Key-words:
Antibiotic-mediated bacterial filamentation - filamentous rods - Pseudomonas aeruginosa
Introduction
The morphologic recognition of organisms remains an important component of the diagnostic
work up of a specimen in general pathology practice. An accurate interpretation requires
familiarity with an organism's typical morphology as well as morphologic variations,
including artificial changes. This case report illustrates the morphologic transformation
of antibiotic altered Pseudomonas aeruginosa in the cerebrospinal fluid of a young
boy.
Clinical History
Our patient is a 17-year-old boy with a history of hydrocephalus and placement of
a ventriculoperitoneal shunt who presented with fever. Recent medical history included
bacteremia, with blood cultures positive for Propionibacterium acnes. On hospital
day 1, the patient was started on empiric broad-spectrum antibiotics: vancomycin (20
mg/kg every 6 h); cefepime (intravenous, 50 mg/kg every 8 h); Flagyl (intravenous,
10 mg/kg every 8 h); and amikacin (intravenous, 20 mg/kg daily). Cultures from cerebrospinal
fluid (CSF) grew pansensitive P. aeruginosa. Subsequent peritoneal fluid and distal
catheter cultures on day 2 postadmission grew P. aeruginosa, and subsequently, the
shunt was removed on day 3 postadmission (shunt hardware cultures also grew P. aeruginosa).
Vancomycin and amikacin were subsequently discontinued (3 days of therapy each). On
day 7 postadmission, a repeat CSF fluid analysis showed an elevated white blood cell
(WBC) count of 674, and gentamicin (intravenous, 2.5 mg/kg every 8 h) was added for
secondary Gram-negative coverage. Flagyl was discontinued on postadmission day 9 after
anaerobic cultures remained negative (9 days of therapy), and gentamicin was discontinued
on postadmission day 10 given recent negative routine CSF cultures (4 days of therapy).
Unfortunately, a culture from the patient's external ventricular drain on postadmission
day 11 was again positive for P. aeruginosa, and ciprofloxacin (intravenous, 10 mg/kg)
was added on postadmission day 12. Subsequent cultures were negative, and ciprofloxacin
was discontinued on postadmission day 17 (6 days of therapy). On postadmission day
31, cefepime was discontinued, a 21-day course after the last negative culture (32-day
therapy in total). Morphologic examination of the CSF cytospin slide from day 1 of
hospital admission showed mixed inflammatory cells along with several long septate
filamentous rods [[Figure 1]]. What are these filamentous rods?
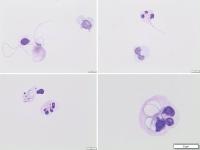 Figure 1: Giemsa-stained cytospin preparation from this childʼfs cerebrospinal fluid showing
long, intra- and extracellular, filamentous rods (a-d)
Figure 1: Giemsa-stained cytospin preparation from this childʼfs cerebrospinal fluid showing
long, intra- and extracellular, filamentous rods (a-d)
Comments
The filamentous rods seen are characteristic of antibiotic-altered P. aeruginosa.
For certain bacteria and antibiotic combinations, there may be inhibition of separation
but not division.[[1]] This results in an elongated septate appearance [which resembles and can be misconstrued
as slender septate fungal hyphae;[[1]],[[2]] [[Figure 1]] and [[Figure 2]]. Note: the difference in size and morphology was compared to pretreatment P. aeruginosa
[[Figure 2]]d. Our patient had another sampling of CSF 2 days after shunt externalization and
subsequent removal, and no bacteria (filamentous, viable, or nonviable) were seen
in the follow-up sample.
 Figure 2: Antibiotic-altered filamentous rods in the cerebrospinal fluid of a child with infected
shunt (a-c) compared in size and appearance to pretreated Pseudomonas aeruginosa (d).
All photos are taken at ʼ100 oil magnification of Giemsa-stained slides
Figure 2: Antibiotic-altered filamentous rods in the cerebrospinal fluid of a child with infected
shunt (a-c) compared in size and appearance to pretreated Pseudomonas aeruginosa (d).
All photos are taken at ʼ100 oil magnification of Giemsa-stained slides
This antibiotic-induced filamentation phenomenon was first reported by Gardner in
1940 and involved in vitro studies of Escherichia coli given subinhibitory concentrations
of penicillin.[[3]] It is now recognized that filamentation is a common and likely survival-related
response that is seen most often in Gram-negative bacilli and subinhibitory concentrations
of antibiotics, particularly those of the β-lactam family.[[1]],[[4]] The literature on the subject, however, is relatively scant, and further, illustrations
are few.[[1]],[[5]],[[6]] It should also be noted that bacteria of the order Actinomycetales (notable genera
include Nocardia, Corynebacterium, Actinomyces, and Rhodococcus) commonly show filamentous
branching formation in the absence of antibiotic administration.[[7]] It is important to keep this phenomenon of antibiotic-induced bacterial filamentation
in mind when analyzing the fluid of a patient that has been treated for bacterial
infection and hence avoid diagnostic pitfalls and potential unnecessary treatment.
Authors' contribution
All authors are involved in the clinical aspects of the reported material and drafting
and final revision of the manuscript.
Compliance with ethical principles
No prior ethical approval is required at our institution for isolated case reports.
Case history and samples are reported anonymously.
Reviewers:
Fauzi A Sagher (Tripoli, Libya)
Elhadi H Aburawi (Al Ain, UAE)
Editors:
Salem A Beshyah (Abu Dhabi, UAE)
Elmahdi A Elkhammas (Columbus OH, USA)





