
Subscribe to RSS
DOI: 10.1055/s-0043-1771517
Early Predictor of Acute Kidney Injury in Newborns with Perinatal Asphyxia
Abstract
Acute kidney injury (AKI) is an independent risk factor for neonatal death. Since neonatal early renal injury usually has no specific clinical symptoms, many AKI cases are often missed the best time of early intervention if there is no relevant examination. Perinatal asphyxia (PA) can lead to AKI. The study aimed to assess efficacy of serum cystatin C (CystC) in early prediction of AKI in full-term neonates with PA. The study was conducted at the neonatal intensive care unit, Assiut University Children Hospital from January 2019 to January 2021. Seventy full-term neonates with documented PA were enrolled in the study. Baseline laboratory data and serum CystC levels were assessed. Out of those 70 neonates with PA, 21 (30%) developed AKI, while 49 (70%) neonates did not develop AKI. Majority of non-AKI group had stage-I hypoxic-ischemic encephalopathy (HIE) (61.2%), while majority of AKI had stage-III HIE (61.9%). A significantly higher serum CystC level was found among AKI group than those without AKI (1.50 ± 0.12 vs. 0.90 ± 0.14, p < 0.001). The predictors for AKI among neonates with PA were low birth weight, serum CystC levels, hypotension, and stage-III HIE. Serum CystC has 94.3% overall accuracy for prediction of AKI. In conclusion, AKI in neonates with PA is common. CystC is a promising biomarker in early prediction of AKI in such cases. Future studies are warranted to confirm these findings.
#
Introduction
The kidneys of neonates are particularly susceptible to hypoperfusion because of the physiologic characteristics of neonatal kidneys, including high renal vascular resistance, high plasma renin activity, low glomerular filtration rate (GFR), decreased intracortical perfusion rate, and decreased reabsorption of sodium in proximal convoluted tubules in the first day of neonatal life.[1] Acute kidney injury (AKI) is defined as kidneys' inability to excrete nitrogenous waste products and maintain fluid and electrolyte homeostasis. It is fairly common in newborn population and is a major contributing factor of neonatal mortality and morbidity.[2] [3]
Perinatal asphyxia (PA) is a serious event that can have significant consequences during the neonatal period. It is a common issue in neonatal care and a major cause of morbidity and mortality among term and preterm neonates.[4] The incidence of PA is estimated to be between 5 and 10 per 1,000 live births and is influenced by factors such as birth weight, gestational age, and access to medical resources in the local area.[5] PA can result in multiorgan dysfunction through redirection of cardiac output to maintain cerebral, cardiac, and adrenal perfusion while potentially compromising perfusion to nonvital organs including skin perfusion, gastrointestinal tract, and kidneys, causing AKI.[6] [7] [8] The incidence of AKI after PA in term neonates ranged from 30 to 56%. During PA, the neonate's body tries to compensate for the lack of oxygen by redirecting blood flow to vital organs, such as brain and heart, at the expense of other organs, such as kidneys. This can lead to reduced blood flow to the kidneys, which can damage the kidney tissue and lead to AKI.[9]
Human cystatin C (CystC) is a small protein produced by all nucleated cells and filtered through the glomerular basement membrane in the kidneys. It is a reliable marker of GFR as it is freely filtered and almost completely reabsorbed in the proximal tubules, without being secreted or metabolized in the kidneys. Due to its characteristics, CystC is considered a more accurate marker of renal function than creatinine, especially in neonates with impaired renal function.[10] Early detection of AKI is crucial for timely interventions to prevent further kidney damage and improve patient outcomes. Currently, serum creatinine is the most commonly used marker for diagnosing AKI, but it has limitations, particularly in neonates. Creatinine production is influenced by muscle mass, which is variable in neonates, and it does not increase until after a significant reduction in GFR has occurred.[11] [12] Several studies have shown that CystC is a useful biomarker for the early detection of AKI in neonates. In a study conducted in a neonatal intensive care unit (NICU), CystC was found to be a better predictor of AKI than creatinine.[13] [14] [15] Another study found that CystC was significantly elevated in neonates with AKI compared with those without AKI, and that CystC levels were detectable before serum creatinine levels increased.[16]
The current study aimed to investigate the role of serum CystC as an early predictor for both diagnosis and short-term outcome evaluation of AKI in full-term neonates with PA admitted to NICU.
#
Patients and Methods
Study Setting and Design
A prospective cohort study was performed at the NICU of Assiut University Children Hospital, Assiut, Egypt from January 2019 to January 2021. Approval of the local ethics committee broad was obtained (approval # 17200233, 06/08/2018), and the study was conducted according to Declaration of Helsinki. The inclusion criteria were full-term neonates (37–42 weeks of gestation), admitted with PA, which was confirmed by the presence of at least two of the following criteria: fetal distress (heart rate <100 beats/minute, late decelerations, or an absence of heart rate variability), thick meconium-stained amniotic fluid and respiratory depression, hypotonia, or bradycardia, low Apgar score (less than 5 at 1 minute or 7 or less at 5 minutes), need for advanced resuscitation (with positive pressure ventilation and oxygen immediately after birth) for more than 1 minute, and blood pH value of less than 7.20 or a base deficit of at least 12 mmol/L within the first hour after birth.[17] The study excluded neonates who met any of the following criteria: gestational age <37 or > 42 weeks, AKI due to causes other than asphyxia, (e.g., septicemia, respiratory distress syndrome, necrotizing enterocolitis, and major congenital anomalies of skeletal, kidney, and urinary tract) or newborns who were born to mothers with renal insufficiency, or who were given nephrotoxic drugs such as aminoglycosides. AKI was defined as an increase in serum creatinine of 0.3 mg/dL or more (≥26.5 µmol/L) or 50% or more from the previous lowest value, or a urinary output of < 1 mL/kg/h on postnatal days 2 to 7, according to the Kidney Disease: Improving Global Outcomes workgroup modified AKI definition for neonates.[18] [19] All neonates showing signs of hypoxic-ischemic encephalopathy (HIE) were classified according to the Sarnat and Sarnat scoring system[20] into three stages, according to the conscious level, neurological, and autonomic parameters.
#
Sample Size Calculation
Total coverage sample technique was applied where all full-term neonates who were admitted to NICU with documented PA during the study period were eligible for the study. A total of 70 full-term neonates (37–42 weeks of gestation) with PA were enrolled in the study.
#
Methods
Before enrolling their neonates in the study, the parents were asked to provide written consent after being informed of the study's details. On admission, all neonates were subjected to the following: full history evaluation including maternal condition during pregnancy (hypertension, premature rupture of membrane, or diabetes mellitus). Natal history included mode and duration of delivery and antepartum or postpartum hemorrhage. Postnatal history including first cry, cyanosis, Apgar score at 1, 5, and 10 minutes, need for resuscitation, medications, anesthesia, respiratory distress, and convulsions. On admission, thorough clinical evaluation was done in form of vital signs (heart rate, respiratory rate, and temperature), general examination, systemic examination, and anthropometric measurements (daily follow-up of body weight and weekly follow-up of head circumference). On admission, blood glucose, arterial blood gases, and blood grouping were done. Other routine laboratory investigations as complete blood count, coagulation profile, serum electrolytes (sodium, potassium, and calcium), urine analysis, urinary sodium and potassium, and liver function tests were done on the second day of life except in case of antepartum hemorrhage, complete blood count was done on admission. Follow-up of these routine investigations was individualized according to each case progression. Daily follow-up of serum creatinine was done for all neonates with PA in the first 3 days of life and continued for the seventh day for those in neonates with rising level. Radiological evaluation was done on the day of admission by abdominal ultrasound to exclude the possibility of any congenital structural anomalies in kidneys or urinary tract.
Serum CystC was estimated during the first day of life by utilized Human Cystatin C (Cys-C) ELISA kit (SinoGeneClon BiotechCo., Ltd, Hangzhou, China).
#
Statistical Analysis
Analyzes was made by IBM SPSS Statistics for Windows, version 23 (IBM SPSS, IBM Corp., Armonk, New York, United States). Shapiro–Wilk's test was used to evaluate normal data distribution. The variables were expressed as mean ± standard deviation for parametric parameters and as frequency (%) for categorized parameters. Unpaired Student “t” test was performed to compare difference between parametric between two groups, while Pearson's chi-square analysis was used to compare categorized variables. Predictors of AKI in the current study were determined by logistic regression analysis. Cutoff point of serum CystC and area under the curve (AUC) for prediction AKI in full-term neonates with PA was determined by receiver operating characteristics (ROC) curve. Level of confidence was kept at 95%, and hence, p-value was significant if p < 0.05.
#
#
Results
Risk Factors for Development of AKI and PA
Out of 70 neonates with PA included in the study, 21 (30%) neonates developed AKI, while the other 49 (70%) neonates did not develop AKI. There were insignificant differences between neonates with and without AKI except for significantly lower birth weight among AKI group (2.83 ± 0.65 vs. 3.19 ± 0.56 kg, p < 0.001). The number of neonates with low birth weight (LBW) were significantly higher in those with AKI versus those without AKI (57.1 vs. 28.6%, p = 0.020). Frequency of antepartum hemorrhage was significantly higher among AKI group versus those without AKI (28.6 vs. 6.1%; p = 0.010). Other risk factors as obstructed labor, meconium aspiration syndrome, cord prolapses, and rupture uterus showed insignificant differences between both groups ([Table 1]).
Abbreviation: AKI, acute kidney injury.
Statistical significant p-Values are shown in bold.
#
Clinical Data and Management of Neonates with and without AKI
There was significant increase among neonates with AKI versus those without AKI in hypotension (38.1 vs. 12.2%, p = 0.010), frequency of mechanical ventilation (MV) (61.9 vs. 18.4%, p < 0.001), use of vasopressor (28.6 vs. 6.1%; p = 0.040), duration of MV (5.22 ± 1.55 vs. 2.56 ± 1.23 days, p = 0.040), and usage of vasopressor (3.40 ± 1.98 vs. 1.50 ± 0.50 days, p = 0.030). Normal urine output in neonates with AKI was significantly lower than those without AKI (61.9 vs. 100.0%, p < 0.001). It was found that majority (61.2%) of neonates without AKI group had stage-I HIE, while majority (61.9%) of those with AKI had stage-III with significant differences between both groups (p < 0.001). Length of hospital stay was significantly longer among those with versus those without AKI (8.28 ± 2.14 vs. 5.41 ± 1.32 days, p < 0.001). Majority of neonates without AKI were discharged (95.9%) and only two neonates (4.1%) were died. Meanwhile, in patients with AKI, only 11 cases (52.4%) were discharged and 10 (47.6%) neonates were deteriorated and died with significant differences between both groups (p < 0.001) ([Table 2]).
Abbreviation: AKI, acute kidney injury.
Statistical significant p-Values are shown in bold.
#
Laboratory Investigations in Neonates with and without AKI
In neonates with AKI versus neonates without AKI, there were significant increase in 48-hour creatinine (103.22 ± 10.11 vs. 99.48 ± 5.35; p < 0.001), 72-hour creatinine (295.19 ± 44.56 vs. 91.33 ± 6.65; p < 0.001), and serum CystC (1.50 ± 0.12 vs. 0.90 ± 0.14; p < 0.001) ([Table 3]).
Abbreviations: AKI, acute kidney injury; CystC, cystatin C; eGFR, estimated glomerular filtration rate; INR, international randomized ratio.
Statistical significant p-Values are shown in bold.
#
Predictors for Acute Kidney Injury among the Studied Neonates
Based on the current study, the predictors for AKI among neonates with PA were LBW (odds ratio [OR] = 1.45, 95% confidence interval [CI]: 1.22–3.98, p = 0.010), hypotension (OR = 2.22, 95% CI: 1.87–4.67, p = 0.010), stage-III HIE (OR = 2.87, 95% CI: 2.01–5.89, p < 0.001), serum CystC (OR = 3.11, 95% CI: 2.22–6.01, p < 0.001) ([Table 4]).
Abbreviations: CI, confidence interval; CystC, cystatin C; HIE, hypoxic-ischemic encephalopathy; OR, odds ratio.
Note: The p-value was significant if < 0.05.
Statistical significant p-Values are shown in bold.
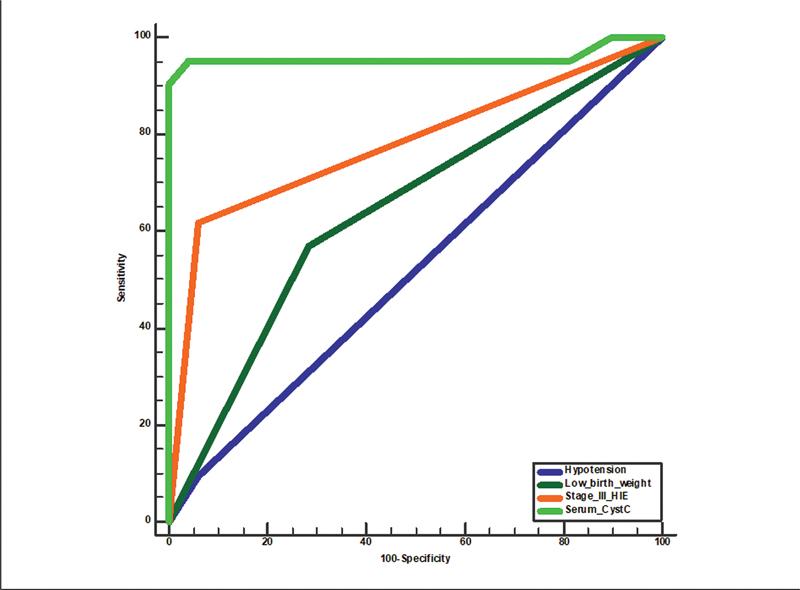
With ROC curve, it was found that serum CystC has the best diagnostic accuracy (94.3%, AUC = 0.939, p < 0.001) for prediction of AKI ([Fig. 1]) followed by stage-III HIE (84.4%, AUC = 0.779, p < 0.001), hypotension (68.6%, AUC = 0.643, p = 0.043), and least was LBW (66.8%, AUC = 0.517, p = 0.824) ([Table 5]).
Abbreviations: AUC, area under the curve; CystC, cystatin C; HIE, hypoxic-ischemic encephalopathy; LBW, low birth weight.
#
#
Discussion
PA is a condition where there is a lack of oxygen (hypoxia) and/or blood flow (ischemia) that is severe and prolonged enough to cause functional and/or biochemical changes in different organs of the body. Since the kidneys are particularly vulnerable to oxygen deprivation, they may experience renal insufficiency within 24 hours of a hypoxic-ischemic episode. If the oxygen deprivation continues, it may even cause irreversible cortical necrosis. Renal injury in PA can occur due to the body's adaptive mechanisms. AKI, acute tubular necrosis, and renal vein thrombosis are all recognized complications of this condition. Among these, AKI is the most common and has a poor prognosis. It may even cause permanent renal damage in up to 40% of the survivors.[21] Traditionally, AKI described as the increase of serum creatinine above 1.5 mg/dL (132 µmol/L). AKI is often observed in neonates, and ∼8 to 24% were observed among those in NICU.[22]
The current study enrolled 70 full-term neonates admitted to NICU with documented PA. This study aimed to assess efficacy of CystC in early prediction of AKI in neonates with PA. Out of 70 neonates included in this study, 21 (30%) neonates developed AKI, while the other 49 (70%) neonates did not develop AKI. The exact prevalence of AKI among neonates with PA is unknown and incidence varies from 6 to 24% in NICUs worldwide.[7] [23] [24] In agreement with results of this study, AKI incidence was 30% in a worldwide study that included data from different four countries (Australia, Canada, India, United States).[25] A low frequency of AKI (13.3%) among neonates with PA was reported by Memon et al at NICU at tertiary care hospital.[26] Alaro et al's study from Kenya revealed 11.7% AKI in cases of birth asphyxia.[27] This variation in the frequency of AKI among neonates with PA may be attributed to different study designs, method and timing of diagnosis of AKI, different sample size.
In the current investigation, PA was found in males more often than females (60.0 vs. 40.0%). Many earlier researches reported predominance of PA in males than females. In a study performed in Hyderabad by Memon et al,[26] 56.7% of PA neonates were males, and 43.3% were females. In a study carried in Kenya, Alaro et al[27] reported that 60% of PA participants were males. In a study done in Sudan by Medani et al,[28] 59% PA neonates were males. Chishty et al[29] reported that 2.6 times as many males as females neonates had PA. Malik et al[30] and Afzal et al[31] reported that 78 and 60% of the PA participants were males.
In the current study, neonates with and without AKI had insignificant difference as regard baseline data apart from significantly lower birth weight among AKI group. Also, AKI group had significantly high frequency of LBW neonates whose birth weight < 2,500 g compared with neonates without AKI (57.1 vs. 28.6%). Previous study noticed that most newborns in AKI group had a birth weight < 2,500 g.[32] Meanwhile, other studies found insignificant difference in neonatal birth weight in neonates with and without AKI.[15] [22]
Also, results of this study revealed significant increase in frequency of antepartum hemorrhage among AKI group versus neonates without AKI (28.6 vs. 6.1%). While other PA risk factors as cord prolapse and meconium aspiration syndrome were comparable in both groups. In agreement with this study, previous study reported significant higher frequency of antepartum hemorrhage among AKI group versus neonates without AKI (1.86 vs. 0.00%).[33]
Another finding in the current study was that frequency of hypotension, MV, and usage of vasopressor were significantly higher among those with AKI compared with those without AKI with significantly longer duration of MV and usage of vasopressor.
In agreement with this study, Viswanathan et al studied 472 extreme LBW neonates and reported that 59 (12.5%) of them developed AKI. The authors also found that neonates with AKI had significantly lower mean systolic blood pressure than those without AKI (25.9 ± 9.9 vs. 35.5 ± 13.7 mm Hg, p < 0.001).[34]
On the contrary, El-Gammacy et al stated that frequency of MV was insignificantly higher among AKI group (61.5 vs. 45.9%; p = 0.33) and yet, they agreed with results of this study as regard vasopressor support that was higher among neonates with AKI (30.8 vs. 8.1%; p = 0.04).[15] Cataldi et al conducted a study and found that there was a significant risk of AKI among infants with a VLBW, with 79% of cases occurring in infants weighing < 1,500 g.[35]
In this study, AKI neonates mostly (61.9%) had nonoliguric AKI. Only 8 (38.1%) neonates had oliguric AKI. This agreed with the study of El-Gammacy et al who reported that 30.8% of AKI group had oliguric AKI.[36]
The results of this study revealed that majority (61.2%) of non-AKI group had stage-I HIE, while majority (61.9%) of those with AKI had stage-III with significant differences between both groups. Also, Gohiya et al stated stage of HIE was more advanced among neonates with AKI.[33]
The main finding in the current study was that there was significantly higher serum CystC among AKI group than those without AKI. In line with this study, a previous study reported similar findings with significant higher serum cystatin c among asphyxiated neonates with AKI (2.35 ± 2.77 vs. 0.96 ± 0.37 (mg/L); p = 0.03).[22]
This study revealed that majority (95.9%) of non-AKI group was discharged and only two patients (4.1%) died. Meanwhile, 10 (47.6%) patients with AKI were deteriorated and died. Also, length of hospital stay was significantly longer among those with AKI versus those without AKI (8.28 ± 2.14 vs. 5.41 ± 1.32 days). Many previous studies agreed with these findings and reported that neonates with AKI had significant longer hospital stay with significant poor prognosis.[36] [37]
Another study stated that although both groups of neonates had insignificant differences as regard hospital stay but hospital mortality was significantly higher among AKI group versus those without AKI (16.8 vs. 0.99%).[33]
Based on the current study, the predictors for AKI among neonates with PA were LBW (OR = 1.45, 95% CI = 1.22–3.98, p < 0.010), hypotension (OR = 2.22, 95% CI = 1.87–4.67, p < 0.010), stage-III HIE (OR = 2.87, 95% CI = 2.01–5.8, p < 0.010), and high serum cystC (OR = 3.11, 95% CI = 2.22–6.01, p < 0.010). With ROC curve, it was found that serum CystC at cutoff point of 1.43 ng/mL has 94.3%, overall accuracy for prediction of AKI with AUC was 0.939, then stage-III HIE (AUC = 0.779, p < 0.001) and LBW (AUC = 0.643, p = 0.043). Hidayati et al studied serum CystC as a predictor of AKI; they found that at cutoff value for CystC 1.605 mg/L, sensitivity was 84.8%; specificity was 67.4%; and accuracy was 67.4%. The AUC for CystC was 84.9%.[32] Previous studies about normal CystC level in neonates are lacking. However, a study showed that CystC levels were 1.54 mg/L ( ± 0.28) at birth, 1.38 mg/L ( ± 0.36) within 48 to 72 hours of life, and 1.50 mg/L ( ± 0.31) after 7 days.[38] In agreement with these findings, previous study stated that ROC curve analysis showed AUC for CystC was 0.692 (sensitivity of 82.0%, specificity of 94%). These values may discriminate in case of reduced GFR after perinatal hypoxia/asphyxia in newborns, but the sample size was not sufficient to validate this cutoff.[39] This indicates that CystC could detect renal dysfunction 1 to 2 days before serum creatinine. This comes in agreement with Ahmed et al who reported that there was increase of CystC before the increase in serum creatinine. These findings suggest that CystC is a more sensitive marker in early detection of AKI preceding serum creatinine increase by a few days.[40]
Limitations of the current study included relatively small sample size, being conducted in single tertiary center, absent of control group to assess serum CystC in healthy neonates, and finally, lack of long-term follow-up to determine effect of CystC on survival analysis of those neonates with PA and AKI.
#
Conclusion
High frequency of AKI (30.0%) was noted in neonates with PA. LBW, stage-III HIE, and elevated serum CystC within first day of life were significantly associated with AKI. Serum CystC is a promising marker for early detection of AKI in full-term neonates with PA. Multiple future studies are required to confirm such results and serial analysis of levels of serum CystC in PA neonates is recommended.
#
#
Conflict of Interest
None declared.
Authors' Contribution
N.H.R., M.A.F. and Y.F.A. conceptualized the work, analyzed, and interpreted, drew and reviewed the first draft and ensured for the integrity and accuracy in the work. A.H.A.A.H. and E.A.H. conceptualized the work, software, validation, visualization, investigation, reviewed the first draft, and ensured for the integrity and accuracy in the work. M.A.S. contributed to data curation, writing—original draft preparation, and ensured for the integrity and accuracy in the work. All the authors approved the final manuscript as submitted and agree to be accountable for all aspects of the work. These authors contributed equally to this work.
-
References
- 1 Friedlich PS, Evans JR, Tulassay T, Seri I. . Acute and chronic renal failure. In: Avery's Diseases of the Newborn. WB Saunders; 2005:1298–1306
- 2 Liava'a MH, Krishnamurthy G, Chai PJ. Low birth weight and other high-risk conditions. Critical Heart Disease Infants Children 2019; x: 371-378
- 3 Coca SG, Singanamala S, Parikh CR. Chronic kidney disease after acute kidney injury: a systematic review and meta-analysis. Kidney Int 2012; 81 (05) 442-448
- 4 Levene M. . Perinatal asphyxia and Hypoxic-ischemic encephalopathy. Forfar and Arneil's Textbook of Pediatrics. 6th edition. Philadelphia: Churchill Livingstone, an Imprint of Elsevier Ltd.; 2003:197–204
- 5 Popescu MR, Panaitescu AM, Pavel B, Zagrean L, Peltecu G, Zagrean A-M. Getting an early start in understanding perinatal asphyxia impact on the cardiovascular system. Front Pediatr 2020; 8 (68) 68
- 6 Oncel MY, Canpolat FE, Arayici S, Alyamac Dizdar E, Uras N, Oguz SS. Urinary markers of acute kidney injury in newborns with perinatal asphyxia (.). Ren Fail 2016; 38 (06) 882-888
- 7 Durkan AM, Alexander RT. Acute kidney injury post neonatal asphyxia. J Pediatr 2011; 158 (2, Suppl): e29-e33
- 8 Nishijima T, Kawasaki Y, Ueno K, Inomata S, Yoshida T. Renal impairment following perinatal asphyxia. Pediatr Neonatol 2021; 62 (04) 451-452
- 9 Selewski DT, Charlton JR, Jetton JG. et al. Neonatal acute kidney injury. Pediatrics 2015; 136 (02) e463-e473
- 10 Herget-Rosenthal S, Marggraf G, Hüsing J. et al. Early detection of acute renal failure by serum cystatin C. Kidney Int 2004; 66 (03) 1115-1122
- 11 Askenazi DJ, Ambalavanan N, Goldstein SL. Acute kidney injury in critically ill newborns: what do we know? What do we need to learn?. Pediatr Nephrol 2009; 24 (02) 265-274
- 12 Nada A, Bonachea EM, Askenazi DJ. Acute Kidney Injury in the Fetus and Neonate. Elsevier; 2017. :22(02):90–97
- 13 Hidayati EL, Utami MD, Rohsiswatmo R, Tridjaja B. Cystatin C compared to serum creatinine as a marker of acute kidney injury in critically ill neonates. Pediatr Nephrol 2021; 36 (01) 181-186
- 14 Kandasamy Y, Smith R, Wright IM. Measuring cystatin C to determine renal function in neonates. Pediatr Crit Care Med 2013; 14 (03) 318-322
- 15 El-Gammacy TM, Shinkar DM, Mohamed NR, Al-Halag AR. Serum cystatin C as an early predictor of acute kidney injury in preterm neonates with respiratory distress syndrome. Scand J Clin Lab Invest 2018; 78 (05) 352-357
- 16 Krawczeski CD, Vandevoorde RG, Kathman T. et al. Serum cystatin C is an early predictive biomarker of acute kidney injury after pediatric cardiopulmonary bypass. Clin J Am Soc Nephrol 2010; 5 (09) 1552-1557
- 17 Boskabadi H, Omidian M, Tavallai S. et al. Serum Hsp70 antigen: early diagnosis marker in perinatal asphyxia. Iran J Pediatr 2015; 25 (02) e381
- 18 Coleman C, Tambay Perez A, Selewski DT, Steflik HJ. Neonatal acute kidney injury. Front Pediatr 2022; 10: 842544
- 19 Leem AY, Park MS, Park BH. et al. Value of serum cystatin C measurement in the diagnosis of sepsis-induced kidney injury and prediction of renal function recovery. Yonsei Med J 2017; 58 (03) 604-612
- 20 Sarnat HB, Sarnat MS. Neonatal encephalopathy following fetal distress. A clinical and electroencephalographic study. Arch Neurol 1976; 33 (10) 696-705
- 21 Gupta BD, Sharma P, Bagla J, Parakh M, Soni JP. Renal failure in asphyxiated neonates. Indian Pediatr 2005; 42 (09) 928-934
- 22 Mehrkesh M, Barekatain B, Gheisari A, Ahmadi M, Shahsanai A. Serum KIM-1 and cystatin levels as the predictors of acute kidney injury in asphyxiated neonates. Iranian Journal of Neonatology 2022; 13 (01) 6-12
- 23 Askenazi DJ, Ambalavanan N, Goldstein SL. Acute kidney injury in critically ill newborns: what do we know? What do we need to learn?. Pediatr Nephrol 2009; 24 (02) 265-274
- 24 Bozkurt O, Yucesoy E. Acute kidney injury in neonates with perinatal asphyxia receiving therapeutic hypothermia. Am J Perinatol 2021; 38 (09) 922-929
- 25 Jetton JG, Boohaker LJ, Sethi SK. et al; Neonatal Kidney Collaborative (NKC). Incidence and outcomes of neonatal acute kidney injury (AWAKEN): a multicentre, multinational, observational cohort study. Lancet Child Adolesc Health 2017; 1 (03) 184-194
- 26 Memon IA, Qudus HA, Waraich IS, Channa S, Marwat A, Lahrasab W. Acute kidney injury in neonates with birth asphyxia at a tertiary care hospital. Pak J Med Health Sci 2021; 15 (03) 573-575
- 27 Alaro D, Bashir A, Musoke R, Wanaiana L. Prevalence and outcomes of acute kidney injury in term neonates with perinatal asphyxia. Afr Health Sci 2014; 14 (03) 682-688
- 28 Medani SA, Kheir AE, Mohamed MB. Acute kidney injury in asphyxiated neonates admitted to a tertiary neonatal unit in Sudan. Sudan J Paediatr 2014; 14 (02) 29-34
- 29 Chishty AL, Iqbal MA, Anjum A, Maqbool S. Risk factor analysis of birth asphyxia at the children's hospital, Lahore. Pak Pediatr J 2002; 26: 47-53
- 30 Malik TS, Chishti AL, Ahmed TM. Short term neurodevelopmental outcome of asphyxiated newborns at tertiary care unit. Pak Pediatr J 2007; 31 (02) 58-61
- 31 Afzal MF, Anjum A, Sultan MA. Risk factor analysis in asphyxiated newborns and their outcome in relation to stage of hypoxic ischemic encephalopathy. Pak Pediatr J 2007; 31 (02) 63-68
- 32 Hidayati EL, Utami MD, Rohsiswatmo R, Tridjaja B. Cystatin C compared to serum creatinine as a marker of acute kidney injury in critically ill neonates. Pediatr Nephrol 2021; 36 (01) 181-186
- 33 Gohiya P, Nadkarni J, Mishra M. Study of neonatal acute kidney injury based on KDIGO criteria. Pediatr Neonatol 2022; 63 (01) 66-70
- 34 Viswanathan S, Manyam B, Azhibekov T, Mhanna MJ. Risk factors associated with acute kidney injury in extremely low birth weight (ELBW) infants. Pediatr Nephrol 2012; 27 (02) 303-311
- 35 Cataldi L, Leone R, Moretti U. et al. Potential risk factors for the development of acute renal failure in preterm newborn infants: a case-control study. Arch Dis Child Fetal Neonatal Ed 2005; 90 (06) F514-F519
- 36 El-Gamasy MA, Nassar MAE. Risk factors for acute kidney injury (AKI) in newly born infants with hypoxic ischemic encephalopathy (HIE). A single center experience. Int J Res Stud Med Health Sci 2017; 2: 1-8
- 37 Momtaz HE, Sabzehei MK, Rasuli B, Torabian S. The main etiologies of acute kidney injury in the newborns hospitalized in the neonatal intensive care unit. J Clin Neonatol 2014; 3 (02) 99-102
- 38 Bardallo Cruzado L, Pérez González E, Martínez Martos Z. et al. Serum cystatin C levels in preterm newborns in our setting: correlation with serum creatinine and preterm pathologies [in English]. Nefrologia 2015; 35 (03) 296-303
- 39 Treiber M, Gorenjak M, Pecovnik Balon B. Serum cystatin-C as a marker of acute kidney injury in the newborn after perinatal hypoxia/asphyxia. Ther Apher Dial 2014; 18 (01) 57-67
- 40 Ahmed AM, Koura HM, Youssef H. et al. Early detection of neonatal kidney disease in high risk neonates admitted to neonatal intensive care unit. World J Med Sci 2014; 11: 518-524
Address for correspondence
Publication History
Received: 07 April 2023
Accepted: 28 June 2023
Article published online:
02 August 2023
© 2023. The Author(s). This is an open access article published by Thieme under the terms of the Creative Commons Attribution License, permitting unrestricted use, distribution, and reproduction so long as the original work is properly cited. (https://creativecommons.org/licenses/by/4.0/)
Georg Thieme Verlag KG
Rüdigerstraße 14, 70469 Stuttgart, Germany
-
References
- 1 Friedlich PS, Evans JR, Tulassay T, Seri I. . Acute and chronic renal failure. In: Avery's Diseases of the Newborn. WB Saunders; 2005:1298–1306
- 2 Liava'a MH, Krishnamurthy G, Chai PJ. Low birth weight and other high-risk conditions. Critical Heart Disease Infants Children 2019; x: 371-378
- 3 Coca SG, Singanamala S, Parikh CR. Chronic kidney disease after acute kidney injury: a systematic review and meta-analysis. Kidney Int 2012; 81 (05) 442-448
- 4 Levene M. . Perinatal asphyxia and Hypoxic-ischemic encephalopathy. Forfar and Arneil's Textbook of Pediatrics. 6th edition. Philadelphia: Churchill Livingstone, an Imprint of Elsevier Ltd.; 2003:197–204
- 5 Popescu MR, Panaitescu AM, Pavel B, Zagrean L, Peltecu G, Zagrean A-M. Getting an early start in understanding perinatal asphyxia impact on the cardiovascular system. Front Pediatr 2020; 8 (68) 68
- 6 Oncel MY, Canpolat FE, Arayici S, Alyamac Dizdar E, Uras N, Oguz SS. Urinary markers of acute kidney injury in newborns with perinatal asphyxia (.). Ren Fail 2016; 38 (06) 882-888
- 7 Durkan AM, Alexander RT. Acute kidney injury post neonatal asphyxia. J Pediatr 2011; 158 (2, Suppl): e29-e33
- 8 Nishijima T, Kawasaki Y, Ueno K, Inomata S, Yoshida T. Renal impairment following perinatal asphyxia. Pediatr Neonatol 2021; 62 (04) 451-452
- 9 Selewski DT, Charlton JR, Jetton JG. et al. Neonatal acute kidney injury. Pediatrics 2015; 136 (02) e463-e473
- 10 Herget-Rosenthal S, Marggraf G, Hüsing J. et al. Early detection of acute renal failure by serum cystatin C. Kidney Int 2004; 66 (03) 1115-1122
- 11 Askenazi DJ, Ambalavanan N, Goldstein SL. Acute kidney injury in critically ill newborns: what do we know? What do we need to learn?. Pediatr Nephrol 2009; 24 (02) 265-274
- 12 Nada A, Bonachea EM, Askenazi DJ. Acute Kidney Injury in the Fetus and Neonate. Elsevier; 2017. :22(02):90–97
- 13 Hidayati EL, Utami MD, Rohsiswatmo R, Tridjaja B. Cystatin C compared to serum creatinine as a marker of acute kidney injury in critically ill neonates. Pediatr Nephrol 2021; 36 (01) 181-186
- 14 Kandasamy Y, Smith R, Wright IM. Measuring cystatin C to determine renal function in neonates. Pediatr Crit Care Med 2013; 14 (03) 318-322
- 15 El-Gammacy TM, Shinkar DM, Mohamed NR, Al-Halag AR. Serum cystatin C as an early predictor of acute kidney injury in preterm neonates with respiratory distress syndrome. Scand J Clin Lab Invest 2018; 78 (05) 352-357
- 16 Krawczeski CD, Vandevoorde RG, Kathman T. et al. Serum cystatin C is an early predictive biomarker of acute kidney injury after pediatric cardiopulmonary bypass. Clin J Am Soc Nephrol 2010; 5 (09) 1552-1557
- 17 Boskabadi H, Omidian M, Tavallai S. et al. Serum Hsp70 antigen: early diagnosis marker in perinatal asphyxia. Iran J Pediatr 2015; 25 (02) e381
- 18 Coleman C, Tambay Perez A, Selewski DT, Steflik HJ. Neonatal acute kidney injury. Front Pediatr 2022; 10: 842544
- 19 Leem AY, Park MS, Park BH. et al. Value of serum cystatin C measurement in the diagnosis of sepsis-induced kidney injury and prediction of renal function recovery. Yonsei Med J 2017; 58 (03) 604-612
- 20 Sarnat HB, Sarnat MS. Neonatal encephalopathy following fetal distress. A clinical and electroencephalographic study. Arch Neurol 1976; 33 (10) 696-705
- 21 Gupta BD, Sharma P, Bagla J, Parakh M, Soni JP. Renal failure in asphyxiated neonates. Indian Pediatr 2005; 42 (09) 928-934
- 22 Mehrkesh M, Barekatain B, Gheisari A, Ahmadi M, Shahsanai A. Serum KIM-1 and cystatin levels as the predictors of acute kidney injury in asphyxiated neonates. Iranian Journal of Neonatology 2022; 13 (01) 6-12
- 23 Askenazi DJ, Ambalavanan N, Goldstein SL. Acute kidney injury in critically ill newborns: what do we know? What do we need to learn?. Pediatr Nephrol 2009; 24 (02) 265-274
- 24 Bozkurt O, Yucesoy E. Acute kidney injury in neonates with perinatal asphyxia receiving therapeutic hypothermia. Am J Perinatol 2021; 38 (09) 922-929
- 25 Jetton JG, Boohaker LJ, Sethi SK. et al; Neonatal Kidney Collaborative (NKC). Incidence and outcomes of neonatal acute kidney injury (AWAKEN): a multicentre, multinational, observational cohort study. Lancet Child Adolesc Health 2017; 1 (03) 184-194
- 26 Memon IA, Qudus HA, Waraich IS, Channa S, Marwat A, Lahrasab W. Acute kidney injury in neonates with birth asphyxia at a tertiary care hospital. Pak J Med Health Sci 2021; 15 (03) 573-575
- 27 Alaro D, Bashir A, Musoke R, Wanaiana L. Prevalence and outcomes of acute kidney injury in term neonates with perinatal asphyxia. Afr Health Sci 2014; 14 (03) 682-688
- 28 Medani SA, Kheir AE, Mohamed MB. Acute kidney injury in asphyxiated neonates admitted to a tertiary neonatal unit in Sudan. Sudan J Paediatr 2014; 14 (02) 29-34
- 29 Chishty AL, Iqbal MA, Anjum A, Maqbool S. Risk factor analysis of birth asphyxia at the children's hospital, Lahore. Pak Pediatr J 2002; 26: 47-53
- 30 Malik TS, Chishti AL, Ahmed TM. Short term neurodevelopmental outcome of asphyxiated newborns at tertiary care unit. Pak Pediatr J 2007; 31 (02) 58-61
- 31 Afzal MF, Anjum A, Sultan MA. Risk factor analysis in asphyxiated newborns and their outcome in relation to stage of hypoxic ischemic encephalopathy. Pak Pediatr J 2007; 31 (02) 63-68
- 32 Hidayati EL, Utami MD, Rohsiswatmo R, Tridjaja B. Cystatin C compared to serum creatinine as a marker of acute kidney injury in critically ill neonates. Pediatr Nephrol 2021; 36 (01) 181-186
- 33 Gohiya P, Nadkarni J, Mishra M. Study of neonatal acute kidney injury based on KDIGO criteria. Pediatr Neonatol 2022; 63 (01) 66-70
- 34 Viswanathan S, Manyam B, Azhibekov T, Mhanna MJ. Risk factors associated with acute kidney injury in extremely low birth weight (ELBW) infants. Pediatr Nephrol 2012; 27 (02) 303-311
- 35 Cataldi L, Leone R, Moretti U. et al. Potential risk factors for the development of acute renal failure in preterm newborn infants: a case-control study. Arch Dis Child Fetal Neonatal Ed 2005; 90 (06) F514-F519
- 36 El-Gamasy MA, Nassar MAE. Risk factors for acute kidney injury (AKI) in newly born infants with hypoxic ischemic encephalopathy (HIE). A single center experience. Int J Res Stud Med Health Sci 2017; 2: 1-8
- 37 Momtaz HE, Sabzehei MK, Rasuli B, Torabian S. The main etiologies of acute kidney injury in the newborns hospitalized in the neonatal intensive care unit. J Clin Neonatol 2014; 3 (02) 99-102
- 38 Bardallo Cruzado L, Pérez González E, Martínez Martos Z. et al. Serum cystatin C levels in preterm newborns in our setting: correlation with serum creatinine and preterm pathologies [in English]. Nefrologia 2015; 35 (03) 296-303
- 39 Treiber M, Gorenjak M, Pecovnik Balon B. Serum cystatin-C as a marker of acute kidney injury in the newborn after perinatal hypoxia/asphyxia. Ther Apher Dial 2014; 18 (01) 57-67
- 40 Ahmed AM, Koura HM, Youssef H. et al. Early detection of neonatal kidney disease in high risk neonates admitted to neonatal intensive care unit. World J Med Sci 2014; 11: 518-524