Keywords
Pancreatobiliary (ERCP/PTCD) - Cholangioscopy - Tissue diagnosis - Strictures
Introduction
Early and accurate diagnosis of neoplastic biliary strictures increases patient survival;
nevertheless, the most commonly used technique, endoscopic retrograde cholangiopancreatography
(ERCP) with brush cytology and biopsy forceps, has low diagnostic yield [1].
To overcome this limitation, new techniques, such as digital single-operator cholangioscopy
(DSOC) and probe-based confocal laser endomicroscopy (pCLE), have been developed [1]
[2]. DSOC enables high-resolution visualization of the bile duct system, tissue sampling,
and interventional therapies [3]
[4]. This technique, involving the visual interpretation of biliary malignancies, is
superior to ERCP in terms of diagnosis of indeterminate biliary lesions, with an overall
sensitivity of 94% and a specificity of 95% [5]. However, DSOC is an advanced endoscopic technique limited to specialized training
and lack of training facilities and formal training guidelines [6].
On the other hand, pCLE enables in vivo histological evaluation of the mucosa through
administration of a contrast agent such as fluorescein, which is administered intravenously
and distributed within the epithelial extracellular matrix and lamina propria, allowing
in vivo evaluation [7]
[8]. This technique achieved adequate sensitivity and specificity for identifying neoplasia,
ranging from 75% to 87% and 76% to 100%, respectively [1]
[2]. However, when pCLE is combined with conventional tissue sampling through a DSOC-guided
pCLE (DSOC-pCLE), the sensitivity and specificity are 93% and 82%, respectively [2]. Considering the cost, difficulty obtaining adequate interobserver agreement, lack
of availability, and minimal improvement in diagnostic accuracy, utilization of pCLE
is quite limited [2].
Currently, DSOC-guided tissue biopsy is utilized where conventional methods do not
achieve diagnosis and as an adjunct to pCLE (when available) [2]. Through direct observation of the lesions, endoscopists can discern areas suggestive
of neoplasia and obtain directed biopsies based on macroscopic patterns, reducing
the number of inconclusive or inadequate tissue sampling, compared with ERCP; thus,
reducing reinterventions and performing early management [9]
[10]
[11]
[12].
A recent study comparing several methods indicated that the combination of pCLE and
DSOC showed observed agreement superior to ERCP and DSOC alone (93.3% vs 70% and 90%,
respectively) [13]. These results indicate that DSOC combined with pCLE can provide an accurate interpretation
of biliary strictures. However, despite high diagnostic accuracy, these procedures
are expensive, and the required equipment is not globally available. Therefore, there
is a need to develop new technologies capable of providing additional data for detection
of neoplasia and guide the best possible site for tissue acquisition.
In recent years, artificial intelligence (AI) tools have been applied in gastrointestinal
endoscopy, mainly for cancer detection [14]. Notably, convolutional neural network models (CNNs) are capable of extracting information
and classifying features from images and/or videos [14]. Currently, CNN models trained to identify areas suggestive of neoplasia in indeterminate
biliary strictures have been proposed [15]
[16]
[17]. These models achieve high diagnostic accuracy when used to interpret images; nevertheless,
until recently, these AI models could not be applied in real time during live procedures
[15]
[16]. However, a newly developed CNN model capable of real-time analysis (AIWorks – Cholangioscopy,
mdconsgroup, Guayaquil, Ecuador) has shown an 80% observed agreement during clinical
validation [18]. Currently, there is limited information comparing DSOC-based AI models and DSOC-pCLE
for identification of neoplastic lesions. Thus, we aimed to compare the diagnostic
accuracy of a DSOC-based AI model with DSOC-pCLE for identifying neoplasia in patients
with indeterminate biliary strictures.
Patients and methods
Study design and ethics
This retrospective study was performed at the Instituto Ecuatoriano de Enfermedades
Digestivas, a tertiary academic center in Guayaquil, Ecuador. The study protocol was
approved by the institutional review board and designed in accordance with the Declaration
of Helsinki and STARD 2015 guidelines. Patients or their legal guardians provided
written informed consent for analysis and publication of the recorded videos before
undergoing the procedures.
Population selection
Consecutive patients who underwent DSOC and DSOC-pCLE procedures from January 2014
to May 2022 were included. Data from patients aged ≥ 18 years old who underwent DSOC
and DSOC-pCLE were included for analysis. Patients were excluded if: 1) any DSOC and/or
DSOC-pCLE videos and/or images were unavailable; 2) they had no histological confirmation,
based on biopsy or surgical resection; and/or 3) < 12 months of follow-up data were
available.
Endoscopic procedures
DSOC procedure
All patients were placed in a supine position under general anesthesia and received
antibiotic prophylaxis. Then they were assessed using a standard duodenoscope (Pentax
ED 3670TK; Pentax Medical, Hoya Corp., Tokyo, Japan), Pentax EPK-I and EPK-i5010 video
processors, and a second-generation SpyGlass DS Digital System (Boston Scientific,
Marlborough, Massachusetts, United States) or a 9F eyeMAX cholangioscope (Micro-tech,
Nanjing, China). The SpyScope DS II catheter (SpyGlass DS Digital System) or the eyeMAX
cholangioscope were passed proximally into the bile duct, suction was used to remove
bile, sterile saline solution was infused to optimize imaging, and the cholangioscope
was slowly withdrawn. Ultimately, systematic inspection of the ductal mucosa was performed.
A minimum of four biopsy samples were taken from areas suggestive of neoplasia and
visual impressions of the endoscopist was classified according to the Carlos Robles-Medranda
classification [11].
pCLE procedure
Consecutively after DSOC, patients underwent a DSOC-pCLE procedure. Patients were
intravenously injected with 5 mL 10% fluorescein (BioGlo, Sofar Productos, Bogota,
Colombia) and then pCLE was performed by passing a 1.0-mm Cellvizio CholangioFlex
probe (Mauna Kea Technologies, Paris, France) through the cholangioscope working channel.
The probe was gently placed in contact with the mucosa to avoid trauma. For DSOC-pCLE,
the Miami malignancy criteria and the Paris inflammatory criteria were used. Miami
malignancy criteria constituted thick white and dark bands, dark clumps, or epithelium;
on the other hand, the Paris classification inflammatory criteria included vascular
congestion, roughness aspect, increased interglandular space, and thickened reticular
stricture [19]
[20].
Offline video analysis by expert endoscopists
The pCLE videos were reviewed by two expert endoscopists (C.R.M. & J.A.V.) who were
blinded to any clinical or ERCP information at the moment of offline video analysis.
They indicated which descriptive criteria were present or absent in the videos.
pCLE Miami and Paris disaggregated criteria (pCLE, probe-based confocal laser
endomicroscopy.):
-
Presence or absence of dark bands
-
Presence or absence of white bands
-
Presence or absence of dark clumps
-
Presence or absence of epithelium
-
Presence or absence of fluorescein leak
-
Presence or absence of vascular congestion
-
Presence or absence of rough appearance
-
Presence or absence of reticular thickening
-
Presence or absence of increased intraglandular space
The expert endoscopists evaluated all cases using both classifications (Miami and
Paris) and more Miami classification malignancy criteria, observed by the endoscopists,
than Paris classification inflammatory criteria constituted neoplasia. For DSOC- and
pCLE-guided biopsy, corresponding histological findings constituted neoplasia.
Offline video analysis with AIWorks-Cholangioscopy software
All recorded DSOC procedures were analyzed offline with the AIWorks-Cholangioscopy
software (mdconsgroup, Guayaquil, Ecuador). AIWorks-Cholangioscopy is a CNN trained
to identify bile duct mucosal abnormalities, commonly observed features of neoplastic
lesions that can be recognized by various currently available classification systems
(CRM, Mendoza) [11]
[21], when identifying the following criteria: neovascularity, surface irregularities,
polyploids, ulcerations or friability. This model was developed using YOLOv5 (You
Only Look Once version 5, Washington, United States) and can delimit potential neoplastic
lesions with a bounding box with high recall and precision ([Fig. 1]) [18].
 Fig. 1 Step-by-step visual interpretation of application of the AIWorks-Cholangioscopy (mdconsgroup,
Guayaquil, Ecuador) software for video analysis.
Fig. 1 Step-by-step visual interpretation of application of the AIWorks-Cholangioscopy (mdconsgroup,
Guayaquil, Ecuador) software for video analysis.
For each patient, model output highlighted any areas that were deemed suggestive of
neoplasia with a bounding box, and a screenshot that could be accessed within the
software was automatically saved ([Video 1]). For the present study, an observer (J.B-B.) blinded to any clinical data or ERCP
information recorded the judgement output by the AI and marked detection or absence
of detection of areas suggestive of neoplasia provided by the AIWorks-Cholangioscopy
software for each DSOC video. The information was registered in a database for comparison
with the pathology, 12-month follow-up, DSOC-pCLE, and DSOC visual impression data.
utomatic detection of areas suggestive of neoplasia using the AIWorks-Cholangioscopy
software in a patient with biopsy-confirmed cholangiocarcinoma. The detected areas
are highlighted with green bounding boxes.Video 1
Statistical analysis
Technical considerations
Statistical analysis was performed using R v4.1.2 (R Foundation for Statistical Computing;
Vienna, Austria) by our institutional biostatistician (M.P-T.). P < 0.05 was considered to indicate statistical significance.
Sample size
Based on the observed agreement of 93.3% and 80% of DSOC-pCLE [13] and DSOC-based AI model [18], respectively, a size effect of h = 0.4036 was calculated. Considering a 5% alfa and 20% beta errors, a sample size
of 76 pairs was necessary to demonstrate DSOC-pCLE observed agreement was higher than
that reached by the DSOC-based AI model, with 80% power statistic. A pair was defined
as a patient who was assessed through DSOC-pCLE and DSOC-based AI model.
Descriptive analysis
Numerical variables are presented as the mean (standard deviation) or median (interquartile
range) depending on the normality of their statistical distribution, which was assessed
with the Kolmogorov‒Smirnov test. Corresponding categorical variables are described
as frequencies (%) with 95% confidence intervals.
Diagnostic accuracy
Sensitivity, specificity, positive and negative predictive values, and observed agreement
of DSOC visual impression, DSOC-pCLE, DSOC and pCLE-guided biopsy, and DSOC-AI model
were calculated to evaluate diagnostic accuracy. Receiver operator characteristic
analysis was performed, and to compare the areas under the receiver operator curve
(AUCs) of the diagnostic methods, we performed DeLong’s test. The reference standard
for neoplasia was based on further clinical evaluation, imaging, or surgical specimen
findings during a 12-month follow-up period. A subanalysis by distal vs proximal lesion
location was performed.
Results
Baseline characteristics
A total of 90 patients were included in the study and 21 patients were excluded ([Fig. 2]). Baseline characteristics of the patients were as follows ([Table 1]). Mean age was 66.4 years ± 13.7 and 56.7% were female. Tumor suspicion was the
most common indication (55.6%). Strictures were most commonly proximal and middle
lesions from the common bile duct (CBD) (42.2%), with a median size of 22.0 mm (14.3–25.0
mm). Twenty-five of 90 patients (27.8%) had previously undergone ERCP at least once.
A total of 26.1% of cases had previous plastic stent placement, with a median duration
of 60 days (18.0–96.0). The most common neoplastic lesion based on histopathological
results was cholangiocarcinoma (94.4%) ([Fig. 3]). Of the patients, 15.5% underwent surgery.
 Fig. 2 Flowchart of patient recruitment procedures.
Fig. 2 Flowchart of patient recruitment procedures.
Table 1 Baseline characteristics.
|
N = 90
|
|
SD, standard deviation; CBD, common bile duct; IQR, interquartile range; ERCP, endoscopic
retrograde cholangiopancreatography.
|
|
Age (years), mean ± SD
|
66.4 ± 13.7
|
|
|
3 (3.3)
|
|
|
34 (37.8)
|
|
|
53 (58.9)
|
|
Sex (female), n (%)
|
51 (56.7)
|
|
Main indication, n (%)
|
|
|
|
50 (55.6)
|
|
|
31 (34.4)
|
|
|
9 (10.0)
|
|
Lesion location, n (%)
|
|
|
|
38 (42.2)
|
|
|
12/48
|
|
|
26/48
|
|
|
52 (57.8)
|
|
|
30/52
|
|
|
6/52
|
|
|
11/52
|
|
|
5/52
|
|
Lesion size (mm), median (IQR)
|
20 (14.3–25.0)
|
|
Previously performed ERCP, n (%)
|
25 (27.8)
|
|
Previous stent placement, n (%)
|
18 (20.0)
|
|
Stent placement duration (days), median (IQR)
|
60.0 (18.0–96.0)
|
|
Performed biopsy, n (%)
|
90 (100.0)
|
|
No. of biopsy samples taken, median (IQR)
|
4 (1–6)
|
|
Diagnosis after histopathological confirmation, n (%)
|
|
|
|
85 (94.4)
|
|
|
1 (1.1)
|
|
|
2 (2.2)
|
|
|
2 (2.2)
|
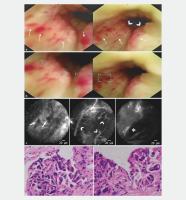 Fig. 3 The case of an 88-year-old male with a lesion extending from the middle third portion
of the common bile duct to the common hepatic duct is presented as representative
example. a Using the 9F eyeMAX cholangioscope, a raised intraductal lesion (arrowhead) with
increased vascularity (arrows) was observed. b AIWorks-Cholangioscopy software detected areas suggestive of neoplasia (green bounding
box) in the same locations identified with the cholangioscope. c pCLE findings revealed dark bands (*), white bands (arrowhead) and dark clumps (arrows).
d Hematoxylin and eosin biopsy slide (100x) revealed malignant glandular tissue covered
with stratified cylindric cells and atypical hypertrophic hyperchromatic nuclei compatible
with cholangiocarcinoma.
Fig. 3 The case of an 88-year-old male with a lesion extending from the middle third portion
of the common bile duct to the common hepatic duct is presented as representative
example. a Using the 9F eyeMAX cholangioscope, a raised intraductal lesion (arrowhead) with
increased vascularity (arrows) was observed. b AIWorks-Cholangioscopy software detected areas suggestive of neoplasia (green bounding
box) in the same locations identified with the cholangioscope. c pCLE findings revealed dark bands (*), white bands (arrowhead) and dark clumps (arrows).
d Hematoxylin and eosin biopsy slide (100x) revealed malignant glandular tissue covered
with stratified cylindric cells and atypical hypertrophic hyperchromatic nuclei compatible
with cholangiocarcinoma.
Diagnostic accuracy
For evaluating diagnostic accuracy, the four diagnostic methods were compared with
respect to several performance metrics ([Table 2] [total]). Diagnoses based on DSOC visual impressions achieved 95.6% observed agreement,
with 96.5% sensitivity and 75% specificity. pCLE achieved a 94.4%, 94.2%, and 100%
observed agreement, sensitivity, and specificity, respectively. DSOC and pCLE-guided
biopsies achieved 97.7%, 100% and 97.9% sensitivity, specificity, and observed agreement,
respectively. Finally, the DSOC-based AI model detection software achieved 97.7% sensitivity,
75% specificity and 96.7% observed agreement. The AUC for DSOC-AI was 0.790, DSOC
direct visualization had an AUC of 0.740, pCLE had an AUC of 0.720, and DSOC and pCLE-guided
biopsies had an AUC of 0.830. When comparing with DSOC-AI using the DeLong’s test,
there were no statistically significant differences among diagnostics accuracy of
these methods (DSOC direct visualization, P = 0.763; pCLE, P = 0.634; and pCLE-guided biopsies, P = 0.809).
Table 2 Diagnostic accuracy of visual impressions during digital single-operator cholangioscopy
(DSOC), DSOC-guided probed-based confocal endomicroscopy (pCLE), DSOC and pCLE-guided
biopsy, and a DSOC-based artificial intelligence (AI) model [n/T; % (95% CI)].
|
Sensitivity
|
Specificity
|
Positive predictive value
|
Negative predictive value
|
Observed agreement
|
AUC
(P value*)
|
|
CI, confidence interval; AUC, area under the curve; pCLE, probed-based confocal laser
endomicroscopy
*DeLong’s test.
|
|
Total (N = 90)
|
|
DSOC-based AI model
|
97.7% (91.9–99.7)
|
75% (19.4–99.4)
|
98.8% (93.6–99.9)
|
60% (14.7–94.7)
|
96.7% (90.6–99.3)
|
0.790 (reference)
|
|
DSOC direct visualization
|
96.5% (90.1–99.3)
|
75.0% (19.4–99.4)
|
98.8% (93.5–99.9)
|
50.0% (11.8–88.2)
|
95.6% (89.0–98.8)
|
0.740
(P = 0.763)
|
|
DSOC-guided pCLE
|
94.2% (86.9–98.1)
|
100% (39.8–100)
|
100% (95.6–100)
|
44.4% (13.7–78.8)
|
94.4% (87.5–98.2)
|
0.720 (P = 0.634)
|
|
DSOC and pCLE- guided biopsy
|
97.7%
(91.9–99.7)
|
100%
(39.8–100)
|
100%
(95.7–100)
|
66.7%
(22.3–95.7)
|
97.8%
(92.2–99.7)
|
0.830
(P = 0.809)
|
|
Lesions from distal and middle CBD (n = 38)
|
|
DSOC-based AI model
|
94.44 (81.34–99.32)
|
100 (15.81–100)
|
100 (89.72–100)
|
50 (6.76–93.24)
|
94.74 (82.25–99.36)
|
0.750 (reference)
|
|
DSOC direct visualization
|
97.22 (85.47–99.93)
|
100 (15.81–100)
|
100 (90–100)
|
66.67 (9.43–99.16)
|
97.37 (86.19–99.93)
|
0.833 (P = 0.707)
|
|
DSOC-guided
pCLE
|
88.89
(73.94–96.89)
|
100
(15.81–100)
|
100
(89.11–100)
|
33.33
(4.33–77.72)
|
89.47
(75.2–97.06)
|
0.667
(P=0.643)
|
|
DSOC and pCLE- guided biopsy
|
97.22 (85.47–99.93)
|
100 (15.81–100)
|
100 (90–100)
|
66.67 (9.43–99.16)
|
97.37 (86.19–99.93)
|
0.833 (P=0.707)
|
|
Lesions from proximal CBD, common hepatic duct, hilum, and intrahepatic duct (n=52)
|
|
DSOC-based AI model
|
100 (92.89–100)
|
50 (1.26–98.74)
|
98.04 (89.55–99.95)
|
100 (2.5–100)
|
98.08 (89.74–99.95)
|
0.990 (reference)
|
|
DSOC direct visualization
|
96 (86.29–99.51)
|
50 (1.26–98.74)
|
97.96 (89.15–99.95)
|
33.33 (0.84–90.57)
|
94.23 (84.05–98.79)
|
0.656 (P < 0.001)
|
|
DSOC-guided pCLE
|
98 (89.35–99.95)
|
100 (15.81–100)
|
100 (92.75–100)
|
66.67 (9.43–99.16)
|
98.08 (89.74–99.95)
|
0.833 (P = 0.108)
|
|
DSOC and pCLE- guided biopsy
|
98 (89.35–99.95)
|
100 (15.81–100)
|
100 (92.75–100)
|
66.67 (9.43–99.16)
|
98.08 (89.74–99.95)
|
0.833 (P = 0.108)
|
In evaluating distal lesions, specifically from the distal or middle CBD, DSOC direct
visualization, as well as DSOC and pCLE-guided biopsy, demonstrated superior performance
compared with the DSOC-based AI model. When comparing with the AI, both methods achieved
the same higher sensitivity (97.22% vs 94.44%), negative predictive value (NPV) (66.67%
vs 50%), and observed agreement (97.37% vs 94.74%), although the differences were
not statistically significant (P = 0.707). Conversely, in distal lesions, DSOC-guided pCLE showed the lowest sensitivity
(88.89%), NPV (33.33%), and observed agreement (89.47%), with the differences again
not statistically significant (P = 0.643) ([Table 2] [lesions from distal and middle CBD]).
Although DSOC direct visualization performed well in assessing lesions in the distal
or middle CBD, a contrasting situation was observed when evaluating lesions in the
proximal CBD, common hepatic duct, hilum, and intrahepatic duct (52; 57.8%). Here,
the DSOC-based AI model achieved the highest sensitivity (100%) and NPV (100%), along
with the same highest observed agreement (98.08%) as DSOC-guided pCLE and DSOC and
pCLE-guided biopsy. Although the DSOC-based AI model did not significantly outperform
DSOC-guided pCLE and DSOC and pCLE-guided biopsy, it did achieve a significantly higher
AUC compared with DSOC direct visualization (0.990 vs 0.656; P < 0.001) ([Table 2] [lesions from proximal CBD, common hepatic duct, hilum, and intrahepatic duct]).
Discussion
The present study aimed to compare the diagnostic accuracy of a DSOC-based AI model
with DSOC-pCLE for identifying neoplasia in patients with indeterminate biliary strictures.
We found that the diagnostic accuracy for neoplastic lesion identification of the
AI model was similar to that for DSOC-pCLE, DSOC- and pCLE-guided biopsies and diagnoses
based on DSOC visual impressions, indicating that AI tools can accurately aid endoscopists
in identification of neoplasia during DSOC.
AI models can be classified as computer-assisted detection (CADe) or diagnostic devices
(CADx). This classification depends on whether the model detects mucosal lesions or
patterns (CADe) or characterizes lesions, for example, as benign or malignant lesions
(CADx) [22]. Currently, there are still no CADx tools for DSOC capable of accurately classifying
indeterminate biliary strictures, and thus, diagnosis is dependent on biopsy sampling.
On the other hand, several CADe tools have been proposed, but their widespread use
is limited to application in still images and it has not been able to perform adequately
during real-time procedures [15]
[16]. In addition, the diagnostic accuracy of CADe tools previously has been evaluated
with still images only, and thus, the high diagnostic accuracy obtain in these cases
cannot be extrapolated to reflect real clinical applications.
Robles-Medranda et al. performed a multicenter study initially evaluating application
of the AIWorks-Cholangioscopy software (mdconsgroup, Guayaquil, Ecuador) to still
images and obtained values similar to those obtained by Saraiva et al and Pereira
et al., with an observed agreement > 90.0% [15]
[16]
[18]. However, when recorded DSOC procedures of patients with neoplasia were input into
the model, its diagnostic accuracy changed, showing a sensitivity of 90.5%, a specificity
of 68.2%, a PPV of 74.0%, an NPV of 87.8%, and an observed agreement of 80.0%.
In the present study, we performed offline assessment of prerecorded DSOC videos of
patients with a confirmed diagnosis of neoplastic lesions. The AI model obtained the
following parameters: 97.7% sensitivity, 75.0% specificity, 98.8% PPV, 60.0% NPV,
and 96.7% observed agreement. These values were similar to those obtained for diagnosis
based on endoscopists’ visual impressions (96.5%, 75.0%, 98.8%, 50.0%, 95.6%, respectively).
In addition, Robles-Medranda et al. compared the AI software with diagnosis based
on visual impressions of a group of expert advanced endoscopists and a group of nonexperts;
the model obtained higher diagnostic accuracy than both groups. Similarly, here, the
AI model achieved a higher AUC (0.790) than diagnosis based on visual impressions
(0.740, P = 0.763); however, the difference between the two methods was not significant.
A recent systematic review evaluating application of CADe tools during cholangioscopy
included five studies. The models analyzed in these studies obtained high diagnostic
accuracy [23]. The CNN model applied for lesion detection in still images achieved 98.6%, 98.0%,
and 98.0% sensitivity, specificity, and observed agreement, respectively [18], with a 60 frames-per-second reading rate. Thus, CNN models appear to be promising
AI tools for diagnosis of potentially malignant biliary strictures.
pCLE technology allows microscopy detection in vivo through application of fluorescein
[24]
[25]
[26]. Two classifications have been proposed for biliary stricture analysis: the Miami
classification, based on the malignancy criteria, and the Paris criteria, based on
inflammatory criteria [26]. The Miami classification has a high sensitivity (98.0%) but low specificity (67.0%)
due to increased false-positive rates caused by lack of criteria ensuring unique identification
of malignant lesions [27]. Compared with the Miami classification, the sensitivity and specificity achieved
by the Paris criteria for inflammatory lesions were 81.0% and 83.0%, respectively
[28].
Using both classifications simultaneously to establish an objective measurement, such
as image scoring systems, could improve pCLE diagnostic performance [29]. In the present study, two observers analyzed the pCLE data and marked the presence
or absence of observed features from both the Miami and Paris classifications in a
disaggregated manner. Then, applying both classifications though Boolean operator,
we determined if a lesion was malignant or inflammatory based on presence of most
Miami criteria detected or most Paris criteria, respectively. Using this analysis,
DSOC-pCLE achieved 94.2% and 100% sensitivity and specificity, respectively.
Both modalities (DSOC-AI and pCLE) had similar AUCs (0.760 vs. 0.720, P = 0.634) and high observed agreement (96.7% and 94.4%, respectively). However, both
techniques obtained nominally lower diagnostic accuracy than biopsies. Despite the
lack of a significant difference between the DSOC-AI, DSOC-pCLE, and DSOC/pCLE-guided
biopsies, biopsies are still necessary for diagnosis confirmation; however, AI tools
will be able to provide real-time assistance in terms of AI-guided biopsy sampling
during DSOC procedures, improving the quality of samples obtained and reducing the
rate of inadequate biopsies. In addition, AI models could be used as second opinion
tools aiding in the decision-making process in complicated cases in which visual impression
is uncertain [30]. As computational resources improve, faster and more accurate AI models could be
developed to improve diagnostic accuracy and provide higher detection and recall,
increasing the quality of samples [31].
In addition to their diagnostic performance, the high cost of DSOC and pCLE must be
considered [13]. Few studies have evaluated the costs of single-use pCLE probes, and none have investigated
the cost of AI-assisted DSOC. Notably, Tanisaka et al. reported that the costs for
pCLE with DSOC surpass those for ERCP [13]. The potential reason for the procedure’s high cost includes the single-use pCLE
probe and the elevated costs of the most commonly available cholangioscope. The AIWorks-Cholangioscopy
model used here was trained with different brands of cholangioscopes (eyeMAX, Micro-Tech,
Nianjing, China; Spyglass, Boston Scientific, Marlborough, Massachusetts, United States)
and is cloud-based software; therefore, the software can be paired with different
brands of cholangioscopes with potentially lower cost. This tool may allow AI-guided
DSOC biopsy sampling to be performed as an alternative to DSOC-pCLE biopsy, requiring
the same amount of equipment as a traditional DSOC, and therefore, less equipment
compared with DSOC-pCLE. In addition, by performing biopsies guided by AI, the number
of samples required, and reinterventions could be reduced [18].
The limitations of the present study included its retrospective analysis and single-center
design, and the low number of benign cases. Considering the low NPV obtained by the
different studied methods, it is advisable to continue using pCLE in cases in in which
no neoplastic lesions were recognized during an AI-guided DSOC. Even so, this study
provided information about the clinical application of several DSOC-related methods.
Real-world studies are required to compare the AI model and pCLE to confirm the obtained
results. In addition, studies evaluating the cost-effectiveness of both procedures
are needed.
Conclusions
In conclusion, the DSOC-AI model demonstrated offline diagnostic accuracy similar
to that of DSOC-pCLE, DSOC alone, and DSOC- and pCLE-guided biopsies, providing insight
about novel technologies that could aid endoscopists in accurate identification of
neoplasia.





