

RSS-Feed abonnieren
DOI: 10.1055/s-0042-1755274
Management of Acute Liver Failure: Update 2022
Autoren
Abstract
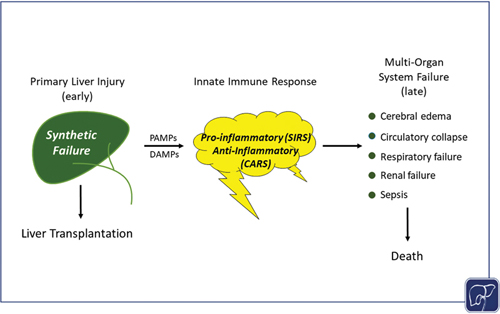
Abbreviated pathogenesis and clinical course of the acute liver failure syndrome. The pathogenesis and clinical course of the syndrome of acute liver failure (ALF) differs depending upon the etiology of the primary liver injury. In turn, the severity of the liver injury and resulting synthetic failure is often the primary determinant of whether a patient is referred for emergency liver transplantation. Injuries by viral etiologies trigger the innate immune system via pathogen-associated molecular patterns (PAMPs), while toxin-induced (and presumably ischemia-induced) injuries do so via damage-associated molecular patterns (DAMPs). The course of the clinical syndrome further depends upon the relative intensity and composition of cytokine release, resulting in an early proinflammatory phenotype (SIRS) and later compensatory anti-inflammatory response phenotype (CARS). The outcomes of overwhelming immune activation are the systemic (extrahepatic) features of ALF (cardiovascular collapse, cerebral edema, acute kidney injury, respiratory failure, sepsis) which ultimately determine the likelihood of death.
Acute liver failure (ALF) continues to carry a high risk of mortality or the need for transplantation despite recent improvements in overall outcomes over the past two decades. Optimal management begins with identifying that liver failure is indeed present and its etiology, since outcomes and the need for transplantation vary widely across the different etiologies. Most causes of ALF can be divided into hyperacute (ischemia and acetaminophen) and subacute types (other etiologies), based on time of evolution of signs and symptoms of liver failure; the former evolve in 3 to 4 days and the latter typically in 2 to 4 weeks. Both involve intense release of cytokines and hepatocellular contents into the circulation with multiorgan effects/consequences.
Management involves optimizing fluid balance and cardiovascular support, including the use of continuous renal replacement therapy, vasopressors, and pulmonary ventilation. Early evaluation for liver transplantation is advised particularly for acetaminophen toxicity, which evolves so rapidly that delay is likely to lead to death.
Vasopressor support, high-grade hepatic encephalopathy, and unfavorable (subacute) etiologies heighten the need for urgent listing for liver transplantation. Prognostic scores such as Kings Criteria, Model for End-Stage Liver Disease, and the Acute Liver Failure Group prognostic index take these features into account and provide reasonable but imperfect predictive accuracy. Future treatments may include liver support devices and/or agents that improve hepatocyte regeneration.
Keywords
encephalopathy - coagulopathy - hepatocyte injury - renal replacement therapy - prognostic scorePublikationsverlauf
Artikel online veröffentlicht:
24. August 2022
© 2022. Thieme. All rights reserved.
Thieme Medical Publishers, Inc.
333 Seventh Avenue, 18th Floor, New York, NY 10001, USA
-
References
- 1 Rakela J, Lange SM, Ludwig J, Baldus WP. Fulminant hepatitis: Mayo Clinic experience with 34 cases. Mayo Clin Proc 1985; 60 (05) 289-292
- 2 Bernal W, Hyyrylainen A, Gera A. et al. Lessons from look-back in acute liver failure? A single centre experience of 3300 patients. J Hepatol 2013; 59 (01) 74-80
- 3 Reuben A, Tillman H, Fontana RJ. et al. Outcomes in adults with acute liver failure (ALF) from 1998–2013: an observational cohort study. Ann Intern Med 2016; 164 (11) 724-732
- 4 Moreau R, Jalan R, Gines P. et al; CANONIC Study Investigators of the EASL–CLIF Consortium. Acute-on-chronic liver failure is a distinct syndrome that develops in patients with acute decompensation of cirrhosis. Gastroenterology 2013; 144 (07) 1426-1437 , 1437.e1–1437.e9
- 5 Lee WM. Acetaminophen (APAP) hepatotoxicity-isn't it time for APAP to go away?. J Hepatol 2017; 67 (06) 1324-1331
- 6 Hoofnagle JH, Björnsson ES. Drug-induced liver injury—types and phenotypes. N Engl J Med 2019; 381 (03) 264-273
- 7 Stravitz RT, Lee WM. Acute liver failure. Lancet 2019; 394 (10201): 869-881
- 8 Mendizabal M, Marciano S, Videla MG. et al. Changing etiologies and outcomes of acute liver failure: perspectives from 6 transplant centers in Argentina. Liver Transpl 2014; 20 (04) 483-489
- 9 Chalasani N, Bonkovsky HL, Fontana R. et al; United States Drug Induced Liver Injury Network. Features and outcomes of 899 patients with drug-induced liver injury: the DILIN prospective study. Gastroenterology 2015; 148 (07) 1340-52 .e7
- 10 Reddy KR, Beavers KL, Hammond SP, Lim JK, Falck-Ytter YT. American Gastroenterological Association Institute. American Gastroenterological Association Institute guideline on the prevention and treatment of hepatitis B virus reactivation during immunosuppressive drug therapy. Gastroenterology 2015; 148 (01) 215-219 , quiz e16–e17
- 11 ) Viral hepatitis surveillance—United States, 2017. Atlanta: US Department of Health and Human Services, Centers for Disease Control and Prevention; 2019. Accessed on June 13, 2022, at: /hepatitis/statistics/2017surveillance/index.htm
- 12 Nelson NP, Weng MK, Hofmeister MG. et al. Prevention of hepatitis A virus infection in the United States: recommendations of the Advisory Committee on Immunization Practices, 2020. MMWR Recomm Rep 2020; 69 (05) 1-38
- 13 Rao A, Rule JA, Hameed B, Ganger D, Fontana RJ, Lee WM. Secular trends in severe idiosyncratic drug-induced liver injury in North America: an update from the ALFSG registry. Am J Gastroenterol 2022; In press
- 14 Heard K, Rumack BH, Green JL. et al. A single-arm clinical trial of a 48-hour intravenous N-acetylcysteine protocol for treatment of acetaminophen poisoning. Clin Toxicol (Phila) 2014; 52 (05) 512-518
- 15 Davern II TJ, James LP, Hinson JA. et al; Acute Liver Failure Study Group. Measurement of serum acetaminophen-protein adducts in patients with acute liver failure. Gastroenterology 2006; 130 (03) 687-694
- 16 Khandelwal N, James LP, Sanders C, Larson AM, Lee WM. Acute Liver Failure Study Group. Unrecognized acetaminophen toxicity as a cause of indeterminate acute liver failure. Hepatology 2011; 53 (02) 567-576
- 17 Leventhal TM, Gottfried M, Olson JC, Subramanian RM, Hameed B, Lee WM. Acute Liver Failure Study Group. Acetaminophen is undetectable in plasma form more than half of patients believed to have acute liver failure due to overdose. Clin Gastroenterol Hepatol 2019; 17 (10) 2110-2116
- 18 James LP, Letzig L, Simpson PM. et al. Pharmacokinetics of acetaminophen-protein adducts in adults with acetaminophen overdose and acute liver failure. Drug Metab Dispos 2009; 37 (08) 1779-1784
- 19 Fix OK, Liou I, Karvellas CJ. et al; Acute Liver Failure Study Group. Development and pilot of a checklist for management of acute liver failure in the intensive care unit. PLoS One 2016; 11 (05) e0155500
- 20 Shalimar KS, Kedia S, Gunjan D. et al. Acute liver failure due to hepatitis E virus infection is associated with better survival than other etiologies in Indian patients. Dig Dis Sci 2017; 62 (04) 1058-1066
- 21 Ganger DR, Rule J, Rakela J. et al; Acute Liver Failure Study Group. Acute liver failure of indeterminate etiology: a comprehensive systematic approach by an expert committee to establish causality. Am J Gastroenterol 2018; 113 (09) 1319-1328
- 22 Somasekar S, Lee D, Rule J. et al. Viral surveillance in serum samples from patients with acute liver failure by metagenomic next-generation sequencing. Clin Infect Dis 2017; 65 (09) 1477-1485
- 23 Long A, Magrath M, Mihalopoulos M. et al. Changes in epidemiology of overdoses in an urban county hospital after 20 years. Am J Gastro 2022; In press
- 24 Stravitz RT, Kramer AH, Davern T. et al. Acute Liver Failure Study Group. Intensive care of patients with acute liver failure: recommendations of the U.S. Acute Liver Failure Study Group. Crit Care Med 2007; 35 (11) 2498-2508
- 25 Rabinowich L, Wendon J, Bernal W, Shibolet O. Clinical management of acute liver failure: results of an international multi-center survey. World J Gastroenterol 2016; 22 (33) 7595-7603
- 26 Lee WM, Hynan LS, Rossaro L. et al; Acute Liver Failure Study Group. Intravenous N-acetylcysteine improves transplant-free survival in early stage non-acetaminophen acute liver failure. Gastroenterology 2009; 137 (03) 856-864 , 864.e1
- 27 Siu JT, Nguyen T, Turgeon RD. N-acetylcysteine for non-paracetamol (acetaminophen)-related acute liver failure. Cochrane Database Syst Rev 2020; 12: CD012123
- 28 Hennes EM, Zeniya M, Czaja AJ. et al; International Autoimmune Hepatitis Group. Simplified criteria for the diagnosis of autoimmune hepatitis. Hepatology 2008; 48 (01) 169-176
- 29 Stravitz RT, Lefkowitch JH, Fontana RJ. et al; Acute Liver Failure Study Group. Autoimmune acute liver failure: proposed clinical and histological criteria. Hepatology 2011; 53 (02) 517-526
- 30 Leung PSC, Rossaro L, Davis PA. et al; Acute Liver Failure Study Group. Antimitochondrial antibodies in acute liver failure: implications for primary biliary cirrhosis. Hepatology 2007; 46 (05) 1436-1442
- 31 Yeoman AD, Westbrook RH, Zen Y. et al. Prognosis of acute severe autoimmune hepatitis (AS-AIH): the role of corticosteroids in modifying outcome. J Hepatol 2014; 61 (04) 876-882
- 32 Czaja AJ. Corticosteroids or not in severe acute or fulminant autoimmune hepatitis: therapeutic brinksmanship and the point beyond salvation. Liver Transpl 2007; 13 (07) 953-955
- 33 Rahim MN, Miquel R, Heneghan MA. Approach to the patient with acute severe autoimmune hepatitis. JHEP Rep 2020; 2 (06) 100149
- 34 De Martin E, Coilly A, Chazouillères O. et al; FILFOIE consortium – France. Early liver transplantation for corticosteroid non-responders with acute severe autoimmune hepatitis: the SURFASA score. J Hepatol 2021; 74 (06) 1325-1334
- 35 Mendizabal M, Marciano S, Videla MG. et al. Fulminant presentation of autoimmune hepatitis: clinical features and early predictors of corticosteroid treatment failure. Eur J Gastroenterol Hepatol 2015; 27 (06) 644-648
- 36 Kumar M, Satapathy S, Monga R. et al. A randomized controlled trial of lamivudine to treat acute hepatitis B. Hepatology 2007; 45 (01) 97-101
- 37 Yu J-W, Sun L-J, Yan B-Z, Kang P, Zhao Y-H. Lamivudine treatment is associated with improved survival in fulminant hepatitis B. Liver Int 2011; 31 (04) 499-506
- 38 Tillmann HL, Hadem J, Leifeld L. et al. Safety and efficacy of lamivudine in patients with severe acute or fulminant hepatitis B, a multicenter experience. J Viral Hepat 2006; 13 (04) 256-263
- 39 Dao DY, Seremba E, Ajmera V, Sanders C, Hynan LS, Lee WM. Acute Liver Failure Study Group. Use of nucleoside (tide) analogues in patients with hepatitis B-related acute liver failure. Dig Dis Sci 2012; 57 (05) 1349-1357
- 40 Mantzoukis K, Rodríguez-Perálvarez M, Buzzetti E. et al. Pharmacological interventions for acute hepatitis B infection: an attempted network meta-analysis. Cochrane Database Syst Rev 2017; 3 (03) CD011645
- 41 Norvell JP, Blei AT, Jovanovic BD, Levitsky J. Herpes simplex virus hepatitis: an analysis of the published literature and institutional cases. Liver Transpl 2007; 13 (10) 1428-1434
- 42 Nanchal R, Subramanian R, Karvellas CJ. et al. Guidelines for the management of adult acute and acute-on-chronic liver failure in the ICU: cardiovascular, endocrine, hematologic, pulmonary, and renal considerations. Crit Care Med 2020; 48 (03) e173-e191
- 43 Lee WM, Stravitz RT, Larson AM. Introduction to the AASLD Position Paper on acute liver failure. Hepatology 2012; 55: 965-967
- 44 Harry R, Auzinger G, Wendon J. The clinical importance of adrenal insufficiency in acute hepatic dysfunction. Hepatology 2002; 36 (02) 395-402
- 45 Audimoolam VK, McPhail MJ, Willars C. et al. Predicting fluid responsiveness in acute liver failure: a prospective study. Anesth Analg 2017; 124 (02) 480-486
- 46 Larsen FS, Schmidt LE, Bernsmeier C. et al. High-volume plasma exchange in patients with acute liver failure: an open randomised controlled trial. J Hepatol 2016; 64 (01) 69-78
- 47 Stahl K, Hadem J, Schneider A. et al. Therapeutic plasma exchange in acute liver failure. J Clin Apher 2019; 34 (05) 589-597
- 48 Maiwall R, Bajpai M, Singh A. et al. Standard-volume plasma exchange improves outcomes in patients with acute liver failure: a randomized controlled trial. Clin Gastroenterol Hepatol 2022; 20 (04) e831-e854
- 49 MacDonald AJ, Subramanian RM, Olson JC. et al; Use of the molecular adsorbent recirculating system in acute liver failure: results of a multicenter propensity score-matched study. Crit Care Med 2022; 50 (02) 286-295
- 50 MacDonald AJ, Speiser JL, Ganger DR. et al; US Acute Liver Failure Study Group. Clinical and neurologic outcomes in acetaminophen-induced acute liver failure: A 21-year multicenter cohort study. Clin Gastroenterol Hepatol 2021; 19 (12) 2615-2625 .e3
- 51 Karvellas CJ, Fix OK, Battenhouse H, Durkalski V, Sanders C, Lee WM. U S Acute Liver Failure Study Group. Outcomes and complications of intracranial pressure monitoring in acute liver failure: a retrospective cohort study. Crit Care Med 2014; 42 (05) 1157-1167
- 52 Rajajee V, Williamson CA, Fontana RJ, Courey AJ, Patil PG. Noninvasive intracranial pressure assessment in acute liver failure. Neurocrit Care 2018; 29 (02) 280-290
- 53 Murphy N, Auzinger G, Bernel W, Wendon J. The effect of hypertonic sodium chloride on intracranial pressure in patients with acute liver failure. Hepatology 2004; 39 (02) 464-470
- 54 Kalal CR, Maiwall R, Choudhary A. et al. Mannitol is comparable to hypertonic saline for raised intracranial pressure in Acute Liver Failure (MAHAL Study): a RCT. Dig Dis 2021
- 55 Hamdi T, Yessayan L, Yee J, Szamosfalvi B. High sodium continuous veno-venous hemodialysis with regional citrate anticoagulation and online dialysate generation in patients with acute liver failure and cerebral edema. Hemodial Int 2018; 22 (02) 184-191
- 56 Clemmesen JO, Larsen FS, Kondrup J, Hansen BA, Ott P. Cerebral herniation in patients with acute liver failure is correlated with arterial ammonia concentration. Hepatology 1999; 29 (03) 648-653
- 57 Bernal W, Hall C, Karvellas CJ, Auzinger G, Sizer E, Wendon J. Arterial ammonia and clinical risk factors for encephalopathy and intracranial hypertension in acute liver failure. Hepatology 2007; 46 (06) 1844-1852
- 58 Cordoba J, Blei AT, Mujais S. Determinants of ammonia clearance by hemodialysis. Artif Organs 1996; 20 (07) 800-803
- 59 Slack AJ, Auzinger G, Willars C. et al. Ammonia clearance with haemofiltration in adults with liver disease. Liver Int 2014; 34 (01) 42-48
- 60 Warrillow S, Fisher C, Bellomo R. Correction and control of hyperammonemia in acute liver failure: the impact of continuous renal replacement timing, intensity, and duration. Crit Care Med 2020; 48 (02) 218-224
- 61 Cardoso FS, Gottfried M, Tujios S, Olson JC, Karvellas CJ. US Acute Liver Failure Study Group. Continuous renal replacement therapy is associated with reduced serum ammonia levels and mortality in acute liver failure. Hepatology 2018; 67 (02) 711-720
- 62 Acharya SK, Bhatia V, Sreenivas V, Khanal S, Panda SK. Efficacy of L-ornithine L-aspartate in acute liver failure: a double-blind, randomized, placebo-controlled study. Gastroenterology 2009; 136 (07) 2159-2168
- 63 Jalan R, Lee WM. Treatment of hyperammonemia in liver failure: a tale of two enzymes. Gastroenterology 2009; 136 (07) 2048-2051
- 64 Stravitz RT, Gottfried M, Durkalski V. et al; Acute Liver Failure Study Group. Safety, tolerability, and pharmacokinetics of l-ornithine phenylacetate in patients with acute liver injury/failure and hyperammonemia. Hepatology 2018; 67 (03) 1003-1013
- 65 Jalan R, Olde Damink SW, Deutz NE, Hayes PC, Lee A. Moderate hypothermia in patients with acute liver failure and uncontrolled intracranial hypertension. Gastroenterology 2004; 127 (05) 1338-1346
- 66 Stravitz RT, Larsen FS. Therapeutic hypothermia for acute liver failure. Crit Care Med 2009; 37 (7, Suppl): S258-S264
- 67 Bernal W, Murphy N, Brown S. et al. A multicentre randomized controlled trial of moderate hypothermia to prevent intracranial hypertension in acute liver failure. J Hepatol 2016; 65 (02) 273-279
- 68 Stravitz RT, Ellerbe C, Durkalski V. et al; Acute Liver Failure Study Group. Bleeding complications in acute liver failure. Hepatology 2018; 67 (05) 1931-1942
- 69 Lisman T, Stravitz RT. Rebalanced hemostasis in patients with acute liver failure. Semin Thromb Hemost 2015; 41 (05) 468-473
- 70 Stravitz RT, Lisman T, Luketic VA. et al. Minimal effects of acute liver injury/acute liver failure on hemostasis as assessed by thromboelastography. J Hepatol 2012; 56 (01) 129-136
- 71 Habib M, Roberts LN, Patel RK, Wendon J, Bernal W, Arya R. Evidence of rebalanced coagulation in acute liver injury and acute liver failure as measured by thrombin generation. Liver Int 2014; 34 (05) 672-678
- 72 Stravitz RT, Ellerbe C, Durkalski V, Reuben A, Lisman T, Lee WM. Acute Liver Failure Study Group. Thrombocytopenia is associated with multi-organ system failure in patients with acute liver failure. Clin Gastroenterol Hepatol 2016; 14 (04) 613-620 .e4
- 73 Driever EG, Stravitz RT, Zhang J. et al. VWF/ADAMTS13 imbalance, but not global coagulation or fibrinolysis, is associated with outcome and bleeding in acute liver failure. Hepatology 2021; 73 (05) 1882-1891
- 74 Stravitz RT, Bowling R, Bradford RL. et al. Role of procoagulant microparticles in mediating complications and outcome of acute liver injury/acute liver failure. Hepatology 2013; 58 (01) 304-313
- 75 Stravitz RT, Fontana RJ, Meinzer C. et al; ALF Study Group. Coagulopathy, bleeding events, and outcome according to rotational thromboelastometry in patients with acute liver injury/failure. Hepatology 2021; 74 (02) 937-949
- 76 Stravitz RT. Algorithms for managing coagulation disorders in patients with liver disease. Hepatol Int 2018; 12 (05) 390-401
- 77 O'Grady JG, Alexander GJ, Hayllar KM, Williams R. Early indicators of prognosis in fulminant hepatic failure. Gastroenterology 1989; 97 (02) 439-445
- 78 Bernuau J, Goudeau A, Poynard T. et al. Multivariate analysis of prognostic factors in fulminant hepatitis B. Hepatology 1986; 6 (04) 648-651
- 79 Cholongitas E, Theocharidou E, Vasianopoulou P. et al. Comparison of the Sequential Organ Failure Assessment score with the King's College Hospital criteria and the model for end-stage liver disease score for the prognosis of acetaminophen-induced acute liver failure. Liver Transpl 2012; 18 (04) 405-412
- 80 Schmidt LE, Larsen FS. MELD score as a predictor of liver failure and death in patients with acetaminophen-induced liver injury. Hepatology 2007; 45 (03) 789-796
- 81 Yantorno SE, Kremers WK, Ruf AE, Trentadue JJ, Podestá LG, Villamil FG. MELD is superior to King's College and Clichy's criteria to assess prognosis in fulminant hepatic failure. Liver Transpl 2007; 13 (06) 822-828
- 82 McPhail MJ, Farne H, Senvar N, Wendon JA, Bernal W. Ability of King's College Criteria and Model for End-Stage Liver Disease scores to predict mortality of patients with acute liver failure. A meta-analysis. Clin Gastroenterol Hepatol 2016; 14 (04) 516-525 .e5, quiz e43–e45
- 83 Rutherford A, King LY, Hynan LS. et al; ALF Study Group. Development of an accurate index for predicting outcomes of patients with acute liver failure. Gastroenterology 2012; 143 (05) 1237-1243
- 84 Craig DG, Simpson KJ. Accuracy of the ALFSG index as a triage marker in acute liver failure. Gastroenterology 2013; 144 (01) e25
- 85 Koch DG, Tillman H, Durkalski V, Lee WM, Reuben A. Development of a model to predict transplant-free survival of patients with acute liver failure. Clin Gastroenterol Hepatol 2016; 14 (08) 1199-1206 .e2
- 86 Hadem J, Stiefel P, Bahr MJ. et al. Prognostic implications of lactate, bilirubin, and etiology in German patients with acute liver failure. Clin Gastroenterol Hepatol 2008; 6 (03) 339-345
- 87 Figueira ERR, Rocha-Filho JA, Lanchotte C. et al. Creatinine-lactate score predicts mortality in non-acetaminophen-induced acute liver failure in patients listed for liver transplantation. BMC Gastroenterol 2021; 21 (01) 252-255
- 88 Mitchell I, Bihari D, Chang R, Wendon J, Williams R. Earlier identification of patients at risk from acetaminophen-induced acute liver failure. Crit Care Med 1998; 26 (02) 279-284
- 89 Kumar R, Shalimar, Sharma H. et al. Prospective derivation and validation of early dynamic model for predicting outcome in patients with acute liver failure. Gut 2012; 61 (07) 1068-1075
- 90 Bernal W, Wang Y, Maggs J. et al. Development and validation of a dynamic outcome prediction model for paracetamol-induced acute liver failure: a cohort study. Lancet Gastroenterol Hepatol 2016; 1 (03) 217-225
- 91 Fontana RJ, Stravitz RT, Durkalski V. et al. Prognostic value of the 13 C-methacetin breath test in adults with acute liver failure and non-acetaminophen acute liver injury. Hepatology 2021; 74 (02) 961-972
- 92 Schmidt LE, Dalhoff K. Alpha-fetoprotein is a predictor of outcome in acetaminophen-induced liver injury. Hepatology 2005; 41 (01) 26-31
- 93 Schmidt LE, Dalhoff K. Serum phosphate is an early predictor of outcome in severe acetaminophen-induced hepatotoxicity. Hepatology 2002; 36 (03) 659-665
- 94 Antoniades CG, Berry PA, Davies ET. et al. Reduced monocyte HLA-DR expression: a novel biomarker of disease severity and outcome in acetaminophen-induced acute liver failure. Hepatology 2006; 44 (01) 34-43
- 95 Schiødt FV, Rossaro L, Stravitz RT, Shakil AO, Chung RT, Lee WM. Acute Liver Failure Study Group. Gc-globulin and prognosis in acute liver failure. Liver Transpl 2005; 11 (10) 1223-1227
- 96 Karvellas CJ, Speiser JL, Tremblay M, Lee WM, Rose CF. US Acute Liver Failure Study Group. Elevated FABP1 serum levels are associated with poorer survival in acetaminophen-induced acute liver failure. Hepatology 2017; 65 (03) 938-949
- 97 Karvellas CJ, Speiser JL, Tremblay M, Lee WM, Rose CF. US Acute Liver Failure Study Group. Elevated serum liver-type fatty acid binding protein levels in non-acetaminophen acute liver failure patients with organ dysfunction. Dig Dis Sci 2021; 66 (01) 273-283
- 98 Tavabie OD, Karvellas CJ, Salehi S. et al; United States Acute Liver Failure Study Group. A novel microRNA-based prognostic model outperforms standard prognostic models in patients with acetaminophen-induced acute liver failure. J Hepatol 2021; 75 (02) 424-434
- 99 Zabron A, Quaglia A, Fatourou E. et al. Clinical and prognostic associations of liver volume determined by computed tomography in acute liver failure. Liver Int 2018; 38 (09) 1592-1601
- 100 Donaldson BW, Gopinath R, Wanless IR. et al. The role of transjugular liver biopsy in fulminant liver failure: relation to other prognostic indicators. Hepatology 1993; 18 (06) 1370-1376
- 101 Singhal A, Vadlamudi S, Stokes K. et al. Liver histology as predictor of outcome in patients with acute liver failure. Transpl Int 2012; 25 (06) 658-662
- 102 Ndekwe P, Ghabril MS, Zang Y, Mann SA, Cummings OW, Lin J. Substantial hepatic necrosis is prognostic in fulminant liver failure. World J Gastroenterol 2017; 23 (23) 4303-4310
- 103 Kanjo A, Ocskay K, Gede N. et al. Efficacy and safety of liver support devices in acute and hyperacute liver failure: a systematic review and network meta-analysis. Sci Rep 2021; 11 (01) 4189
- 104 Germani G, Theocharidou E, Adam R. et al. Liver transplantation for acute liver failure in Europe: outcomes over 20 years from the ELTR database. J Hepatol 2012; 57 (02) 288-296
- 105 Freeman Jr RB, Steffick DE, Guidinger MK, Farmer DG, Berg CL, Merion RM. Liver and intestine transplantation in the United States, 1997-2006. Am J Transplant 2008; 8 (4 Pt 2): 958-976
- 106 Barshes NR, Lee TC, Balkrishnan R, Karpen SJ, Carter BA, Goss JA. Risk stratification of adult patients undergoing orthotopic liver transplantation for fulminant hepatic failure. Transplantation 2006; 81 (02) 195-201
- 107 Reddy KR, Ellerbe C, Schilsky M. et al; Acute Liver Failure Study Group. Determinants of outcome among patients with acute liver failure listed for liver transplantation in the United States. Liver Transpl 2016; 22 (04) 505-515
- 108 Wong NZ, Reddy KR, Bittermann T. Acute liver failure etiology is an independent predictor of waitlist outcome but not posttransplantation survival in a national cohort. Liver Transpl 2022; 28 (01) 39-50
- 109 Campsen J, Blei AT, Emond JC. et al; Adult-to-Adult Living Donor Liver Transplantation Cohort Study Group. Outcomes of living donor liver transplantation for acute liver failure: the adult-to-adult living donor liver transplantation cohort study. Liver Transpl 2008; 14 (09) 1273-1280
- 110 Yamashiki N, Sugawara Y, Tamura S. et al. Outcomes after living donor liver transplantation for acute liver failure in Japan: results of a nationwide survey. Liver Transpl 2012; 18 (09) 1069-1077
- 111 Chen HS, Joo DJ, Shaheen M. et al. Randomized trial of spheroid reservoir bioartificial liver in porcine model of post-hepatectomy liver failure. Hepatology 2019; 69 (01) 329-342
- 112 Ahmadi AR, Chicco M, Wesson RN. et al. Stem cell mobilization is lifesaving in a large animal preclinical model of acute liver failure. Ann Surg 2018; 268 (04) 620-631
- 113 Wuestefeld T, Pesic M, Rudalska R. et al. A direct in vivo RNAi screen identifies MKK4 as a key regulator of liver regeneration. Cell 2013; 153 (02) 389-401
- 114 Bernal W, Donaldson N, Wyncoll D, Wendon J. Blood lactate as an early predictor of outcome in paracetamol-induced acute liver failure: a cohort study. Lancet 2002; 359 (9306): 558-563