Background
Ischemia-reperfusion (I/R) causes oxidative injury and ischemic fiber degeneration
(IFD), due to injury of the neuron and axon, after enough ischemic times, i.e.4–5
hours of peripheral nerve ischemia [[1],[2]]. Maximal intercellular adhesion molecule-1 (ICAM-1) expression on endoneural vessels
and polymorphonuclear monocytes reaches a peak at 24 th hour and macrophages increases
nearly four fold at 48–72 hour of reperfusion after a 5 h of near-complete ischemia
[[3]]. All these cells are responsible for demyelinisation and IFD at prolonged reperfusion
after enough ischemic times in peripheral nerves [[4],[5]]. Nerve lipid hydroperoxides reaches greatest levels at 3 hour and a gradual decline
follows over the next month with reperfusion [[6]]. An aggrevated reperfusion injury in Streptozocine induced diabetic rats could
be seen with less severe ischemic times [[7]]. Clinical experience related to I/R injury of peripheral nerve shows that neurologic
recovery is possible, if reperfusion starts within 6 hours after ischemia [[8]].
Allow for protection of briefly ischemic tissues against the harmful effects of subsequent
prolonged ischemia is a phenomennon called as Ischemic Preconditioning (IP)[[9]]. There are two distinct types of protection afforded by this adaptational reponse,
i.e. acute and delayed preconditioning. The factors that initiate the acute and delayed
preconditioning responses appear to be similiar. However, the protective effects of
acute preconditioning are protein synthesis independent, while the effects of delayed
preconditioning require protein synthesis. Adaptational responses to I/R injury have
been demonstrated in different tissue types [[10],[11],[12],[13],[14]]. IP has not been studied in I/R model of peripheral nerve before. We aimed to study
the effects of acute IP on I/R injury of peripheral nerve in rats.
Materials and methods
Animals
All animals were obtained from Experimental Research Laboratory of Sutcuimam University
School of Medicine. The experimental design was approved by the Ethical commite of
KSU. 200–250 g adult male spraque-dawley rats were used in the study. The animals
were fed with standart rats diets until the surgical procedures.
We examined I/R induced pathological and biochemical changes along the lenght of scaitic
nerve. Major arteries which supply rat hindlimb were occluded for 4 hours. Reperfusion
was accomplished by the release of ties of abdominal aorta and its branches. Nerve
pathology and biochemical analysis in sciatic nerve samples of the rats were assesed
after 3 hours and 7 days of reperfusion. A total of 70 rats were used in the study.
The study was divided into two part. Part 1 included the biochemical examination of
Ischemia, I/R and I/R+IP on sciatic nerves of rats at the early period. Part 2 which
consisted of 3 groups aimed to evaluate the histopathological changes in the nerves
7 days after the experimentation. The rats were randomly divided into following groups,
7 rats in each;
Part 1:Short time effects of I/R and IP
Group I- Normal adult male rats (Non-isch): Non-ischemic group, no intervention was made,
simply sciatic nerve samples were taken.
Group II- Ischemic group (Ischemic control-0hR): 4 hours of limb ischemia were done and the
samples were taken from the sciatic nerves after ischemic insult.
Group III- Ischemia-reperfusion group (3hR): 4 hours of ischemia and following 3 hours of reperfusion
were done. After I/R of sciatic nerves samples were taken.
Group IV- I/R plus ischemic preconditioning group (3hR+IP): Preconditioning (three cycles
of 5 minutes of short ischemia with 2 minute’s intervals), and then 4 hours of ischemia
with 3 hours of reperfusion.
Part 2: Long time effetcs of I/R and IP
Group 1- I/R with long duration (7dR):4 hours of ischemia and 7 days of reperfusion.
Group 2- Preconditioning plus I/R with long duration (7dR+IP): The same preconditioning protocol
with the group IV, and then, 4 hours of ischemia with following 7 days of reperfusion.
In both groups, sciatic nerve samples taken from both limb at 7th day were examined
histopathologically.
Group 3- Sham operated group: Abdominal aorta and its collaterals were simply exposed under
anesthesia, but no intervention was done. Then abdominal incision was primarly closed.
At 7th day, sciatic nerve samples were taken as done in the other groups.
Model of severe nerve ischemia
Our model of severe nerve ischemia was produced by tying of the iliolumbar and inferior
mesenteric arteries followed by the temporary occlusion of the abdominal aorta and
both iliac arteries [[15]]. We tied off all identifiable anastomotic vessels, including the iliolumbar and
inferior mesenteric arteries. The aorta and iliac arteries were tied with a silk suture
(6-0), using a slip-knot technique for rapid release, when needed. Measurements of
the femoral blood pressure (BP) were used to monitor the completeness of the occlusion,
and direct inspection of the sciatic nerve epineurial vessels showed that blood flow
had been arrested. Sluggish flow was sometimes seen in these vessels several minutes
after aortic occlusion, presumably due to partial reestablishment of anastomotic flow.
Ischemia-reperfusion and ischemic preconditioning model
The rat was anesthetized with intraperitoneal pentobarbital (60 mg/kg) followed by
surgery to produce IR. Ischemia was produced by ligating the abdominal aorta, the
right iliac artery, the right femoral artery, and all identifiable collateral vessels
supplying the sciatic nerves with 6-0 silk sutures. After 3 h of ischemia at 35°C,
the ties were released using a slipknot technique for ready release and rapid reperfusion
[[16]]. This procedure was done in IP groups for 3 times before the prolonged ischemia.
Sciatic nerves were harvested at 3 hours and 1 week after ischemia surgery for the
MDA measurements and histopathological studies, respectively.
Neuropathology: edema and axonal vacoulisation
A sciatic nerve segment at 2 cm long was harvested from each animal. The sciatic nerves
were osmicated, dehydrated, infiltrated, and embedded in Spurr’s resin. Longitidunal
sections of 1.0 cm were stained with hematoxylen eozine. Under 40× magnification,
these sections were graded for edema and axonal vacoulisation using previously described
methods [[17]]. The axon may be swollen or shrunken, watery and light, or dark and shrunken. Secondary
myelin changes were typically seen, including attenuation, collapse, or break-down.
For each section, the vacoulisation and edema were semi-quantitatively graded from
0 to 3 as follows: 0-normal, 1-mild, 2-moderate and 3-severe. No distinction was made
as to endoneurial, perivascular, or subperineurial edema. A mean value for each rat
was calculated after examination of four sections represented that case.
Statistics
The values were expressed as mean ± standart of deviation. The differences between
the groups were analysed by using ANOVA. Non-parametric data was evaluated by Mann
Whithney-U test. A p value less than 0.05 was considered as significant.
Results
MDA levels in sciatic nerve
During the occlusion of aorta and iliac arteries, the measurements of femoral blood
pressure aproximated to zero values in rats of all the groups.
The MDA levels of nerve tissue segments in different groups and nerve vacuolisation
degrees is shown in the [table 1]. Ischemic preconditioning group had significantly lower nerve MDA levels than reperfusion
group (p < 0.001). The differences between ischemic, IP and non-ischemic control groups
were not significant (p > 0.05), ([figure 1]).
Table 1
Non-parametric evaluation scores in part 2 experimentation.
|
Parameter
|
I/R
|
IP
|
Sham
|
|
Edema
|
3
|
2*
|
0**
|
|
Vacoulisation
|
2
|
1
|
0
|
The scale for the evaluated parameters as follows: normal-0, mild-1, moderate-2, severe-3
for endoneurial edema;no vacoulisation-0, mild vacoulisation-1, massive vacoulisation-2
for axonal vacuolisation.(* p < 0.05 for I/R versus IP, **p < 0.00001 for I/R versus
IP).
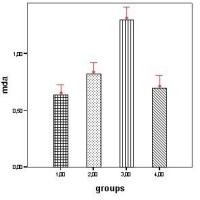 Figure 1
Figure 1
Sciatic nerve MDA (nmol/mg protein) levels in groups. (1.00:non-ischemic controls,
2.00:ischemic preconditioning, 3.00:ischemia-3 h reperfusion, 4.00:ischemia only).
Bars show means. Error bars show 95.0% CI of means.
Histopathologic changes
Great cytoplasmic vacoulisation caused by proliferation and dilation of the rough
and smooth endoplasmic reticulum and golgi apparatus was observed in I/R and IP groups
of part 2 experimentation. The intramyelinic edema within nerve fibers was seen not
only in perivascular region, but also, in endoneurial vessels ([Figures 2], [3] and [4]). IP group had a significantly good histopathologic score than I/R group (p < 0.05).
[Table 1] shows the scores in the groups.
 Figure 2
Figure 2
Normal architechture of sciatic nerve of rat is seen (sham group), Hematoxylen esozine
40× magnification.
 Figure 3
Figure 3
Increased axonal vacuolisation degeneration is seen at longitidunal section of sciatic
nerve (I/R group, score 3), Hematoxylen esozine 40× magnification.
 Figure 4
Figure 4
Mild vacuolisation in axons of sciatic nerve (ischemic preconditioning group, score
2), Hematoxylen esozine 40× magnification.
Discussion
Nerve pathology in acute ischemic injury has beeen delineated in peripheral nerve
and reperfusion injury could amplify ischemic pathology. Nerve ischemia plays a major
role in the development of pathological alteration in varous neuropathies and the
effects of ischemia are amplified by reperfusion in various tissues. In nerve tissue,
two types of edema is described after I/R; endoneural edema and intramyelinic edema
[[17]]. Endoneural edema reflects in blood-nerve barrier and possibly reflects endoneural
events especially severity of IFD. Myelin appears to be particularly susceptible to
activated free radicals, activated neutrophils and cytokine formation. Severe ischemia
to nerve results in energy rundown followed by conduction failure and fiber degeneration.
Inflammatory responses to IR have not only been confined to a few days (up to 7–14
days) of reperfusion, but also much more extended time (up to 42 days) of reperfusion
[[18]]. Between 7 days and 14 days of reperfusion, the IFD was reported to be the most
prominent. Morphological changes of IFD at the light microscopic level occur in concert
with endoneurial edema at the 7 and 14 day reperfusion time-points. I/R injury of
sciatic nerve has been shown to increase proinlammatory cytokines which are primarly
responsible demyelinization after reperfusion in peripheral nerves [[19]]. Another important indicator of I/R injury of peripheral nerve is Nitric Oxide
products which were found as increased at the first 24 hours of reperfusion in nerve
tissue and their elevation has been reported to play an essential role in reducing
the severity of the I/R injury by inhibiting neutrophil adhesion in postcapillary
venules and by decreasing microvascular constriction [[20]]. In our study, axonal changes at 7 th day were evaluated. It has been seen that
IP treated group showed less cytoplasmic vacuolisation and edema formation than I/R
group (p < 0.05). This finding was concominant to the finding of decreased oxidative
injury (i.e. decreased MDA levels in nerve tissue) seen in IP pretreated group.
Previously protective effects of IP in intestine, liver, myocard, skeletal muscle
and pancreas tissues has been shown [[10],[11],[12],[13],[14],[21],[22]]. What play role in the protective effect of IP is not exactly known, but some putative
mechanims, which are mostly dealed with countering the proinflammatory and proapoptotic
effects generated during IR have been put forward [[23]]. IP has been shown to decrease the formation of hydroxyl radicals during reperfusion
[[24]]. A reduced TNF-alpha and ICAM-1 mRNA expression seen after IP may account for the
inhibitory effects of IP on leukocyte adhesion and ameloriated microcirculatory disturbance
after IR in vivo [[23],[24],[25],[26]].
The protective effects of IP against lesions caused by subsequent severe ischemia
was primarly described in the heart by Murry et al [[9]]. Increased antioxidant enzyme activities which may be an indirect indicator of
the reduced injury after I/R has been shown in brain ischemic tolerance by IP [[27]]. However to best of our knowledge, nobody has studied this phenomennon in peripheral
somatic nerve. The benefical effect of IP in rat sciatic nerve was manifested by a
reduction in MDA tissue levels at 3th hour of reperfusion and ischemic fiber degeneration
(IFD) at 7 th postischemic day of reperfusion, in the present study. Lida et al. identified
pathologically three phases as follows: phase 1-early reperfusion minimal edema; phase-2
7 th and 14 th day of reperfusion prominent fiber degeneration and endoneurial edema;
phase-3 28 th and 42 th days abundant small regenerating fiber clusters, minimal edema
[[18]]. Our observation period is limited to up 7th day, i.e. phase-1. To best of our
knowledge, this is the first semiquantitative study that shows an decreased IFD after
IR due to the pretreatment with IP. Further studies are needed for understanding that
IP may have strategic role in treatment of I/R related peripheral nerve injuries.






