

Subscribe to RSS
DOI: 10.1055/s-0044-1789273
Low-Compared with High-Dose Regimen of Induction Chemotherapy in Locally Advanced Nasopharyngeal Cancer: A Systematic Review and Meta-analysis
Authors

Abstract
Introduction
International recommendation supports induction chemotherapy (IC) followed by concurrent chemoradiotherapy (CCRT) as a new standard of care for locally advanced nasopharyngeal cancer (LA-NPC) which give a survival benefit. TPF is one of the IC regimens which consists of docetaxel (75 mg/m2, 1 hour infusion), cisplatin (75 mg/m2, 0.5–3 hours), and 5-fluorouracil (600 mg/m2, 4 days). Previous retrospective study in Chinese population reported low-dose TPF (L-TPF), consists of docetaxel (60 mg/m2), cisplatin (65 mg/m2), and then 5-fluorouracil (550 mg/m2/d; 5 days), showed better tolerance and compliance rates, with similar efficacy to high-dose TPF (H-TPF). Thus, we aim to evaluate the current evidence of the effect of L-TPF compared with H-TPF on survival and tolerance as IC in LA-NPC.
Methods
Data were collected from PubMed, PubMed Central, and Science Direct, using combinations of keywords related to neoadjuvant chemotherapy (NAC) or IC, TPF dose regimen, and LA-NPC. The included studies investigated the efficacy and toxicity of IC with a TPF regimen. The quality of each included study was assessed using the Newcastle–Ottawa scale for cohort studies and the JADAD scale for randomized controlled trial (RCT). Only moderate- and good-quality studies were further evaluated in the meta-analysis.
Results
A total of six studies consisting of 509 NAC patients were included. All the studies evaluated overall survival (OS) and progression-free survival (PFS). Quantitative analysis showed that L-TPF + CCRT significantly showed good OS (hazard ratio [HR] = 0.50; 95% confidence interval [CI], 0.33–0.76; p = 0.001) but not PFS (HR = 0.45; 95% CI, 0.16–1.25; p = 0.13). Common chemotoxicities that were found in both groups were neutropenia and anemia.
Conclusion
L-TPF IC had a significant positive effect on the survival of LA-NPC patients. Further, larger multicenter RCT studies are needed to focus on evaluating the optimal TPF regimen dose in LA-NPC.
Introduction
Nasopharyngeal carcinoma (NPC) is one of the most common aggressive malignancies of the head and neck, which is highly endemic in Southeast Asia, North Africa, and Southern China. According to the Global Cancer Statistics, there were 133,354 new cases of NPC diagnosed and 80,008 deaths occurred worldwide in 2020.[1] The initial presentation of NPC is atypical and unspecific, which can be manifested as pain in the nose, ears, neck, or head. As a result, up to 80% of NPC were diagnosed at locally advanced stage.[2]
Due to its anatomical location near critical structures, surgical treatment is not the main strategy for NPC. NPC is sensitive to chemoradiation; therefore, the mainstay of NPC treatment is the combination of radiotherapy and chemotherapy (concurrent chemoradiotherapy [CCRT]). Several studies had reported that induction chemotherapy (IC) followed by CCRT was superior to CCRT alone for locally advanced nasopharyngeal cancer (LA-NPC), manifesting as higher overall survival (OS), progression-free survival (PFS), and distant metastasis-free survival (DMFS).[3] [4] [5] [6]
The combination of IC + CCRT is recommended in the latest National Comprehensive Cancer Network Guidelines, with not only survival benefits but also early alleviation of symptoms, better radiotherapy compliance with reduced targets, and elimination of small metastatic lesions which is the main failure pattern of LA-NPC.[7] [8]
TPF is one of the IC regimens which consists of docetaxel, cisplatin, and 5-fluorouracil. A randomized controlled trial (RCT) by Sun et al reported that TPF IC followed by CCRT significantly improved OS, DMFS, and failure-free survival compared with CCRT alone.[9] Previous retrospective studies in Chinese patients reported low-dose TPF (L-TPF), consists of docetaxel (60 mg/m2), cisplatin (65 mg/m2), and then 5-fluorouracil (550 mg/m2/d; 5 days), showed better tolerance and compliance rates, and similar efficacy to high-dose TPF (H-TPF) (docetaxel [75 mg/m2; 1 hour infusion], cisplatin [75 mg/m2; 0.5–3 hours], and then 5-fluorouracil [600 mg/m2/d; 4 days]). NPC patients receiving H-TPF had more frequent treatment delays due to chemotoxicity, such as grades 3 and 4 anemia, thrombocytopenia, and neutropenia.[10]
The optimal dose of TPF in IC + CCRT for NPC patients is still unclear. Thus, we aim to evaluate the effect of L-TPF + CCRT and H-TPF + CCRT on survival and chemotoxicity in LA-NPC patients.
Materials and Methods
Search Strategy
This systematic review has been registered in PROSPERO (international database of prospectively registered systematic reviews) (CRD42023483635). A literature search for this systematic review was conducted in online resources, including PubMed, PubMed Central (PMC), and Science Direct. The literature search was done from November 13–16, 2023, using keywords related to NPC, TPF regimen, survival, and chemotoxicity (listed in [Table 1]). Systematic analysis approaches were used in this study, including PICO analysis (P: LA-NPC patients of any age; I: L-TPF regimen; C: H-TPF regimen; O: OS, PFS, and chemotoxicity).
The studies that we included are cohort studies or RCTs with participants of any age, who were diagnosed with LA-NPC. The participants were treated with systemic chemotherapeutic agents with or without radiotherapy. The studies must report data of survival, including OS and PFS, and chemotherapy toxicity. The studies must be in English language and published by the end of October 2023. Unpublished articles, abstracts or lectures, dissertations, books and book chapters, editorials, online articles, letters to the editor or opinion pieces, poster or conference presentations, case reports, case series, meta-analyses, animal studies, cross-sectional, case–control studies, systematic reviews, and literature reviews were excluded. We also excluded studies with reported opinions or outcomes through nonstandardized questionnaires or studies with other main outcomes, such as psychological outcomes. Studies that include patients with pregnancy or lactating females or other types of cancer as primary exposure were also excluded. Studies that include patients with cardiac arrhythmia, coronary heart disease, peripheral neuropathy, or any psychiatric disorders that may affect treatment compliance were also excluded.
Data selection, extraction, and analysis were conducted by two independent reviewers. Any dissimilarities were resolved through discussing with the third author and reaching a general agreement between the reviewers. The reviewers evaluated the titles and abstracts for all selected studies using the PRISMA search strategy. Relevant titles and abstracts from each database were chosen. If there is limited information for the reviewers to determine the inclusion and exclusion criteria, the full texts will be evaluated. References that are found in the included and excluded articles were reviewed to discover studies that failed to be included through the primary search.
Data Extraction
Data regarding authors' name; year of publication; study design; country of the study; inclusion and exclusion criteria; mean age of study population; population size and NPC stage; TPF regimen dose; and main outcomes (OS, PFS, and chemotoxicity) were extracted by at least two reviewers.
Collective article reviews were performed on three databases. Full-text articles of the appropriate studies were read and assessed. Quality assessment is conducted according to the Newcastle–Ottawa scale (NOS) for cohort studies and the JADAD scale for RCT with minimal two reviewers.[11] The study selection process is illustrated in a flow diagram ([Fig. 1]).[12]

Outcome Definitions
Primary outcome includes OS, PFS, and chemotoxicity. OS is defined as the length of time from either the date of diagnosis or the start of treatment for a disease, such as cancer, that patients diagnosed with the disease are still alive.[13] PFS is defined as the length of time during and after the treatment of a disease, such as cancer, that a patient lives with the disease, but it does not get worse.[14] Chemotoxicity is toxicity due to chemical effects, especially the effects of chemotherapy.[15]
Quality Assessment
The quality of the included cohort studies was assessed using the NOS. The three domains assessed included: (1) selection of study groups (four points), (2) comparability of the groups (two points), and (3) assessment of the outcome (three points). A score of 5 or less was considered poor, 6 or 7 was considered moderate, and 8 or 9 was considered good quality.[11] JADAD scale was used for assessing RCTs. The JADAD scale is a five-point scale for evaluating the quality of randomized trials in which three points or more indicate superior quality. The scale contains two questions each for randomization and masking, and one question evaluating reporting of withdrawals and dropouts. Studies with poor quality will be excluded.[16]
Two independent researchers assessed the quality of methods and standard of outcome reporting in the included studies. Disagreements between the researchers were resolved through consensus or the opinion of a third reviewer. The quality of evidence assessment using the GRADE (Cochrane Group) analysis of findings was not done.
Statistical Analysis
RevMan version 5.4 software (Cochrane Collaboration) was used to conduct the meta-analysis. Hazard ratio (HR) and its 95% confidence interval (CI) were used to evaluate OS and PFS. We estimated the HR and 95% CI based on the method by Tierney et al if there is no available data on HRs and 95% CI from the study.[17] Inconsistency index (I 2) test, ranging from 0 to 100%, was used to assess heterogeneity of the studies. If the value of I 2 >50% or p < 0.10, it indicates that the heterogeneity is statistically significant, and therefore, random-effect model was used.[18] All p-values in this meta-analysis were two-tailed, and the statistical significance was set at ≤0.05. Subgroup analyses were performed by classifying studies according to regions. If meta-analysis could not be conducted, study results were presented descriptively.
Results
Literature Search
The initial search through online databases identified a total of 657 studies, with 12 studies from PubMed, 462 studies from PMC, 166 studies from Science Direct, and 17 studies identified through literature or other sources. The search process was followed by the screening of titles and abstracts, and the remaining studies were further assessed for eligibility. After a series of selections according to inclusion criteria and exclusion of duplicated studies, we acquired six studies for this systematic review and meta-analysis. The selection process is shown in [Fig. 1].
Quality Assessment
The result of the quality assessment is presented in [Table 2]. According to the NOS quality assessment, there was one study with good quality and three studies with moderate quality. Two RCT studies were assessed using the JADAD scale and both were high quality. There was no study with poor quality; therefore, all the studies were included in this review.
Abbreviation: RCT, randomized controlled trial.
Star symbol Indicates points.
Characteristics of the Included Studies
The characteristics of the included studies are presented in [Table 3]. A total of six studies were included in this quantitative analysis. There were two RCTs and four cohort studies. The studies were published between the year 2016 and 2022. The countries of the studies are China, Japan, Jordan, France, and Tunisia. All the included studies had evaluated OS and PFS.
Abbreviations: CCRT, concurrent chemoradiotherapy; CI, confidence interval; HR, hazard ratio; H-TPF, high-TPF; L-TPF, low-TPF; NAC, neoadjuvant chemotherapy; OS, overall survival; PFS, progression-free survival; RCT, randomized controlled trial; TNM, Tumor Node Metastasis.
Characteristics of the Studied Population
The studies consisted of 503 nasopharyngeal cancer patients, with TNM staging of II to IVb. All patients underwent IC with a TPF regimen plus CCRT. Three of the studies used L-TPF with a similar range of dose regimens. Dose regimens of L-TPF by Sun et al were docetaxel (60 mg/m2) on day 1, cisplatin (60 mg/m2) on day 1, and 5-fluorouracil (600 mg/m2) per day as a continuous 120-hour infusion on days 1 to 5.[9] Dose regimens by Kawahira et al were docetaxel (60–70 mg/m2) on day 1, cisplatin (60–70 mg/m2) on day 1, and 5-fluorouracil (750 mg/m2) per day as a continuous 120-hour infusion on days 1 to 5.[19] Meanwhile, Zhu et al used docetaxel (60 mg/m2) on day 1, cisplatin (20–25 mg/m2) on day 1, and 5-fluorouracil (600 mg/m2) per day as a continuous 120-hour infusion on days 1 to 5.[20] Three other studies used H-TPF which consisted of docetaxel (75 mg/m2) on day 1, cisplatin (75 mg/m2) on day 1, and 5-fluorouracil (750–1,000 mg/m2/d) on days 1 to 5.[21] [22] [23]
Primary Outcomes
Overall Survival
A total of six studies evaluated OS in NPC patients receiving L-TPF or H-TPF.[9] [19] [20] [21] [22] [23] The population of patients receiving L-TPF and H-TPF were 340 and 163 patients, respectively. The synthesized result of OS is presented in [Fig. 2]. There was no significant heterogeneity found (I 2 = 0% and p > 0.10); therefore, the fixed-effect model was used. We found that L-TPF was significantly associated with improved OS, with a pooled HR of 0.50 (95% CI, 0.33–0.76; p = 0.001). H-TPF was not significantly associated with improved OS in NPC patients (p = 0.08).

Progression-Free Survival
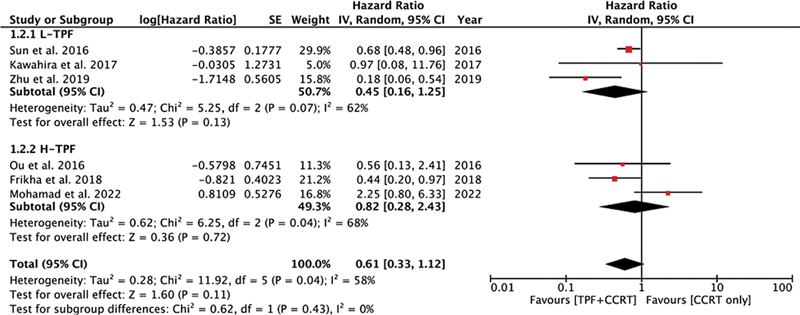
All the included studies evaluated PFS in NPC patients receiving L-TPF or H-TPF.[9] [19] [20] [21] [22] [23] The synthesized result of PFS is presented in [Fig. 3]. Random-effect model was used due to the presence of significant heterogeneity found among studies (I 2 >50% and p < 0.10). We found that both L-TPF and H-TPF were not associated with improved PFS in NPC patients (p = 0.13 and p = 0.72, respectively).
Chemotherapy Toxicity
Chemotherapy toxicity was reported in all recruited studies. However, due to limited data available from the studies, analysis was not done. Studies with L-TPF had reported similar incidence of grades 3 and 4 chemotoxicity. Among these, neutropenia, febrile neutropenia, leukopenia, stomatitis, and anorexia were the most prevalent.[9] [19] [20] Conversely, H-TPF + CCRT, as studied by Ou et al, demonstrated less total cumulative incidence of grades 3 and 4 toxicities than CCRT only.[21] However, studies by Frikha et al and Mohamad et al had contrasting results. Frikha et al reported a similar rate of grades 3 and 4 toxicity in the H-TPF + CCRT group and CCRT-only group, mainly neutropenia, febrile neutropenia, mucositis, alopecia, and asthenia.[22] Study by Mohamad et al reported more frequent grade 2 anemia, late grade 2 brain toxicity, and late grade 2 dysphagia in the H-TPF group.[23]
Discussion
This systematic review examined survival and chemotherapy toxicity in NPC patients undergoing different TPF dose regimens. The results indicated that both L-TPF and H-TPF were not associated with improved PFS in NPC patients. Conversely, L-TPF significantly improved OS in NPC patients. However, H-TPF did not show significant improvement in terms of OS. Patients in the L-TPF group had better tolerance and compliance rates than H-TPF, suggesting L-TPF may be a more effective treatment option for improving survival outcomes. This may be because of the increased toxicity in H-TPF regimens that delayed further chemotherapy schedule and this may impact the survival. However, further investigation into factors contributing to the reduced efficacy of H-TPF compared with L-TPF may be warranted.
In 2017, Jin et al compared the efficacy and toxicity between L-TPF and H-TPF in NPC patients. The study reported that L-TPF was superior to H-TPF in terms of survival and chemotoxicities. The result could be attributed to multiple factors. Treatment delays were more common in the H-TPF group than in the L-TPF group (33.3 vs. 19.4%, p = 0.034), which could counteract any possible survival benefits of H-TPF by allowing tumor cell proliferation.[10] Previous research by Lee et al and Loong et al showed that OS and locoregional control were significantly impacted by the total dose of cisplatin given during CCRT.[24] [25] According to Jin et al, there were fewer patients in the H-TPF group that finished two cycles of concurrent cisplatin (p < 0.001). This was due to hematologic and nonhematologic adverse events in the H-TPF group that restrict the completion of treatment.[10]
Chemotoxicity and adverse events were the major problems causing incomplete treatment cycles, particularly in H-TPF patients. However, our included studies had inconsistent results. The included studies demonstrated that both hematological toxicities, such as anemia and leukopenia, and nonhematological toxicities, such as stomatitis, mucositis, and anorexia, were common in L-TPF patients. One study had reported that H-TPF was associated with less total cumulative incidence of grades 3 and 4 adverse events. Another study had shown a similar rate of grades 3 and 4 toxicity in the H-TPF + CCRT group and CCRT-only group. Meanwhile, Mohamad et al reported more frequent adverse events, such as grade 2 anemia, late grade 2 brain toxicity, and late grade 2 dysphagia in the H-TPF group. Further investigations regarding the chemotherapy toxicity effect of different TPF dose regimens are required.
There were several limitations in this analysis. The limited number of samples and included studies may cause a limitation of the power of pooled results for survival analysis. There were also differences in the dose regimen of cisplatin and 5-fluorouracil in both L-TPF and H-TPF groups which may cause bias in the result. Analysis of chemotoxicity was not done due to limited data from the included studies.
One of the strengths of our study is that all studies with poor quality were excluded from this review. Thus, all the included studies were of moderate and good qualities. Our review focused on LA-NPC patients only; therefore, it is more specific.
Understanding the literature support for these findings further strengthens the implications for clinical practice and emphasizes the need for continued research to elucidate the factors underlying the differential outcomes between L-TPF and H-TPF in NPC patients. By building upon the existing evidence, future studies can contribute to a more comprehensive understanding of the efficacy and mechanisms of these treatment regimens.
Implications for Clinical Practice
The findings that support the superiority of L-TPF over H-TPF in terms of survival in NPC patients have significant implications for clinical practice. The consideration of the mechanistic dissimilarities, toxicity profiles, and patient-specific factors can guide oncologists in making informed decisions regarding the selection of treatment regimens for NPC.
Beyond the comparison of L-TPF and H-TPF, the challenges in treatment selection and patient care in NPC are multifaceted. The complexity of NPC, which may involve tumor staging, histological subtypes, and individual variations in disease progression, necessitates a patient-specific approach to treatment decision-making. Factors such as the presence of distant metastases, involvement of critical structures in the head and neck region, and the potential for chemotherapy toxicities further emphasize the need for personalized care pathways for NPC patients.
The management of NPC often involves a multimodal treatment approach, which may include a combination of chemotherapy, radiotherapy, and in some cases, targeted therapies, or immunotherapies. Understanding the interplay between these modalities and their potential additive or synergistic effects is crucial for optimizing treatment outcomes. Additionally, the sequencing of these modalities and their timing in relation to disease progression represents a dynamic area of research and clinical decision-making.
Conclusion
The comparison of L-TPF and H-TPF in NPC patients has revealed important considerations for clinical practice and patient care. The superior OS and better tolerance associated with L-TPF exhibit its potential as a preferred treatment regimen for NPC patients. Further, larger multicenter RCT studies are needed to focus on evaluating the optimal TPF regimen dose in LA-NPC. However, the diverse nature of NPC and the complexities involved in treatment selection and patient care necessitate a tailored and multidisciplinary approach. The insights gained from this analysis highlight the need for personalized treatment strategies that consider not only the efficacy of a given regimen but also its tolerability, impact on patient quality of life, and potential toxicities.
Conflict of Interest
None declared.
-
References
- 1 Sung H, Ferlay J, Siegel RL. et al. Global cancer statistics 2020: GlOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin 2021; 71 (03) 209-249
- 2 Mao YP, Xie FY, Liu LZ. et al. Re-evaluation of 6th edition of AJCC staging system for nasopharyngeal carcinoma and proposed improvement based on magnetic resonance imaging. Int J Radiat Oncol Biol Phys 2009; 73 (05) 1326-1334
- 3 Blanchard P, Lee A, Marguet S. et al; MAC-NPC Collaborative Group. Chemotherapy and radiotherapy in nasopharyngeal carcinoma: an update of the MAC-NPC meta-analysis. Lancet Oncol 2015; 16 (06) 645-655
- 4 Li WF, Chen NY, Zhang N. et al. Concurrent chemoradiotherapy with/without induction chemotherapy in locoregionally advanced nasopharyngeal carcinoma: long-term results of phase 3 randomized controlled trial. Int J Cancer 2019; 145 (01) 295-305
- 5 Liang ZG, Zhu XD, Tan AH. et al. Induction chemotherapy followed by concurrent chemoradiotherapy versus concurrent chemoradiotherapy with or without adjuvant chemotherapy for locoregionally advanced nasopharyngeal carcinoma: meta-analysis of 1,096 patients from 11 randomized controlled trials. Asian Pac J Cancer Prev 2013; 14 (01) 515-521
- 6 Zhou R, Zhu J, Chen X, Liu Y, Wang Y, Zhang T. The efficacy and safety of docetaxel, cisplatin and fluorouracil (TPF)-based induction chemotherapy followed by concurrent chemoradiotherapy for locoregionally advanced nasopharyngeal carcinoma: a meta-analysis. Clin Transl Oncol 2020; 22 (03) 429-439
- 7 Wu LR, Liu YT, Jiang N. et al. Ten-year survival outcomes for patients with nasopharyngeal carcinoma receiving intensity-modulated radiotherapy: an analysis of 614 patients from a single center. Oral Oncol 2017; 69: 26-32
- 8 Chua DTT, Ma J, Sham JST. et al. Long-term survival after cisplatin-based induction chemotherapy and radiotherapy for nasopharyngeal carcinoma: a pooled data analysis of two phase III trials. J Clin Oncol 2005; 23 (06) 1118-1124
- 9 Sun Y, Li WF, Chen NY. et al. Induction chemotherapy plus concurrent chemoradiotherapy versus concurrent chemoradiotherapy alone in locoregionally advanced nasopharyngeal carcinoma: a phase 3, multicentre, randomised controlled trial. Lancet Oncol 2016; 17 (11) 1509-1520
- 10 Jin T, Zhang Q, Jiang F. et al. Neoadjuvant chemotherapy with different dose regimens of docetaxel, cisplatin and fluorouracil (TPF) for locoregionally advanced nasopharyngeal carcinoma: a retrospective study. Oncotarget 2017; 8 (59) 100764-100772
- 11 Lo CKL, Mertz D, Loeb M. Newcastle-Ottawa scale: comparing reviewers' to authors' assessments. BMC Med Res Methodol 2014; 14 (01) 45
- 12 Moher D, Liberati A, Tetzlaff J, Altman DG. PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med 2009; 6 (07) e1000097
- 13 Definition of overall survival-NCI dictionary of cancer terms; national cancer Institute (Internet). Accessed July 14, 2020 at: https://www.cancer.gov/publications/dictionaries/cancer-terms/def/overall-survival
- 14 Definition of progression-free survival- NCI dictionary of cancer terms- National cancer institute (Internet). Accessed July 14, 2020 at: https://www.cancer.gov/publications/dictionaries/cancer-terms/def/progression-free-survival
- 15 Ghom AG, Mhaske S. Textbook of Oral Pathology. 2nd ed.. India: Jaypee Brothers, Medical Publishers Pvt. Limited; 2013: 1025
- 16 Augestad KM, Berntsen G, Lassen K, Bellika JG, Wootton R, Lindsetmo RO. Study Group of Research Quality in Medical Informatics and Decision Support (SQUID). Standards for reporting randomized controlled trials in medical informatics: a systematic review of CONSORT adherence in RCTs on clinical decision support. J Am Med Inform Assoc 2012; 19 (01) 13-21
- 17 Tierney JF, Stewart LA, Ghersi D, Burdett S, Sydes MR. Practical methods for incorporating summary time-to-event data into meta-analysis. Trials 2007; 8 (01) 16
- 18 Higgins JPT, Thompson SG, Deeks JJ, Altman DG. Measuring inconsistency in meta-analyses. BMJ 2003; 327 (7414): 557-560
- 19 Kawahira M, Yokota T, Hamauchi S. et al. Survival benefit of adding docetaxel, cisplatin, and 5-fluorouracil induction chemotherapy to concurrent chemoradiotherapy for locally advanced nasopharyngeal carcinoma with nodal Stage N2-3. Jpn J Clin Oncol 2017; 47 (08) 705-712
- 20 Zhu J, Duan B, Shi H. et al. Comparison of GP and TPF induction chemotherapy for locally advanced nasopharyngeal carcinoma. Oral Oncol 2019; 97: 37-43
- 21 Ou D, Blanchard P, El Khoury C. et al. Induction chemotherapy with docetaxel, cisplatin and fluorouracil followed by concurrent chemoradiotherapy or chemoradiotherapy alone in locally advanced non-endemic nasopharyngeal carcinoma. Oral Oncol 2016; 62: 114-121
- 22 Frikha M, Auperin A, Tao Y. et al; GORTEC. A randomized trial of induction docetaxel-cisplatin-5FU followed by concomitant cisplatin-RT versus concomitant cisplatin-RT in nasopharyngeal carcinoma (GORTEC 2006-02). Ann Oncol 2018; 29 (03) 731-736
- 23 Mohamad I, Abu-Hijleh F, Mayta E. et al. Comparison of two standard treatment approached in locoregionanly advanced nasopharyngeal carcinoma. South Asian J Cancer 2022; 11 (03) 223-228
- 24 Lee AWM, Tung SY, Ngan RKC. et al. Factors contributing to the efficacy of concurrent-adjuvant chemotherapy for locoregionally advanced nasopharyngeal carcinoma: combined analyses of NPC-9901 and NPC-9902 Trials. Eur J Cancer 2011; 47 (05) 656-666
- 25 Loong HH, Ma BBY, Leung SF. et al. Prognostic significance of the total dose of cisplatin administered during concurrent chemoradiotherapy in patients with locoregionally advanced nasopharyngeal carcinoma. Radiother Oncol 2012; 104 (03) 300-304
Address for correspondence
Publication History
Received: 29 March 2024
Accepted: 26 July 2024
Article published online:
23 August 2024
© 2024. MedIntel Services Pvt Ltd. This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/)
Thieme Medical and Scientific Publishers Pvt. Ltd.
A-12, 2nd Floor, Sector 2, Noida-201301 UP, India
-
References
- 1 Sung H, Ferlay J, Siegel RL. et al. Global cancer statistics 2020: GlOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin 2021; 71 (03) 209-249
- 2 Mao YP, Xie FY, Liu LZ. et al. Re-evaluation of 6th edition of AJCC staging system for nasopharyngeal carcinoma and proposed improvement based on magnetic resonance imaging. Int J Radiat Oncol Biol Phys 2009; 73 (05) 1326-1334
- 3 Blanchard P, Lee A, Marguet S. et al; MAC-NPC Collaborative Group. Chemotherapy and radiotherapy in nasopharyngeal carcinoma: an update of the MAC-NPC meta-analysis. Lancet Oncol 2015; 16 (06) 645-655
- 4 Li WF, Chen NY, Zhang N. et al. Concurrent chemoradiotherapy with/without induction chemotherapy in locoregionally advanced nasopharyngeal carcinoma: long-term results of phase 3 randomized controlled trial. Int J Cancer 2019; 145 (01) 295-305
- 5 Liang ZG, Zhu XD, Tan AH. et al. Induction chemotherapy followed by concurrent chemoradiotherapy versus concurrent chemoradiotherapy with or without adjuvant chemotherapy for locoregionally advanced nasopharyngeal carcinoma: meta-analysis of 1,096 patients from 11 randomized controlled trials. Asian Pac J Cancer Prev 2013; 14 (01) 515-521
- 6 Zhou R, Zhu J, Chen X, Liu Y, Wang Y, Zhang T. The efficacy and safety of docetaxel, cisplatin and fluorouracil (TPF)-based induction chemotherapy followed by concurrent chemoradiotherapy for locoregionally advanced nasopharyngeal carcinoma: a meta-analysis. Clin Transl Oncol 2020; 22 (03) 429-439
- 7 Wu LR, Liu YT, Jiang N. et al. Ten-year survival outcomes for patients with nasopharyngeal carcinoma receiving intensity-modulated radiotherapy: an analysis of 614 patients from a single center. Oral Oncol 2017; 69: 26-32
- 8 Chua DTT, Ma J, Sham JST. et al. Long-term survival after cisplatin-based induction chemotherapy and radiotherapy for nasopharyngeal carcinoma: a pooled data analysis of two phase III trials. J Clin Oncol 2005; 23 (06) 1118-1124
- 9 Sun Y, Li WF, Chen NY. et al. Induction chemotherapy plus concurrent chemoradiotherapy versus concurrent chemoradiotherapy alone in locoregionally advanced nasopharyngeal carcinoma: a phase 3, multicentre, randomised controlled trial. Lancet Oncol 2016; 17 (11) 1509-1520
- 10 Jin T, Zhang Q, Jiang F. et al. Neoadjuvant chemotherapy with different dose regimens of docetaxel, cisplatin and fluorouracil (TPF) for locoregionally advanced nasopharyngeal carcinoma: a retrospective study. Oncotarget 2017; 8 (59) 100764-100772
- 11 Lo CKL, Mertz D, Loeb M. Newcastle-Ottawa scale: comparing reviewers' to authors' assessments. BMC Med Res Methodol 2014; 14 (01) 45
- 12 Moher D, Liberati A, Tetzlaff J, Altman DG. PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med 2009; 6 (07) e1000097
- 13 Definition of overall survival-NCI dictionary of cancer terms; national cancer Institute (Internet). Accessed July 14, 2020 at: https://www.cancer.gov/publications/dictionaries/cancer-terms/def/overall-survival
- 14 Definition of progression-free survival- NCI dictionary of cancer terms- National cancer institute (Internet). Accessed July 14, 2020 at: https://www.cancer.gov/publications/dictionaries/cancer-terms/def/progression-free-survival
- 15 Ghom AG, Mhaske S. Textbook of Oral Pathology. 2nd ed.. India: Jaypee Brothers, Medical Publishers Pvt. Limited; 2013: 1025
- 16 Augestad KM, Berntsen G, Lassen K, Bellika JG, Wootton R, Lindsetmo RO. Study Group of Research Quality in Medical Informatics and Decision Support (SQUID). Standards for reporting randomized controlled trials in medical informatics: a systematic review of CONSORT adherence in RCTs on clinical decision support. J Am Med Inform Assoc 2012; 19 (01) 13-21
- 17 Tierney JF, Stewart LA, Ghersi D, Burdett S, Sydes MR. Practical methods for incorporating summary time-to-event data into meta-analysis. Trials 2007; 8 (01) 16
- 18 Higgins JPT, Thompson SG, Deeks JJ, Altman DG. Measuring inconsistency in meta-analyses. BMJ 2003; 327 (7414): 557-560
- 19 Kawahira M, Yokota T, Hamauchi S. et al. Survival benefit of adding docetaxel, cisplatin, and 5-fluorouracil induction chemotherapy to concurrent chemoradiotherapy for locally advanced nasopharyngeal carcinoma with nodal Stage N2-3. Jpn J Clin Oncol 2017; 47 (08) 705-712
- 20 Zhu J, Duan B, Shi H. et al. Comparison of GP and TPF induction chemotherapy for locally advanced nasopharyngeal carcinoma. Oral Oncol 2019; 97: 37-43
- 21 Ou D, Blanchard P, El Khoury C. et al. Induction chemotherapy with docetaxel, cisplatin and fluorouracil followed by concurrent chemoradiotherapy or chemoradiotherapy alone in locally advanced non-endemic nasopharyngeal carcinoma. Oral Oncol 2016; 62: 114-121
- 22 Frikha M, Auperin A, Tao Y. et al; GORTEC. A randomized trial of induction docetaxel-cisplatin-5FU followed by concomitant cisplatin-RT versus concomitant cisplatin-RT in nasopharyngeal carcinoma (GORTEC 2006-02). Ann Oncol 2018; 29 (03) 731-736
- 23 Mohamad I, Abu-Hijleh F, Mayta E. et al. Comparison of two standard treatment approached in locoregionanly advanced nasopharyngeal carcinoma. South Asian J Cancer 2022; 11 (03) 223-228
- 24 Lee AWM, Tung SY, Ngan RKC. et al. Factors contributing to the efficacy of concurrent-adjuvant chemotherapy for locoregionally advanced nasopharyngeal carcinoma: combined analyses of NPC-9901 and NPC-9902 Trials. Eur J Cancer 2011; 47 (05) 656-666
- 25 Loong HH, Ma BBY, Leung SF. et al. Prognostic significance of the total dose of cisplatin administered during concurrent chemoradiotherapy in patients with locoregionally advanced nasopharyngeal carcinoma. Radiother Oncol 2012; 104 (03) 300-304
