

Subscribe to RSS
DOI: 10.1055/a-2240-3482
In Vivo Kinematic Analysis of Mobile-Bearing Unicompartmental Knee Arthroplasty during High Flexion Activities
Authors
Abstract
Mobile-bearing (MB) unicompartmental knee arthroplasty (UKA) has high conformity between the femoral articular surface and the meniscal bearing; therefore, the surface and subsurface contact stress is reduced. Additionally, the survival rate is high. However, the in vivo kinematics of MB UKA knees during high-flexion activities of daily living remain unknown. The aim of this study was to investigate in vivo the three-dimensional kinematics of MB UKA knees during high-flexion activities of daily living. A total of 17 knees of 17 patients who could achieve kneeling after MB UKA were examined. Under fluoroscopy, each patient performed squatting and kneeling motions. To estimate the spatial position and orientation of the knee, a two-dimensional/three-dimensional registration technique was used. We evaluated the femoral rotation and varus–valgus angle relative to the tibia and the anteroposterior translation of the medial sulcus (medial side) and lateral epicondyle (lateral side) of the femur on the plane perpendicular to the tibial mechanical axis in each flexion angle. From 130° to 140° of flexion, the femoral external rotation during squatting was significantly smaller than that during kneeling. Additionally, the medial side of the femur during squatting was significantly more posteriorly located compared with that during kneeling. There was no significant difference between squatting and kneeling in terms of the lateral side of the femur and the varus–valgus position in each flexion angle. At high flexion angle, the kinematics of MB UKA knees may differ depending on the performance.
Recently, several studies have reported that patient's satisfaction with total knee arthroplasty (TKA) is not good.[1] [2] [3] However, some studies have reported that patient's satisfaction with unicompartmental knee arthroplasty (UKA) is better than that of TKA.[4] [5] This fact suggests that the preservation of the anterior cruciate ligament and the lateral compartment leads to good result. Therefore, it is important to analyze the kinematics of UKA knees to investigate the reason. Several studies have examined the kinematics of UKA knees in activities of daily living.[6] [7] [8] [9] However, there is no study that compared the kinematics of UKA knees among activities of daily living. Therefore, the presence or absence of a difference in the kinematics of UKA knees in daily activities remains unknown. Furthermore, especially in Asia, people usually bend their knees deeply in daily living such as when sitting on the floor, kneeling, yoga, and praying. Hence, patients desire for high flexion after UKA. Therefore, it is also important to clarify the kinematics of UKA knees during high-flexion activities.
Regarding fixed-bearing (FB) UKA, some studies have demonstrated that the kinematics of the knees after FB UKA replicated the kinematics of normal knees during gait or in vitro.[10] [11] [12] [13] However, Mochizuki et al[8] have reported that the kinematics of the knee after FB UKA were not the same as normal during squatting.
Mobile-bearing (MB) UKA has high conformity between the femoral articular surface and the meniscal bearing; therefore, the surface and subsurface contact stress is reduced.[14] [15] [16] [17] [18] Pandit et al[19] have reported that the 15-year survival rate of MB UKA was more than 90%. Furthermore, MB UKA knees have been suggested to be superior to FB UKA knees in their restoration of normal tibiofemoral biomechanics.[16] [20] [21] [22] Moreover, Peersman et al[14] have reported that the kinematics of unloaded MB UKA knees resemble that of normal knees in an in vitro study. However, the in vivo kinematics of MB UKA knees during high-flexion activities of daily living remain unknown.
The aim of this study was to investigate the in vivo three-dimensional (3D) kinematics of MB UKA knees during high-flexion activities of daily living. The hypothesis of this study was that the in vivo kinematics of MB UKA knees differ depending on the high-flexion activities of daily living such as squatting and kneeling.
Materials and Methods
A total of 17 knees of 17 patients who could achieve kneeling after MB UKA (Oxford partial knee; Zimmer Biomet GK, Warsaw, IN) were examined. The patients provided written informed consent to participate in the current investigation. The study has institutional review board approval, with documentation. At the time of fluoroscopic analysis, the mean duration of postoperative follow-up was 9.7 months (standard deviation [SD]: 2.8 months), the mean height was 158.0 cm (SD: 7.7 cm), and the mean body weight was 71.7 kg (SD: 7.0 kg). Of the 17 knees included in the analysis, 8 were contributed by male patients, and the other 9 were by female patients. The new Knee Society scores[23] are reported in [Table 1]. All patients had undergone MB UKA to treat medial knee joint osteoarthritis (OA) (Kellgren–Lawrence grade III). The mean hip–knee–ankle angle at the time of analysis was 5.2° (SD: 3.6°). All values were expressed as mean (SD). The radiographic component positions were evaluated according to the Knee Society TKA roentgenography evaluation ([Fig. 1]).[24] On the anteroposterior (AP) view, the femoral component was set at an angle of 96.8° (SD: 4.3°) and the tibial component was set at an angle of 86.7° (SD: 2.3°) (α and β angles, respectively). On the lateral view, the femoral component was aligned at a flexion angle of 9.3° (SD: 5.1°) and the tibial component was aligned at an angle of 84.7° (SD: 2.7°) (γ and δ angles, respectively).
Abbreviation: SD, standard deviation.

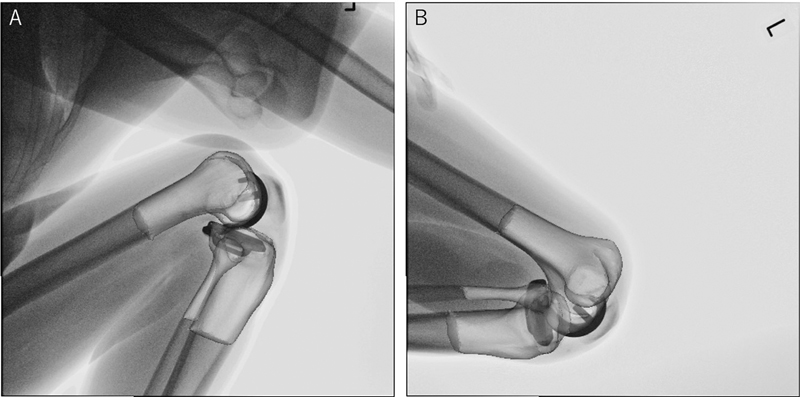
Under fluoroscopy, each patient performed squatting and kneeling motions at a natural pace ([Fig. 2], and [Video 1]). The patients practiced the motion several times before recording. The sequential motion was recorded as digital X-ray images (1,024 × 1,024 × 12 bits/pixel, 7.5-Hz serial spot images as a DICOM file) using a 17-inch (43-cm) flat panel detector system (Ultimax-i DREX-U180, Toshiba Medical Systems, Tochigi, Japan; ZEXIRA DREX-ZX80, Toshiba, Tokyo, Japan). Furthermore, all images were processed by dynamic range compression, enabling edge-enhanced images. To estimate spatial position and orientation of the knee, a 2D/3D registration technique was used.[25] [26] This technique is based on a contour-based registration algorithm using single-view fluoroscopic images and 3D computer-aided design (CAD) models. We created 3D bone models from computed tomography before surgery, which were used for CAD models ([Fig. 3]). The estimation accuracy for relative motion between 3D bone models was ≤1° in rotation and ≤1 mm in translation.[26]

Video 1 Fluoroscopic analysis. Each patient performed squatting and kneeling motions under fluoroscopy.
A local coordinate system at the bone model was produced according to a previous study.[26] [27] Knee rotations were described using the joint rotational convention of Grood and Suntay.[28] We evaluated the femoral rotation and varus–valgus angle relative to the tibia and the AP translation of the medial sulcus (medial side) and lateral epicondyle (lateral side) of the femur on the plane perpendicular to the tibial mechanical axis in each flexion angle.[26] AP translation was calculated as the percentage relative to the proximal AP dimension of the tibia.[26] External and internal rotations were denoted as positive and negative, respectively. Valgus and varus were defined as positive and negative, respectively. The positive and negative values of AP translation were defined as anterior and posterior to the axis of the tibia, respectively.
Statistical Analysis
The results were analyzed using SPSS version 25 (IBM Corp., Armonk, NY). Wilcoxon signed-rank tests were used to analyze the flexion angle between squatting and kneeling. Repeated measures analysis of variance and post-hoc pairwise comparison (Bonferroni test) were used to analyze the differences in rotation angle, varus–valgus angle, and AP translation between squatting and kneeling. A p-value <0.05 was considered statistically significant.
A power analysis indicated that 11 patients would be required using EZR[29] when α was set as 0.05 and power at 0.8.
Results
Flexion Angle
During squatting, knees were gradually flexed from 3.3° (SD: 5.2°) to 136.2° (SD: 10.7°). During kneeling, knees were gradually flexed from 102.6° (SD: 8.1°) to 145.1° (SD: 7.3°). The maximum knee flexion angle during squatting was significantly smaller than that during kneeling (p < 0.001).
Rotation Angle
During squatting, femurs displayed 12.1° (SD: 5.4°) external rotation relative to the tibia from 0° to 140° of flexion. During kneeling, femurs displayed 6.0° (SD: 5.7°) external rotation relative to the tibia from 110° to 140° of flexion. From 130° to 140° of flexion, the femoral external rotation during squatting was significantly smaller than that during kneeling (p = 0.01 respectively) ([Fig. 4]).

Varus–Valgus Angle
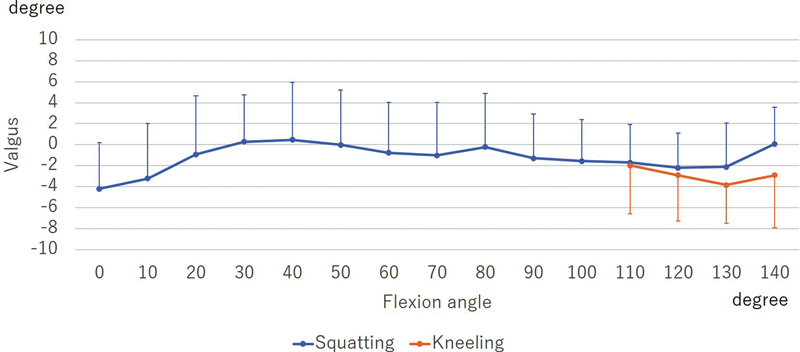
Regarding varus–valgus motion, the knees during both squatting and kneeling did not move significantly (p = 0.28 and 0.69). Additionally, there was no significant difference between squatting and kneeling in terms of the varus–valgus position in each flexion angle (p = 0.39) ([Fig. 5]).
AP Translation
During squatting, the AP translation of the medial side indicated 17.6% (SD: 12.5%) posterior movement from 0° to 140° of flexion. During kneeling, it indicated 11.2% (SD: 12.0%) posterior movement from 110° to 140° of flexion. From 130° to 140° of flexion, the medial side of the femur during squatting was significantly more posteriorly located compared with that during kneeling (130° of flexion: p < 0.001, 140° of flexion: p = 0.002) ([Fig. 6]).

AP translation of the lateral side of the femur during squatting indicated 50.0% (SD: 14.2%) posterior movement from 0° to 140° of flexion. During kneeling, it indicated 25.1% (SD: 7.1%) posterior movement from 110° to 140° of flexion. There was no significant difference between squatting and kneeling (p = 0.13) ([Fig. 7]).

Discussion
This study has evaluated for the first time the in vivo kinematics of patients after MB UKA during high-flexion activities of daily living using CAD model of fluoroscopically captured images.
At high flexion angle, the femoral external rotation during squatting was smaller than that during kneeling. Furthermore, the medial side of the femur during squatting was more posteriorly located compared with that during kneeling. These suggest that the medial side of the UKA knees more easily slide posteriorly during weight-bearing activity. In this study, the posterior tibial slope of the medial side was 5.3° (SD: 2.7°). Weber et al[30] have demonstrated that a higher posterior tibial slope produced posterior translation of the femur on the medial side of MB UKA knees in the simulation study. Moreover, MB UKA has low conformity between the meniscal bearing and the tibial articular surface due to the flat-on-flat design. The posterior tibial slope and low conformity between the meniscal bearing and the tibial articular surface may affect posterior slide during weight-bearing activity. Meanwhile, the medial side during kneeling did not indicate significant movement with flexion similar to that of normal knees.[26] This suggests that kneeling is a medially stabilized activity which indicates a medial-pivot pattern. During kneeling, the medial contact pressure increases.[31] This medial contact pressure might induce the medial-pivot kinematics.
Peersman et al[14] have demonstrated that the in vitro kinematics of unloaded MB UKA knees closely resembled those of normal knees. In normal knees, there are significant differences between squatting and kneeling. Meanwhile, femoral external rotation was more than 20° during both activities.[26] In this study, there were significant differences between squatting and kneeling at high flexion angle, with approximately 10° of femoral rotation during squatting and less than 10° during kneeling. This suggests that the in vivo kinematics of MB UKA knees were also different between squatting and kneeling, similar to the kinematics of normal knees. However, the amount of femoral external rotation with flexion of MB UKA knees might be smaller than that of normal knees. Several studies that investigated the in vivo kinematics of TKA knees during high-flexion activities have reported that the amount of femoral external rotation with flexion of TKA knees was smaller than that of normal knees.[32] [33] Additionally, Banks et al[9] have examined the in vivo kinematics of FB UKA knees during lunge and kneeling, and the amount of femoral external rotation was similar to that of the current study. These suggest that the femoral external rotation with flexion of MB UKA knees is similar to those of FB UKA knees and TKA knees. Furthermore, during high-flexion activities, femoral rotation with knees flexion after UKA and TKA is difficult to recreate compared with that of normal knees. Hamai et al[34] have reported that the femoral external rotation of OA knees during high-flexion activities was smaller than that of normal knees due to increased collateral stiffness and other soft tissue contractures. In the current study, there were no significant difference between squatting and kneeling in the lateral side. However, the amount of posterior translation (squatting: 50.0%, kneeling: 25.1%) was smaller than that of normal knees (squatting: 78.7%, kneeling: 40.2%).[26] Therefore, posterolateral stiffness may affect the different kinematics between MB UKA knees and normal knees. Furthermore, Mochizuki et al[8] have reported that the kinematics of FB UKA was similar to that of preoperative knees. These suggest that the kinematics of preoperative OA knees might affect the kinematics of MB UKA knees.
Regarding the varus–valgus angle, there was no significant difference between squatting and kneeling. A previous study has demonstrated that the varus–valgus angle with flexion of normal knees did not differ significantly during squatting and kneeling.[26] This suggests that the varus–valgus kinematics of MB UKA knees may recreate those of normal knees.
The maximum flexion angle of MB UKA knees during kneeling was larger than that during squatting. The maximum flexion angle of MB UKA knees during kneeling was beyond 145°. Regarding TKA, Niki et al[33] have reported that Japanese-style sitting requires beyond 145° of flexion, same with the result of this study. The high-flexion sitting that Asian patients desire after MB UKA may require beyond 145°.
Some limitations of this study need to be discussed. First, this study did not compare between MB UKA and FB UKA. The difference between MB UKA and FB UKA remains unclear. Second, this study analyzed patients who achieved kneeling. The kinematics of patients who cannot perform kneeling might differ. Third, during kneeling, the dorsum of the foot contacted the ground, and the ankle was plantarflexed. This ankle position might induce greater internal rotation of the tibia which can affect femoral rotation.
Conclusion
In MB UKA, femoral external rotation with flexion was observed during both squatting and kneeling. At high flexion angle, the kinematics may differ depending on the activities.
Conflict of Interest
None declared.
-
References
- 1 Marx RG, Jones EC, Atwan NC, Closkey RF, Salvati EA, Sculco TP. Measuring improvement following total hip and knee arthroplasty using patient-based measures of outcome. J Bone Joint Surg Am 2005; 87 (09) 1999-2005
- 2 Ethgen O, Bruyère O, Richy F, Dardennes C, Reginster JY. Health-related quality of life in total hip and total knee arthroplasty. A qualitative and systematic review of the literature. J Bone Joint Surg Am 2004; 86 (05) 963-974
- 3 Wylde V, Blom AW, Whitehouse SL, Taylor AH, Pattison GT, Bannister GC. Patient-reported outcomes after total hip and knee arthroplasty: comparison of midterm results. J Arthroplasty 2009; 24 (02) 210-216
- 4 Von Keudell A, Sodha S, Collins J, Minas T, Fitz W, Gomoll AH. Patient satisfaction after primary total and unicompartmental knee arthroplasty: an age-dependent analysis. Knee 2014; 21 (01) 180-184
- 5 Liddle AD, Pandit H, Judge A, Murray DW. Patient-reported outcomes after total and unicompartmental knee arthroplasty: a study of 14,076 matched patients from the National Joint Registry for England and Wales. Bone Joint J 2015; 97-B (06) 793-801
- 6 Motesharei A, Rowe P, Blyth M, Jones B, Maclean A. A comparison of gait one year post operation in an RCT of robotic UKA versus traditional Oxford UKA. Gait Posture 2018; 62: 41-45
- 7 Millar LJ, Banger M, Rowe PJ, Blyth M, Jones B, Maclean A. A five-year follow up of gait in robotic assisted vs conventional unicompartmental knee arthroplasty. Gait Posture 2018; 65: 31-32
- 8 Mochizuki T, Sato T, Blaha JD. et al. Kinematics of the knee after unicompartmental arthroplasty is not the same as normal and is similar to the kinematics of the knee with osteoarthritis. Knee Surg Sports Traumatol Arthrosc 2014; 22 (08) 1911-1917
- 9 Banks SA, Fregly BJ, Boniforti F, Reinschmidt C, Romagnoli S. Comparing in vivo kinematics of unicondylar and bi-unicondylar knee replacements. Knee Surg Sports Traumatol Arthrosc 2005; 13 (07) 551-556
- 10 Catani F, Benedetti MG, Bianchi L, Marchionni V, Giannini S, Leardini A. Muscle activity around the knee and gait performance in unicompartmental knee arthroplasty patients: a comparative study on fixed- and mobile-bearing designs. Knee Surg Sports Traumatol Arthrosc 2012; 20 (06) 1042-1048
- 11 Becker R, Mauer C, Stärke C. et al. Anteroposterior and rotational stability in fixed and mobile bearing unicondylar knee arthroplasty: a cadaveric study using the robotic force sensor system. Knee Surg Sports Traumatol Arthrosc 2013; 21 (11) 2427-2432
- 12 Heyse TJ, El-Zayat BF, De Corte R. et al. UKA closely preserves natural knee kinematics in vitro. Knee Surg Sports Traumatol Arthrosc 2014; 22 (08) 1902-1910
- 13 Patil S, Colwell Jr CW, Ezzet KA, D'Lima DD. Can normal knee kinematics be restored with unicompartmental knee replacement?. J Bone Joint Surg Am 2005; 87 (02) 332-338
- 14 Peersman G, Slane J, Vuylsteke P. et al. Kinematics of mobile-bearing unicompartmental knee arthroplasty compared to native: results from an in vitro study. Arch Orthop Trauma Surg 2017; 137 (11) 1557-1563
- 15 Emerson Jr RH, Hansborough T, Reitman RD, Rosenfeldt W, Higgins LL. Comparison of a mobile with a fixed-bearing unicompartmental knee implant. Clin Orthop Relat Res 2002; (404) 62-70
- 16 Smith TO, Hing CB, Davies L, Donell ST. Fixed versus mobile bearing unicompartmental knee replacement: a meta-analysis. Orthop Traumatol Surg Res 2009; 95 (08) 599-605
- 17 Walker T, Heinemann P, Bruckner T, Streit MR, Kinkel S, Gotterbarm T. The influence of different sets of surgical instrumentation in Oxford UKA on bearing size and component position. Arch Orthop Trauma Surg 2017; 137 (07) 895-902
- 18 Ettinger M, Zoch JM, Becher C. et al. In vitro kinematics of fixed versus mobile bearing in unicondylar knee arthroplasty. Arch Orthop Trauma Surg 2015; 135 (06) 871-877
- 19 Pandit H, Hamilton TW, Jenkins C, Mellon SJ, Dodd CA, Murray DW. The clinical outcome of minimally invasive Phase 3 Oxford unicompartmental knee arthroplasty: a 15-year follow-up of 1000 UKAs. Bone Joint J 2015; 97-B (11) 1493-1500
- 20 Gleeson RE, Evans R, Ackroyd CE, Webb J, Newman JH. Fixed or mobile bearing unicompartmental knee replacement? A comparative cohort study. Knee 2004; 11 (05) 379-384
- 21 Li MG, Yao F, Joss B, Ioppolo J, Nivbrant B, Wood D. Mobile vs. fixed bearing unicondylar knee arthroplasty: a randomized study on short term clinical outcomes and knee kinematics. Knee 2006; 13 (05) 365-370
- 22 Suzuki T, Ryu K, Kojima K. et al. Evaluation of spacer block technique using tensor device in unicompartmental knee arthroplasty. Arch Orthop Trauma Surg 2015; 135 (07) 1011-1016
- 23 Scuderi GR, Bourne RB, Noble PC, Benjamin JB, Lonner JH, Scott WN. The new Knee Society Knee Scoring System. Clin Orthop Relat Res 2012; 470 (01) 3-19
- 24 Ewald FC. The Knee Society total knee arthroplasty roentgenographic evaluation and scoring system. Clin Orthop Relat Res 1989; (248) 9-12
- 25 Yamazaki T, Watanabe T, Nakajima Y. et al. Improvement of depth position in 2-D/3-D registration of knee implants using single-plane fluoroscopy. IEEE Trans Med Imaging 2004; 23 (05) 602-612
- 26 Kono K, Tomita T, Futai K. et al. In vivo three-dimensional kinematics of normal knees during different high-flexion activities. Bone Joint J 2018; 100-B (01) 50-55
- 27 Kawashima K, Tomita T, Tamaki M, Murase T, Yoshikawa H, Sugamoto K. In vivo three-dimensional motion analysis of osteoarthritic knees. Mod Rheumatol 2013; 23 (04) 646-652
- 28 Grood ES, Suntay WJ. A joint coordinate system for the clinical description of three-dimensional motions: application to the knee. J Biomech Eng 1983; 105 (02) 136-144
- 29 Kanda Y. Investigation of the freely available easy-to-use software ‘EZR’ for medical statistics. Bone Marrow Transplant 2013; 48 (03) 452-458
- 30 Weber P, Woiczinski M, Steinbrück A. et al. Increase in the tibial slope in unicondylar knee replacement: analysis of the effect on the kinematics and ligaments in a weight-bearing finite element model. BioMed Res Int 2018; 2018: 8743604
- 31 Lee TQ. Biomechanics of hyperflexion and kneeling before and after total knee arthroplasty. Clin Orthop Surg 2014; 6 (02) 117-126
- 32 Grieco TF, Sharma A, Dessinger GM, Cates HE, Komistek RD. In vivo kinematic comparison of a bicruciate stabilized total knee arthroplasty and the normal knee using fluoroscopy. J Arthroplasty 2018; 33 (02) 565-571
- 33 Niki Y, Takeda Y, Udagawa K, Enomoto H, Toyama Y, Suda Y. Is greater than 145degrees of deep knee flexion under weight-bearing conditions safe after total knee arthroplasty?: a fluoroscopic analysis of Japanese-style deep knee flexion. Bone Joint J 2013; 95-B (06) 782-787
- 34 Hamai S, Moro-oka TA, Miura H. et al. Knee kinematics in medial osteoarthritis during in vivo weight-bearing activities. J Orthop Res 2009; 27 (12) 1555-1561
Address for correspondence
Publication History
Received: 07 June 2023
Accepted: 07 January 2024
Accepted Manuscript online:
08 January 2024
Article published online:
01 February 2024
© 2024. Thieme. All rights reserved.
Thieme Medical Publishers, Inc.
333 Seventh Avenue, 18th Floor, New York, NY 10001, USA
-
References
- 1 Marx RG, Jones EC, Atwan NC, Closkey RF, Salvati EA, Sculco TP. Measuring improvement following total hip and knee arthroplasty using patient-based measures of outcome. J Bone Joint Surg Am 2005; 87 (09) 1999-2005
- 2 Ethgen O, Bruyère O, Richy F, Dardennes C, Reginster JY. Health-related quality of life in total hip and total knee arthroplasty. A qualitative and systematic review of the literature. J Bone Joint Surg Am 2004; 86 (05) 963-974
- 3 Wylde V, Blom AW, Whitehouse SL, Taylor AH, Pattison GT, Bannister GC. Patient-reported outcomes after total hip and knee arthroplasty: comparison of midterm results. J Arthroplasty 2009; 24 (02) 210-216
- 4 Von Keudell A, Sodha S, Collins J, Minas T, Fitz W, Gomoll AH. Patient satisfaction after primary total and unicompartmental knee arthroplasty: an age-dependent analysis. Knee 2014; 21 (01) 180-184
- 5 Liddle AD, Pandit H, Judge A, Murray DW. Patient-reported outcomes after total and unicompartmental knee arthroplasty: a study of 14,076 matched patients from the National Joint Registry for England and Wales. Bone Joint J 2015; 97-B (06) 793-801
- 6 Motesharei A, Rowe P, Blyth M, Jones B, Maclean A. A comparison of gait one year post operation in an RCT of robotic UKA versus traditional Oxford UKA. Gait Posture 2018; 62: 41-45
- 7 Millar LJ, Banger M, Rowe PJ, Blyth M, Jones B, Maclean A. A five-year follow up of gait in robotic assisted vs conventional unicompartmental knee arthroplasty. Gait Posture 2018; 65: 31-32
- 8 Mochizuki T, Sato T, Blaha JD. et al. Kinematics of the knee after unicompartmental arthroplasty is not the same as normal and is similar to the kinematics of the knee with osteoarthritis. Knee Surg Sports Traumatol Arthrosc 2014; 22 (08) 1911-1917
- 9 Banks SA, Fregly BJ, Boniforti F, Reinschmidt C, Romagnoli S. Comparing in vivo kinematics of unicondylar and bi-unicondylar knee replacements. Knee Surg Sports Traumatol Arthrosc 2005; 13 (07) 551-556
- 10 Catani F, Benedetti MG, Bianchi L, Marchionni V, Giannini S, Leardini A. Muscle activity around the knee and gait performance in unicompartmental knee arthroplasty patients: a comparative study on fixed- and mobile-bearing designs. Knee Surg Sports Traumatol Arthrosc 2012; 20 (06) 1042-1048
- 11 Becker R, Mauer C, Stärke C. et al. Anteroposterior and rotational stability in fixed and mobile bearing unicondylar knee arthroplasty: a cadaveric study using the robotic force sensor system. Knee Surg Sports Traumatol Arthrosc 2013; 21 (11) 2427-2432
- 12 Heyse TJ, El-Zayat BF, De Corte R. et al. UKA closely preserves natural knee kinematics in vitro. Knee Surg Sports Traumatol Arthrosc 2014; 22 (08) 1902-1910
- 13 Patil S, Colwell Jr CW, Ezzet KA, D'Lima DD. Can normal knee kinematics be restored with unicompartmental knee replacement?. J Bone Joint Surg Am 2005; 87 (02) 332-338
- 14 Peersman G, Slane J, Vuylsteke P. et al. Kinematics of mobile-bearing unicompartmental knee arthroplasty compared to native: results from an in vitro study. Arch Orthop Trauma Surg 2017; 137 (11) 1557-1563
- 15 Emerson Jr RH, Hansborough T, Reitman RD, Rosenfeldt W, Higgins LL. Comparison of a mobile with a fixed-bearing unicompartmental knee implant. Clin Orthop Relat Res 2002; (404) 62-70
- 16 Smith TO, Hing CB, Davies L, Donell ST. Fixed versus mobile bearing unicompartmental knee replacement: a meta-analysis. Orthop Traumatol Surg Res 2009; 95 (08) 599-605
- 17 Walker T, Heinemann P, Bruckner T, Streit MR, Kinkel S, Gotterbarm T. The influence of different sets of surgical instrumentation in Oxford UKA on bearing size and component position. Arch Orthop Trauma Surg 2017; 137 (07) 895-902
- 18 Ettinger M, Zoch JM, Becher C. et al. In vitro kinematics of fixed versus mobile bearing in unicondylar knee arthroplasty. Arch Orthop Trauma Surg 2015; 135 (06) 871-877
- 19 Pandit H, Hamilton TW, Jenkins C, Mellon SJ, Dodd CA, Murray DW. The clinical outcome of minimally invasive Phase 3 Oxford unicompartmental knee arthroplasty: a 15-year follow-up of 1000 UKAs. Bone Joint J 2015; 97-B (11) 1493-1500
- 20 Gleeson RE, Evans R, Ackroyd CE, Webb J, Newman JH. Fixed or mobile bearing unicompartmental knee replacement? A comparative cohort study. Knee 2004; 11 (05) 379-384
- 21 Li MG, Yao F, Joss B, Ioppolo J, Nivbrant B, Wood D. Mobile vs. fixed bearing unicondylar knee arthroplasty: a randomized study on short term clinical outcomes and knee kinematics. Knee 2006; 13 (05) 365-370
- 22 Suzuki T, Ryu K, Kojima K. et al. Evaluation of spacer block technique using tensor device in unicompartmental knee arthroplasty. Arch Orthop Trauma Surg 2015; 135 (07) 1011-1016
- 23 Scuderi GR, Bourne RB, Noble PC, Benjamin JB, Lonner JH, Scott WN. The new Knee Society Knee Scoring System. Clin Orthop Relat Res 2012; 470 (01) 3-19
- 24 Ewald FC. The Knee Society total knee arthroplasty roentgenographic evaluation and scoring system. Clin Orthop Relat Res 1989; (248) 9-12
- 25 Yamazaki T, Watanabe T, Nakajima Y. et al. Improvement of depth position in 2-D/3-D registration of knee implants using single-plane fluoroscopy. IEEE Trans Med Imaging 2004; 23 (05) 602-612
- 26 Kono K, Tomita T, Futai K. et al. In vivo three-dimensional kinematics of normal knees during different high-flexion activities. Bone Joint J 2018; 100-B (01) 50-55
- 27 Kawashima K, Tomita T, Tamaki M, Murase T, Yoshikawa H, Sugamoto K. In vivo three-dimensional motion analysis of osteoarthritic knees. Mod Rheumatol 2013; 23 (04) 646-652
- 28 Grood ES, Suntay WJ. A joint coordinate system for the clinical description of three-dimensional motions: application to the knee. J Biomech Eng 1983; 105 (02) 136-144
- 29 Kanda Y. Investigation of the freely available easy-to-use software ‘EZR’ for medical statistics. Bone Marrow Transplant 2013; 48 (03) 452-458
- 30 Weber P, Woiczinski M, Steinbrück A. et al. Increase in the tibial slope in unicondylar knee replacement: analysis of the effect on the kinematics and ligaments in a weight-bearing finite element model. BioMed Res Int 2018; 2018: 8743604
- 31 Lee TQ. Biomechanics of hyperflexion and kneeling before and after total knee arthroplasty. Clin Orthop Surg 2014; 6 (02) 117-126
- 32 Grieco TF, Sharma A, Dessinger GM, Cates HE, Komistek RD. In vivo kinematic comparison of a bicruciate stabilized total knee arthroplasty and the normal knee using fluoroscopy. J Arthroplasty 2018; 33 (02) 565-571
- 33 Niki Y, Takeda Y, Udagawa K, Enomoto H, Toyama Y, Suda Y. Is greater than 145degrees of deep knee flexion under weight-bearing conditions safe after total knee arthroplasty?: a fluoroscopic analysis of Japanese-style deep knee flexion. Bone Joint J 2013; 95-B (06) 782-787
- 34 Hamai S, Moro-oka TA, Miura H. et al. Knee kinematics in medial osteoarthritis during in vivo weight-bearing activities. J Orthop Res 2009; 27 (12) 1555-1561