

Subscribe to RSS
DOI: 10.1055/a-1535-8807
The COVID-19 Pandemic and the Need for an Integrated and Equitable Approach: An International Expert Consensus Paper
Authors
Abstract
Background One year after the declaration of the coronavirus disease 2019 (COVID-19) pandemic by the World Health Organization (WHO) and despite the implementation of mandatory physical barriers and social distancing, humanity remains challenged by a long-lasting and devastating public health crisis.
Management Non-pharmacological interventions (NPIs) are efficient mitigation strategies. The success of these NPIs is dependent on the approval and commitment of the population. The launch of a mass vaccination program in many countries in late December 2020 with mRNA vaccines, adenovirus-based vaccines, and inactivated virus vaccines has generated hope for the end of the pandemic.
Current Issues The continuous appearance of new pathogenic viral strains and the ability of vaccines to prevent infection and transmission raise important concerns as we try to achieve community immunity against severe acute respiratory syndrome coronavirus type 2 (SARS-CoV-2) and its variants. The need of a second and even third generation of vaccines has already been acknowledged by the WHO and governments.
Perspectives There is a critical and urgent need for a balanced and integrated strategy for the management of the COVID-19 outbreaks organized on three axes: (1) Prevention of the SARS-CoV-2 infection, (2) Detection and early diagnosis of patients at risk of disease worsening, and (3) Anticipation of medical care (PDA).
Conclusion The “PDA strategy” integrated into state policy for the support and expansion of health systems and introduction of digital organizations (i.e., telemedicine, e-Health, artificial intelligence, and machine-learning technology) is of major importance for the preservation of citizens' health and life world-wide.
Introduction
One year since the declaration of the severe acute respiratory syndrome coronavirus type 2 (SARS-CoV-2) as a pandemic infection by the World Health Organization (WHO), physical barriers and social distancing have been implemented in most countries. Nevertheless, humanity is facing a long-lasting and devastating public health crisis which has already cost more than 3,800,900 lives with at least 176,052,575 cases as of June 12, 2021. In most of the countries worldwide, hospitals and health care systems were under an unprecedented pressure during the three epidemic waves. A fourth epidemic wave seems very probable whereas the tolerance of the populations and the resistance of economies at the lockdown policies are reaching their limits.[1]
During the spring of 2020, the world faced the new coronavirus pandemic with limited knowledge of SARS-CoV-2 and the resulting coronavirus disease 2019 (COVID-19), without widely available validated diagnostic tools, therapeutic strategies, and prepared health care systems. Therefore, in most countries the mandatory national lockdown was the only strategy to control virus propagation, to save lives, and to protect health systems from collapse. Since then, non-pharmacological interventions (NPIs)—particularly curfews and lockdowns—and vaccinations have been the principal strategies for the management of the epidemic waves. In addition, large-scale population testing has been adopted for epidemiological surveillance at regional and national levels.
The molecular evolution of SARS-CoV-2 is another public health threat since transmission rates appear to have increased with some recently identified variant strains with varying pathogenicity and potentially higher resistance to natural and vaccine-induced immunity.[2] [3] [4] Management of the forthcoming epidemic waves will become a major issue for public health, the world economy as well as for social adhesion and democracy. Considerable knowledge on the biological characteristics of SARS-CoV-2, the pathophysiology and natural history of COVID-19, and diagnostic tools and therapeutic strategies has been gained and has significantly improved the clinical outcomes of the patients with severe or critical COVID-19.
This article reviews the limitations of the current policies for the management of the pandemic and proposes an integrated and balanced strategy including the anticipated management of patients with COVID-19.
Limitations of the “Stop and Go” Strategy
NPIs, including simple physical barriers (i.e., masks, hand washing, and distancing), radical measures to avoid crowding and to reduce social contact (such as closing of restaurants, bars, commercial shops, curfew), mandatory national lockdowns combined with testing the population by RT-PCR (reverse transcription polymerase chain reaction) for SARS-COV-2 and close tracing of contact cases are efficient for the mitigation of the pandemic and decrease of the virus reproduction number (R0).[5] [6]
The “Stop and Go” strategy is a temporary measure mainly intending to reduce the number of new cases per day, to facilitate contact tracing, and to diminish severe COVID-19 requiring hospitalization.[7] [8] [9] Individual's compliance with a series of behavioral recommendations provided by the public health authorities plays a critical role in the control and prevention of SARS-CoV2 infection. The success of such severe NPI requires the approval and the commitment of the population. Sociocultural, psychosocial, and social cognitive factors are determinants of individual differences in the health preventative behaviors.[10] [11]
The available hospital beds and the number of the health care workers at the conventional wards and intensive care units (ICUs) are major factors which, together with the strength of the epidemic wave, determine the intensity and the duration of the NPI. Nevertheless, they have devastating midterm and long-term effects on socioeconomic activity and may restrict human constitutional rights and increase social inequalities.[12] [13]
A complementary mitigation strategy relies principally on intensive investment in epidemiological surveillance, contact tracing, and isolation of infected cases, which are more easily accomplished when the number of new infections per day is limited as recommended by the WHO accompanied by localized lockdowns.[14] [15] Hence, the management of patients with COVID-19, at least in European countries, remains centralized in hospitals, whereas primary health care structures are less implicated and an organized campaign for therapeutic intervention in the community is still limited.[16]
The long-term strategy is actually based on the concept of fast development and accelerated authorization of vaccines. Indeed this is an efficient way to increase the population's immunity against SARS-CoV-2. Moreover, high vaccination rates are associated with lower infection rates at later time points among the unvaccinated citizens.[17] Accordingly, application of wide-scale international vaccination programs could lead to the control of the pandemic and to the decrease of R0. Indeed, in European Union (EU) countries the main plan is to vaccinate 70% to 80% of the entire adult population by the summer of 2021.[18] However, sufficient vaccine doses are far from being available leading to serious doubts about the short-term success of vaccination. In addition, vaccination acceptance is highly variable from one country to another and largely depends on the public trust on state policy for the management of the pandemic and the impact of misinformation spreading on large social media.[19] [20] [21]
Considerations to Improve the Feasibility of Vaccination Programs
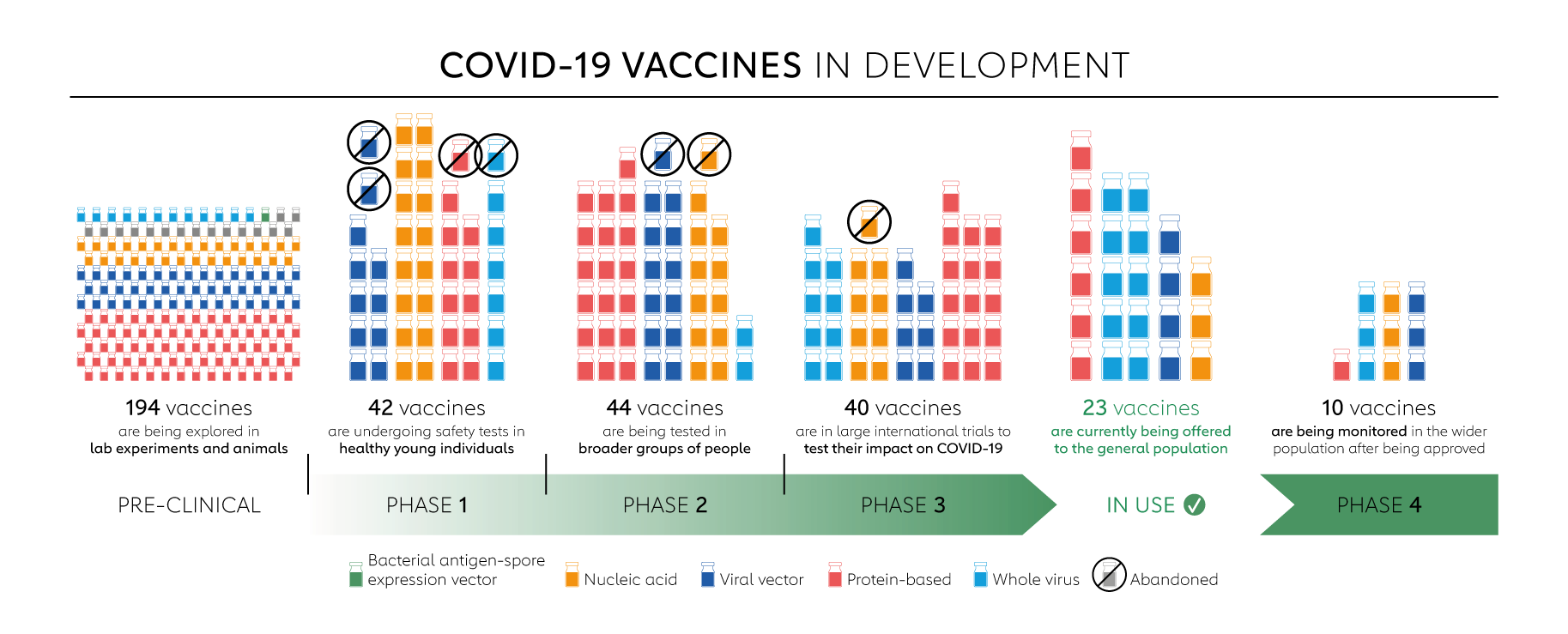
There are four categories of vaccines tested in clinical trials: whole virus, protein subunit, viral vector and nucleic acid (RNA and DNA). To date, 185 vaccines have been explored in laboratory experiments and animals and 97 are in phases I to III. [Table 1] summarizes the vaccines which have been studied in phase III trials and the results have been published or communicated in press releases of the companies. Among the 15 vaccines which are currently being offered to the general population, 2 are nucleic acid based, 2 are protein based, 4 are viral vector based, and 7 are whole virus.[22] Among them, the most widely used vaccines in mass vaccination programs to prevent symptomatic COVID-19 are those encoding the spike protein antigen of SARS-CoV-2 in mRNA-based technology (BNT162b2 -BioNTech/Pfizer and mRNA1273—Moderna) and adenovirus vector-based vaccines (Gamaleya, AstraZeneca, CanSino, Johnson & Johnson). In addition, three inactivated virus vaccines (Sinovac, Sinopharm, Bharat Biotech) are also used in some countries. The launching of the vaccination program in December 2020 generated hope for the forthcoming end of the pandemic. Nevertheless, real-life concerns emerged about the midterm efficacy of the vaccines and developing limitations of the feasibility of a rapid mass vaccination program on a global level whereas some concerns because of very rare thrombotic complications emerged. Several important limitations can be outlined.
Scientific Reviewer Committee Members: Gregory Y. H. Lip, Michael Makris, Sam Schulman, Wolfgang Siess, Christian Weber
-
The phase III trials of the vaccines have variable endpoints such as (1) protecting against the most severe forms of COVID-19, (2) reducing hospitalization for COVID-19, (3) preventing infection and/or transmission of SARS-CoV-2. Knowledge of protection against mild COVID-19 disease is also needed. The designs of the randomized clinical trials might overestimate the level of vaccine protection compared with real-world settings.[23]
The translation of the efficacy of the vaccines and the duration of protective immunity, the protection of the virus spread, or even the protection of some groups of citizens which were not included in the studies (i.e., multimorbid patients, children) need to be specifically tested.[24] [25] [26]
-
The cost of vaccines (particularly those based on mRNA technology) raises a major obstacle for vaccination of large populations, especially in developing and low-income countries.[27] Limitations of production plants and supply chains provoke significant delays and compromise the implementation and the trust of the population to vaccinate. Indeed, mRNA vaccines' stability, storage, and distribution require very low temperature chain logistics which are limited notably in less developed countries. The applicability of the global vaccination program is questioned, particularly in low- and middle-income countries, having limited human and financial resources.
-
Wealthy nations representing just 13% of the world's population have already accounted for 51% of the promised doses of leading COVID-19 vaccines.[28] Until April 2021, although more than 700 million vaccine doses have been administered globally, richer countries have received more than 87%, and low-income countries just 0.2%.[29] The vaccines are essentially absent in most countries of the sub-Saharan African region, Asia, and South America. Even in developed countries, there are great discrepancies in the vaccination rate ranging from 8% to 98%.[30] Chile is a notable exemption regarding the vaccination rate of the population (47% of the population is fully vaccinated as of June 12). Surprisingly, this did not prevent an intensive third epidemic wave which actually hit the country, underlining that even a high vaccination rate, which is lower than the threshold of community immunity, is not sufficient to prevent an epidemic wave. These data reveal an important gap between the production capacities of the pharmaceutical companies and consortiums, producers of vaccines, and the need for the rapid mass vaccination of the world population. This gap together with the commercial strategies of some pharmaceutical companies raises serious ethical questions and drawbacks in the application of the vaccination worldwide with significant negative consequences on public health.[31] [32]
Vaccines' nationalism, as it has been described by the WHO, compromises the effective control of the pandemic and could increase the risk of the SARS-CoV-2 mutations and appearance of resistant variants of the virus.[33] In addition, the great discrepancies in the vaccination rate among countries reveal the geopolitical concurrence at the international level. These factors raise serious concerns regarding the achievement, before the end of 2021, of collective immunity at the threshold of 70% to 80%, which has been set by the WHO as a prerequisite for the control of the pandemic.
-
The low vaccination rate has an enormous impact on the national and global economy. According to the World Bank, world's gross domestic product of the global economy probably shrank by 4.3% in 2020 (i.e., $3.94 trillion).[34] A study commissioned by the International Chamber of Commerce Research Foundation showed that the global economy stands to lose as much as $9.2 trillion if governments fail to ensure developing economies access to COVID-19 vaccines. As much as half of this amount will fall on advanced economies.[35]
To challenge this issue, the COVAX (COVID-19 Vaccines Global Access Facility), which is co-led by GAVI (the Vaccine Alliance), the Coalition for Epidemic Preparedness Innovations, and the WHO aim to guarantee fair and equitable access to COVID-19 vaccines to every country in the world. In addition, WHO calls to promote technology transfer to low- and middle-income countries with the potential capacity to accelerate global production of COVID-19 vaccines.[36]
-
The fast evolution and transmission of SARS-CoV-2 has generated several particular mutations across geographic regions. The continuous appearance of new SARS-CoV-2 variants and strains with a longer-term potential for immune escape from natural or vaccinal immunity raises important concerns on the threshold of the vaccinated population required to gain collective immunity, and on the efficacy of the vaccines against novel SARS-CoV-2 variants.[16] [37] [38] The S-protein, which is considered as the optimal target for vaccine and drug development, is highly glycosylated and polymorphic and relatively tolerant to the mutation process of viruses. Actually, mutation in the S-protein is a central way for the virus to adapt to its host and gain new functions such as escape to immune response, infectivity, and transfer to new species.[39] Several SARS-CoV-2 “variants of concern” have been described that warranted special scrutiny. These include the United Kingdom (UK) variant (B.1.1.7), South Africa variant (B.1.351), Brazilian variants (P.1 and P.2), California variants (B.1.429/CAL.20C and B.1.427/CAL.20C), and the Indian variant (B.1.617).[40] [41] These variants were designated as “concerning” predominantly due to their reported enhanced person-to-person transmission in some geographic areas, and they have since been detected in several countries worldwide.[42] [43] [44] A novel SARS-CoV-2 variant derived from clade 19B (HMN.19B variant or Henri Mondor variant) has been recently identified and is actually circulating in France.[45] Whether HMN.19B will be less susceptible to protection by natural, therapeutic, or vaccine-induced immune responses remains to be determined. Some SARS-CoV-2 variants such as the Danish[46] one disappear rapidly, whereas others, like the most recent Indian strain, represent a real threat due to the high transmission rate. Thus, there is a real challenge for the continuous development of effective vaccines or monoclonal antibodies with broadly protective activities.[47] [48] [49]
Today the indian variant—also called δ-variant is dominant and seems to be responsible for the forthcoming 4th epidemic wave. It is not surprising, but rather concerning, that SARS-CoV-2 variants with variable degrees of resistance to some of the vaccines emerged.[50] [51] The need for a second and even third generation of vaccines, which overcome the resistance of the new variants, has already been acknowledged by the scientific community.[52] The discussion on the design of clinical trials, the procedure for validation, and production of new vaccines and even vaccine mixtures has already started.[53] It seems that this will follow the paradigm of flu vaccines where a continuous development of vaccines against new strains is the rule for the future.
A global and extensive vaccine strategy in all the countries is thus mandatory to limit as much as possible the consequences of a boomerang-like pandemic with limited countries vaccinated, but not really protected against emerging variants in the numerous not yet vaccinated countries or communities. The efficacy of that program is based on a rapid and global deployment of a vaccine shield under the WHO hospices.
-
The legal frames of intellectual property limit the major projects for production of COVID-19 vaccines to less than 10 pharmaceutical companies and corporations worldwide and render the vaccines more expensive and still rare. The risk of seeing the emergence of vaccine black markets should not be neglected. Surprisingly, the infrastructure and the production capacity of the pharmaceutical industry in the EU and other countries in Asia, Africa, and Latin America remain largely unused. If the actual status quo about intellectual property protection prevails, human health and social and economic stability of the nations will be definitively linked to the business plans of the pharmaceutical companies. This is at the very least a nonproductive liaison.
In that exceptional world situation, a real rupture with the traditional management of individual intellectual property is needed in the service of the general and common interest of humanity. In France, a legal procedure called “licence d'office” exists and it would allow the country to produce high amounts of patented vaccines in case of a sanitary emergency, as is currently the case.
-
Some rare cases of unusual, severe thrombotic events (i.e., cerebral venous sinus thrombosis or splanchnic vein thrombosis) and moderate to severe thrombocytopenia, strong increase of D-dimer or disseminated intravascular coagulation, have been reported in citizens who received the AstraZeneca vaccine[54] [55] and Johnson & Johnson vaccine[56] [57] and have caused a great deal of concern within the population and the medical community. This type of vaccine-induced immune thrombotic thrombocytopenia (VITT), also called thrombosis with thrombocytopenia syndrome, implies an immunological reaction that mimics heparin-induced thrombocytopenia (HIT) or catastrophic antiphospholipid syndrome.[58] The incidence of VITT has been estimated to be approximately 1 per 100,000 doses.[59] High levels of heparin-platelet-factor 4 (PF4) antibodies were identified in patients with VITT. These antibodies activate platelets monocytes and polymorphonuclear leukocytes and induce thrombocytopenia and thrombosis with a mechanism similar to that seen in HIT.[55] [60] Positive PF4/polyanion enzyme immunoassays can occur after SARS-CoV-2 vaccination with both mRNA- and adenoviral vector-based vaccines, but the majority of these antibodies likely have minor (if any) clinical relevance.[60] Scientific societies and experts on thrombosis stress the value of continuing vaccination programs to protect citizens against severe COVID-19 and to slow viral circulation, particularly of the variants. The diagnostic and therapeutic algorithms available today decrease the probability of serious complications or fatal outcomes of VITT.[61] [62] Some rare cases of classical venous thromboembolism (VTE) have been observed in citizens who received the mRNA-based vaccines.[63] Hence, the benefit of vaccination is clearly higher than any risk. Despite systematic pharmacological thromboprophylaxis in patients hospitalized with COVID-19 at the conventional ward or ICU, the incidence of thrombosis ranges from 7–8% to 25–30% respectively.[64] [65] [66] In Western countries, the actual mortality rate in patients with COVID-19 admitted to the ICUs is up to 30%, whereas the morbidity of long COVID-19 complications is not negligible.[67] [68] Nevertheless, this situation might negatively affect the psychological adherence of the population at the vaccination program and raise some concerns leading to enhanced pharmacovigilance. Vaccine hesitancy threatens to reverse the progress made in the massive vaccination program.
-
To improve the efficacy of the vaccination process, combined vaccination approaches using two types of vaccines instead of one type of vaccine are currently being considered. Such approaches may provide broader spectral protection against COVID-19 variants. Additional benefits may include improved long-term safety outcomes in the use of these agents compared with one type of vaccine. A few small clinical trials are currently in progress to demonstrate the effect of combination approaches; however, there is a need for preclinical trials to understand the mechanisms involved for the control of viral infection along with the efficacy and safety outcomes.[69]
Think Globally and Act Locally
There is an increasing consensus among experts that globally SARS-CoV-2 is likely to remain endemic in the medium term even when many parts of the world reach collective immunity.[70] In addition, the limitations of the “Stop and Go” strategy, the prolonged duration of the pandemic, the devastating consequences on public health (including the non-COVID-19-related morbidity and mortality), social adherence and the shrinkage of global economy impose the elaboration of a balanced and integrated strategy for the management of the pandemic. This new strategy includes mitigation measures, collective immunity, and targeted medical interventions for prompt, home-based medical care of patients at high risk for COVID-19 disease worsening, aiming the prevention of SARS-CoV-2 infection and the severe morbidity of patients with COVID-19. Furthermore, this strategy is expected to release the pressure on hospitals during the epidemic waves.
Profiles of Populations at Risk
The majority of the infected population is asymptomatic or develops the mild and moderate nonsevere and nonspecific form of COVID-19. About 15% of infected patients develop severe COVID-19 that requires hospitalization in a conventional ward and 5% of patients suffer a critical disease and require ICU admission.[71] It is well established that clinical worsening of patients with COVID-19 is induced by the cytokine storm related with exacerbated inflammatory response, blood hypercoagulability, and activation of endothelial cells, which start after the 5th day of the disease.[72] [73] Microvascular thrombosis in the lungs and other organs and pulmonary embolism (PE) are major causes of morbidity and mortality in patients with severe or critical COVID-19.[74] Thrombosis is a leading cause of mortality in patients with COVID-19. Indeed, the mortality increases by more than two times in patients with COVID-19 who present VTE as compared with those without VTE.[64] [75] Noteworthy, approximately 38% of patients with COVID-19 who died at home had VTE and in 12% PE was the cause of death, showing that the risk of thrombosis is mainly determined by SARS-CoV-2 infection and COVID-19 severity.[76] [77] Meta-analysis including more than 40,000 patients with COVID-19 showed that although with routine administration of the recommended pharmacological thromboprophylaxis the rate of symptomatic, objectively documented VTE was 7% in those hospitalized in conventional ward and 28% in those admitted to the ICU.[64] [75]
Consequently, a rationalized strategy aiming at early identification of patients with COVID-19 at high risk of worsening and the prompt offer of medical care, including antithrombotic treatment, is expected to contribute to the improvement of the clinical outcomes and hopefully could decrease hospital congestion. Nevertheless, this method needs to be coupled with prompt quarantine for up to at least 10 days and contact tracing to control virus spread. This approach, beyond the evident benefit of public health, could lead to a lessening of the pressure on hospitals.
The profile of patients at risk of severe or critical COVID-19 has been well described. Male gender is associated with the risk of disease worsening. The risk is further amplified by the combined vascular comorbidities present in older people. About 65% of patients with critical COVID-19 hospitalized in the ICU and 40% of patients with severe COVID-19 hospitalized in a conventional hospital ward have pre-existing vascular disease (personal history of arteriopathy or arterial thrombosis, patients with history of ischemic stroke, carotid artery disease, coronary artery disease or acute myocardial infraction, peripheral artery disease, or arterial thrombosis of rare localization, patients with history of deep vein thrombosis, PE, or vein thrombosis of rare localization [i.e., cerebral vein thrombosis, splanchnic vein thrombosis, upper limb thrombosis] or present with cardiovascular risk factors [hypertension, diabetes, or obesity]). Patients with COVID-19 and dementia, congestive heart failure, atrial fibrillation or chronic obstructive pulmonary disease, liver or renal disease, or some forms of immunosuppression are at high risk of disease worsening or death. VTE risk assessment models such as the IMPROVE-DD VTE model have undergone extensive external validation in hospitalized COVID-19 patients and have shown good discrimination to identify high-risk patients.[78] Cancer patients, particularly those with metastatic solid cancer with COVID-19, show about twofold higher mortality.[79] [80] [81] [82] [83] [84] On the other hand, well-controlled blood pressure and glucose levels in citizens with arterial hypertension or type 2 diabetes mellitus respectively are associated with markedly lower mortality as compared with individuals with poorer control of these parameters during hospitalization for COVID-19.[85] There are many disparities in the risk and outcomes from COVID-19. Old age, men, living in more deprived areas—mostly urban, Black, Asian, and Minority Ethnic groups with more inequalities—and comorbidities are at higher risk for mortality.[86]
Clinical and biological risk assessment models for COVID-19 disease worsening, though not perfect yet, are continually improving. Furthermore, electronic health (e-Health) technologies and artificial intelligence/machine-learning tools will help in early diagnosis, better precision, and personalized therapeutic approaches for COVID-19 patients.[87] [88]
Introduction of “mobile apps” in the daily life of citizens may improve their education on early recognition of COVID-19 symptoms and facilitate prompt diagnosis of SARS-CoV-2 infection, warrant the connection with the primary health care center and the treating physicians for safer and effective follow-up of the patients and early identification of those who are at high risk for disease worsening. The e-Health technologies will allow the offer of high-quality health care to populations who otherwise were restricted from accessing it before, for financial or geographic reasons.[89] [90] Artificial intelligence/machine-learning-based risk assessment models show improved accuracy and clinical performance. The introduction of the appropriate biomarkers of disease worsening, treatment efficacy, etc. will allow personalized and optimized therapeutic strategies (i.e., adaptation of the doses and duration of the antithrombotic treatment according to the phase and severity of COVID-19).[89] [91] [92] These technological tools will contribute to gather valuable data for both the users themselves and health care providers and policy makers, who can use these data on a more aggregated level to assess the local or regional health status and (expected) pressure on the health care system.[93] [94] [95]
Spatial and Social Dimensions of SARS-CoV-2 Pandemic and Risk of COVID-19 Worsening
COVID-19, as all pandemics, has a spatial dimension that has to be managed. The burden of the COVID-19 crisis varies considerably not only across countries, but also across regions and municipalities within urban agglomerations. Areas with higher population density, environmental degradation, air pollution, poverty, and social inequalities have been hit harder by the pandemic.[96] [97] [98] [99] Optimal temperature and humidity may also favor virus dissemination. On the other hand, rural areas and smaller islands are prone to be poorly equipped with fewer hospital beds and less health care workers as compared with metropolitan areas. Even though commonly the virus first took hold in urban areas, over the past few months some countries experienced the health effect spreading toward low-density areas. For example, in the United States, the highest augmentation in the number of deaths occurring in October 2020 was in rural counties not neighboring a metropolitan area. Spatial analysis is needed to determine clusters of the hardest-hit areas and to recognize the associations with circumstantial factors of vulnerability, like minority ethnic groups or low-income areas.[100] Spatial modeling has been a significant factor of the epidemiological toolkit guiding public health and government policy responses, and maps and charts that compare places have become key media for intensifying understanding of the pandemic.[101] Better information on such vulnerable groups and a more accurate picture of the parts of the population with the poorest health outcomes is important. Greater attention may offer a better selection for risk stratification, more adequately limiting the consequences of this outbreak. Being closer and more contextualized in our approach will allow for a localized and dedicated management of these preventive strategies involving a concentric manner with all of the health providers and not only the public hospitals.
Prevention, Detection, Anticipation
It is mandatory that national governments and the EU Commission explore all possible ideas and strategies to fulfill the difficult task of protecting the life and health of their citizens. There is an urgent need for a new, balanced, and integrated strategy for the management of the COVID-19 outbreak organized on the following three axes—Prevention, Detection, and Anticipation (PDA):
-
Prevention of the SARS-CoV-2 infection.
-
Detection and early diagnosis of patients at risk of disease worsening.
-
Anticipation of medical care.
The PDA, as a global strategy, is complementary to individual “barrier measures” and aims to improve patients' care at home, to decrease hospital congestion and to prevent new severe lockdowns. The principles of the PDA strategy are organized for offering an equilibrated way to improve the quality of life and limit all the pandemic side-effects.
The PDA strategy, is articulated as follows:
Prevention: A master plan for the prevention of SARS-CoV-2 infection, mitigation of virus spread, and development of collective immunity on global level (needs to be urgently launched and implemented by the WHO and the national governments; [Fig. 1]).
-
Accelerated massive vaccination, epidemiological surveillance, and tracing of contact cases are prerequisites for effective and long-lasting control of the pandemic and the decrease of the likelihood of the appearance of more virulent viral strains.[102] Indeed, vaccines and tests accessible to all countries at affordable costs are of paramount importance both for ethical and practical reasons. Today, the functions of public health systems and social and economic stability are linked to profit-based decisions regarding vaccines; diagnostic methods and therapies depend on the business plans of less than 10 pharmaceutical companies and a few states. China, Russia, India, and Western states, as major state players in the management of the pandemic, need to fully cooperate in terms of truly understanding the epidemiology of the pandemic and its management. Pharmaceutical companies and consortiums having a pivotal role in the development of vaccines, diagnostic tests, and treatments for COVID-19 need to cooperate and diffuse technological knowhow for massive production of the tools required for the control of the pandemic. According to the WHO and the World Trade Organization, there is an urgent need for “global solidarity and unhindered global sharing of technology and knowhow.”[103] [104] The recent recommendations of the Council for Trade-Related Aspects of Intellectual Property Rights of the World Trade Organization should be taken into consideration,[105] without blind limitations of the Trade Related Aspects of the Intellectual Property Rights Agreement especially in the light of a devastating pandemic. Unconditioned technology transfers should be eased so that the production and supply of COVID-19 medical goods, including vaccines and tests, will be boosted and more global access to them will be available. In the same line, the elaboration of an enlarged industrial action plan coordinated by the WHO is required for the development and production of the second-generation vaccines, free of patent restrictions.
-
Improvement of sanitary conditions and setup of primary health care structures dedicated for COVID-19, particularly in environmentally and socially sensitive urban zones, and also in areas where access to medical services is challenging. Analysis of the data from the epidemic waves of SARS-CoV-2 allows identification of the regions accumulating risk factors for enhanced viral spread and/or severe COVID-19 evolution. This information will allow a rationalized spatial territorial distribution of primary health care structures dedicated to patients with COVID-19. Registration, at the community level, of the citizens exposed at high risk for virus infection or being at high risk of disease worsening if infected with SARS-CoV-2 will improve the efficacy of targeted actions for the control of the pandemic. A local patient pathway with all identified health actors and relays proposed to offer a closer and more adapted strategy for on-site patient management and personalized care is needed. It is time to set up a Global and Personalized Strategy (COVID-19 GPS network) considering all the dimensions of patient frailty facing this pandemic (physical, psychological, social, professional, cultural, economic).
-
Harmonization of awareness gaps: While the COVID-19 pandemic has a catastrophic impact on public health and the economy globally, there remains an awareness gap among public sectors or there is a denial or lack of acceptance of the severe nature of this disease, which is more evident in younger people. Therefore, generation-based gaps and uniform acceptance of the guidelines and the urgent need of vaccination are crucial in the control of this pandemic. Digitization approaches using social media such as Twitter, Instagram, and others may be helpful in facilitating this approach. Notably the generation-based gaps, especially for the younger groups, can be planned by having advocacy platforms led by identified representatives of these groups with opinion impacts. Public personalities including politicians, movie stars and other artists, religious leaders, sports personalities, and other persons of public impact may contribute in defined programs to narrow the awareness gap and promote the development of global guidelines. Some such initiatives are already in place and have shown an impact in narrowing the awareness gaps in recognition of the severity of the COVID-19 pandemic.[106]

Detection of the dynamics of the virus circulation and detection of patients with COVID-19 and prompt identification of those at risk of disease worsening are acknowledged as necessary steps for the offer of effective medical care ([Fig. 2]).

-
Monitoring and epidemiological surveillance with wastewater-based survey network, polymerase chain reaction, and rapid screening tests for SARS-CoV-2 infection are now available free of charge to many countries to identify citizens with asymptomatic or early stages of infection and to reduce the spreading of the virus.
-
Intensive tracking needs to be developed for each patient diagnosed with infection in the workplace, schools, and locally, when there are outbreaks. It is necessary to develop an epidemiological surveillance network at regional and national levels involving virus tracing in the wastewaters (for the countries which are still missing it) to continuously and validly assess the course of the pandemic. To that respect it is important to underline that wastewater survey for SARS-CoV-2 is now considered as an essential tool to evaluate virus dissemination, notably in situations where massive testing is not possible. Very recently, the EU recommended each of its members to develop a wastewater-based survey network. Such a survey has to be implemented in a slightly different form in developing countries as well, notably when massive individual testing is not possible. Furthermore, appropriate bio-banking facilities for new SARS-CoV-2 strains and global observatories of population levels of protective immunity are prerequisites for the early detection of potential dangerous situations. In addition, e-applications are of help for continuous tracking. Importantly, tracking needs to be coupled with the rapid detection of positive cases and early patients' isolation. Therefore, quarantine conditions should be carefully examined—notably for people with low incomes—since they are a condition for an efficient acceptance. The problem of the implementation of digital tracking and population compliance are also major keys of their epidemiological interest.
-
Educational programs must be elaborated (1) for citizens with risk factors or underlying diseases with increased risk of COVID-19 worsening, aiming for their training on the application of physical and social distancing measures, early recognition of COVID-19 symptoms, and communication with the medical staff at least by telemedicine and (2) for physicians, particularly general practitioners and family doctors, aiming for their training on early recognition of the risk of COVID-19 worsening in their patient list and the implementation of the recommendations for COVID-19 prompt diagnosis and ambulatory management. Patients with vascular disease or cardiovascular risk factors as well as patients with cancer, who represent a rather large portion of the adult population in the community, should be under regular medical follow-up for the improvement of the adherence to the antihypertensive treatment (including angiotensin-converting enzyme inhibitors or angiotensin receptor blockers), antithrombotic (antiplatelets or anticoagulant) treatment, lipid lowering treatment (i.e., statins), and the antihyperglycemic medications according to the recommendations of the relevant consensus statements and scientific societies. It is important to renew all of these prescriptions for avoiding any rupture and omission in these vulnerable patients.
Anticipation of medical treatment in patients with COVID-19 is essential for improved clinical outcome ([Fig. 3]).[107]

-
Early diagnosis of COVID-19 with a simple and feasible methodology at the level of the primary health care structures is of major importance for prompt medical care. A regional procedure for prioritized hospitalization of patients at high risk or with early signs for disease worsening should be considered by health authorities since it is expected to improve the clinical outcomes.
-
Home-based medical care of patients with COVID-19: Within the first 5 to 7 days after SARS-CoV-2 infection the symptoms of CVOID-19 are related principally with the viral load. Afterwards, the clinical evolution is determined by host reaction (cytokine storm, hypercoagulability, endothelial cell activation), which is amplified in patients at risk for disease worsening.[108] [109] Home based-medical care for patients at risk for disease worsening aims at prompt administration of therapeutic agents targeting the viral load (those which are available and recommended today and those which will be available in the future), the prevention and treatment of COVID-19 complications, the treatment of underlying diseases, the prevention of secondary infections, and the support of organ function in time.
-
Early treatment administration at out-patient receiving home-based medical care is recommended today for the initial phase of COVID-19 (i.e., monoclonal antibodies against SARS-CoV-2, or other antiviral treatments available and approved by health authorities) and pharmacological thromboprophylaxis in patients at high risk for VTE or disease worsening. General, nonspecific therapies such as strengthened supportive treatment, vitamin-D administration, adequate energy intake, evaluation of water and electrolyte balance, and effective oxygen therapy measures are also important to be administered promptly by the general practitioner and home-based medical care staff.[110] [111]
Early administration of antithrombotic agents such as low-molecular-weight heparin (LMWH), direct orally active factor Xa inhibitors (apixaban, rivaroxaban), or sulodexide to patients at risk of disease worsening reduces the risk of hospitalization, need for oxygen support, or even mortality.[112] [113] [114] [115] [116] [117] Nevertheless, particularly for LMWHs, the optimal dose needs to be thoroughly evaluated.[118] The organization of the necessary framework for home-based medical care will be of major importance for the optimal administration of the forthcoming specific antiviral treatments which are currently under investigation or clinical development.[119]
-
Personalized therapeutic strategy and prompt identification of patients who need prioritized hospitalization based on regular clinical follow-up of the patients (i.e., by performing the recommended blood tests and applying the available risk assessment tools) will contribute to the improvement of the clinical outcome.[120]
-
Long-COVID syndrome is currently observed in patients who recovered from the acute disease. It has now been documented that one third of the COVID-19 patients suffer from varying degrees of behavioral and mental disorders with a wide range of symptoms.[121] [122] Additionally, the behavioral impact of COVID-19 in the general public is well documented. This includes depression, anxiety, and behavioral disorders requiring professional interventions.[123] The severity of these problems ranges widely with complex manifestations. Psychological programs for citizens are another approach to implement defined programs and solidarity networks to manage these issues.[124] The aggravation and prolongation of such a frail situation is leading to many other diseases (treatment omissions and diagnosis delays) and family fractures (violence, divorce, separation) as indirect consequences of this pandemic which has turned every facet of life upside down. Posthospital discharge VTE may also be considered and prevented.
-
Homogenization of therapeutic protocols: The COVID-19 pandemic has pressurized the medical community to make medical decisions and recommendations based on limited anecdotal, observational, and, in some cases, a complete absence of evidence.[125] [126] Individual medical institutions have created their own institutional algorithms, presumably based on local individual expertise and consensus, as well as interim professional society and governmental recommendations.[127] The ongoing clinical trials on antithrombotics and other treatments for patients with COVID-19 will offer guidelines supported by a high level of evidence. Nevertheless, the harmonization of diagnostic and therapeutic protocols principally at the levels of the primary health care structures needs to start and to be implemented rapidly.
Conclusions
The SARS-CoV-2 pandemic enters into a new phase which is characterized by the following:
-
Knowledge on the characteristics of variants of SARS-CoV-2, their pathophysiology, and clinical courses of COVID-19.
-
Availability of high-quality diagnostic rapid screening tests for SARS-CoV-2 tests which allow accurate epidemiological surveillance and tracing of contact cases with an affordable cost, which will allow effective mitigation of the pandemic.
-
Availability of vaccines is a fundamental element for accelerated development of worldwide collective immunity.
-
Description and identification of population groups which are at higher risk of COVID-19 infection and vulnerable to develop severe COVID-19 or a worsening disease.
-
Development and availability of validated risk assessment models which together with the clinical experience gained by physicians allow the earlier identification of patients at risk of disease worsening. This methodology is expected to be optimized in the forthcoming period and will offer its more systematic application.
-
Development of therapeutic strategies and treatment guidance which include antiviral agents (i.e., monoclonal antibodies or other drugs) antithrombotic and anti-inflammatory agents, vitamins which may improve the clinical course of the patients with COVID-19 if they are administered as early as possible after symptom declaration, and diagnosis of the disease.
-
Development of e-Health tools and artificial intelligence-based methodology can improve the benefit of the mitigation policies by decreasing the financial and social costs of the severe NPIs and allows for prompt and personalized medicine in patients with COVID-19.
-
Acquisition of a collective experience by the medical community, the citizens, and the policy makers in the management of the pandemic will allow the adaptation of the strategies according to local customs and cultural characteristics of the populations.
The PDA strategy offers to policy makers the possibility for a rapid elaboration of concrete integrated and equitable program for the management of the next phases of the pandemic to preserve the health of peoples and the social cohesion.
This Document is Endorsed by
-
VAS-European Independent Foundation in Angiology/Vascular Medicine
-
International Union of Angiology
-
Lebanese Society of Hematology and Blood Transfusion (LSHBT)
-
Lebanese Joint Coalition Against Thrombosis (LJCAT)
-
Serbian Lymphoma Group
-
Global Thrombosis Forum (GTF)
-
Balkan Thrombosis Forum
-
European Venous Forum
-
Asociación para el Estudio de la Medicina Vascular en España (ASEMEVE)
-
Russian Academy of Sciences
-
Cyprus Medical Association
-
Chinese Academy of Medical Sciences
-
Moroccan Society of Vascular Diseases.
Conflict of Interest
None declared.
Acknowledgments
The working group thankfully acknowledges the endorsement of various organizations for this publication. We are also thankful to all of the contributors for their input in developing this document. A special thanks to Ms. Erin Healy-Erickson for her skillful assistance in preparing this communication. The authors are thankful to Yorgos Konstantinou (imagistan.com) for designing the visuals.
* Scientific Reviewer Committee Members: Gregory Y. H. Lip, Michael Makris, Sam Schulman, Wolfgang Siess, Christian Weber
-
References
- 1 https://solidarites-sante.gouv.fr/IMG/pdf/avis_conseil_scientifique_6_mai_2021.pdf andhttps://www.lemonde.fr/podcasts/article/2021/06/30/le-variant-delta-peut-il-declencher-une-quatrieme-vague_6086296_5463015.html
- 2 Challen R, Brooks-Pollock E, Read JM, Dyson L, Tsaneva-Atanasova K, Danon L. Risk of mortality in patients infected with SARS-CoV-2 variant of concern 202012/1: matched cohort study. BMJ 2021; 372 (579) n579
- 3 Garcia-Beltran WF, Lam EC, St Denis K. et al. Multiple SARS-CoV-2 variants escape neutralization by vaccine-induced humoral immunity. Cell 2021; 184 (09) 2372-2383.e9
- 4 Paul P, France AM, Aoki Y. et al. Genomic Surveillance for SARS-CoV-2 variants circulating in the united states, December 2020-May 2021. MMWR Morb Mortal Wkly Rep 2021; 70 (23) 846-850
- 5 Johanna N, Citrawijaya H, Wangge G. Mass screening vs lockdown vs combination of both to control COVID-19: a systematic review. J Public Health Res 2020; 9 (04) 2011
- 6 Riccardo F, Ajelli M, Andrianou XD. et al; COVID-19 working group. Epidemiological characteristics of COVID-19 cases and estimates of the reproductive numbers 1 month into the epidemic, Italy, 28 January to 31 March 2020. Euro Surveill 2020; 25 (49) 2000790
- 7 Carrat F, Touvier M, Severi G. et al; SAPRIS study group. Incidence and risk factors of COVID-19-like symptoms in the French general population during the lockdown period: a multi-cohort study. BMC Infect Dis 2021; 21 (01) 169
- 8 Gaudart J, Landier J, Huiart L. et al. Factors associated with the spatial heterogeneity of the first wave of COVID-19 in France: a nationwide geo-epidemiological study. Lancet 2021; 6 (04) E222-E231
- 9 Timelli L, Girardi E. Effect of timing of implementation of containment measures on Covid-19 epidemic. The case of the first wave in Italy. PLoS One 2021; 16 (01) e0245656
- 10 Denford S, Morton KS, Lambert H. et al. Understanding patterns of adherence to COVID-19 mitigation measures: a qualitative interview study. J Public Health 2021;
- 11 Raude J, Lecrique JM, Lasbeur L. et al. Determinants of preventive behaviors in response to the COVID-19 pandemic in France: comparing the sociocultural, psychosocial, and social cognitive explanations. Front Psychol 2020; 11: 584500
- 12 https://univ-droit.fr/actualites-de-la-recherche/appels/34809-covid-19-constitutional-political-and-social-threats-and-challenges-in-france-and-the-united-kingdom Accessed June 27, 2021
- 13
SciencePo..
OSC papers. Accessed June 27, 2021 at: https://spire.sciencespo.fr/hdl:/2441/6vv2fug6nb8t29ilm995n9hbnh/resources/op-2020-1.pdf
- 14 Contreras S, Dehning J, Loidolt M. et al. The challenges of containing SARS-CoV-2 via test-trace-and-isolate. Nat Commun 2021; 12 (01) 378
- 15 Bendavid E, Oh C, Bhattacharya J, Ioannidis JPA. Assessing mandatory stay-at-home and business closure effects on the spread of COVID-19. Eur J Clin Invest 2021; 51 (04) e13484
- 16 Atlani-Duault L, Chauvin F, Yazdanpanah Y. et al. France's COVID-19 response: balancing conflicting public health traditions. Lancet 2020; 396 (10246) 219-221
- 17 Milman O, Yelin I, Aharony N. et al. Community-level evidence for SARS-CoV-2 vaccine protection of unvaccinated individuals. Nat Med 2021;
- 18
European Commission..
Commission sets out key actions for a united front to beat COVID-19. Accessed June
27, 2021 at: https://ec.europa.eu/commission/presscorner/detail/en/IP_21_143
- 19 Lazarus JV, Ratzan SC, Palayew A. et al. A global survey of potential acceptance of a COVID-19 vaccine. Nat Med 2021; 27 (02) 225-228
- 20 Brandt EJ, Rosenberg J, Waselewski ME. et al. National study of youth opinions on vaccination for COVID-19 in the U.S. J Adolesc Health 2021; 68 (05) 869-872
- 21 Schmelz K, Bowles S. Overcoming COVID-19 vaccination resistance when alternative policies affect the dynamics of conformism, social norms, and crowding out. Proc Natl Acad Sci U S A 2021; 118 (25) e2104912118
- 22
Gavi..
COVID-19 vaccines in development. Accessed June 27, 2021 at: https://www.gavi.org/sites/default/files/covid/covid-19-vaccines-development-phases.png
- 23 Kim JH, Marks F, Clemens JD. Looking beyond COVID-19 vaccine phase 3 trials. Nat Med 2021; 27 (02) 205-211
- 24 Baden LR, El Sahly HM, Essink B. et al; COVE Study Group. Efficacy and safety of the mRNA-1273 SARS-CoV-2 vaccine. N Engl J Med 2021; 384 (05) 403-416
- 25 Polack FP, Thomas SJ, Kitchin N. et al; C4591001 Clinical Trial Group. Safety and efficacy of the BNT162b2 mRNA Covid-19 vaccine. N Engl J Med 2020; 383 (27) 2603-2615
- 26 Logunov DY, Dolzhikova IV, Shcheblyakov DV. et al. Safety and efficacy of an rAd26 and rAd5 vector-based heterologous prime-boost COVID-19 vaccine: an interim analysis of a randomised controlled phase 3 trial in Russia. Lancet 2021; 397 (10275): 671-681
- 27 Angelis A, Baltussen R, Tervonen T. The need for novel approaches in assessing the value of COVID-19 vaccines. Am J Public Health 2021; 111 (02) 205-208
- 28
Oxfam..
Small group of rich nations have bought up more than half the future supply of leading
COVID-19 vaccine contenders. Accessed June 27, 2021 at: https://www.oxfam.org/fr/node/14233
- 29
UN News..
Low-income countries have received just 0.2 per cent of all COVID-19 shots given.
Accessed June 27, 2021 at: https://news.un.org/en/story/2021/04/1089392
- 30
Our World in Data..
Coronavirus (COVID-19) vaccinations. Accessed June 27, 2021 at: https://ourworldindata.org/covid-vaccinations
- 31 Emanuel EJ, Luna F, Schaefer GO, Tan KC, Wolff J. Enhancing the WHO's proposed framework for distributing COVID-19 vaccines among countries. Am J Public Health 2021; 111 (03) 371-373
- 32
WHO..
Statement on the fifth meeting of the International Health Regulations (2005) Emergency
Committee regarding the coronavirus disease (COVID-19) pandemic. Accessed June 27,
2021 at: https://www.who.int/news/item/30-10-2020-statement-on-the-fifth-meeting-of-the-international-health-regulations-(2005)-emergency-committee-regarding-the-coronavirus-disease-(covid-19)-pandemic
- 33
Foreign Policy..
Vaccine nationalism harms everyone and protects no one. Accessed June 27, 2021 at:
https://foreignpolicy.com/2021/02/02/vaccine-nationalism-harms-everyone-and-protects-no-one/
- 34
Statista..
Impact of the coronavirus pandemic on the global economy - statistics & facts. Accessed
June 27, 2021 at: https://www.statista.com/topics/6139/covid-19-impact-on-the-global-economy/
- 35
ICC..
Study shows vaccine nationalism could cost rich countries US$4.5 trillion. Accessed
June 27, 2021 at: https://iccwbo.org/media-wall/news-speeches/study-shows-vaccine-nationalism-could-cost-rich-countries-us4-5-trillion/
- 36
WHO..
Statement on the sixth meeting of the International Health Regulations (2005) Emergency
Committee regarding the coronavirus disease (COVID-19) pandemic. Accessed June 27,
2021 at: https://www.who.int/news/item/15-01-2021-statement-on-the-sixth-meeting-of-the-international-health-regulations-(2005)-emergency-committee-regarding-the-coronavirus-disease-(covid-19)-pandemic
- 37 Callaway E. Fast-spreading COVID variant can elude immune responses. Nature 2021; 589 (7843): 500-501
- 38 Callaway E. The coronavirus is mutating - does it matter?. Nature 2020; 585 (7824): 174-177
- 39 Hacisuleyman E, Hale C, Saito Y. et al. Vaccine breakthrough infections with SARS-CoV-2 variants. N Engl J Med 2021; 384 (23) 2212-2218
- 40 Long SW, Olsen RJ, Christensen PA. et al. Sequence analysis of 20,453 severe acute respiratory syndrome coronavirus 2 genomes from the Houston Metropolitan area identifies the emergence and widespread distribution of multiple isolates of all major variants of concern. Am J Pathol 2021; 191 (06) 983-992
- 41
Outbreak.info..
Accessed June 27, 2021 at: https://outbreak.info/situation-reports
- 42 Huang SW, Wang SF. SARS-CoV-2 entry related viral and host genetic variations: implications on COVID-19 severity, immune escape, and infectivity. Int J Mol Sci 2021; 22 (06) 3060
- 43 Gómez CE, Perdiguero B, Esteban M. Emerging SARS-CoV-2 variants and impact in global vaccination programs against SARS-CoV-2/COVID-19. Vaccines (Basel) 2021; 9 (03) 243
- 44 Fergie J, Srivastava A. Immunity to SARS-CoV-2: lessons learned. Front Immunol 2021; 12: 654165
- 45 Fourati S, Decousser JW, Khouider S. et al. Novel SARS-CoV-2 variant derived from Clade 19B, France. Emerg Infect Dis 2021; 27 (05) 1540-1543
- 46
WHO..
SARS-CoV-2 mink-associated variant strain – Denmark. Accessed June 27, 2021 at:
https://www.who.int/csr/don/06-november-2020-mink-associated-sars-cov2-denmark/en/
- 47 Walls AC, Park YJ, Tortorici MA, Wall A, McGuire AT, Veesler D. Structure, function, and antigenicity of the SARS-CoV-2 spike glycoprotein. Cell 2020; 181 (02) 281.e6-292.e6
- 48 Shu Y, McCauley J. GISAID: Global initiative on sharing all influenza data - from vision to reality. Euro Surveill 2017; 22 (13) 30494
- 49 Shajahan A, Supekar NT, Gleinich AS, Azadi P. Deducing the N- and O-glycosylation profile of the spike protein of novel coronavirus SARS-CoV-2. Glycobiology 2020; 30 (12) 981-988
- 50 Collier DA, De Marco A, Ferreira IATM. et al; CITIID-NIHR BioResource COVID-19 Collaboration; COVID-19 Genomics UK (COG-UK) Consortium. Sensitivity of SARS-CoV-2 B.1.1.7 to mRNA vaccine-elicited antibodies. Nature 2021; 593 (7857): 136-141
- 51 Madhi SA, Baillie V, Cutland CL. et al; NGS-SA Group; Wits-VIDA COVID Group. Efficacy of the ChAdOx1 nCoV-19 Covid-19 vaccine against the B.1.351 variant. N Engl J Med 2021; 384 (20) 1885-1898
- 52 Steuwer B, Jamrozik E, Eyal N. Prioritizing second-generation SARS-CoV-2 vaccines through low-dosage challenge studies. Int J Infect Dis 2021; 105: 307-311
- 53 Callaway E, Ledford H. How to redesign COVID vaccines so they protect against variants. Nature 2021; 590 (7844): 15-16
- 54
EMA.
COVID-19 Vaccine AstraZeneca: benefits still outweigh the risks despite possible link
to rare blood clots with low blood platelets. Accessed June 27, 2021 at: https://www.ema.europa.eu/en/news/covid-19-vaccine-astrazeneca-benefits-still-outweigh-risks-despite-possible-link-rare-blood-clots
- 55 Greinacher A, Thiele T, Warkentin TE, Weisser K, Kyrle PA, Eichinger S. Thrombotic thrombocytopenia after ChAdOx1 nCov-19 vaccination. N Engl J Med 2021; 384 (22) 2092-2101
- 56
CDC..
Joint CDC and FDA statement on Johnson & Johnson COVID-19 vaccine. Accessed June
27, 2021 at: https://www.cdc.gov/media/releases/2021/s0413-JJ-vaccine.html
- 57
EMA..
COVID-19 Vaccine Janssen: EMA finds possible link to very rare cases of unusual blood
clots with low blood platelets. Accessed June 27, 2021 at: https://www.ema.europa.eu/en/news/covid-19-vaccine-janssen-ema-finds-possible-link-very-rare-cases-unusual-blood-clots-low-blood
- 58 Schultz NH, Sørvoll IH, Michelsen AE. et al. Thrombosis and thrombocytopenia after ChAdOx1 nCoV-19 vaccination. N Engl J Med 2021; 384 (22) 2124-2130
- 59 Pottegård A, Lund LC, Karlstad Ø. et al. Arterial events, venous thromboembolism, thrombocytopenia, and bleeding after vaccination with Oxford-AstraZeneca ChAdOx1-S in Denmark and Norway: population based cohort study. BMJ 2021; 373 (1114): n1114
- 60 Thiele T, Ulm L, Holtfreter S. et al. Frequency of positive anti-PF4/polyanion antibody tests after COVID-19 vaccination with ChAdOx1 nCoV-19 and BNT162b2. Blood 2021;
- 61
ISTH..
ISTH interim guidance for the diagnosis and treatment on vaccine-induced immune thrombotic
thrombocytopenia (updated 20 April, 2021). Accessed June 27, 2021 at: https://cdn.ymaws.com/www.isth.org/resource/resmgr/ISTH_VITT_Guidance_2.pdf
- 62 Elalamy I, Gerotziafas G, Alamowitch S. et al. SARS-CoV-2 vaccine and thrombosis: expert opinions. Thromb Haemost 2021;
- 63 Carli G, Nichele I, Ruggeri M, Barra S, Tosetto A. Deep vein thrombosis (DVT) occurring shortly after the second dose of mRNA SARS-CoV-2 vaccine. Intern Emerg Med 2021; 16 (03) 803-804
- 64 Jiménez D, García-Sanchez A, Rali P. et al. Incidence of VTE and bleeding among hospitalized patients with coronavirus disease 2019: a systematic review and meta-analysis. Chest 2021; 159 (03) 1182-1196
- 65 Nopp S, Moik F, Jilma B, Pabinger I, Ay C. Risk of venous thromboembolism in patients with COVID-19: a systematic review and meta-analysis. Res Pract Thromb Haemost 2020; 4 (07) 1178-1191
- 66 Roubinian NH, Dusendang JR, Mark DG. et al. Incidence of 30-day venous thromboembolism in adults tested for SARS-CoV-2 infection in an integrated health care system in Northern California. JAMA Intern Med 2021; 181 (07) 997-1000
- 67 Grasselli G, Greco M, Zanella A. et al; COVID-19 Lombardy ICU Network. Risk factors associated with mortality among patients with COVID-19 in intensive care units in Lombardy, Italy. JAMA Intern Med 2020; 180 (10) 1345-1355
- 68
NICE..
COVID-19 rapid guideline: managing the long-term effects of COVID-19. NICE guideline
[NG188]. https://www.nice.org.uk/GUIDANCE/ng188 Accessed June 27, 2021
- 69 Ledford H. Could mixing COVID vaccines boost immune response?. Nature 2021; 590 (7846): 375-376
- 70 Phillips N. The coronavirus is here to stay - here's what that means. Nature 2021; 590 (7846): 382-384
- 71
World Health Organization.
Clinical management of severe acute respiratory infection (SARI) when COVID-19 disease
is suspected. Interim guidance 13 March 2020. Accessed June 27, 2021 at: https://www.who.int/publications-detail/clinical-management-of-severe-acute-respiratory-infection-when-novel-coronavirus-(ncov)-infection-is-suspected
- 72 Chauhan AJ, Wiffen LJ, Brown TP. COVID-19: A collision of complement, coagulation and inflammatory pathways. J Thromb Haemost 2020; 18 (09) 2110-2117
- 73 Terpos E, Ntanasis-Stathopoulos I, Elalamy I. et al. Hematological findings and complications of COVID-19. Am J Hematol 2020; 95 (07) 834-847
- 74 Menter T, Haslbauer JD, Nienhold R. et al. Postmortem examination of COVID-19 patients reveals diffuse alveolar damage with severe capillary congestion and variegated findings in lungs and other organs suggesting vascular dysfunction. Histopathology 2020; 77 (02) 198-209
- 75 Malas MB, Naazie IN, Elsayed N, Mathlouthi A, Marmor R, Clary B. Thromboembolism risk of COVID-19 is high and associated with a higher risk of mortality: a systematic review and meta-analysis. EClinicalMedicine 2020; 29: 100639
- 76 Edler C, Schröder AS, Aepfelbacher M. et al. Dying with SARS-CoV-2 infection-an autopsy study of the first consecutive 80 cases in Hamburg, Germany. Int J Legal Med 2020; 134 (04) 1275-1284
- 77 Calabrese F, Pezzuto F, Fortarezza F. et al. Pulmonary pathology and COVID-19: lessons from autopsy. The experience of European Pulmonary Pathologists. Virchows Arch 2020; 477 (03) 359-372
- 78 Spyropoulos AC, Cohen SL, Gianos E. et al; COVID‒19 Consortium Group. Validation of the IMPROVE-DD risk assessment model for venous thromboembolism among hospitalized patients with COVID-19. Res Pract Thromb Haemost 2021; 5 (02) 296-300
- 79 Gerotziafas GT, Catalano M, Colgan MP. et al; Scientific Reviewer Committee. Guidance for the management of patients with vascular disease or cardiovascular risk factors and COVID-19: position paper from VAS-European Independent Foundation in Angiology/Vascular Medicine. Thromb Haemost 2020; 120 (12) 1597-1628
- 80 Harrison SL, Fazio-Eynullayeva E, Lane DA, Underhill P, Lip GYH. Higher mortality of ischaemic stroke patients hospitalized with COVID-19 compared to historical controls. Cerebrovasc Dis 2021; 50 (03) 326-331
- 81 Vaughan CJ, Cronin H, Ryan PM, Caplice NM. Obesity and COVID-19: A Virchow's triad for the 21st century. Thromb Haemost 2020; 120 (11) 1590-1593
- 82 Gerotziafas GT, Sergentanis TN, Voiriot G. et al. Derivation and validation of a predictive score for disease worsening in patients with COVID-19. Thromb Haemost 2020; 120 (12) 1680-1690
- 83 Ribas A, Sengupta R, Locke T. et al; AACR COVID-19 and Cancer Task Force. Priority COVID-19 vaccination for patients with cancer while vaccine supply is limited. Cancer Discov 2021; 11 (02) 233-236
- 84 Harrison SL, Fazio-Eynullayeva E, Lane DA, Underhill P, Lip GYH. Atrial fibrillation and the risk of 30-day incident thromboembolic events, and mortality in adults ≥ 50 years with COVID-19. J Arrhythm 2020; 37 (01) 231-237
- 85 Zhu L, She ZG, Cheng X. et al. Association of blood glucose control and outcomes in patients with COVID-19 and pre-existing type 2 diabetes. Cell Metab 2020; 31 (06) 1068.e3-1077.e3
- 86
GOV.UK..
COVID-19: review of disparities in risks and outcomes. Accessed June 27, 2021 at:
https://www.gov.uk/government/publications/covid-19-review-of-disparities-in-risks-and-outcomes
- 87 Quiroz JC, Feng YZ, Cheng ZY. et al. Development and validation of a machine learning approach for automated severity assessment of COVID-19 based on clinical and imaging data: retrospective study. JMIR Med Inform 2021; 9 (02) e24572
- 88 Horgan D, Hackett J, Westphalen CB. et al. Digitalisation and COVID-19: the perfect storm. Biomed Hub 2020; 5 (03) 1341-1363
- 89
European Commission..
Accessed June 27, 2021 at: https://ec.europa.eu/health/sites/default/files/expert_panel/docs/015_access_healthservices_en.pdf
- 90
WHO..
Telemedicine. Accessed June 27, 2021 at: https://www.who.int/goe/publications/goe_telemedicine_2010.pdf
- 91 Thachil J, Tang N, Gando S. et al. Laboratory haemostasis monitoring in COVID-19. J Thromb Haemost 2020; 18 (08) 2058-2060
- 92 Wang L, Yang L, Bai L, Huang Z, Peng Y. Association between D-dimer level and chest CT severity score in patients with SARS-COV-2 pneumonia. Sci Rep 2021; 11 (01) 11636
- 93 Zamberg I, Manzano S, Posfay-Barbe K, Windisch O, Agoritsas T, Schiffer E. A mobile health platform to disseminate validated institutional measurements during the COVID-19 outbreak: utilization-focused evaluation study. JMIR Public Health Surveill 2020; 6 (02) e18668
- 94 Timmers T, Janssen L, Stohr J, Murk JL, Berrevoets MAH. Using eHealth to support COVID-19 education, self-assessment, and symptom monitoring in the Netherlands: observational study. JMIR Mhealth Uhealth 2020; 8 (06) e19822
- 95
European Commission..
Accessed June 27, 2021 at: https://ec.europa.eu/health/sites/default/files/ehealth/docs/2018_provision_marketstudy_telemedicine_en.pdf
- 96 Bourdrel T, Annesi-Maesano I, Alahmad B, Maesano CN, Bind MA. The impact of outdoor air pollution on COVID-19: a review of evidence from in vitro, animal, and human studies. Eur Respir Rev 2021; 30 (159) 200242
- 97 Ahmed F, Ahmed N, Pissarides C, Stiglitz J. Why inequality could spread COVID-19. Lancet Public Health 2020; 5 (05) e240
- 98 Bilal, Bashir MF, Benghoul M. et al. Environmental pollution and COVID-19 outbreak: insights from Germany. Air Qual Atmos Health 2020;
- 99 Brosemer K, Schelly C, Gagnon V. et al. The energy crises revealed by COVID: intersections of indigeneity, inequity, and health. Energy Res Soc Sci 2020; 68: 101661
- 100 Cordes J, Castro MC. Spatial analysis of COVID-19 clusters and contextual factors in New York City. Spat Spatio-Temporal Epidemiol 2020; 34: 100355
- 101 Rose-Redwood R, Kitchin R, Apostolopoulou E. et al. Geographies of the COVID-19 pandemic. Dialogues Hum Geogr 2020; 10 (02) 97-106
- 102
WHO..
Déclaration du Mécanisme COVAX sur les nouveaux variants du SARS-CoV-2. Accessed
June 27, 2021 at: https://www.who.int/fr/news/item/08-02-2021-covax-statement-on-new-variants-of-sars-cov-2
- 103
WHO..
Global solidarity in the fight against COVID-19 takes centre stage during Regional
Director's visit to Russian Federation. Accessed June 27, 2021 at: https://www.euro.who.int/en/about-us/regional-director/news/news/2020/09/global-solidarity-in-the-fight-against-covid-19-takes-centre-stage-during-regional-directors-visit-to-russian-federation
- 104
Human Rights Watch..
Urgently waive intellectual property rules for vaccine. Accessed June 27, 2021 at:
https://www.hrw.org/news/2020/12/10/urgently-waive-intellectual-property-rules-vaccine
- 105
World Trade Organization..
Waiver from certain provisions of the trips agreement for the prevention, containment
and treatment of COVID-19. Accessed June 27, 2021 at: https://docs.wto.org/dol2fe/Pages/SS/directdoc.aspx?filename=q:/IP/C/W669.pdf&Open=True
- 106
European Commission..
Improving pandemic preparedness and management. Accessed June 27, 2021 at: https://ec.europa.eu/info/sites/default/files/jointopinion_improvingpandemicpreparednessandmanagement_nov2020_0.pdf
- 107 Wang G, Luo FM, Liu D. et al; Sichuan & Wuhan Collaboration Research Group, and Sichuan Treatment Expert Group for COVID-19, China. Differences in the clinical characteristics and outcomes of COVID-19 patients in the epicenter and peripheral areas of the pandemic from China: a retrospective, large-sample, comparative analysis. BMC Infect Dis 2021; 21 (01) 206
- 108 Bordallo B, Bellas M, Cortez AF, Vieira M, Pinheiro M. Severe COVID-19: what have we learned with the immunopathogenesis?. Adv Rheumatol 2020; 60 (01) 50
- 109 Gencer S, Lacy M, Atzler D, van der Vorst EPC, Döring Y, Weber C. Immunoinflammatory, thrombohaemostatic, and cardiovascular mechanisms in COVID-19. Thromb Haemost 2020; 120 (12) 1629-1641
- 110 Levy E, Delvin E, Marcil V, Spahis S. Can phytotherapy with polyphenols serve as a powerful approach for the prevention and therapy tool of novel coronavirus disease 2019 (COVID-19)?. Am J Physiol Endocrinol Metab 2020; 319 (04) E689-E708
- 111 Lordan R. Notable developments for vitamin D amid the COVID-19 pandemic, but caution warranted overall: a narrative review. Nutrients 2021; 13 (03) 740
- 112 Drago F, Gozzo L, Li L, Stella A, Cosmi B. Use of enoxaparin to counteract COVID-19 infection and reduce thromboembolic venous complications: a review of the current evidence. Front Pharmacol 2020; 11: 579886
- 113 Billett HH, Reyes-Gil M, Szymanski J. et al. Anticoagulation in COVID-19: effect of enoxaparin, heparin, and apixaban on mortality. Thromb Haemost 2020; 120 (12) 1691-1699
- 114 D'Amato G, Acanfora L, Delli Paoli L, D'Amato M. Preventive home therapy for symptomatic patients affected by COVID-19 and followed by teleconsultations. Multidiscip Respir Med 2021; 16 (01) 748
- 115 Capell WH, Barnathan ES, Piazza G. et al. Rationale and design for the study of rivaroxaban to reduce thrombotic events, hospitalization and death in outpatients with COVID-19: The PREVENT-HD study. Am Heart J 2021; 235: 12-23
- 116 Gonzalez-Ochoa AJ, Raffetto JD, Hernández AG. et al. Sulodexide in the treatment of patients with early stages of COVID-19: a randomized controlled trial. Thromb Haemost 2021; 121 (07) 944-954
- 117 Schulman S, Harenberg J. Anticoagulant treatment of COVID-19 as early as possible – sulodexide and perspectives. Thromb Haemost 2021; 121 (07) 849-853
- 118 Patell R, Chiasakul T, Bauer E, Zwicker JI. Pharmacologic thromboprophylaxis and thrombosis in hospitalized patients with COVID-19: a pooled analysis. Thromb Haemost 2021; 121 (01) 76-85
- 119 Bikdeli B, Madhavan MV, Gupta A. et al; Global COVID-19 Thrombosis Collaborative Group. Pharmacological agents targeting thromboinflammation in COVID-19: review and implications for future research. Thromb Haemost 2020; 120 (07) 1004-1024
- 120 Dalekos GN, Stefos A, Georgiadou S. et al. Lessons from pathophysiology: use of individualized combination treatments with immune interventional agents to tackle severe respiratory failure in patients with COVID-19. Eur J Intern Med 2021; 88: 52-62
- 121 Naidu SB, Shah AJ, Saigal A. et al. The high mental health burden of “Long COVID” and its association with on-going physical and respiratory symptoms in all adults discharged from hospital. Eur Respir J 2021; 2004364: 2004364
- 122 Huang C, Huang L, Wang Y. et al. 6-month consequences of COVID-19 in patients discharged from hospital: a cohort study. Lancet 2021; 397 (10270): 220-232
- 123 Al-Aly Z, Xie Y, Bowe B. High-dimensional characterization of post-acute sequelae of COVID-19. Nature 2021; 594 (7862): 259-264
- 124 Vink M, Vink-Niese A. Could cognitive behavioural therapy be an effective treatment for long COVID and post COVID-19 fatigue syndrome? Lessons from the Qure study for Q-fever fatigue syndrome. Healthcare (Basel) 2020; 8 (04) 552
- 125
National Institutes of Health..
Coronavirus disease 2019 (COVID-19) treatment guidelines. Accessed May 17, 2020 at:
https://www.covid19treatmentguidelines.nih.gov/
- 126 Patell R, Midha S, Kimani S. et al. Variability in institutional guidance for COVID-19-associated coagulopathy in the United States. Thromb Haemost 2020; 120 (12) 1725-1732
- 127 Cohoon KP, Mahé G, Tafur AJ, Spyropoulos AC. Emergence of institutional antithrombotic protocols for coronavirus 2019. Res Pract Thromb Haemost 2020; 4 (04) 510-517
{kind=link}
Address for correspondence
Publication History
Received: 04 May 2021
Accepted: 17 June 2021
Accepted Manuscript online:
24 June 2021
Article published online:
20 July 2021
© 2021. The Author(s). This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/)
Georg Thieme Verlag KG
Rüdigerstraße 14, 70469 Stuttgart, Germany
-
References
- 1 https://solidarites-sante.gouv.fr/IMG/pdf/avis_conseil_scientifique_6_mai_2021.pdf andhttps://www.lemonde.fr/podcasts/article/2021/06/30/le-variant-delta-peut-il-declencher-une-quatrieme-vague_6086296_5463015.html
- 2 Challen R, Brooks-Pollock E, Read JM, Dyson L, Tsaneva-Atanasova K, Danon L. Risk of mortality in patients infected with SARS-CoV-2 variant of concern 202012/1: matched cohort study. BMJ 2021; 372 (579) n579
- 3 Garcia-Beltran WF, Lam EC, St Denis K. et al. Multiple SARS-CoV-2 variants escape neutralization by vaccine-induced humoral immunity. Cell 2021; 184 (09) 2372-2383.e9
- 4 Paul P, France AM, Aoki Y. et al. Genomic Surveillance for SARS-CoV-2 variants circulating in the united states, December 2020-May 2021. MMWR Morb Mortal Wkly Rep 2021; 70 (23) 846-850
- 5 Johanna N, Citrawijaya H, Wangge G. Mass screening vs lockdown vs combination of both to control COVID-19: a systematic review. J Public Health Res 2020; 9 (04) 2011
- 6 Riccardo F, Ajelli M, Andrianou XD. et al; COVID-19 working group. Epidemiological characteristics of COVID-19 cases and estimates of the reproductive numbers 1 month into the epidemic, Italy, 28 January to 31 March 2020. Euro Surveill 2020; 25 (49) 2000790
- 7 Carrat F, Touvier M, Severi G. et al; SAPRIS study group. Incidence and risk factors of COVID-19-like symptoms in the French general population during the lockdown period: a multi-cohort study. BMC Infect Dis 2021; 21 (01) 169
- 8 Gaudart J, Landier J, Huiart L. et al. Factors associated with the spatial heterogeneity of the first wave of COVID-19 in France: a nationwide geo-epidemiological study. Lancet 2021; 6 (04) E222-E231
- 9 Timelli L, Girardi E. Effect of timing of implementation of containment measures on Covid-19 epidemic. The case of the first wave in Italy. PLoS One 2021; 16 (01) e0245656
- 10 Denford S, Morton KS, Lambert H. et al. Understanding patterns of adherence to COVID-19 mitigation measures: a qualitative interview study. J Public Health 2021;
- 11 Raude J, Lecrique JM, Lasbeur L. et al. Determinants of preventive behaviors in response to the COVID-19 pandemic in France: comparing the sociocultural, psychosocial, and social cognitive explanations. Front Psychol 2020; 11: 584500
- 12 https://univ-droit.fr/actualites-de-la-recherche/appels/34809-covid-19-constitutional-political-and-social-threats-and-challenges-in-france-and-the-united-kingdom Accessed June 27, 2021
- 13
SciencePo..
OSC papers. Accessed June 27, 2021 at: https://spire.sciencespo.fr/hdl:/2441/6vv2fug6nb8t29ilm995n9hbnh/resources/op-2020-1.pdf
- 14 Contreras S, Dehning J, Loidolt M. et al. The challenges of containing SARS-CoV-2 via test-trace-and-isolate. Nat Commun 2021; 12 (01) 378
- 15 Bendavid E, Oh C, Bhattacharya J, Ioannidis JPA. Assessing mandatory stay-at-home and business closure effects on the spread of COVID-19. Eur J Clin Invest 2021; 51 (04) e13484
- 16 Atlani-Duault L, Chauvin F, Yazdanpanah Y. et al. France's COVID-19 response: balancing conflicting public health traditions. Lancet 2020; 396 (10246) 219-221
- 17 Milman O, Yelin I, Aharony N. et al. Community-level evidence for SARS-CoV-2 vaccine protection of unvaccinated individuals. Nat Med 2021;
- 18
European Commission..
Commission sets out key actions for a united front to beat COVID-19. Accessed June
27, 2021 at: https://ec.europa.eu/commission/presscorner/detail/en/IP_21_143
- 19 Lazarus JV, Ratzan SC, Palayew A. et al. A global survey of potential acceptance of a COVID-19 vaccine. Nat Med 2021; 27 (02) 225-228
- 20 Brandt EJ, Rosenberg J, Waselewski ME. et al. National study of youth opinions on vaccination for COVID-19 in the U.S. J Adolesc Health 2021; 68 (05) 869-872
- 21 Schmelz K, Bowles S. Overcoming COVID-19 vaccination resistance when alternative policies affect the dynamics of conformism, social norms, and crowding out. Proc Natl Acad Sci U S A 2021; 118 (25) e2104912118
- 22
Gavi..
COVID-19 vaccines in development. Accessed June 27, 2021 at: https://www.gavi.org/sites/default/files/covid/covid-19-vaccines-development-phases.png
- 23 Kim JH, Marks F, Clemens JD. Looking beyond COVID-19 vaccine phase 3 trials. Nat Med 2021; 27 (02) 205-211
- 24 Baden LR, El Sahly HM, Essink B. et al; COVE Study Group. Efficacy and safety of the mRNA-1273 SARS-CoV-2 vaccine. N Engl J Med 2021; 384 (05) 403-416
- 25 Polack FP, Thomas SJ, Kitchin N. et al; C4591001 Clinical Trial Group. Safety and efficacy of the BNT162b2 mRNA Covid-19 vaccine. N Engl J Med 2020; 383 (27) 2603-2615
- 26 Logunov DY, Dolzhikova IV, Shcheblyakov DV. et al. Safety and efficacy of an rAd26 and rAd5 vector-based heterologous prime-boost COVID-19 vaccine: an interim analysis of a randomised controlled phase 3 trial in Russia. Lancet 2021; 397 (10275): 671-681
- 27 Angelis A, Baltussen R, Tervonen T. The need for novel approaches in assessing the value of COVID-19 vaccines. Am J Public Health 2021; 111 (02) 205-208
- 28
Oxfam..
Small group of rich nations have bought up more than half the future supply of leading
COVID-19 vaccine contenders. Accessed June 27, 2021 at: https://www.oxfam.org/fr/node/14233
- 29
UN News..
Low-income countries have received just 0.2 per cent of all COVID-19 shots given.
Accessed June 27, 2021 at: https://news.un.org/en/story/2021/04/1089392
- 30
Our World in Data..
Coronavirus (COVID-19) vaccinations. Accessed June 27, 2021 at: https://ourworldindata.org/covid-vaccinations
- 31 Emanuel EJ, Luna F, Schaefer GO, Tan KC, Wolff J. Enhancing the WHO's proposed framework for distributing COVID-19 vaccines among countries. Am J Public Health 2021; 111 (03) 371-373
- 32
WHO..
Statement on the fifth meeting of the International Health Regulations (2005) Emergency
Committee regarding the coronavirus disease (COVID-19) pandemic. Accessed June 27,
2021 at: https://www.who.int/news/item/30-10-2020-statement-on-the-fifth-meeting-of-the-international-health-regulations-(2005)-emergency-committee-regarding-the-coronavirus-disease-(covid-19)-pandemic
- 33
Foreign Policy..
Vaccine nationalism harms everyone and protects no one. Accessed June 27, 2021 at:
https://foreignpolicy.com/2021/02/02/vaccine-nationalism-harms-everyone-and-protects-no-one/
- 34
Statista..
Impact of the coronavirus pandemic on the global economy - statistics & facts. Accessed
June 27, 2021 at: https://www.statista.com/topics/6139/covid-19-impact-on-the-global-economy/
- 35
ICC..
Study shows vaccine nationalism could cost rich countries US$4.5 trillion. Accessed
June 27, 2021 at: https://iccwbo.org/media-wall/news-speeches/study-shows-vaccine-nationalism-could-cost-rich-countries-us4-5-trillion/
- 36
WHO..
Statement on the sixth meeting of the International Health Regulations (2005) Emergency
Committee regarding the coronavirus disease (COVID-19) pandemic. Accessed June 27,
2021 at: https://www.who.int/news/item/15-01-2021-statement-on-the-sixth-meeting-of-the-international-health-regulations-(2005)-emergency-committee-regarding-the-coronavirus-disease-(covid-19)-pandemic
- 37 Callaway E. Fast-spreading COVID variant can elude immune responses. Nature 2021; 589 (7843): 500-501
- 38 Callaway E. The coronavirus is mutating - does it matter?. Nature 2020; 585 (7824): 174-177
- 39 Hacisuleyman E, Hale C, Saito Y. et al. Vaccine breakthrough infections with SARS-CoV-2 variants. N Engl J Med 2021; 384 (23) 2212-2218
- 40 Long SW, Olsen RJ, Christensen PA. et al. Sequence analysis of 20,453 severe acute respiratory syndrome coronavirus 2 genomes from the Houston Metropolitan area identifies the emergence and widespread distribution of multiple isolates of all major variants of concern. Am J Pathol 2021; 191 (06) 983-992
- 41
Outbreak.info..
Accessed June 27, 2021 at: https://outbreak.info/situation-reports
- 42 Huang SW, Wang SF. SARS-CoV-2 entry related viral and host genetic variations: implications on COVID-19 severity, immune escape, and infectivity. Int J Mol Sci 2021; 22 (06) 3060
- 43 Gómez CE, Perdiguero B, Esteban M. Emerging SARS-CoV-2 variants and impact in global vaccination programs against SARS-CoV-2/COVID-19. Vaccines (Basel) 2021; 9 (03) 243
- 44 Fergie J, Srivastava A. Immunity to SARS-CoV-2: lessons learned. Front Immunol 2021; 12: 654165
- 45 Fourati S, Decousser JW, Khouider S. et al. Novel SARS-CoV-2 variant derived from Clade 19B, France. Emerg Infect Dis 2021; 27 (05) 1540-1543
- 46
WHO..
SARS-CoV-2 mink-associated variant strain – Denmark. Accessed June 27, 2021 at:
https://www.who.int/csr/don/06-november-2020-mink-associated-sars-cov2-denmark/en/
- 47 Walls AC, Park YJ, Tortorici MA, Wall A, McGuire AT, Veesler D. Structure, function, and antigenicity of the SARS-CoV-2 spike glycoprotein. Cell 2020; 181 (02) 281.e6-292.e6
- 48 Shu Y, McCauley J. GISAID: Global initiative on sharing all influenza data - from vision to reality. Euro Surveill 2017; 22 (13) 30494
- 49 Shajahan A, Supekar NT, Gleinich AS, Azadi P. Deducing the N- and O-glycosylation profile of the spike protein of novel coronavirus SARS-CoV-2. Glycobiology 2020; 30 (12) 981-988
- 50 Collier DA, De Marco A, Ferreira IATM. et al; CITIID-NIHR BioResource COVID-19 Collaboration; COVID-19 Genomics UK (COG-UK) Consortium. Sensitivity of SARS-CoV-2 B.1.1.7 to mRNA vaccine-elicited antibodies. Nature 2021; 593 (7857): 136-141
- 51 Madhi SA, Baillie V, Cutland CL. et al; NGS-SA Group; Wits-VIDA COVID Group. Efficacy of the ChAdOx1 nCoV-19 Covid-19 vaccine against the B.1.351 variant. N Engl J Med 2021; 384 (20) 1885-1898
- 52 Steuwer B, Jamrozik E, Eyal N. Prioritizing second-generation SARS-CoV-2 vaccines through low-dosage challenge studies. Int J Infect Dis 2021; 105: 307-311
- 53 Callaway E, Ledford H. How to redesign COVID vaccines so they protect against variants. Nature 2021; 590 (7844): 15-16
- 54
EMA.
COVID-19 Vaccine AstraZeneca: benefits still outweigh the risks despite possible link
to rare blood clots with low blood platelets. Accessed June 27, 2021 at: https://www.ema.europa.eu/en/news/covid-19-vaccine-astrazeneca-benefits-still-outweigh-risks-despite-possible-link-rare-blood-clots
- 55 Greinacher A, Thiele T, Warkentin TE, Weisser K, Kyrle PA, Eichinger S. Thrombotic thrombocytopenia after ChAdOx1 nCov-19 vaccination. N Engl J Med 2021; 384 (22) 2092-2101
- 56
CDC..
Joint CDC and FDA statement on Johnson & Johnson COVID-19 vaccine. Accessed June
27, 2021 at: https://www.cdc.gov/media/releases/2021/s0413-JJ-vaccine.html
- 57
EMA..
COVID-19 Vaccine Janssen: EMA finds possible link to very rare cases of unusual blood
clots with low blood platelets. Accessed June 27, 2021 at: https://www.ema.europa.eu/en/news/covid-19-vaccine-janssen-ema-finds-possible-link-very-rare-cases-unusual-blood-clots-low-blood
- 58 Schultz NH, Sørvoll IH, Michelsen AE. et al. Thrombosis and thrombocytopenia after ChAdOx1 nCoV-19 vaccination. N Engl J Med 2021; 384 (22) 2124-2130
- 59 Pottegård A, Lund LC, Karlstad Ø. et al. Arterial events, venous thromboembolism, thrombocytopenia, and bleeding after vaccination with Oxford-AstraZeneca ChAdOx1-S in Denmark and Norway: population based cohort study. BMJ 2021; 373 (1114): n1114
- 60 Thiele T, Ulm L, Holtfreter S. et al. Frequency of positive anti-PF4/polyanion antibody tests after COVID-19 vaccination with ChAdOx1 nCoV-19 and BNT162b2. Blood 2021;
- 61
ISTH..
ISTH interim guidance for the diagnosis and treatment on vaccine-induced immune thrombotic
thrombocytopenia (updated 20 April, 2021). Accessed June 27, 2021 at: https://cdn.ymaws.com/www.isth.org/resource/resmgr/ISTH_VITT_Guidance_2.pdf
- 62 Elalamy I, Gerotziafas G, Alamowitch S. et al. SARS-CoV-2 vaccine and thrombosis: expert opinions. Thromb Haemost 2021;
- 63 Carli G, Nichele I, Ruggeri M, Barra S, Tosetto A. Deep vein thrombosis (DVT) occurring shortly after the second dose of mRNA SARS-CoV-2 vaccine. Intern Emerg Med 2021; 16 (03) 803-804
- 64 Jiménez D, García-Sanchez A, Rali P. et al. Incidence of VTE and bleeding among hospitalized patients with coronavirus disease 2019: a systematic review and meta-analysis. Chest 2021; 159 (03) 1182-1196
- 65 Nopp S, Moik F, Jilma B, Pabinger I, Ay C. Risk of venous thromboembolism in patients with COVID-19: a systematic review and meta-analysis. Res Pract Thromb Haemost 2020; 4 (07) 1178-1191
- 66 Roubinian NH, Dusendang JR, Mark DG. et al. Incidence of 30-day venous thromboembolism in adults tested for SARS-CoV-2 infection in an integrated health care system in Northern California. JAMA Intern Med 2021; 181 (07) 997-1000
- 67 Grasselli G, Greco M, Zanella A. et al; COVID-19 Lombardy ICU Network. Risk factors associated with mortality among patients with COVID-19 in intensive care units in Lombardy, Italy. JAMA Intern Med 2020; 180 (10) 1345-1355
- 68
NICE..
COVID-19 rapid guideline: managing the long-term effects of COVID-19. NICE guideline
[NG188]. https://www.nice.org.uk/GUIDANCE/ng188 Accessed June 27, 2021
- 69 Ledford H. Could mixing COVID vaccines boost immune response?. Nature 2021; 590 (7846): 375-376
- 70 Phillips N. The coronavirus is here to stay - here's what that means. Nature 2021; 590 (7846): 382-384
- 71
World Health Organization.
Clinical management of severe acute respiratory infection (SARI) when COVID-19 disease
is suspected. Interim guidance 13 March 2020. Accessed June 27, 2021 at: https://www.who.int/publications-detail/clinical-management-of-severe-acute-respiratory-infection-when-novel-coronavirus-(ncov)-infection-is-suspected
- 72 Chauhan AJ, Wiffen LJ, Brown TP. COVID-19: A collision of complement, coagulation and inflammatory pathways. J Thromb Haemost 2020; 18 (09) 2110-2117
- 73 Terpos E, Ntanasis-Stathopoulos I, Elalamy I. et al. Hematological findings and complications of COVID-19. Am J Hematol 2020; 95 (07) 834-847
- 74 Menter T, Haslbauer JD, Nienhold R. et al. Postmortem examination of COVID-19 patients reveals diffuse alveolar damage with severe capillary congestion and variegated findings in lungs and other organs suggesting vascular dysfunction. Histopathology 2020; 77 (02) 198-209
- 75 Malas MB, Naazie IN, Elsayed N, Mathlouthi A, Marmor R, Clary B. Thromboembolism risk of COVID-19 is high and associated with a higher risk of mortality: a systematic review and meta-analysis. EClinicalMedicine 2020; 29: 100639
- 76 Edler C, Schröder AS, Aepfelbacher M. et al. Dying with SARS-CoV-2 infection-an autopsy study of the first consecutive 80 cases in Hamburg, Germany. Int J Legal Med 2020; 134 (04) 1275-1284
- 77 Calabrese F, Pezzuto F, Fortarezza F. et al. Pulmonary pathology and COVID-19: lessons from autopsy. The experience of European Pulmonary Pathologists. Virchows Arch 2020; 477 (03) 359-372
- 78 Spyropoulos AC, Cohen SL, Gianos E. et al; COVID‒19 Consortium Group. Validation of the IMPROVE-DD risk assessment model for venous thromboembolism among hospitalized patients with COVID-19. Res Pract Thromb Haemost 2021; 5 (02) 296-300
- 79 Gerotziafas GT, Catalano M, Colgan MP. et al; Scientific Reviewer Committee. Guidance for the management of patients with vascular disease or cardiovascular risk factors and COVID-19: position paper from VAS-European Independent Foundation in Angiology/Vascular Medicine. Thromb Haemost 2020; 120 (12) 1597-1628
- 80 Harrison SL, Fazio-Eynullayeva E, Lane DA, Underhill P, Lip GYH. Higher mortality of ischaemic stroke patients hospitalized with COVID-19 compared to historical controls. Cerebrovasc Dis 2021; 50 (03) 326-331
- 81 Vaughan CJ, Cronin H, Ryan PM, Caplice NM. Obesity and COVID-19: A Virchow's triad for the 21st century. Thromb Haemost 2020; 120 (11) 1590-1593
- 82 Gerotziafas GT, Sergentanis TN, Voiriot G. et al. Derivation and validation of a predictive score for disease worsening in patients with COVID-19. Thromb Haemost 2020; 120 (12) 1680-1690
- 83 Ribas A, Sengupta R, Locke T. et al; AACR COVID-19 and Cancer Task Force. Priority COVID-19 vaccination for patients with cancer while vaccine supply is limited. Cancer Discov 2021; 11 (02) 233-236
- 84 Harrison SL, Fazio-Eynullayeva E, Lane DA, Underhill P, Lip GYH. Atrial fibrillation and the risk of 30-day incident thromboembolic events, and mortality in adults ≥ 50 years with COVID-19. J Arrhythm 2020; 37 (01) 231-237
- 85 Zhu L, She ZG, Cheng X. et al. Association of blood glucose control and outcomes in patients with COVID-19 and pre-existing type 2 diabetes. Cell Metab 2020; 31 (06) 1068.e3-1077.e3
- 86
GOV.UK..
COVID-19: review of disparities in risks and outcomes. Accessed June 27, 2021 at:
https://www.gov.uk/government/publications/covid-19-review-of-disparities-in-risks-and-outcomes
- 87 Quiroz JC, Feng YZ, Cheng ZY. et al. Development and validation of a machine learning approach for automated severity assessment of COVID-19 based on clinical and imaging data: retrospective study. JMIR Med Inform 2021; 9 (02) e24572
- 88 Horgan D, Hackett J, Westphalen CB. et al. Digitalisation and COVID-19: the perfect storm. Biomed Hub 2020; 5 (03) 1341-1363
- 89
European Commission..
Accessed June 27, 2021 at: https://ec.europa.eu/health/sites/default/files/expert_panel/docs/015_access_healthservices_en.pdf
- 90
WHO..
Telemedicine. Accessed June 27, 2021 at: https://www.who.int/goe/publications/goe_telemedicine_2010.pdf
- 91 Thachil J, Tang N, Gando S. et al. Laboratory haemostasis monitoring in COVID-19. J Thromb Haemost 2020; 18 (08) 2058-2060
- 92 Wang L, Yang L, Bai L, Huang Z, Peng Y. Association between D-dimer level and chest CT severity score in patients with SARS-COV-2 pneumonia. Sci Rep 2021; 11 (01) 11636
- 93 Zamberg I, Manzano S, Posfay-Barbe K, Windisch O, Agoritsas T, Schiffer E. A mobile health platform to disseminate validated institutional measurements during the COVID-19 outbreak: utilization-focused evaluation study. JMIR Public Health Surveill 2020; 6 (02) e18668
- 94 Timmers T, Janssen L, Stohr J, Murk JL, Berrevoets MAH. Using eHealth to support COVID-19 education, self-assessment, and symptom monitoring in the Netherlands: observational study. JMIR Mhealth Uhealth 2020; 8 (06) e19822
- 95
European Commission..
Accessed June 27, 2021 at: https://ec.europa.eu/health/sites/default/files/ehealth/docs/2018_provision_marketstudy_telemedicine_en.pdf
- 96 Bourdrel T, Annesi-Maesano I, Alahmad B, Maesano CN, Bind MA. The impact of outdoor air pollution on COVID-19: a review of evidence from in vitro, animal, and human studies. Eur Respir Rev 2021; 30 (159) 200242
- 97 Ahmed F, Ahmed N, Pissarides C, Stiglitz J. Why inequality could spread COVID-19. Lancet Public Health 2020; 5 (05) e240
- 98 Bilal, Bashir MF, Benghoul M. et al. Environmental pollution and COVID-19 outbreak: insights from Germany. Air Qual Atmos Health 2020;
- 99 Brosemer K, Schelly C, Gagnon V. et al. The energy crises revealed by COVID: intersections of indigeneity, inequity, and health. Energy Res Soc Sci 2020; 68: 101661
- 100 Cordes J, Castro MC. Spatial analysis of COVID-19 clusters and contextual factors in New York City. Spat Spatio-Temporal Epidemiol 2020; 34: 100355
- 101 Rose-Redwood R, Kitchin R, Apostolopoulou E. et al. Geographies of the COVID-19 pandemic. Dialogues Hum Geogr 2020; 10 (02) 97-106
- 102
WHO..
Déclaration du Mécanisme COVAX sur les nouveaux variants du SARS-CoV-2. Accessed
June 27, 2021 at: https://www.who.int/fr/news/item/08-02-2021-covax-statement-on-new-variants-of-sars-cov-2
- 103
WHO..
Global solidarity in the fight against COVID-19 takes centre stage during Regional
Director's visit to Russian Federation. Accessed June 27, 2021 at: https://www.euro.who.int/en/about-us/regional-director/news/news/2020/09/global-solidarity-in-the-fight-against-covid-19-takes-centre-stage-during-regional-directors-visit-to-russian-federation
- 104
Human Rights Watch..
Urgently waive intellectual property rules for vaccine. Accessed June 27, 2021 at:
https://www.hrw.org/news/2020/12/10/urgently-waive-intellectual-property-rules-vaccine
- 105
World Trade Organization..
Waiver from certain provisions of the trips agreement for the prevention, containment
and treatment of COVID-19. Accessed June 27, 2021 at: https://docs.wto.org/dol2fe/Pages/SS/directdoc.aspx?filename=q:/IP/C/W669.pdf&Open=True
- 106
European Commission..
Improving pandemic preparedness and management. Accessed June 27, 2021 at: https://ec.europa.eu/info/sites/default/files/jointopinion_improvingpandemicpreparednessandmanagement_nov2020_0.pdf
- 107 Wang G, Luo FM, Liu D. et al; Sichuan & Wuhan Collaboration Research Group, and Sichuan Treatment Expert Group for COVID-19, China. Differences in the clinical characteristics and outcomes of COVID-19 patients in the epicenter and peripheral areas of the pandemic from China: a retrospective, large-sample, comparative analysis. BMC Infect Dis 2021; 21 (01) 206
- 108 Bordallo B, Bellas M, Cortez AF, Vieira M, Pinheiro M. Severe COVID-19: what have we learned with the immunopathogenesis?. Adv Rheumatol 2020; 60 (01) 50
- 109 Gencer S, Lacy M, Atzler D, van der Vorst EPC, Döring Y, Weber C. Immunoinflammatory, thrombohaemostatic, and cardiovascular mechanisms in COVID-19. Thromb Haemost 2020; 120 (12) 1629-1641
- 110 Levy E, Delvin E, Marcil V, Spahis S. Can phytotherapy with polyphenols serve as a powerful approach for the prevention and therapy tool of novel coronavirus disease 2019 (COVID-19)?. Am J Physiol Endocrinol Metab 2020; 319 (04) E689-E708
- 111 Lordan R. Notable developments for vitamin D amid the COVID-19 pandemic, but caution warranted overall: a narrative review. Nutrients 2021; 13 (03) 740
- 112 Drago F, Gozzo L, Li L, Stella A, Cosmi B. Use of enoxaparin to counteract COVID-19 infection and reduce thromboembolic venous complications: a review of the current evidence. Front Pharmacol 2020; 11: 579886
- 113 Billett HH, Reyes-Gil M, Szymanski J. et al. Anticoagulation in COVID-19: effect of enoxaparin, heparin, and apixaban on mortality. Thromb Haemost 2020; 120 (12) 1691-1699
- 114 D'Amato G, Acanfora L, Delli Paoli L, D'Amato M. Preventive home therapy for symptomatic patients affected by COVID-19 and followed by teleconsultations. Multidiscip Respir Med 2021; 16 (01) 748
- 115 Capell WH, Barnathan ES, Piazza G. et al. Rationale and design for the study of rivaroxaban to reduce thrombotic events, hospitalization and death in outpatients with COVID-19: The PREVENT-HD study. Am Heart J 2021; 235: 12-23
- 116 Gonzalez-Ochoa AJ, Raffetto JD, Hernández AG. et al. Sulodexide in the treatment of patients with early stages of COVID-19: a randomized controlled trial. Thromb Haemost 2021; 121 (07) 944-954
- 117 Schulman S, Harenberg J. Anticoagulant treatment of COVID-19 as early as possible – sulodexide and perspectives. Thromb Haemost 2021; 121 (07) 849-853
- 118 Patell R, Chiasakul T, Bauer E, Zwicker JI. Pharmacologic thromboprophylaxis and thrombosis in hospitalized patients with COVID-19: a pooled analysis. Thromb Haemost 2021; 121 (01) 76-85
- 119 Bikdeli B, Madhavan MV, Gupta A. et al; Global COVID-19 Thrombosis Collaborative Group. Pharmacological agents targeting thromboinflammation in COVID-19: review and implications for future research. Thromb Haemost 2020; 120 (07) 1004-1024
- 120 Dalekos GN, Stefos A, Georgiadou S. et al. Lessons from pathophysiology: use of individualized combination treatments with immune interventional agents to tackle severe respiratory failure in patients with COVID-19. Eur J Intern Med 2021; 88: 52-62
- 121 Naidu SB, Shah AJ, Saigal A. et al. The high mental health burden of “Long COVID” and its association with on-going physical and respiratory symptoms in all adults discharged from hospital. Eur Respir J 2021; 2004364: 2004364
- 122 Huang C, Huang L, Wang Y. et al. 6-month consequences of COVID-19 in patients discharged from hospital: a cohort study. Lancet 2021; 397 (10270): 220-232
- 123 Al-Aly Z, Xie Y, Bowe B. High-dimensional characterization of post-acute sequelae of COVID-19. Nature 2021; 594 (7862): 259-264
- 124 Vink M, Vink-Niese A. Could cognitive behavioural therapy be an effective treatment for long COVID and post COVID-19 fatigue syndrome? Lessons from the Qure study for Q-fever fatigue syndrome. Healthcare (Basel) 2020; 8 (04) 552
- 125
National Institutes of Health..
Coronavirus disease 2019 (COVID-19) treatment guidelines. Accessed May 17, 2020 at:
https://www.covid19treatmentguidelines.nih.gov/
- 126 Patell R, Midha S, Kimani S. et al. Variability in institutional guidance for COVID-19-associated coagulopathy in the United States. Thromb Haemost 2020; 120 (12) 1725-1732
- 127 Cohoon KP, Mahé G, Tafur AJ, Spyropoulos AC. Emergence of institutional antithrombotic protocols for coronavirus 2019. Res Pract Thromb Haemost 2020; 4 (04) 510-517