacco J, Paquet E. Imaging features of constrictive pericarditis: beyond pericardial thickening. Can Assoc Radiol J 2009; 60 (01) 40-46
- 14 Cosyns B, Plein S, Nihoyanopoulos P. et al; European Association of Cardiovascular Imaging (EACVI), European Society of Cardiology Working Group (ESC WG) on Myocardial and Pericardial diseases. European Association of Cardiovascular Imaging (EACVI) position paper: multimodality imaging in pericardial disease. Eur Heart J Cardiovasc Imaging 2015; 16 (01) 12-31
- 15 Çetin MS, Özcan Çetin EH, Özdemir M. et al. Effectiveness of computed tomography attenuation values in characterization of pericardial effusion. Anatol J Cardiol 2017; 17 (04) 322-327
- 16 Das KM, Mansoori TA, Alattar YH. et al. Tuberculosis of the heart: a diagnostic challenge. Tomography 2022; 8 (04) 1649-1665
- 17 Rosmini S, Seraphim A, Captur G. et al. 247 characterisation of pleural and pericardial effusions with T1 mapping. Eur Heart J Cardiovasc Imaging 2019; 20 (Suppl. 02) jez120
- 18 Vidalakis E, Kolentinis M, Gawor M, Vasquez M, Nagel E. CMR in pericardial diseases - an update. Curr Cardiovasc Imaging Rep 2020; 13 (04) 14
- 19 Chetrit M, Chahine J, Ramchand J. et al. Abstract 13990: will native T1-mapping of the pericardium replace late gadolinium enhancement?. Circulation 2019; 140 (Suppl. 01) A13990
- 20 Masui T, Finck S, Higgins CB. Constrictive pericarditis and restrictive cardiomyopathy: evaluation with MR imaging. Radiology 1992; 182 (02) 369-373
- 21 Masui T, Finck S, Higgins CB. Constrictive pericarditis and restrictive cardiomyopathy: evaluation with MR imaging. Radiology 1992; 182 (02) 369-373
- 22 Nishimura RA. Constrictive pericarditis in the modern era: a diagnostic dilemma. Heart 2001; 86 (06) 619-623
- 23 Conte E, Revaiah PC, Tan TC. Pericardial diseases: the emerging role for cardiac magnetic resonance imaging in the diagnosis of pericardial diseases. Eur Heart J Case Rep 2022; 6 (04) ytac164
- 24 Dixit R, Chowdhury V, Singh S. Case report: myocardial tuberculosis-MRI. Indian J Radiol Imaging 2009; 19 (01) 57-59
- 25 Jeilan M, Schmitt M, McCann G, Davies J, Leverment J, Chin D. Images in cardiovascular medicine. Cardiac tuberculoma. Circulation 2008; 117 (07) 984-986
- 26 Desai N, Desai S, Chaddha U, Gable B. Tuberculous myopericarditis: a rare presentation in an immunocompetent host. BMJ Case Rep 2013; 2013 (01) bcr2012007749-bcr2012007749
- 27 Hamedanchi and Daliri - 2009 - A Vanishing Cardiac Mass.pdf. Accessed January 20, 2024 at: https://www.jto.org/article/S1556-0864(15)30966-7/pdf
- 28 Wren C, Stovin PG. Isolated interventricular septal tuberculoma causing complete heart block. Thorax 1982; 37 (02) 149-150
- 29 Michira BN, Alkizim FO, Matheka DM. Patterns and clinical manifestations of tuberculous myocarditis: a systematic review of cases. Pan Afr Med J 2015; 21: 118
- 30 Rose AG. Cardiac tuberculosis. A study of 19 patients. Arch Pathol Lab Med 1987; 111 (05) 422-426
- 31 Cantinotti M, De Gaudio M, de Martino M. et al. Intracardiac left atrial tuberculoma in an eleven-month-old infant: case report. BMC Infect Dis 2011; 11 (01) 359
- 32 Hashmani S, Tipoo Sultan FA, Masood MQ. Unusual presentation of a young man with disseminated tuberculosis and right ventricular mass. BMJ Case Rep 2016; 2016: bcr2016216964
- 33 Gulati GS, Kothari SS. Diffuse infiltrative cardiac tuberculosis. Ann Pediatr Cardiol 2011; 4 (01) 87-89