

Subscribe to RSS
DOI: 10.1055/a-2469-4896
An International Consensus Practical Guide on Left Atrial Appendage Closure for the Non-implanting Physician: Executive Summary
Authors
Funding This project was investigator-proposed and conducted and was supported by an educational grant from Boston Scientific for the payment of Article Processing Charges. The sponsor was not involved in the construction of the manuscript.

Abstract
Many patients with atrial fibrillation (AF) who are in need of stroke prevention are not treated with oral anticoagulation or discontinue treatment shortly after its initiation. Despite the availability of direct oral anticoagulants (DOACs), such undertreatment has improved somewhat but is still evident. This is due to continued risks of bleeding events or ischemic strokes while on DOAC, poor treatment compliance, or aversion to anticoagulant therapy. Because of significant improvements in procedural safety over the years left atrial appendage closure (LAAC), using a catheter-based, device implantation approach, is increasingly favored for the prevention of thromboembolic events in AF patients who cannot have long-term oral anticoagulation. This article is an executive summary of a practical guide recently published by an international expert consensus group, which introduces the LAAC devices and briefly explains the implantation technique. The indications and device follow-up are more comprehensively described. This practical guide, aligned with published guideline/guidance, is aimed at those non-implanting physicians who may need to refer patients for consideration of LAAC.
Keywords
anticoagulation - atrial fibrillation - bleeding - left atrial appendage closure - left atrial appendage occlusion - stroke - preventionIntroduction
Atrial fibrillation (AF) is the most common sustained cardiac arrhythmia in adults and is associated with increased mortality and morbidity from stroke, heart failure, dementia, and hospitalizations.[1] Due to longer life expectancy and better treatment of conditions associated with high AF risk, such as heart failure, the prevalence and incidence of AF have been continuously rising.[2]
Stroke prevention is central to AF management, and multiple oral anticoagulant (OAC) drugs are recommended. These are categorized in two broad classes[3]: (i) vitamin K antagonists (VKAs), which reduce the synthesis of functional coagulation factors; and (ii) direct oral anticoagulants (DOACs), which inhibit the action of certain coagulation factors. In the trials comparing VKAs with placebo, OAC reduced the risk of stroke by 64% and all-cause mortality by 26%.[4] However, in Europe and North America, VKAs have been almost entirely replaced by DOACs in the management of AF patients without significant valvular heart disease. In a meta-analysis of trials comparing VKA with DOACs, involving more than 70,000 patients with AF, treatment with DOACs was associated with a significant reduction in all strokes by 19%, which was mainly driven by a significant reduction in hemorrhagic stroke (Hazard Ratio [HR] 0.49, 95% confidence interval [CI] 0.38–0.64).[5] In the trials, the risk of major bleeding in the gastrointestinal (GI) tract is not much reduced in comparison to VKAs, and may actually be increased as compared with VKAs with some DOACs. There remains a residual risk of stroke in 0.8 per 100 patient-years.[6]
Nonetheless, anticoagulants generally increase the risk of bleeding; thus, doctors, patients, and caregivers are sometimes reluctant to use them, especially in more clinically complex patients.[7]
Although the balance between stroke prevention and major bleeding is improved with DOACs, the bleeding problem is not eliminated.[8] The major bleeding rate remains between 1 and 3 per 100 patient-years, but over a 3-year period it was 11% in an LAAC/OAC meta-analysis and in the DOAC versus VKA pre-approval trials it was 5.9% with DOACs over 32 months.[9] In AF patients with a GI bleed on anticoagulant there is a very high risk of a recurrent bleed (27 per 100 patient-years).[10] In some situations of severe bleeds (e.g., intracranial hemorrhage [ICH]) there remains treatment uncertainty.[11] Indeed, any bleeding is a “red flag” for adverse outcomes in such high-risk patients, yet OAC is often discontinued leading to worse outcomes.[12]
In patients who have suffered serious bleeding and/or are at high risk of bleeding or in whom VKA/DOAC treatment has failed to prevent AF-related stroke, there is increasing use of interventional techniques. Closure or occlusion of the left atrial (LA) appendage,[13] the intra-cardiac site at which most thrombi form in patients with AF, can be achieved by a reasonably safe catheter-based procedure known as LA appendage closure (LAAC) or LA appendage occlusion (LAAO). However, knowledge of LAAC is often limited outside the interventional cardiology and electrophysiology communities.
Patients with AF who might benefit from this therapeutic approach are often under the care of a general cardiologist, general or primary care physician, gerontologist, nephrologist, gastroenterologist, neurologist or stroke physician, etc. An understanding and appreciation of the value and applicability of LAAC are needed by all of those who care for patients with AF at risk of stroke but with a medical history, comorbidity, or lifestyle that prevents adequate long-term anticoagulation.
This is an executive summary of a practical guide for the non-implanting physician, written by an international multidisciplinary expert group consisting of members of the European Society of Cardiology Council on Stroke and physicians from other interested specialties. This practical guide is not meant to be a manual for those who implant the device. The full document has been published in Europace,[14] and the current executive summary provides the salient points from the full document.
Evidence Base for LAAC
The efficacy and safety of LAAC were first shown in the randomized PROTECT-AF (data collection from 2005) and PREVAIL (data collection from 2010) clinical trials in which AF patients without obvious contraindications to warfarin were randomized to either LAAC with Watchman (with warfarin and aspirin for at least 45 days after the procedure) or warfarin aiming at an international normalized ratio (INR) of 2 to 3 (n = 1114). After a 5-year follow-up, LAAC provided stroke prevention comparable to VKA with a significant reduction in major bleeding, hemorrhagic stroke, disabling/fatal stroke, cardiovascular death, and all-cause death.[15]
The PRAGUE-17 randomized trial (data collection from 2015) compared LAAC (Amulet or Watchman) with DOAC, mainly apixaban, (n = 402) showing noninferiority for LAAC in the prevention of stroke/transient ischemic attack (TIA), cardiovascular death, and clinically relevant bleeding and superiority in preventing nonprocedural bleeding over 4 years.[16]
[Fig. 1] shows clinical outcomes from the three RCTs comparing LAAC versus VKA/DOAC.[17] It can be seen that the point estimate for the ischemic stroke rate is 5.6% with LAAC compared with 3.6% with OAC. This adverse trend is not significant but it is a concern that detracts from a more extensive acceptance of LAAC therapy as a legitimate alternative to OAC prophylaxis. One propensity-matched analysis has suggested that strokes in patients with LAAC are less disabling than those seen in patients receiving DOAC therapy.[18]

There are multiple observational studies and registries of AF patients undergoing LAAC with various devices (ACP, Amulet, Watchman, Watchman FLX), mostly showing a 60 to 80% reduction in the rate of ischemic stroke and major bleeding compared with predicted rates based on the CHA2DS2-VASc and HAS-BLED score values (e.g., ACP registry,[19] Amulet Observational Study,[20] EWOLUTION,[21] NCDR-LAAO registry,[22] [23] PINNACLE FLX[24]).
A recent meta-analysis of studies comparing LAAC with DOAC (n = 4411) showed the risk of stroke/TIA to be similar between LAAC and DOAC, whereas LAAC was superior in reducing cardiovascular mortality, and major and non-major bleeding.[25] In the randomized LAAOS-III study (n = 4770), surgical LAAC in addition to DOAC (continued in approximately 70% of all study patients) was associated with a 33% reduction in the risk of stroke/TIA after 3 years.[26] A recent network meta-analysis based on seven RCTs, with overall 73,199 patients, found that both LAAC and DOACs reduced the risk of all-cause death compared with VKAs, with LAAC ranked as the best treatment for reducing major bleeding and death, while DOACs emerged as the best treatment for preventing stroke or systemic embolism.[27]
Factor XI inhibitors are currently being investigated for thromboprophylaxis in AF patients and ongoing trials include OCEANIC-AF and OCEANIC-AFINA with asundexian,[28] AZALEA-TIMI 71[29] and LILAC-TIMI 76 with abelacimab,[30] and LIBREXIA-AF with milvexian and comparing factor XI inhibitors against DOACs or placebo.[31] The OCEANIC-AF trial was stopped early due to an excess of stroke and thromboembolism compared with apixaban, although major bleeding was less.[32] Pending other ongoing trial data showing these new drugs can prevent thromboembolism without a substantial bleeding risk, a comparison with LAAC will be needed. Of note, the AZALEA trial was also terminated prematurely but because there was substantially less bleeding with abelacimab than with rivaroxaban.
Currently, there are no RCT-based data on LAAC in patients who are intolerant of or contraindicated for OAC, who are a subgroup of AF patients treated with LAAC in clinical practice today and the subgroup that would likely have the greatest benefit from LAAC ([Table 1]). Patient recruitment into these trials has been slow, e.g., ASAP-TOO,[33] CLOSURE-AF,[34] STROKECLOSE,[35] CLEARANCE,[36] COMPARE-LAAO,[37] [38] and LAA-KIDNEY[39] among others. The ASAP-TOO trial was terminated prematurely due to slow enrolment but patient follow-up is still active.
|
CLOSURE-AF[34] |
STROKE-CLOSE[35] |
CLEARANCE [36] |
LAA-KIDNEY[39] |
COMPARE LAAO |
|
|---|---|---|---|---|---|
|
Patient population |
AF and high bleeding risk (HAS-BLED ≥3; prior major bleeding) |
AF and ICH within 12 months |
AF and ICH or intracerebral amyloid vasculopathy |
AF and end-stage kidney disease |
NVAF patients with CHA2DS2-VASc ≥2 and absolute contraindication to (D)OAC |
|
Number of patients |
1000 |
600 |
530 |
430 |
609 |
|
Randomization |
LAAC versus best medical care |
Amulet versus best medical care (2:1) |
Watchman FLX versus best medical care |
Amulet versus best medical care |
Amulet or Watchman FLX versus nothing +/− APT (2:1) |
|
Primary endpoint |
Stroke, SE, major bleeding, or CV death at 2 years |
Stroke, SE, major bleeding, or all-cause mortality at 2 years |
Stroke, SE, major bleeding, or CV death at 3 years |
Time to first stroke, SE, CV death, or major bleeding |
• Any stroke. • Composite of stroke, TIA, and SE |
Abbreviations: AF, atrial fibrillation; APT, antiplatelet therapy; CRF; CV, cardiovascular; CHA2DS2-VASc, Congestive heart failure, Hypertension, Age ≥75 years, Diabetes mellitus, Stroke, Vascular disease, Age 65–74 years, Sex category (female); (D)OAC, (direct) oral anticoagulant; ICH, intracerebral bleeding; LAAC, left atrial appendage closure; NVAF, Non-valvular atrial fibrillation; SE, systemic embolism; TIA, transient ischemic attack.
Based on the currently available evidence and clinical experience, LAAC is now being investigated in broad populations of AF patients in large-scale trials. In the OPTION trial,[40] [41] AF patients undergoing catheter ablation for AF were randomized to LAAC or DOAC after ablation. In the CHAMPION-AF trial[42] and CATALYST trial,[43] AF patients with no contraindications to DOACs and CHA2DS2-VASc of ≥2 for men and CHA2DS2-VASc of ≥3 for women are randomized to LAAC or DOAC ([Table 2]). In the OCCLUSION-AF trial[44] AF patients with a recent ischemic stroke are randomized to either LAAC or DOAC.[45]
|
OPTION[41] |
CHAMPION-AF[42] |
CATALYST[43] |
|
|---|---|---|---|
|
Patient population |
CHA2DS2-VASc ≥ 2 (men) CHA2DS2-VASc ≥ 3 (women) |
CHA2DS2-VASc ≥ 2 (men) CHA2DS2-VASc ≥ 3 (women) |
CHA2DS2-VASc ≥ 3 initially, now updated to CHA2DS2-VASc ≥ 2 (men) CHA2DS2-VASc ≥ 3 (women) |
|
Number of patients |
1600 |
3000 |
2650 |
|
Randomization |
WM FLX vs. OAC |
WM FLX vs. DOAC |
Amulet vs. DOAC |
|
Primary endpoint |
Stroke, SE, or death at 3 years (non-inferiority) Major or clinically relevant bleeding at 3 years (superiority) |
Stroke, SE, or CV death at 3 years (non-inferiority) Major or clinically relevant bleeding at 3 years (superiority) |
Stroke, SE, or CV death at 2 years (non-inferiority) Major or clinically relevant bleeding at 2 years (superiority) |
|
Enrolment status |
Completed |
Completed |
Enrolling |
Abbreviations: CV, cardiovascular; CHA2DS2-VASc, Congestive heart failure, Hypertension, Age ≥75 years, Diabetes mellitus, Stroke, Vascular disease, Age 65–74 years, Sex category (female); DOAC, direct oral anticoagulant; LAAC, left atrial appendage closure; SE, systemic embolism; WM FLX, Watchman FLX.
There are also several observational studies on special AF patient subpopulations undergoing LAAC (i.e., patients with prior ICH, prior ischemic stroke, renal failure, stroke despite anticoagulation) suggesting a net benefit of LAAC in the prevention of stroke and bleeding. Some of those studies are propensity score matched comparing LAAC in AF patients with a prior ICH to standard therapy[46] or LAAC to DOAC.[47]
Indications for LAAC
Stroke reduction in patients with AF requires more than thromboprophylaxis, hence the move toward a holistic or integrated care approach to AF management. Such evidence-based holistic management is recommended in many guidelines including the Atrial fibrillation Better Care (ABC) pathway.[48] [49] Other guidelines have used (untested) variants of the pathway, such as SOS and AF-CARE.[50] [51] A practicing clinician's perspective on recent AF guidelines has recently been published.[52] Adherence to the ABC pathway strategy is associated with a 31% reduction in stroke, as well as lower mortality and bleeding, which is supported by various retrospective and prospective cohort studies from different parts of the world,[53] as well as post-hoc analysis from adjudicated outcomes from clinical trials.[54] [55]
Transcatheter LAAC has been increasingly used as an antithrombotic approach in patients with AF, especially in the United States of America.[22] [56] Although contemporary European AF registry–based studies reported a <1% use of LAAC in clinical practice,[57] [58] a trend toward increasing use of LAAC in Europe has been recently observed, including the changing profile of AF patients undergoing the procedure (i.e., less frail and generally less comorbid patients).[59]
Guideline recommendations and consensus statements on the use of transcatheter LAAC for the prevention of stroke and systemic thromboembolism in patients with AF are summarized in [Tables 3] and [4] and [Fig. 2].
|
Guideline recommendations for transcatheter LAAC for stroke prevention in patients with AF at increased (moderate to high) risk of stroke |
||||
|---|---|---|---|---|
|
Society |
Wording of recommendation |
AF patient group(s) for which LAA closure is recommended |
Class/Strength |
Level of evidence |
|
ACCP 2018[60] |
We suggest |
With absolute contraindications for OAC In ICH survivors at high risk of recurrent ICH (e.g., those with probable cerebral amyloid angiopathy) |
Weak Ungraded |
Low |
|
CSANZ 2018[61] |
May be considered |
With contraindications to OAC |
Strong |
Low |
|
ESC 2020[63] |
May be considered |
With contraindications for long-term OAC (e.g., ICH without a reversible cause) |
IIb |
B |
|
CCS 2020[64] |
We suggest |
With absolute contraindications to OAC |
Weak |
Low |
|
APHRS 2021[48] |
May be considered |
With clear contraindications for long-term OAC (e.g., ICH without a reversible cause) |
NA |
NA |
|
SCAI/HRS[65] |
May be considered |
With contraindications for long-term anticoagulant treatment (e.g., those with a previous life-threatening bleed without reversible cause) |
IIb |
B |
|
ACC/HRS/ ACCP/HRS[140] |
Is reasonable |
With a moderate to high risk of stroke (CHA2DS2-VASc score ≥2), and a contraindication to long-term oral anticoagulation due to a non-reversible cause |
IIa |
B-NR |
|
May be reasonable |
With AF and a moderate to high risk of stroke and a high risk of major bleeding on oral anticoagulation, LAAO may be a reasonable alternative to oral anticoagulation based on patient's preference, with careful consideration of procedural risk and with the understanding that the evidence for oral anticoagulation is more extensive |
IIb |
B-R |
|
|
ESC 2024[51] |
May be considered |
Percutaneous LAA occlusion may be considered in patients with AF and contraindications for long-term anticoagulant treatment to prevent ischemic stroke and thromboembolism |
IIb |
C |
Abbreviations: ACC/AHA/HRS, American College of Cardiology/American Heart Association/Heart Rhythm Society; ACCP, American College of Chest Physicians; AF, atrial fibrillation; APHRS, Asia Pacific Heart Rhythm Society; B-NR, level of evidence B according to non-randomized data; B-R, level of evidence B according to randomized data; CCS, Canadian Cardiovascular Society; CSANZ, Cardiac Society of Australia and New Zealand; ESC, European Society of Cardiology; ICH, intracerebral hemorrhage; INR, international normalized ratio; LAA, left atrial appendage; LAAC, left atrial appendage closure; LAAO, left atrial appendage occlusion; OAC, oral anticoagulant.
|
Consensus statements for percutaneous LAAC for stroke prevention in patients with AF at increased (or moderate to high) risk of stroke |
||
|---|---|---|
|
Group |
Wording of the statement |
Consensus statement |
|
EHRA/EAPCI 2020[66] |
May receive/be considered for |
Patients eligible for long-term OAC Patients who are eligible for long-term OAC may receive an LAAC instead of long-term OAC only if they refuse OAC despite explanation. |
|
May receive/be considered for |
Patients at high risk of bleeding with long-term OAC In patients with an elevated bleeding risk during long-term OAC, LAAC may be considered. |
|
|
May receive/be considered for |
Patients noncompliant to OAC In patients with documented noncompliance, LAAC can be discussed as a therapeutic alternative after attempts to resolve the reasons for noncompliance. |
|
|
Should |
AF patients with CHA2DS2-VASc score ≥2 (3 in females) who have absolute contraindications for long-term OAC may be considered for LAAC if a single antiaggregant can be given for a minimum period (2–4 weeks). In patients with an elevated bleeding risk during long-term OAC (e.g., post-ICH) an individual risk–benefit assessment needs to be performed between OAC and LAAC. Any AF patients with an increased risk for stroke and embolism and no contraindication for OAC should receive personal and detailed advice that according to current evidence long-term OAC treatment is the preferred prophylactic strategy. |
|
|
Should not |
In patients who are opposed to chronic drug intake, LAAC is currently not offered as an equally effective treatment alternative. |
|
|
The Munich consensus document 2017[67] |
Potential indications |
Patient not eligible for long-term OAC therapy (absolute or relative contraindications to OAC), including: • High risk of bleeding (ICH or gastrointestinal bleeding), • History of major or minor bleeding with or without OAC (symptomatic bleeding in critical organ, i.e., ocular, pericardial, spinal cord, or recurrent epistaxis needing medical attention), • Increased risk of bleeding due to a physical condition and/or comorbidities (i.e., recurrent falls with head trauma and significant musculoskeletal injury, need for additional dual antiplatelet therapy for coronary artery disease/stenting, diffuse intracranial amyloid angiopathy, bowel angiodysplasia, severe renal insufficiency/hemodialysis, blood cell dyscrasia), or • Inability to take OAC for reasons other than high risk of bleeding (intolerance, documented poor adherence, documented variability in the INR on VKA, high-risk occupation with increased injury potential, patient's choice). Thromboembolic event or documented presence of thrombus in the LAA despite adequate OAC therapy. |
Abbreviations: AF, atrial fibrillation; CHA2DS2-VASc, Congestive heart failure, Hypertension, Age ≥75 years, Diabetes mellitus, Stroke, Vascular disease, Age 65–74 years, Sex category (female); EAPCI, European Association of Percutaneous Coronary Intervention; EHRA, European Heart Rhythm Association; ICH, intracranial hemorrhage; INR, international normalized ratio; VKA, vitamin K antagonist; LAA, left atrial appendage; LAAC, left atrial appendage closure; OAC, oral anticoagulant.

Formal guideline documents have consistently recommended percutaneous LAAC for AF patients with contraindications to long-term OAC, using a low class of recommendation and low level of evidence, although the 2023 ACC/AHA/ACCP/HRS guidelines have recently upgraded this to a level IIa recommendation and have added a IIb recommendation for LAAO as an alternative to oral anticoagulation ([Table 3]).[48] [50] [60] [61] [62] [63] [64] [65] The 2024 ESC guidelines on AF management maintain a class IIb recommendation for LAAC.[51] Consensus documents explain the recommendations in more detail and extend the implications ([Table 4]),[66] [67] thus also including AF patients who:
-
Suffer from major bleeding events during anticoagulant therapy
-
Have a high risk of nonmodifiable anticoagulant bleeding
-
Had a thromboembolic event or LAA thrombosis while on optimal OAC[68]
-
Refuse or are noncompliant to long-term OAC
-
Undergo catheter ablation with electrical isolation of the LAA
-
Have a procedure involving transseptal puncture and need long-term thromboembolic protection
Methodological differences (rigid interpretation of the evidence base, particularly clinical trials for guidelines, and a less formal process also utilizing observational data for consensus documents) result in official professional society recommendations in guidelines and broader non-official advice in consensus documents.[69]
The most recent consensus documents addressing the use of transcatheter LAAC for the prevention of stroke and systemic embolism in patients with AF emphasize that LAAC should not be routinely offered to patients unwilling to take OAC therapy or who are simply noncompliant with their anticoagulation medication, before providing them with detailed counseling. Careful individual risk–benefit assessment and shared decision-making should be undertaken in each patient[70] ([Practical Box 1]).
|
When to consider referral for LAAC |
|---|
|
AF and significant risk of stroke CHA2DS2VASc ≥2 (men) CHA2DS2VASc ≥3 (women) and: |
|
• History of recurrent or irremediable major bleeding |
|
• Recurrent non-major bleeding |
|
• Predicted high risk of bleeding (HAS-BLED ≥3) |
|
• Bleeding disorder (coagulopathy or angiodysplasia) |
|
• Indication for long-term antiplatelet therapy |
|
• Cerebral microbleeds/amyloid cerebral vasculopathy |
|
• Advanced renal failure including dialysis |
|
• Hepatic failure |
|
• Stroke despite appropriate OAC |
|
• Nonadherence to OAC despite attempts to educate the patient |
|
• Electrically isolated LAA after ablation |
Referral Considerations
Responsibility of the Referring Physician
All patients with AF who are being considered for any cardiac intervention must be assessed by taking a cardiac history relating to the presence of AF, major structural or functional heart disease, potentially reversible causes of bleeding, or alternative causes of stroke besides AF. Routine investigations including 12-lead surface electrocardiogram (ECG) and basic laboratory tests will have been performed before a patient is considered for LAAC therapy.
The need for thromboembolic protection in patients with AF must be firmly established utilizing guideline-recommended risk scores, such as the CHA2DS2-VASc score, or given that female–male differences in contemporary data are less apparent,[71] [72] using the non-sex CHA2DS2-VASc (CHA2DS2-VA) score.[73] [74] Their bleeding risk should also be assessed using a validated structured bleeding risk assessment that addresses modifiable and non-modifiable bleeding risks, such as the HAS-BLED score.
Responsibility of the Implanting Physician
The first responsibility of the interventional specialist is to confirm the indication for LAAC. There is a practical value of holding a multidisciplinary team (MDT) meeting to assess patients who have been or are to be referred for LAAC. As the indication is often for non-cardiac problems (neurological, GI, hematological, renal, etc.) such an MDT can assess patient data at an early stage and achieve consensus on an agreed management plan.[75]
Pre-procedural diagnostic workup usually includes transesophageal echocardiography (TOE) or cardiac computed tomography (CT) to delineate LAA anatomy and suitability for closure, and to rule out LAA thrombosis. LAA thrombosis can also be excluded using TOE or intracardiac echocardiography (ICE) at the beginning of the procedure.[76] In general, the presence of LAA thrombus is considered as a contraindication to LAAC. Nonetheless, several case series of LAAC have been reported in patients with a thrombus present only in the distal part of the LAA[77] (see below).
The selection of a specific LAA closure device and its size will depend on the operator's experience and the LAA anatomy as assessed by preprocedural CT or TOE and by peri-procedural TOE or ICE and selective LAA angiography. Cardiac CT offers a better understanding of LAA anatomy and the most accurate measurements.[78] [79]
If the patient is on a DOAC, the treatment may be stopped 1 day before the procedure (i.e., last dose of rivaroxaban or edoxaban in the morning, or apixaban and dabigatran in the evening before the procedure) without bridging ([Practical Box 2]).
|
Before LAAC at the implanting center |
|---|
|
Clinical examination and biochemistry: rule out infection; assess renal function |
|
Transthoracic Echocardiogram (TTE): LV function, valves, pericardium |
|
Cardiac CT or TOE: LAA anatomy; device selection and size; rule out LAA thrombus |
|
Stop OAC; loading dose of antiplatelets |
|
Intravenous prophylactic antibiotics |
Current Methods of Percutaneous LAA Closure
Procedural Steps
LAAC is a standardized procedure that requires specific training of the implanter and interventional team. It is most often undertaken under general anesthesia and is guided by TOE, but ICE or micro/mini TOE is increasingly used making it possible to perform the procedure with local analgesia and light sedation.
Femoral Venous Puncture
Femoral venous access is usually obtained under ultrasound guidance to reduce the risks of vascular complications.[80] [81] [82] [83] [84]
Transseptal Access
Transseptal puncture is a crucial step to safely access the left atrium and successfully deploy a LAAC device. This technique requires specific training and has a learning curve.
Deployment of the Occluder Inside the LAA
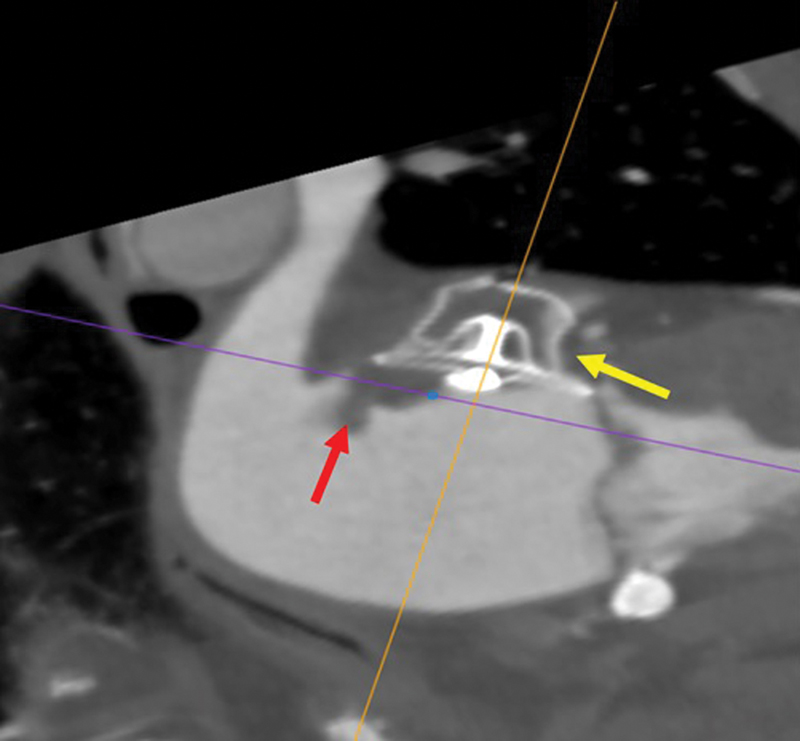
Procedural imaging is of crucial importance for a successful LAAC. The procedure is guided by TOE or ICE, depending on the operator's experience. Device deployment is additionally controlled by fluoroscopy and fusion of preprocedural CT images with fluoroscopy is occasionally used ([Fig. 3]). TOE/ICE is also crucial to confirm the optimal placement of the device and complete sealing of the LAA.

Infective Endocarditis Prophylaxis
Periprocedural antibiotic prophylaxis and standard surgical aseptic measures in the catheter laboratory environment are recommended during the LAA implant procedure (ESC guidelines). Elimination of potential sources of sepsis (including of dental origin) should be considered 2 or more weeks before implantation.[85]
LAAC Devices
A range of devices has been developed to provide safe and efficient LAAC ([Table 5]).[86] [87] [88] [89] [90] [91] Of these the Watchman FLX, Amulet, and LAmbre devices have been extensively studied ([Fig. 4], Panels A, B, and C). Another form of LA occlusion may be achieved using a noose inserted epicardially around the os of the LAAC—the LARIAT device ([Table 3] and [Fig. 5]).
|
Company |
Structure |
Features |
Limitations |
|
|---|---|---|---|---|
|
Watchman FLX ([Fig. 4A]) |
Boston Scientific, Marlborough, Massachusetts, USA |
Endocardial Single component |
High degree of conformability, sealing, and safety |
Shallow LAAs with proximal bifurcation |
|
AMPLATZER Amulet-ACP |
Abbott, St Paul, Minnesota, USA |
Endocardial Dual component |
Possible to seal complex LAA anatomies |
More complex to maneuver |
|
LAmbre |
Lifetech Scientific, Shenzhen, China |
Endocardial Dual component |
Possible to seal complex LAA anatomies |
More complex to maneuver |
|
LARIAT |
SentreHeart, Redwood City, California, USA |
Epicardial suture |
Adjustable size No need for postprocedural OAC |
Both epicardial and endocardial access Postprocedural pericardial pain Not suitable in case of prior cardiac surgery or thoracic radiation |
Abbreviations: LAA, left arial appendage; OAC, oral anticoagulant.


Management of Acute and Early Post-implantation Complications
LAAC has become a relatively low-risk procedure ([Table 6]).[92] [93] [94] [95] Some complications may occur over the longer term, such as late pericardial effusions or device-related thrombosis (DRT), and all physicians following up patients post-procedure must be aware of these.
Abbreviation: LAAC, left atrial appendage closure.
Source: Data were derived from the SURPASS registry of 66.894 Watchman FLX implants performed in the US from August 2020 to March 2022 and from 915 Amulet implants in the randomized Amulet IDE trial 2016–2020.[93] [94] [95]
Pericardial Tamponade
Pericardial effusion or tamponade incidence has decreased from the initially reported rate of 4.3% in the PROTECT AF trial[96] to 0.3% in the SURPASS study that included 16,048 Watchman FLX implants.[93] Most tamponades/effusions occur during the procedure or within 24 hours. To minimize their occurrence, imaging guidance with TOE/ICE is essential for all procedural phases, from transseptal puncture to device placement and release.
LAA perforation can sometimes be managed by just finalizing the LAA device implantation. For significant active pericardial bleeding, autotransfusion is possible to minimize blood loss and the need for transfusion. Reversal of anticoagulation should be considered only in cases with severe hemodynamic deterioration. Surgical intervention is rarely needed ([Table 7]).
Abbreviations: CT, computed tomography; ICE, intracardiac echocardiography; TOE, transesophageal echocardiogram.
Note: The table lists the most frequent mechanisms of pericardial effusion and actions to prevent and manage them.
Although most pericardial effusions occur within 24 hours of LAAC, late pericardial effusions can rarely occur. If a pericardial effusion is suspected, the patient should be immediately referred to the implanting center or the nearest cardiology site for echocardiography and possible pericardiocentesis.
Device Embolization
Device embolization is a rare complication with the most recent LAAC devices (0.01% with WATCHMAN FLX in SURPASS). The risk of embolization is increased with device under-sizing, very proximal implantation, misalignment of the device to the axis of the LAA, and sinus rhythm ([Table 8]). Device embolization can to a large extent be prevented by adequate preprocedural and intra-procedural imaging. Smaller LAAC devices that embolize will most often travel through the left heart and aortic valve to the descending aorta, whereas larger devices will remain in the left atrium or left ventricle. Device embolization is rarely associated with hemodynamic deterioration. Percutaneous retrieval is usually successful with a snare catheter or retrieval forceps ([Fig. 6]). If the device becomes entangled in the mitral valve apparatus, percutaneous snaring can potentially damage the valve and acute surgery might be required.
Abbreviation: LAA, left atrial appendage.

Device-related Thrombosis
The incidence of DRT varies from 2 to 4%, although recent data with newer devices have reported a lower incidence of 1 to 2% per year ([Fig. 7]).[97] [98] [99] [100] [101] [102] [103] [104] [105] [106] DRT is most frequently detected by routine imaging at scheduled follow-up visits after the procedure. It can be diagnosed with TOE or cardiac CT and it is associated with a 4 to 5 times higher risk of stroke/TIA.[107] Besides patient-related risk factors, the risk of DRT can be increased by device implantation that is too deep resulting in incomplete LAA sealing.[108] Hypercoagulability disorders, iatrogenic pericardial effusion, renal failure, and permanent AF are other risk factors for DRT.[107] However, as new devices coated with thromboresistant fluorinated polymers are introduced DRT should become rare and post-implant antithrombotic therapy may be simplified or eliminated.[109]

Management of DRT usually implies escalation of antithrombotic therapy (low molecular weight heparin [LMWH] or DOACs), but this may be challenging or even harmful in patients who are at high bleeding risk. The common practice is to minimize time on anticoagulants until thrombus resolution is verified by imaging ([Figs. 8] and [9]).

Procedure-related Stroke
During early experience, periprocedural stroke occurred occasionally and mainly due to air embolism, but is nowadays rare. In the SURPASS registry, the rate of all-cause stroke was 0.09% in hospital and 0.38% at 45 days.[93] Procedural stroke/TIA may be related to the presence of thrombus/smoke in the LAA or LA, air embolization during the procedure, or development of thrombi on the delivery system or implanted device.
Peri-device Leak (PDL)
The anatomy of the LAA is highly variable and can be very complex, including the landing zone for the LAA device, which is most often non-circular. Consequently, there is a risk of PDL after implantation or in some cases, a smaller lobe of the appendage may not have been occluded by the device.[110] PDL can be diagnosed by TOE or even better with CT. With current procedural techniques and devices, small PDLs are rather frequent, whereas moderate leaks (3–5 mm) are less common and severe leaks (>5 mm) very rare. Medical therapy is usually needed and is chosen according to bleeding risk. For PDL >5 mm, interventional leak closure with plugs, occluders, coils, or radiofrequency (RF) ablation may be considered but medical therapy may also be sufficient ([Figs. 10] and [11])[111] ([Practical Box 3]).
|
LAAC: Benefits, procedure, and periprocedural risk |
|---|
|
Stroke prevention similar to OAC |
|
No need for long-term OAC; reduced risk of bleeding |
|
Procedure performed with local analgesia/light sedation guided by ICE or micro/mini-TEE |
|
Procedure performed with sedation/general anesthesia guided by TEE |
|
Duration of procedure: 30–60 minutes |
|
Procedural risks: |
|
• Pericardial tamponade/effusion: 0.32–2.4% |
|
• Device embolization: 0.01–0.7% |
|
• Stroke: 0.09% |
|
• Death: 0.07% |


Special Populations
There is a large range of medical circumstances in which LAAC therapy may offer an advantage over OAC ([Fig. 12]). Many of these conditions may be associated with severe bleeding complications, ineffectiveness of anticoagulants against thromboembolism, or patient adherence difficulties. Even minor bleeding may have severe effects, for example, patients suffering from cerebral amyloid angiopathy.

Detailed discussion of these “Special Population” scenarios are in [Supplementary Material] (available in the online version). If the use of OAC could be substituted by LAAC, the bleeding risk is mitigated while stroke prevention is retained. Nonetheless, robust long-term data on this population group are lacking.
Anticoagulant/Antiplatelet Therapy Regimens after Left Atrial Appendage Closure
Antithrombotic therapy is required after LAAC to prevent DRT especially in the initial phase, before device endothelization ([Fig. 13]).[70] [112] [113]

Published data on antithrombotic regimens were derived from studies performed on patients who were eligible for anticoagulation (who received VKA or DOAC), as well as from studies performed on patients with intolerance or relative contraindications to anticoagulation, mainly related to prior major bleeding complications (who received antiplatelet therapy).[112]
Clinical RCT data on patients without LAAC have shown that dual antiplatelet therapy with aspirin-clopidogrel had similar major bleeding and ICH rates to warfarin (ACTIVE-W).[114] When aspirin was compared with apixaban in AF patients who refused or were deemed ineligible for warfarin, there was clear superiority of apixaban for the reduction of stroke/SE but the rates of major bleeding and ICH were similar (AVERROES).[115] In the BAFTA trial of elderly (age ≥75 years) AF patients managed in primary care, aspirin monotherapy had similar rates of major bleeding or ICH as warfarin.[116] In elderly AF patients with high-risk features for bleeding, low-dose edoxaban 15 mg was superior for stroke risk reduction, with a nonsignificant difference in major bleeding or ICH to placebo, although major GI bleeding was increased with edoxaban (ELDERCARE-AF).[117]
In practice, after LAAC there is a need to tailor the antithrombosis regimen according to the patient. The best antithrombotic therapy after LAAC needs to provide a balance between the prevention of DRT and the occurrence of major bleeding. The rationale for choosing between the available options ([Table 9] and [Fig. 14]) should be based on physician's assessment of individual patient characteristics, such as bleeding risk and stroke risk, an overall clinical evaluation of the patient's condition, comorbidities, and preference, as well as an evaluation of the reasons for LAAC.[69] [70] [118] As reported in [Table 9], discontinuations of OAC or antiplatelet therapy after LAAC is subject to the absence of other clinical indications for that medication and an assessment, including proper imaging (TOE or CT), demonstrating that there are no significant PDLs (>5 mm), thrombus on the device, or recent history of clinical events. Currently accepted antithrombotic regimens are illustrated in [Fig. 14].
Abbreviations: DOAC, direct oral anticoagulation; INR, international normalized ratio; LAAC, left atrial appendage closure; VKA, vitamin K antagonist.
Note: *OAC schemes are not recommended with the Amulet device unless residual flow around the device is >5 mm.

[Table 9] lists of the main antithrombotic schemes used after LAAC.
In a pooled analysis of data from patients in the PROTECT-AF, PREVAIL, CAP, CAP2, ASAP, and EWOLUTION studies, patients receiving either OACs or antiplatelets post-LAAC implant were matched and compared with regard to the occurrence of nonprocedural bleeding and stroke/systemic thromboembolism over 6 months following implantation. Although DRT was more frequently observed with antiplatelet therapy, the occurrence of major bleeding and stroke/systemic thromboembolism was similar between regimens based on antiplatelets or OAC.[119] [Fig. 14] shows various manufacturer recommendations and less “official” strategies for thrombotic therapy post implant.[120] [121] [122] [123] [124] [125] [126] [127] [128] [129] [130] [131] [132] [133]
Observational data from the years 2016 to 2018 in the United States highlighted how the antithrombotic regimen approved by the FDA for use of the Watchman device was rarely applied.[122] In particular, discharge after implantation on VKA or DOAC without concomitant aspirin was common and associated with lower risk of adverse outcomes. Updated data were presented at the HRS conference in 2023, confirming this finding.[123] In a recent meta-analysis comparing initial antithrombotic therapy following LAAO, monotherapy with DOAC had the highest likelihood of lower thromboembolic events and major bleeding.[124]
A simplified regimen with a short period (2–4 weeks) of a single antiplatelet (ASA or clopidogrel) has also been applied to very select patients with an extremely high bleeding risk on the basis of expert consensus,[70] and reported in observational studies.[125] [126] [127] Additional data on this approach may become available from the CLOSURE-AF[34] and the ARMYDA-Amulet[128] ongoing studies.
Limited but promising observational data are available on post-LAAC treatment with low-dose DOACs, showing reduction of DRT, thromboembolism, and major bleeding events compared with a standard, antiplatelet-based antithrombotic therapy.[129] [130] However, further controlled data are required to assess the value of this strategy. The small, randomized ADALA trial[131] aimed to compare long-term low-dose DOAC therapy (apixaban 2.5 mg twice daily) to a standard dual antiplatelet therapy scheme. The study was terminated after a planned interim analysis showed a significant reduction of bleedings and DRT at 3 months post-implant in the low-dose DOAC arm.[132] The larger ongoing randomized ANDES trial[133] may confirm these preliminary findings.
Post-Discharge LAAC Patient Follow-up
In clinical studies, assessment of the patient's clinical status as well as of the antithrombotic medication was performed 6 months after the implant. In clinical routine, this is less common.
After 1 year of LAAC, a large majority of patients reduce the antithrombotic regimen to a single agent or stop this therapy. In controlled clinical studies TOE imaging was mandatory at the 12-month follow-up visit, although this is rarely done in clinical practice. It was noted that, depending on the device type and the medication used, not uncommonly DRT may occur late after implantation.[134] This may be associated with an increased risk for stroke during long-term follow-up.[135]
Similarly, the presence of PDL at the 12-month imaging contributes to an increased rate of stroke.[136] [137] Both scenarios, DRT as well as PDL, have an impact on the future medical management of the patient. Therefore, it may be advisable to incorporate routine imaging at the 12-month follow-up visit, which is not a common practice in many centers.
In clinical studies with long-term follow-up, patient management beyond 1 year was usually limited to routine clinical assessment. Depending on comorbidities, it seems appropriate to tailor the individual follow-up schedule to the individual risk profile depending on co-existing medical conditions (e.g., every 6–12 months). Specific device-related imaging is not recommended.
In case of adverse clinical events such as stroke, unscheduled visits including imaging for DRT or PDL should be considered ([Practical Box 4]).
|
After LAAC: Postprocedural risk, medication, and follow-up |
|---|
|
Same-day procedure or short hospitalization stay |
|
TTE before discharge: Device position and screening for pericardial effusion |
|
Cardiac CT or TEE: 45 days to 3 months; screening for DRT and PDL |
|
Device-related thrombosis (DRT): 0.23–2.2% |
|
Peri-device leak (PDL): <3 mm: 12.9–27%; 3–5 mm: 3.7–9%; >5 mm: 0.4–1% |
|
Postprocedural medication to reduce risk of DRT: DAPT or OAC 1–3 months, SAPT 6–12 months, reduced-dose DOAC 3–12 months (depending on risk for DRT and bleeding) |
|
Endocarditis prophylaxis 6 months |
Other Cardiac Procedures after Left Atrial Appendage Closure
Direct Current Cardioversion
Direct current cardioversion (DCCV) is frequently used in AF patients as part of a rhythm control strategy. According to current guidelines, patients should be treated by anticoagulation at least 3 weeks before DCCV (AF duration >48 hours) and 4 weeks after to prevent thromboembolic complications. However, patients after LAAC are often at high bleeding risk and therefore unsuitable for anticoagulation before and after DCCV. In two prospectively enrolled patient cohorts involving a total of 242 LAAC patients, DCCV was used effectively without thromboembolic events despite the majority of patients being not on anticoagulant before and after DCCV.[138] [139] In those studies, the majority of patients underwent TOE before DCCV to rule out DRT, large PDLs, device malposition, and other cardiac thrombi.
Currently, the recommendations below can be used as a guide for DCCV in this patient group. There are no specific precautions for pharmacological cardioversion in LAAC patients.
-
DCCV should be avoided the first 3 weeks after LAAC unless there is an acute indication, e.g., acute cardiac decompensation considered to be related to AF.
-
TOE should always be performed before to rule out DRT, large PDL, device malposition, other cardiac thrombi. CT can be used as an alternative to TOE.
-
DCCV can be performed without anticoagulation before and after.
-
Anticoagulation can be considered before and after DCCV in patients with a predicted very high risk of thromboembolic events (severe left atrial dilatation, pronounced spontaneous contrast or sludge in the left atrium, left ventricular ejection fraction (LVEF) <25%, high CHA2DS2-VASc score etc.) depending on an individual assessment of bleeding risk. Recent ACC/AHA/ACCP/HRS guidelines recommend (CoR: IIb, LOE: N-BR) pre-cardioversion imaging for LAAO patients who are not anticoagulated, and anticoagulation peri-cardioversion if there is a DRT or PDL.[140]
Atrial Fibrillation Catheter Ablation
AF catheter ablation and all other types of transcatheter cardiac ablation using various energy delivery sources (RF, cryo, or pulsed-field) can be performed in patients after LAAC. TOE should be performed before AF ablation to rule out DRT, and elective ablation should not be performed before the first follow-up imaging after LAAC, which is typically done after 45 days or later. Anticoagulation post-ablation is recommended but adjusted according to the predicted bleeding risk for the individual patient.
Transcatheter Mitral Interventions, Transcatheter Aortic Valve Implantation and Percutaneous Coronary Intervention
Transcatheter mitral interventions, transcatheter aortic valve implantation (TAVI) and percutaneous coronary intervention (PCI), can all be performed in LAAC patients. Elective mitral intervention or TAVI should be planned not earlier than 45 days after LAAC or later, if possible. TOE should be performed before mitral intervention to rule out DRT or malposition of the device. For PCI, there are no specific LAAC-related precautions.
Conclusion
The advice provided is aligned with current guidelines and guidance documents provided by professional societies. A discussion aid for patients and non-implanting healthcare professionals is provided in [Supplementary Material S1] (available in the online version).
For patients with high AF-related stroke risk who cannot be treated with anticoagulants to prevent stroke and other systemic emboli, LAAC is the only option and is often considered in such circumstances. These patients include those with anticoagulant-related major or life-threatening bleeding, a substantial threat of such bleeding in the presence of anticoagulants, failure of anticoagulants to prevent an embolic ischemic stroke, or inability to comply sufficiently with anticoagulation treatment regimens, etc.
LAAC has been shown to be almost as effective and safer than VKA therapy but data comparing DOACs and LAAC are still insufficient to justify considering LAAC as a valid alternative to DOAC for treatment unless anticoagulation is contraindicated. For the time being LAAC is a second-line therapy. However, many patients may qualify for LAAC treatment, and this Practical Guide is to aid the referral of patients for consideration for LAAC therapy as necessary.
Conflict of Interest
R. B. received personal fees from Bayer, Bristol Myers Squibb, LEO-Pharma, Pfizer, VIATRIS. Research support by the Bavarian State Ministry of Health; CPC University of Colorado; FADOI, Italy. S.Be. received proctor and speaker fees Boston Scientific, Edwards, Abbott, fees go to the Department. L.B. received consultant for Medtronic, Boston Scientific, Adagio and ACUTUS fees go to the Department. G.B. received speaker fees from Bayer, Boehringer Ingelheim, Boston Scientific, Daiichi Sankyo, Janssen, and Sanofi. S.Bo. received consultant for Medtronic, Boston Scientific, Microport, and Zoll. A.J.C. received personal fees from Abbott, Boston Scientific, Medtronic, and Sanofi. W.D. received consulting and speaker fees from Ai Mediq, Bayer, Boehringer Ingelheim, Medtronic, Boston Scientific, Vifor Pharma, travel support from Pharmacosmos, research support from EU (Horizon2020), German Ministry of Education and Research, German Center for Cardiovascular Research, Vifor Pharma. S.G. received consulting and speaker fees from Boston Scientific. M.G. serve as an advisory Board Member for Boston Scientific; Proctor for Boston Scientific, Abbott; Fees for lectures and travel grants: from Boston Scientific, Abbott, Occlutech, Pfizer. K.G.H. received speaker's honoraria, consulting fees, lecture honoraria and/or study grants from Abbott, Amarin; Alexion, AstraZeneca, Bayer Healthcare, Biotronik, Boehringer Ingelheim, Boston Scientific, Bristol-Myers Squibb, Daiichi Sankyo, Edwards Lifesciences, Medtronic, Novartis, Pfizer, Portola, Premier Research, Sanofi, SUN Pharma, and W.L. Gore and Associates. J.E.N.K. received consultant to Boston Scientific, Medtronic, Edwards Lifesciences, Picardia, Venus Medtech, Speaker for Abbott. U.L. received research Grant to Institution from Abbott, Bayer, Speaker or Consulting Honorary from Abbott, Boston Scientific, Bayer; Pfizer, Daiichi Sankyo. G.Y.H.L. received consultant and speaker for BMS/Pfizer, Boehringer Ingelheim, Daiichi-Sankyo, Anthos. No fees are received personally. National Institute for Health and Care Research (NIHR) Senior Investigator and co-principal investigator of the AFFIRMO project on multimorbidity in AF, funded from the European Union's Horizon 2020 research and innovation program under grant agreement No. 899871. J.E.N.K. received research grants Abbott, Boston Scientific, Novo Nordic Foundation JENK: Research grants Abbott, Boston Scientific, Novo Nordic Foundation. E.M. received research grants from Abbott, Biotronik, Boston Scientific, Medtronic, MicroPort and Zoll. Consultant and speaker fees from Abbott, Abbott, Medtronic, and Zoll. J.E.N.K. received research grants Abbott, Boston Scientific, Novo Nordic Foundation. P.O. received speaking honoraria from Bayer, Abbott, Boston Scientific. B.S. received consultant and Speaker for Bostin Scientific, Abbott, Medtronic, Biosense Webster. R.B.S. received funding from the European Research Council (ERC) under the European Union's Horizon 2020 research and innovation program under the grant agreement No. 648131, from the European Union's Horizon 2020 research and innovation program under the grant agreement No. 847770 (AFFECT-EU) and German Center for Cardiovascular Research (DZHK e.V.) (81Z1710103 and 81Z0710114); German Ministry of Research and Education (BMBF 01ZX1408A) and ERACoSysMed3 (031L0239). Wolfgang Seefried project funding German Heart Foundation, Lecture fees and advisory board fees from BMS/Pfizer and Novartis outside this work. C.T. serves as an advisory Board Member of Boston Scientific; Proctor for Boston Scientific and Abbott. Fees for lectures and travel grants from Boston Scientific and Abbott. A portion of the fees goes to the institute. A.T. received consultant and proctor for Abbott, Consultant for Boston Scientific and Pie Medical.
The review process for this paper was fully handled by Christian Weber, Editor in Chief.
-
References
- 1 Linz D, Gawalko M, Betz K. et al. Atrial fibrillation: epidemiology, screening and digital health. Lancet Reg Health Eur 2024; 37: 100786
- 2 Krijthe BP, Kunst A, Benjamin EJ. et al. Projections on the number of individuals with atrial fibrillation in the European Union, from 2000 to 2060. Eur Heart J 2013; 34 (35) 2746-2751
- 3 Chao TF, Potpara TS, Lip GYH. Atrial fibrillation: stroke prevention. Lancet Reg Health Eur 2024; 37: 100797
- 4 Hart RG, Pearce LA, Aguilar MI. Meta-analysis: antithrombotic therapy to prevent stroke in patients who have nonvalvular atrial fibrillation. Ann Intern Med 2007; 146 (12) 857-867
- 5 Ruff CT, Giugliano RP, Braunwald E. et al. Comparison of the efficacy and safety of new oral anticoagulants with warfarin in patients with atrial fibrillation: a meta-analysis of randomised trials. Lancet 2014; 383 (9921): 955-962
- 6 Ray WA, Chung CP, Stein CM. et al. Association of rivaroxaban vs apixaban with major ischemic or hemorrhagic events in patients with atrial fibrillation. JAMA 2021; 326 (23) 2395-2404
- 7 Romiti GF, Proietti M, Bonini N. et al; GLORIA-AF Investigators. Clinical complexity domains, anticoagulation, and outcomes in patients with atrial fibrillation: a report from the GLORIA-AF Registry Phase II and III. Thromb Haemost 2022; 122 (12) 2030-2041
- 8 Marijon E, Le Heuzey JY, Connolly S. et al; RE-LY Investigators. Causes of death and influencing factors in patients with atrial fibrillation: a competing-risk analysis from the randomized evaluation of long-term anticoagulant therapy study. Circulation 2013; 128 (20) 2192-2201
- 9 Carnicelli AP, Hong H, Connolly SJ. et al; COMBINE AF (A Collaboration Between Multiple Institutions to Better Investigate Non-Vitamin K Antagonist Oral Anticoagulant Use in Atrial Fibrillation) Investigators. Direct oral anticoagulants versus warfarin in patients with atrial fibrillation: patient-level network meta-analyses of randomized clinical trials with interaction testing by age and sex. Circulation 2022; 145 (04) 242-255
- 10 Little D, Chai-Adisaksopha C, Hillis C. et al. Resumption of anticoagulant therapy after anticoagulant-related gastrointestinal bleeding: a systematic review and meta-analysis. Thromb Res 2019; 175: 102-109
- 11 Ivany E, Lotto RR, Lip GYH, Lane DA. Managing uncertainty: physicians' decision making for stroke prevention for patients with atrial fibrillation and intracerebral hemorrhage. Thromb Haemost 2022; 122 (09) 1603-1611
- 12 Winijkul A, Kaewkumdee P, Yindeengam A, Lip GYH, Krittayaphong R. Clinical outcomes of patients with atrial fibrillation who survived from bleeding event: the results from COOL-AF Thailand registry. Thromb Haemost 2024; 124 (11) 991-1002
- 13 Karim N, Ho SY, Nicol E. et al. The left atrial appendage in humans: structure, physiology, and pathogenesis. Europace 2020; 22 (01) 5-18
- 14 Potpara T, Grygier M, Häusler KG. et al. Practical guide on left atrial appendage closure for the non-implanting physician: an international consensus paper. Europace 2024; 26 (04) euae035
- 15 Reddy VY, Doshi SK, Kar S. et al; PREVAIL and PROTECT AF Investigators. 5-year outcomes after left atrial appendage closure: from the PREVAIL and PROTECT AF trials. J Am Coll Cardiol 2017; 70 (24) 2964-2975
- 16 Osmancik P, Herman D, Neuzil P. et al; PRAGUE-17 Trial Investigators. 4-year outcomes after left atrial appendage closure versus nonwarfarin oral anticoagulation for atrial fibrillation. J Am Coll Cardiol 2022; 79 (01) 1-14
- 17 Turagam MK, Osmancik P, Neuzil P, Dukkipati SR, Reddy VY. Left atrial appendage closure versus oral anticoagulants in atrial fibrillation: a meta-analysis of randomized trials. J Am Coll Cardiol 2020; 76 (23) 2795-2797
- 18 Turagam MK, Kawamura I, Neuzil P. et al. Severity of ischemic stroke after left atrial appendage closure vs nonwarfarin oral anticoagulants. JACC Clin Electrophysiol 2023
- 19 Tzikas A, Shakir S, Gafoor S. et al. Left atrial appendage occlusion for stroke prevention in atrial fibrillation: multicentre experience with the AMPLATZER Cardiac Plug. EuroIntervention 2016; 11 (10) 1170-1179
- 20 Hildick-Smith D, Landmesser U, Camm AJ. et al. Left atrial appendage occlusion with the Amplatzer™ Amulet™ device: full results of the prospective global observational study. Eur Heart J 2020; 41 (30) 2894-2901
- 21 Boersma LV, Ince H, Kische S. et al; EWOLUTION Investigators. Efficacy and safety of left atrial appendage closure with WATCHMAN in patients with or without contraindication to oral anticoagulation: 1-year follow-up outcome data of the EWOLUTION trial. Heart Rhythm 2017; 14 (09) 1302-1308
- 22 Freeman JV, Varosy P, Price MJ. et al. The NCDR left atrial appendage occlusion registry. J Am Coll Cardiol 2020; 75 (13) 1503-1518
- 23 Price MJ, Slotwiner D, Du C. et al. Clinical outcomes at 1 year following transcatheter left atrial appendage occlusion in the United States. JACC Cardiovasc Interv 2022; 15 (07) 741-750
- 24 Doshi SK, Kar S, Sadhu A. et al; PINNACLE FLX investigators [Link]. Two-year outcomes with a next-generation left atrial appendage device: final results of the PINNACLE FLX trial. J Am Heart Assoc 2023; 12 (04) e026295
- 25 Waranugraha Y, Lin LY, Tsai CT. Head-to-head comparison between left atrial appendage occlusion and non-vitamin K oral anticoagulants in non-valvular atrial fibrillation patients: a systematic review and meta-analysis study. Trends Cardiovasc Med 2023
- 26 Whitlock RP, Belley-Cote EP, Paparella D. et al; LAAOS III Investigators. Left atrial appendage occlusion during cardiac surgery to prevent stroke. N Engl J Med 2021; 384 (22) 2081-2091
- 27 Oliva A, Ioppolo AM, Chiarito M. et al. Left atrial appendage closure compared with oral anticoagulants for patients with atrial fibrillation: a systematic review and network meta-analysis. J Am Heart Assoc 2024; 13 (16) e034815
- 28 Bayer. A Study to Learn How Well the Study Treatment Asundexian Works and How Safe it is Compared to Apixaban to Prevent Stroke or Systemic Embolism in People with Irregular and Often Rapid Heartbeat (Atrial Fibrillation), and at Risk for Stroke (OCEANIC-AF). 2022. Accessed at: https://classic.clinicaltrials.gov/show/NCT05643573
- 29 Anthos Therapeutics Inc., The TIMI Study Group. Laboratory Corporation of America. Safety and Tolerability of Abelacimab (MAA868) vs. Rivaroxaban in Patients with Atrial Fibrillation (AZALEA-TIMI 71). 2021. Accessed at: https://classic.clinicaltrials.gov/show/NCT04755283
- 30 Anthos Therapeutics Inc. Study to Evaluate the Efficacy and Safety of AbeLacimab in High-Risk Patients with Atrial Fibrillation Who Have Been Deemed Unsuitable for Oral Anticoagulation (LILAC-TIMI 76). 2022. Accessed at: https://classic.clinicaltrials.gov/show/NCT05712200
- 31 Janssen Research Development LLC. Bristol-Myers Squibb. A Study of Milvexian Versus Apixaban in Participants with Atrial Fibrillation (LIBREXIA-AF). 2023. Accessed at: https://classic.clinicaltrials.gov/show/NCT05757869
- 32 Piccini JP, Patel MR, Steffel J. et al; OCEANIC-AF Steering Committee and Investigators. Asundexian versus apixaban in patients with atrial fibrillation. N Engl J Med 2024 (e-pub ahead of print)
- 33 Boston Scientific Corporation. Assessment of the WATCHMAN™ Device in Patients Unsuitable for Oral Anticoagulation (ASAP-TOO). 2017. Accessed at: https://classic.clinicaltrials.gov/show/NCT02928497
- 34 Charite University Berlin Germany, Deutsches Zentrum für Herz-Kreislauf-Forschung, Atrial Fibrillation Network, Stiftung Institut fuer Herzinfarktforschung. Left Atrial Appendage CLOSURE in Patients with Atrial Fibrillation Compared to Medical Therapy (CLOSURE-AF). 2018. Accessed at: https://classic.clinicaltrials.gov/show/NCT03463317
- 35 Karolinska Institutet, Abbott Medical Devices. Prevention of Stroke by Left Atrial Appendage Closure in Atrial Fibrillation Patients After Intracerebral Hemorrhage. 2017. Accessed at: https://classic.clinicaltrials.gov/show/NCT02830152
- 36 Jena University Hospital. Comparison of LAA-Closure vs Oral Anticoagulation in Patients with NVAF and Status Post Intracranial Bleeding. 2020. Accessed at: https://classic.clinicaltrials.gov/show/NCT04298723
- 37 Huijboom M, Maarse M, Aarnink E. et al. COMPARE LAAO: rationale and design of the randomized controlled trial “COMPARing Effectiveness and safety of Left Atrial Appendage Occlusion to standard of care for atrial fibrillation patients at high stroke risk and ineligible to use oral anticoagulation therapy.”. Am Heart J 2022; 250: 45-56
- 38 R&D Cardiologie, Research ZTNOfH, Development. Left Atrial Appendage Occlusion for AF Patients Unable to Use Oral Anticoagulation Therapy (COMPARE-LAAO). 2021. Accessed at: https://classic.clinicaltrials.gov/show/NCT04676880
- 39 Eitel I. Left Atrial Appendage Closure in Patients with Non-valvular Atrial Fibrillation and End-stage Chronic KIDNEY Disease (LAA-KIDNEY). 2022. Accessed at: https://classic.clinicaltrials.gov/show/NCT05204212
- 40 Wazni OM, Boersma L, Healey JS. et al. Comparison of anticoagulation with left atrial appendage closure after atrial fibrillation ablation: rationale and design of the OPTION randomized trial. Am Heart J 2022; 251: 35-42
- 41 Boston Scientific Corporation. Comparison of Anticoagulation with Left Atrial Appendage Closure After AF Ablation (OPTION). 2019. Accessed at: https://classic.clinicaltrials.gov/show/NCT03795298
- 42 Kar S, Doshi SK, Alkhouli M. et al. Rationale and design of a randomized study comparing the Watchman FLX device to DOACs in patients with atrial fibrillation. Am Heart J 2023; 264: 123-132
- 43 Abbott Medical Devices. Amplatzer Amulet LAAO vs. NOAC (CATALYST). 2020. Accessed at: https://classic.clinicaltrials.gov/show/NCT04226547
- 44 University of Aarhus, Aarhus University Hospital, Aalborg University Hospital, Odense University Hospital, Sahlgrenska University Hospital Sweden, Karolinska University Hospital, et al. Left Atrial Appendage Occlusion Versus Novel Oral Anticoagulation for Stroke Prevention in Atrial Fibrillation (Occlusion-AF). 2019. Accessed at: https://classic.clinicaltrials.gov/show/NCT03642509
- 45 Korsholm K, Damgaard D, Valentin JB. et al. Left atrial appendage occlusion vs novel oral anticoagulation for stroke prevention in atrial fibrillation: rationale and design of the multicenter randomized occlusion-AF trial. Am Heart J 2022; 243: 28-38
- 46 Nielsen-Kudsk JE, Johnsen SP, Wester P. et al. Left atrial appendage occlusion versus standard medical care in patients with atrial fibrillation and intracerebral haemorrhage: a propensity score-matched follow-up study. EuroIntervention 2017; 13 (03) 371-378
- 47 Nielsen-Kudsk JE, Korsholm K, Damgaard D. et al. Clinical outcomes associated with left atrial appendage occlusion versus direct oral anticoagulation in atrial fibrillation. JACC Cardiovasc Interv 2021; 14 (01) 69-78
- 48 Chao TF, Joung B, Takahashi Y. et al. 2021 focused update consensus guidelines of the Asia Pacific Heart Rhythm Society on stroke prevention in atrial fibrillation: executive summary. Thromb Haemost 2022; 122 (01) 20-47
- 49 Wang Y, Guo Y, Qin M. et al; Expert Reviewers. 2024 Chinese expert consensus guidelines on the diagnosis and treatment of atrial fibrillation in the elderly, endorsed by Geriatric Society of Chinese Medical Association (Cardiovascular Group) and Chinese Society of Geriatric Health Medicine (Cardiovascular Branch): executive summary. Thromb Haemost 2024; 124 (10) 897-911
- 50 Joglar JA, Chung MK, Armbruster AL. et al; Writing Committee Members. 2023 ACC/AHA/ACCP/HRS guideline for the diagnosis and management of atrial fibrillation: a report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. J Am Coll Cardiol 2024; 83 (01) 109-279
- 51 Van Gelder IC, Rienstra M, Bunting KV. et al; ESC Scientific Document Group. 2024 ESC guidelines for the management of atrial fibrillation developed in collaboration with the European Association for Cardio-Thoracic Surgery (EACTS). Eur Heart J 2024; 45 (36) 3314-3414
- 52 Potpara T, Romiti GF, Sohns C. The 2024 European Society of Cardiology guidelines for diagnosis and management of atrial fibrillation: a viewpoint from a practicing clinician's perspective. Thromb Haemost 2024
- 53 Romiti GF, Pastori D, Rivera-Caravaca JM. et al. Adherence to the “Atrial Fibrillation Better Care” pathway in patients with atrial fibrillation: impact on clinical outcomes—a systematic review and meta-analysis of 285,000 patients. Thromb Haemost 2022; 122 (03) 406-414
- 54 Patel SM, Palazzolo MG, Murphy SA. et al. Evaluation of the atrial fibrillation better care pathway in the ENGAGE AF-TIMI 48 trial. Europace 2022; 24 (11) 1730-1738
- 55 Proietti M, Romiti GF, Olshansky B, Lane DA, Lip GYH. Comprehensive management with the ABC (Atrial Fibrillation Better Care) pathway in clinically complex patients with atrial fibrillation: a post hoc ancillary analysis from the AFFIRM trial. J Am Heart Assoc 2020; 9 (10) e014932
- 56 Shrestha B, Poudel B, Poudel D, Diaz Fraga J. National yearly trend of utilization and procedural complication of the Watchman device in the United States. Cureus 2022; 14 (06) e25567
- 57 Boriani G, Proietti M, Laroche C. et al; EORP-AF Long-Term General Registry Investigators. Association between antithrombotic treatment and outcomes at 1-year follow-up in patients with atrial fibrillation: the EORP-AF General Long-Term Registry. Europace 2019; 21 (07) 1013-1022
- 58 Potpara TS, Dan GA, Trendafilova E. et al; BALKAN-AF Investigators. Stroke prevention in atrial fibrillation and “real world” adherence to guidelines in the Balkan Region: the BALKAN-AF survey. Sci Rep 2016; 6: 20432
- 59 Juhl Madsen O, Lamberts MK, Fosboel EL, Gislason G, Olesen JB, Strange JE. Trends in percutaneous left atrial appendage occlusion and 1-year mortality: a nationwide cohort study. Eur Heart J 2022; 43 (Suppl. 02) ehac544.2137
- 60 Lip GYH, Banerjee A, Boriani G. et al. Antithrombotic therapy for atrial fibrillation: CHEST guideline and expert panel report. Chest 2018; 154 (05) 1121-1201
- 61 Brieger D, Amerena J, Attia J. et al; NHFA CSANZ Atrial Fibrillation Guideline Working Group. National Heart Foundation of Australia and the Cardiac Society of Australia and New Zealand: Australian clinical guidelines for the diagnosis and management of atrial fibrillation 2018. Heart Lung Circ 2018; 27 (10) 1209-1266
- 62 January CT, Wann LS, Calkins H. et al. 2019 AHA/ACC/HRS focused update of the 2014 AHA/ACC/HRS guideline for the management of patients with atrial fibrillation: a report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Rhythm Society. J Am Coll Cardiol 2019; 74 (01) 104-132
- 63 Hindricks G, Potpara T, Dagres N. et al; ESC Scientific Document Group. 2020 ESC guidelines for the diagnosis and management of atrial fibrillation developed in collaboration with the European Association for Cardio-Thoracic Surgery (EACTS): the task force for the diagnosis and management of atrial fibrillation of the European Society of Cardiology (ESC) developed with the special contribution of the European Heart Rhythm Association (EHRA) of the ESC. Eur Heart J 2021; 42 (05) 373-498
- 64 Andrade JG, Aguilar M, Atzema C. et al; Members of the Secondary Panel. The 2020 Canadian Cardiovascular Society/Canadian Heart Rhythm Society comprehensive guidelines for the management of atrial fibrillation. Can J Cardiol 2020; 36 (12) 1847-1948
- 65 Saw J, Holmes DR, Cavalcante JL. et al. SCAI/HRS expert consensus statement on transcatheter left atrial appendage closure. JACC Cardiovasc Interv 2023; 16 (11) 1384-1400
- 66 Glikson M, Wolff R, Hindricks G. et al. EHRA/EAPCI expert consensus statement on catheter-based left atrial appendage occlusion—an update. EuroIntervention 2020; 15 (13) 1133-1180
- 67 Tzikas A, Holmes Jr DR, Gafoor S. et al. Percutaneous left atrial appendage occlusion: the Munich consensus document on definitions, endpoints, and data collection requirements for clinical studies. Europace 2017; 19 (01) 4-15
- 68 Anic A, Bakovic D, Jurisic Z. et al. Diagnostic and therapeutic pathways for the malignant left atrial appendage: European Heart Rhythm Association physician survey. Europace 2023; 25 (07) 25
- 69 Camm AJ. Leap or lag: left atrial appendage closure and guidelines. Europace 2023; 25 (05) 25
- 70 Glikson M, Wolff R, Hindricks G. et al; ESC Scientific Document Group. EHRA/EAPCI expert consensus statement on catheter-based left atrial appendage occlusion—an update. Europace 2020; 22 (02) 184
- 71 Teppo K, Airaksinen KEJ, Jaakkola J. et al. Ischaemic stroke in women with atrial fibrillation: temporal trends and clinical implications. Eur Heart J 2024; 45 (20) 1819-1827
- 72 Nielsen PB, Brøndum RF, Nøhr AK, Overvad TF, Lip GYH. Risk of stroke in male and female patients with atrial fibrillation in a nationwide cohort. Nat Commun 2024; 15 (01) 6728
- 73 Teppo K, Lip GYH, Airaksinen KEJ. et al. Comparing CHA2DS2-VA and CHA2DS2-VASc scores for stroke risk stratification in patients with atrial fibrillation: a temporal trends analysis from the retrospective Finnish AntiCoagulation in Atrial Fibrillation (FinACAF) cohort. Lancet Reg Health Eur 2024; 43: 100967
- 74 Yoshimura H, Providencia R, Finan C, Schmidt AF, Lip GYH. Refining the CHA2DS2VASc risk stratification scheme: shall we drop the sex category criterion?. Europace 2024; 26 (11) euae280
- 75 National Institute for Health and Clinical Excellence. Percutaneous occlusion of the left atrial appendage in non-valvular atrial fibrillation for the prevention of thromboembolism. 2010; available at: https://www.nice.org.uk/guidance/ipg400/documents/thoracoscopic-exclusion-of-the-left-atrial-appendage-in-atrial-fibrillation-with-or-without-other-cardiac-surgery-for-the-prevention-of-thromboembolism-overview2
- 76 Di Biase L, Briceno DF, Trivedi C. et al. Is transesophageal echocardiogram mandatory in patients undergoing ablation of atrial fibrillation with uninterrupted novel oral anticoagulants? Results from a prospective multicenter registry. Heart Rhythm 2016; 13 (06) 1197-1202
- 77 Lee OH, Kim JS, Pak HN. et al. Feasibility of left atrial appendage occlusion for left atrial appendage thrombus in patients with persistent atrial fibrillation. Am J Cardiol 2018; 121 (12) 1534-1539
- 78 Korsholm K, Berti S, Iriart X. et al. Expert recommendations on cardiac computed tomography for planning transcatheter left atrial appendage occlusion. JACC Cardiovasc Interv 2020; 13 (03) 277-292
- 79 Osmancik P, Herman D, Linkova H, Hozman M, Labos M. A comparison of cardiac computed tomography, transesophageal and intracardiac echocardiography, and fluoroscopy for planning left atrial appendage closure. J Atr Fibrillation 2021; 13 (06) 20200449
- 80 Sharma PS, Padala SK, Gunda S, Koneru JN, Ellenbogen KA. Vascular complications during catheter ablation of cardiac arrhythmias: a comparison between vascular ultrasound guided access and conventional vascular access. J Cardiovasc Electrophysiol 2016; 27 (10) 1160-1166
- 81 Yamagata K, Wichterle D, Roubícek T. et al. Ultrasound-guided versus conventional femoral venipuncture for catheter ablation of atrial fibrillation: a multicentre randomized efficacy and safety trial (ULTRA-FAST trial). Europace 2018; 20 (07) 1107-1114
- 82 Sobolev M, Shiloh AL, Di Biase L, Slovut DP. Ultrasound-guided cannulation of the femoral vein in electrophysiological procedures: a systematic review and meta-analysis. Europace 2017; 19 (05) 850-855
- 83 Brass P, Hellmich M, Kolodziej L, Schick G, Smith AF. Ultrasound guidance versus anatomical landmarks for subclavian or femoral vein catheterization. Cochrane Database Syst Rev 2015; 1 (01) CD011447
- 84 Kupó P, Pap R, Sághy L. et al. Ultrasound guidance for femoral venous access in electrophysiology procedures—systematic review and meta-analysis. J Interv Card Electrophysiol 2020; 59 (02) 407-414
- 85 Delgado V, Ajmone Marsan N, de Waha S. et al; ESC Scientific Document Group. 2023 ESC Guidelines for the management of endocarditis. Eur Heart J 2023; 44 (39) 3948-4042
- 86 Vizzari G, Grasso C, Sardone A. et al. Real-world experience with the new Watchman FLX device: data from two high-volume Sicilian centers. The FLX-iEST registry. Catheter Cardiovasc Interv 2022; 100 (01) 154-160
- 87 Price MJ, Friedman DJ, Du C. et al. Comparative safety of transcatheter LAAO with the first-generation Watchman and next-generation Watchman FLX devices. JACC Cardiovasc Interv 2022; 15 (21) 2115-2123
- 88 Paitazoglou C, Meincke F, Bergmann MW. et al. The ALSTER-FLX registry: 3-month outcomes after left atrial appendage occlusion using a next-generation device, a matched-pair analysis to EWOLUTION. Heart Rhythm 2022; 19 (06) 917-926
- 89 Lakkireddy D, Thaler D, Ellis CR. et al; Amulet IDE Investigators. Outcomes of the roll-in cohort of the Amulet IDE trial of left atrial appendage occlusion. Heart Rhythm O2 2022; 3 (05) 493-500
- 90 Chen S, Chun KRJ, Bordignon S. et al. Left atrial appendage occlusion using LAmbre Amulet and Watchman in atrial fibrillation. J Cardiol 2019; 73 (04) 299-306
- 91 Tilz RR, Fink T, Bartus K. et al. A collective European experience with left atrial appendage suture ligation using the LARIAT+ device. Europace 2020; 22 (06) 924-931
- 92 Betts TR, Grygier M, Nielsen Kudsk JE. et al; FLXibility investigators. Real-world clinical outcomes with a next-generation left atrial appendage closure device: the FLXibility Post-Approval Study. Europace 2023; 25 (03) 914-921
- 93 Bhogal S, Aladin AI, Wermers JP, Morrison N, Gray N, Waksman R. Review of late-breaking trials from CRT 2022. Cardiovasc Revasc Med 2022; 40S: 3-7
- 94 Merdler I, Reddy PK, Bhogal S. et al. Review of late-breaking trials from CRT 2023. Cardiovasc Revasc Med 2023; 53S: S3-S9
- 95 Lakkireddy D, Thaler D, Ellis CR. et al. Amplatzer Amulet left atrial appendage occluder versus Watchman device for stroke prophylaxis (Amulet IDE): a randomized, controlled trial. Circulation 2021; 144 (19) 1543-1552
- 96 Holmes DR, Reddy VY, Turi ZG. et al; PROTECT AF Investigators. Percutaneous closure of the left atrial appendage versus warfarin therapy for prevention of stroke in patients with atrial fibrillation: a randomised non-inferiority trial. Lancet 2009; 374 (9689): 534-542
- 97 Reddy VY, Doshi SK, Sievert H. et al; PROTECT AF Investigators. Percutaneous left atrial appendage closure for stroke prophylaxis in patients with atrial fibrillation: 2.3-year follow-up of the PROTECT AF (Watchman Left Atrial Appendage System for Embolic Protection in Patients with Atrial Fibrillation) trial. Circulation 2013; 127 (06) 720-729
- 98 Bergmann MW, Betts TR, Sievert H. et al. Safety and efficacy of early anticoagulation drug regimens after WATCHMAN left atrial appendage closure: three-month data from the EWOLUTION prospective, multicentre, monitored international WATCHMAN LAA closure registry. EuroIntervention 2017; 13 (07) 877-884
- 99 Berti S, Pastormerlo LE, Rezzaghi M. et al. Left atrial appendage occlusion in high-risk patients with non-valvular atrial fibrillation. Heart 2016; 102 (24) 1969-1973
- 100 Korsholm K, Nielsen KM, Jensen JM, Jensen HK, Andersen G, Nielsen-Kudsk JE. Transcatheter left atrial appendage occlusion in patients with atrial fibrillation and a high bleeding risk using aspirin alone for post-implant antithrombotic therapy. EuroIntervention 2017; 12 (17) 2075-2082
- 101 Landmesser U, Schmidt B, Nielsen-Kudsk JE. et al. Left atrial appendage occlusion with the AMPLATZER Amulet device: periprocedural and early clinical/echocardiographic data from a global prospective observational study. EuroIntervention 2017; 13 (07) 867-876
- 102 Saw J, Tzikas A, Shakir S. et al. Incidence and clinical impact of device-associated thrombus and peri-device leak following left atrial appendage closure with the Amplatzer Cardiac Plug. JACC Cardiovasc Interv 2017; 10 (04) 391-399
- 103 Kar S, Doshi SK, Sadhu A. et al; PINNACLE FLX Investigators. Primary outcome evaluation of a next-generation left atrial appendage closure device: results from the PINNACLE FLX trial. Circulation 2021; 143 (18) 1754-1762
- 104 Ellis CR, Jackson GG, Kanagasundram AN. et al. Left atrial appendage closure in patients with prohibitive anatomy: insights from PINNACLE FLX. Heart Rhythm 2021; 18 (07) 1153-1161
- 105 Korsholm K, Samaras A, Andersen A, Jensen JM, Nielsen-Kudsk JE. The Watchman FLX device: first European experience and feasibility of intracardiac echocardiography to guide implantation. JACC Clin Electrophysiol 2020; 6 (13) 1633-1642
- 106 Paitazoglou C, Bergmann MW, Ince H. et al; theEWOLUTION Investigators. True efficacy of LAA closure: patient outcomes on long-term single-antiplatelet or no therapy: insights from the EWOLUTION registry. J Invasive Cardiol 2022; 34 (05) E348-E355
- 107 Simard T, Jung RG, Lehenbauer K. et al. Predictors of device-related thrombus following percutaneous left atrial appendage occlusion. J Am Coll Cardiol 2021; 78 (04) 297-313
- 108 Cepas-Guillén P, Flores-Umanzor E, Leduc N. et al. Impact of device implant depth after left atrial appendage occlusion. JACC Cardiovasc Interv 2023; 16 (17) 2139-2149
- 109 Saliba WI, Kawai K, Sato Y. et al. Enhanced thromboresistance and endothelialization of a novel fluoropolymer-coated left atrial appendage closure device. JACC Clin Electrophysiol 2023; 9 (8 Pt 2): 1555-1567
- 110 Lakkireddy D, Nielsen-Kudsk JE, Windecker S. et al. Mechanisms, predictors, and evolution of severe peri-device leaks with two different left atrial appendage occluders. Europace 2023; 25 (09) 25
- 111 Della Rocca DG, Murtaza G, Di Biase L. et al. Radiofrequency energy applications targeting significant residual leaks after Watchman implantation: a prospective, multicenter experience. JACC Clin Electrophysiol 2021; 7 (12) 1573-1584
- 112 Chen S, Weise FK, Chun KRJ, Schmidt B. Antithrombotic strategies after interventional left atrial appendage closure: an update. Expert Rev Cardiovasc Ther 2018; 16 (09) 675-678
- 113 Branca L, Tomasoni D, Cimino G. et al. Impact and predictors of device-related thrombus after percutaneous left atrial appendage closure. J Cardiovasc Med (Hagerstown) 2023; 24 (01) 12-19
- 114 Connolly S, Pogue J, Hart R. et al; ACTIVE Writing Group of the ACTIVE Investigators. Clopidogrel plus aspirin versus oral anticoagulation for atrial fibrillation in the Atrial fibrillation Clopidogrel Trial with Irbesartan for prevention of Vascular Events (ACTIVE W): a randomised controlled trial. Lancet 2006; 367 (9526): 1903-1912
- 115 Connolly SJ, Eikelboom J, Joyner C. et al; AVERROES Steering Committee and Investigators. Apixaban in patients with atrial fibrillation. N Engl J Med 2011; 364 (09) 806-817
- 116 Mant J, Hobbs FD, Fletcher K. et al; BAFTA investigators, Midland Research Practices Network (MidReC). Warfarin versus aspirin for stroke prevention in an elderly community population with atrial fibrillation (the Birmingham Atrial Fibrillation Treatment of the Aged Study, BAFTA): a randomised controlled trial. Lancet 2007; 370 (9586): 493-503
- 117 Okumura K, Akao M, Yoshida T. et al; ELDERCARE-AF Committees and Investigators. Low-dose edoxaban in very elderly patients with atrial fibrillation. N Engl J Med 2020; 383 (18) 1735-1745
- 118 Riegler L, Palermi S, Scarafile R. et al. Clinical and multi-modality imaging approach in the selection of patients for left atrial appendage closure. Rev Cardiovasc Med 2021; 22 (04) 1197-1204
- 119 Søndergaard L, Wong YH, Reddy VY. et al. Propensity-matched comparison of oral anticoagulation versus antiplatelet therapy after left atrial appendage closure with WATCHMAN. JACC Cardiovasc Interv 2019; 12 (11) 1055-1063
- 120 Cruz-González I, Trejo-Velasco B. Percutaneous left atrial appendage occlusion in the current practice. Kardiol Pol 2021; 79 (03) 255-268
- 121 Ledwoch J, Sievert K, Boersma LVA. et al; EWOLUTION Investigators. Initial and long-term antithrombotic therapy after left atrial appendage closure with the WATCHMAN. Europace 2020; 22 (07) 1036-1043
- 122 Freeman JV, Higgins AY, Wang Y. et al. Antithrombotic therapy after left atrial appendage occlusion in patients with atrial fibrillation. J Am Coll Cardiol 2022; 79 (18) 1785-1798
- 123 Freeman J, Hsu JC, Kapadia S. et al. Ce-452771–4 outcomes with different postprocedural antithrombotic therapy regimens following left atrial appendage occlusion. Heart Rhythm 2023; 20: S36-S37
- 124 Carvalho PEP, Gewehr DM, Miyawaki IA. et al. Comparison of initial antithrombotic regimens after left atrial appendage occlusion: a systematic review and network meta-analysis. J Am Coll Cardiol 2023; 82 (18) 1765-1773
- 125 Mhanna M, Beran A, Al-Abdouh A. et al. Single versus dual antiplatelet therapy following left atrial appendage occlusion in patients with high bleeding risk. Curr Probl Cardiol 2022; 47 (09) 101269
- 126 Vignali L, Gurgoglione FL, Barocelli F. et al. Looking for optimal antithrombotic strategy after transcatheter left atrial appendage occlusion: a real-world comparison of different antiplatelet regimens. Int J Cardiol 2023; 371: 92-99
- 127 Rodriguez-Gabella T, Nombela-Franco L, Regueiro A. et al. Single antiplatelet therapy following left atrial appendage closure in patients with contraindication to anticoagulation. J Am Coll Cardiol 2016; 68 (17) 1920-1921
- 128 Azienda Ospedaliero Universitaria Maggiore della Carita, Abbott Medical Devices. Head-to-head Comparison of Single Versus Dual Antiplatelet Treatment Strategy After Percutaneous Left Atrial Appendage Closure: A Multicenter, Randomized Study (ARMYDA-AMULET). 2021. Accessed at: https://classic.clinicaltrials.gov/show/NCT05554822
- 129 Cepas-Guillen PL, Flores-Umanzor E, Regueiro A. et al. Low dose of direct oral anticoagulants after left atrial appendage occlusion. J Cardiovasc Dev Dis 2021; 8 (11) 8
- 130 Della Rocca DG, Magnocavallo M, Di Biase L. et al. Half-dose direct oral anticoagulation versus standard antithrombotic therapy after left atrial appendage occlusion. JACC Cardiovasc Interv 2021; 14 (21) 2353-2364
- 131 Freixa X. Apixaban vs Dual Antiplatet Therapy Study After Left Atrial Appendage Occlosure (ADALA). 2019 Accessed at: https://classic.clinicaltrials.gov/show/NCT05632445
- 132 Freixa X, Cruz-González I, Cepas-Guillén P. et al. Low dose direct oral anticoagulation vs. DAPT after LAAO. Euro PCR 2023
- 133 Centre de Recherche de l'Institut Universitaire de Cardiologie et de Pneumologie de Quebec, Institut universitaire de cardiologie et de pneumologie de Québec University Laval. Short-Term Anticoagulation Versus Antiplatelet Therapy for Preventing Device Thrombosis Following Left Atrial Appendage Closure (ANDES). 2018. Accessed at: https://classic.clinicaltrials.gov/show/NCT03568890
- 134 Schmidt B, Nielsen-Kudsk JE, Ellis CR. et al. Incidence, predictors, and clinical outcomes of device-related thrombus in the Amulet IDE trial. JACC Clin Electrophysiol 2023; 9 (01) 96-107
- 135 Dukkipati SR, Kar S, Holmes DR. et al. Device-related thrombus after left atrial appendage closure: incidence, predictors, and outcomes. Circulation 2018; 138 (09) 874-885
- 136 Dukkipati SR, Holmes Jr DR, Doshi SK. et al. Impact of peridevice leak on 5-year outcomes after left atrial appendage closure. J Am Coll Cardiol 2022; 80 (05) 469-483
- 137 Alkhouli M, Du C, Killu A. et al. Clinical impact of residual leaks following left atrial appendage occlusion: insights from the NCDR LAAO registry. JACC Clin Electrophysiol 2022; 8 (06) 766-778
- 138 Sharma SP, Turagam MK, Gopinathannair R. et al. Direct current cardioversion of atrial fibrillation in patients with left atrial appendage occlusion devices. J Am Coll Cardiol 2019; 74 (18) 2267-2274
- 139 Maarse M, Wintgens LIS, Ponomarenko A. et al. Impact of anticoagulation strategy after left atrial appendage occlusion in patients requiring direct current cardioversion. J Cardiovasc Electrophysiol 2021; 32 (03) 737-744
- 140 Joglar JA, Chung MK, Armbruster AL. et al. ACC/AHA/ACCP/HRS guideline for the diagnosis and management of atrial fibrillation: a report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation 2024; 149 (01) e1-e156
Address for correspondence
Publication History
Received: 12 November 2024
Accepted: 14 November 2024
Article published online:
10 December 2024
© 2024. Thieme. All rights reserved.
Georg Thieme Verlag KG
Oswald-Hesse-Straße 50, 70469 Stuttgart, Germany
-
References
- 1 Linz D, Gawalko M, Betz K. et al. Atrial fibrillation: epidemiology, screening and digital health. Lancet Reg Health Eur 2024; 37: 100786
- 2 Krijthe BP, Kunst A, Benjamin EJ. et al. Projections on the number of individuals with atrial fibrillation in the European Union, from 2000 to 2060. Eur Heart J 2013; 34 (35) 2746-2751
- 3 Chao TF, Potpara TS, Lip GYH. Atrial fibrillation: stroke prevention. Lancet Reg Health Eur 2024; 37: 100797
- 4 Hart RG, Pearce LA, Aguilar MI. Meta-analysis: antithrombotic therapy to prevent stroke in patients who have nonvalvular atrial fibrillation. Ann Intern Med 2007; 146 (12) 857-867
- 5 Ruff CT, Giugliano RP, Braunwald E. et al. Comparison of the efficacy and safety of new oral anticoagulants with warfarin in patients with atrial fibrillation: a meta-analysis of randomised trials. Lancet 2014; 383 (9921): 955-962
- 6 Ray WA, Chung CP, Stein CM. et al. Association of rivaroxaban vs apixaban with major ischemic or hemorrhagic events in patients with atrial fibrillation. JAMA 2021; 326 (23) 2395-2404
- 7 Romiti GF, Proietti M, Bonini N. et al; GLORIA-AF Investigators. Clinical complexity domains, anticoagulation, and outcomes in patients with atrial fibrillation: a report from the GLORIA-AF Registry Phase II and III. Thromb Haemost 2022; 122 (12) 2030-2041
- 8 Marijon E, Le Heuzey JY, Connolly S. et al; RE-LY Investigators. Causes of death and influencing factors in patients with atrial fibrillation: a competing-risk analysis from the randomized evaluation of long-term anticoagulant therapy study. Circulation 2013; 128 (20) 2192-2201
- 9 Carnicelli AP, Hong H, Connolly SJ. et al; COMBINE AF (A Collaboration Between Multiple Institutions to Better Investigate Non-Vitamin K Antagonist Oral Anticoagulant Use in Atrial Fibrillation) Investigators. Direct oral anticoagulants versus warfarin in patients with atrial fibrillation: patient-level network meta-analyses of randomized clinical trials with interaction testing by age and sex. Circulation 2022; 145 (04) 242-255
- 10 Little D, Chai-Adisaksopha C, Hillis C. et al. Resumption of anticoagulant therapy after anticoagulant-related gastrointestinal bleeding: a systematic review and meta-analysis. Thromb Res 2019; 175: 102-109
- 11 Ivany E, Lotto RR, Lip GYH, Lane DA. Managing uncertainty: physicians' decision making for stroke prevention for patients with atrial fibrillation and intracerebral hemorrhage. Thromb Haemost 2022; 122 (09) 1603-1611
- 12 Winijkul A, Kaewkumdee P, Yindeengam A, Lip GYH, Krittayaphong R. Clinical outcomes of patients with atrial fibrillation who survived from bleeding event: the results from COOL-AF Thailand registry. Thromb Haemost 2024; 124 (11) 991-1002
- 13 Karim N, Ho SY, Nicol E. et al. The left atrial appendage in humans: structure, physiology, and pathogenesis. Europace 2020; 22 (01) 5-18
- 14 Potpara T, Grygier M, Häusler KG. et al. Practical guide on left atrial appendage closure for the non-implanting physician: an international consensus paper. Europace 2024; 26 (04) euae035
- 15 Reddy VY, Doshi SK, Kar S. et al; PREVAIL and PROTECT AF Investigators. 5-year outcomes after left atrial appendage closure: from the PREVAIL and PROTECT AF trials. J Am Coll Cardiol 2017; 70 (24) 2964-2975
- 16 Osmancik P, Herman D, Neuzil P. et al; PRAGUE-17 Trial Investigators. 4-year outcomes after left atrial appendage closure versus nonwarfarin oral anticoagulation for atrial fibrillation. J Am Coll Cardiol 2022; 79 (01) 1-14
- 17 Turagam MK, Osmancik P, Neuzil P, Dukkipati SR, Reddy VY. Left atrial appendage closure versus oral anticoagulants in atrial fibrillation: a meta-analysis of randomized trials. J Am Coll Cardiol 2020; 76 (23) 2795-2797
- 18 Turagam MK, Kawamura I, Neuzil P. et al. Severity of ischemic stroke after left atrial appendage closure vs nonwarfarin oral anticoagulants. JACC Clin Electrophysiol 2023
- 19 Tzikas A, Shakir S, Gafoor S. et al. Left atrial appendage occlusion for stroke prevention in atrial fibrillation: multicentre experience with the AMPLATZER Cardiac Plug. EuroIntervention 2016; 11 (10) 1170-1179
- 20 Hildick-Smith D, Landmesser U, Camm AJ. et al. Left atrial appendage occlusion with the Amplatzer™ Amulet™ device: full results of the prospective global observational study. Eur Heart J 2020; 41 (30) 2894-2901
- 21 Boersma LV, Ince H, Kische S. et al; EWOLUTION Investigators. Efficacy and safety of left atrial appendage closure with WATCHMAN in patients with or without contraindication to oral anticoagulation: 1-year follow-up outcome data of the EWOLUTION trial. Heart Rhythm 2017; 14 (09) 1302-1308
- 22 Freeman JV, Varosy P, Price MJ. et al. The NCDR left atrial appendage occlusion registry. J Am Coll Cardiol 2020; 75 (13) 1503-1518
- 23 Price MJ, Slotwiner D, Du C. et al. Clinical outcomes at 1 year following transcatheter left atrial appendage occlusion in the United States. JACC Cardiovasc Interv 2022; 15 (07) 741-750
- 24 Doshi SK, Kar S, Sadhu A. et al; PINNACLE FLX investigators [Link]. Two-year outcomes with a next-generation left atrial appendage device: final results of the PINNACLE FLX trial. J Am Heart Assoc 2023; 12 (04) e026295
- 25 Waranugraha Y, Lin LY, Tsai CT. Head-to-head comparison between left atrial appendage occlusion and non-vitamin K oral anticoagulants in non-valvular atrial fibrillation patients: a systematic review and meta-analysis study. Trends Cardiovasc Med 2023
- 26 Whitlock RP, Belley-Cote EP, Paparella D. et al; LAAOS III Investigators. Left atrial appendage occlusion during cardiac surgery to prevent stroke. N Engl J Med 2021; 384 (22) 2081-2091
- 27 Oliva A, Ioppolo AM, Chiarito M. et al. Left atrial appendage closure compared with oral anticoagulants for patients with atrial fibrillation: a systematic review and network meta-analysis. J Am Heart Assoc 2024; 13 (16) e034815
- 28 Bayer. A Study to Learn How Well the Study Treatment Asundexian Works and How Safe it is Compared to Apixaban to Prevent Stroke or Systemic Embolism in People with Irregular and Often Rapid Heartbeat (Atrial Fibrillation), and at Risk for Stroke (OCEANIC-AF). 2022. Accessed at: https://classic.clinicaltrials.gov/show/NCT05643573
- 29 Anthos Therapeutics Inc., The TIMI Study Group. Laboratory Corporation of America. Safety and Tolerability of Abelacimab (MAA868) vs. Rivaroxaban in Patients with Atrial Fibrillation (AZALEA-TIMI 71). 2021. Accessed at: https://classic.clinicaltrials.gov/show/NCT04755283
- 30 Anthos Therapeutics Inc. Study to Evaluate the Efficacy and Safety of AbeLacimab in High-Risk Patients with Atrial Fibrillation Who Have Been Deemed Unsuitable for Oral Anticoagulation (LILAC-TIMI 76). 2022. Accessed at: https://classic.clinicaltrials.gov/show/NCT05712200
- 31 Janssen Research Development LLC. Bristol-Myers Squibb. A Study of Milvexian Versus Apixaban in Participants with Atrial Fibrillation (LIBREXIA-AF). 2023. Accessed at: https://classic.clinicaltrials.gov/show/NCT05757869
- 32 Piccini JP, Patel MR, Steffel J. et al; OCEANIC-AF Steering Committee and Investigators. Asundexian versus apixaban in patients with atrial fibrillation. N Engl J Med 2024 (e-pub ahead of print)
- 33 Boston Scientific Corporation. Assessment of the WATCHMAN™ Device in Patients Unsuitable for Oral Anticoagulation (ASAP-TOO). 2017. Accessed at: https://classic.clinicaltrials.gov/show/NCT02928497
- 34 Charite University Berlin Germany, Deutsches Zentrum für Herz-Kreislauf-Forschung, Atrial Fibrillation Network, Stiftung Institut fuer Herzinfarktforschung. Left Atrial Appendage CLOSURE in Patients with Atrial Fibrillation Compared to Medical Therapy (CLOSURE-AF). 2018. Accessed at: https://classic.clinicaltrials.gov/show/NCT03463317
- 35 Karolinska Institutet, Abbott Medical Devices. Prevention of Stroke by Left Atrial Appendage Closure in Atrial Fibrillation Patients After Intracerebral Hemorrhage. 2017. Accessed at: https://classic.clinicaltrials.gov/show/NCT02830152
- 36 Jena University Hospital. Comparison of LAA-Closure vs Oral Anticoagulation in Patients with NVAF and Status Post Intracranial Bleeding. 2020. Accessed at: https://classic.clinicaltrials.gov/show/NCT04298723
- 37 Huijboom M, Maarse M, Aarnink E. et al. COMPARE LAAO: rationale and design of the randomized controlled trial “COMPARing Effectiveness and safety of Left Atrial Appendage Occlusion to standard of care for atrial fibrillation patients at high stroke risk and ineligible to use oral anticoagulation therapy.”. Am Heart J 2022; 250: 45-56
- 38 R&D Cardiologie, Research ZTNOfH, Development. Left Atrial Appendage Occlusion for AF Patients Unable to Use Oral Anticoagulation Therapy (COMPARE-LAAO). 2021. Accessed at: https://classic.clinicaltrials.gov/show/NCT04676880
- 39 Eitel I. Left Atrial Appendage Closure in Patients with Non-valvular Atrial Fibrillation and End-stage Chronic KIDNEY Disease (LAA-KIDNEY). 2022. Accessed at: https://classic.clinicaltrials.gov/show/NCT05204212
- 40 Wazni OM, Boersma L, Healey JS. et al. Comparison of anticoagulation with left atrial appendage closure after atrial fibrillation ablation: rationale and design of the OPTION randomized trial. Am Heart J 2022; 251: 35-42
- 41 Boston Scientific Corporation. Comparison of Anticoagulation with Left Atrial Appendage Closure After AF Ablation (OPTION). 2019. Accessed at: https://classic.clinicaltrials.gov/show/NCT03795298
- 42 Kar S, Doshi SK, Alkhouli M. et al. Rationale and design of a randomized study comparing the Watchman FLX device to DOACs in patients with atrial fibrillation. Am Heart J 2023; 264: 123-132
- 43 Abbott Medical Devices. Amplatzer Amulet LAAO vs. NOAC (CATALYST). 2020. Accessed at: https://classic.clinicaltrials.gov/show/NCT04226547
- 44 University of Aarhus, Aarhus University Hospital, Aalborg University Hospital, Odense University Hospital, Sahlgrenska University Hospital Sweden, Karolinska University Hospital, et al. Left Atrial Appendage Occlusion Versus Novel Oral Anticoagulation for Stroke Prevention in Atrial Fibrillation (Occlusion-AF). 2019. Accessed at: https://classic.clinicaltrials.gov/show/NCT03642509
- 45 Korsholm K, Damgaard D, Valentin JB. et al. Left atrial appendage occlusion vs novel oral anticoagulation for stroke prevention in atrial fibrillation: rationale and design of the multicenter randomized occlusion-AF trial. Am Heart J 2022; 243: 28-38
- 46 Nielsen-Kudsk JE, Johnsen SP, Wester P. et al. Left atrial appendage occlusion versus standard medical care in patients with atrial fibrillation and intracerebral haemorrhage: a propensity score-matched follow-up study. EuroIntervention 2017; 13 (03) 371-378
- 47 Nielsen-Kudsk JE, Korsholm K, Damgaard D. et al. Clinical outcomes associated with left atrial appendage occlusion versus direct oral anticoagulation in atrial fibrillation. JACC Cardiovasc Interv 2021; 14 (01) 69-78
- 48 Chao TF, Joung B, Takahashi Y. et al. 2021 focused update consensus guidelines of the Asia Pacific Heart Rhythm Society on stroke prevention in atrial fibrillation: executive summary. Thromb Haemost 2022; 122 (01) 20-47
- 49 Wang Y, Guo Y, Qin M. et al; Expert Reviewers. 2024 Chinese expert consensus guidelines on the diagnosis and treatment of atrial fibrillation in the elderly, endorsed by Geriatric Society of Chinese Medical Association (Cardiovascular Group) and Chinese Society of Geriatric Health Medicine (Cardiovascular Branch): executive summary. Thromb Haemost 2024; 124 (10) 897-911
- 50 Joglar JA, Chung MK, Armbruster AL. et al; Writing Committee Members. 2023 ACC/AHA/ACCP/HRS guideline for the diagnosis and management of atrial fibrillation: a report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. J Am Coll Cardiol 2024; 83 (01) 109-279
- 51 Van Gelder IC, Rienstra M, Bunting KV. et al; ESC Scientific Document Group. 2024 ESC guidelines for the management of atrial fibrillation developed in collaboration with the European Association for Cardio-Thoracic Surgery (EACTS). Eur Heart J 2024; 45 (36) 3314-3414
- 52 Potpara T, Romiti GF, Sohns C. The 2024 European Society of Cardiology guidelines for diagnosis and management of atrial fibrillation: a viewpoint from a practicing clinician's perspective. Thromb Haemost 2024
- 53 Romiti GF, Pastori D, Rivera-Caravaca JM. et al. Adherence to the “Atrial Fibrillation Better Care” pathway in patients with atrial fibrillation: impact on clinical outcomes—a systematic review and meta-analysis of 285,000 patients. Thromb Haemost 2022; 122 (03) 406-414
- 54 Patel SM, Palazzolo MG, Murphy SA. et al. Evaluation of the atrial fibrillation better care pathway in the ENGAGE AF-TIMI 48 trial. Europace 2022; 24 (11) 1730-1738
- 55 Proietti M, Romiti GF, Olshansky B, Lane DA, Lip GYH. Comprehensive management with the ABC (Atrial Fibrillation Better Care) pathway in clinically complex patients with atrial fibrillation: a post hoc ancillary analysis from the AFFIRM trial. J Am Heart Assoc 2020; 9 (10) e014932
- 56 Shrestha B, Poudel B, Poudel D, Diaz Fraga J. National yearly trend of utilization and procedural complication of the Watchman device in the United States. Cureus 2022; 14 (06) e25567
- 57 Boriani G, Proietti M, Laroche C. et al; EORP-AF Long-Term General Registry Investigators. Association between antithrombotic treatment and outcomes at 1-year follow-up in patients with atrial fibrillation: the EORP-AF General Long-Term Registry. Europace 2019; 21 (07) 1013-1022
- 58 Potpara TS, Dan GA, Trendafilova E. et al; BALKAN-AF Investigators. Stroke prevention in atrial fibrillation and “real world” adherence to guidelines in the Balkan Region: the BALKAN-AF survey. Sci Rep 2016; 6: 20432
- 59 Juhl Madsen O, Lamberts MK, Fosboel EL, Gislason G, Olesen JB, Strange JE. Trends in percutaneous left atrial appendage occlusion and 1-year mortality: a nationwide cohort study. Eur Heart J 2022; 43 (Suppl. 02) ehac544.2137
- 60 Lip GYH, Banerjee A, Boriani G. et al. Antithrombotic therapy for atrial fibrillation: CHEST guideline and expert panel report. Chest 2018; 154 (05) 1121-1201
- 61 Brieger D, Amerena J, Attia J. et al; NHFA CSANZ Atrial Fibrillation Guideline Working Group. National Heart Foundation of Australia and the Cardiac Society of Australia and New Zealand: Australian clinical guidelines for the diagnosis and management of atrial fibrillation 2018. Heart Lung Circ 2018; 27 (10) 1209-1266
- 62 January CT, Wann LS, Calkins H. et al. 2019 AHA/ACC/HRS focused update of the 2014 AHA/ACC/HRS guideline for the management of patients with atrial fibrillation: a report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Rhythm Society. J Am Coll Cardiol 2019; 74 (01) 104-132
- 63 Hindricks G, Potpara T, Dagres N. et al; ESC Scientific Document Group. 2020 ESC guidelines for the diagnosis and management of atrial fibrillation developed in collaboration with the European Association for Cardio-Thoracic Surgery (EACTS): the task force for the diagnosis and management of atrial fibrillation of the European Society of Cardiology (ESC) developed with the special contribution of the European Heart Rhythm Association (EHRA) of the ESC. Eur Heart J 2021; 42 (05) 373-498
- 64 Andrade JG, Aguilar M, Atzema C. et al; Members of the Secondary Panel. The 2020 Canadian Cardiovascular Society/Canadian Heart Rhythm Society comprehensive guidelines for the management of atrial fibrillation. Can J Cardiol 2020; 36 (12) 1847-1948
- 65 Saw J, Holmes DR, Cavalcante JL. et al. SCAI/HRS expert consensus statement on transcatheter left atrial appendage closure. JACC Cardiovasc Interv 2023; 16 (11) 1384-1400
- 66 Glikson M, Wolff R, Hindricks G. et al. EHRA/EAPCI expert consensus statement on catheter-based left atrial appendage occlusion—an update. EuroIntervention 2020; 15 (13) 1133-1180
- 67 Tzikas A, Holmes Jr DR, Gafoor S. et al. Percutaneous left atrial appendage occlusion: the Munich consensus document on definitions, endpoints, and data collection requirements for clinical studies. Europace 2017; 19 (01) 4-15
- 68 Anic A, Bakovic D, Jurisic Z. et al. Diagnostic and therapeutic pathways for the malignant left atrial appendage: European Heart Rhythm Association physician survey. Europace 2023; 25 (07) 25
- 69 Camm AJ. Leap or lag: left atrial appendage closure and guidelines. Europace 2023; 25 (05) 25
- 70 Glikson M, Wolff R, Hindricks G. et al; ESC Scientific Document Group. EHRA/EAPCI expert consensus statement on catheter-based left atrial appendage occlusion—an update. Europace 2020; 22 (02) 184
- 71 Teppo K, Airaksinen KEJ, Jaakkola J. et al. Ischaemic stroke in women with atrial fibrillation: temporal trends and clinical implications. Eur Heart J 2024; 45 (20) 1819-1827
- 72 Nielsen PB, Brøndum RF, Nøhr AK, Overvad TF, Lip GYH. Risk of stroke in male and female patients with atrial fibrillation in a nationwide cohort. Nat Commun 2024; 15 (01) 6728
- 73 Teppo K, Lip GYH, Airaksinen KEJ. et al. Comparing CHA2DS2-VA and CHA2DS2-VASc scores for stroke risk stratification in patients with atrial fibrillation: a temporal trends analysis from the retrospective Finnish AntiCoagulation in Atrial Fibrillation (FinACAF) cohort. Lancet Reg Health Eur 2024; 43: 100967
- 74 Yoshimura H, Providencia R, Finan C, Schmidt AF, Lip GYH. Refining the CHA2DS2VASc risk stratification scheme: shall we drop the sex category criterion?. Europace 2024; 26 (11) euae280
- 75 National Institute for Health and Clinical Excellence. Percutaneous occlusion of the left atrial appendage in non-valvular atrial fibrillation for the prevention of thromboembolism. 2010; available at: https://www.nice.org.uk/guidance/ipg400/documents/thoracoscopic-exclusion-of-the-left-atrial-appendage-in-atrial-fibrillation-with-or-without-other-cardiac-surgery-for-the-prevention-of-thromboembolism-overview2
- 76 Di Biase L, Briceno DF, Trivedi C. et al. Is transesophageal echocardiogram mandatory in patients undergoing ablation of atrial fibrillation with uninterrupted novel oral anticoagulants? Results from a prospective multicenter registry. Heart Rhythm 2016; 13 (06) 1197-1202
- 77 Lee OH, Kim JS, Pak HN. et al. Feasibility of left atrial appendage occlusion for left atrial appendage thrombus in patients with persistent atrial fibrillation. Am J Cardiol 2018; 121 (12) 1534-1539
- 78 Korsholm K, Berti S, Iriart X. et al. Expert recommendations on cardiac computed tomography for planning transcatheter left atrial appendage occlusion. JACC Cardiovasc Interv 2020; 13 (03) 277-292
- 79 Osmancik P, Herman D, Linkova H, Hozman M, Labos M. A comparison of cardiac computed tomography, transesophageal and intracardiac echocardiography, and fluoroscopy for planning left atrial appendage closure. J Atr Fibrillation 2021; 13 (06) 20200449
- 80 Sharma PS, Padala SK, Gunda S, Koneru JN, Ellenbogen KA. Vascular complications during catheter ablation of cardiac arrhythmias: a comparison between vascular ultrasound guided access and conventional vascular access. J Cardiovasc Electrophysiol 2016; 27 (10) 1160-1166
- 81 Yamagata K, Wichterle D, Roubícek T. et al. Ultrasound-guided versus conventional femoral venipuncture for catheter ablation of atrial fibrillation: a multicentre randomized efficacy and safety trial (ULTRA-FAST trial). Europace 2018; 20 (07) 1107-1114
- 82 Sobolev M, Shiloh AL, Di Biase L, Slovut DP. Ultrasound-guided cannulation of the femoral vein in electrophysiological procedures: a systematic review and meta-analysis. Europace 2017; 19 (05) 850-855
- 83 Brass P, Hellmich M, Kolodziej L, Schick G, Smith AF. Ultrasound guidance versus anatomical landmarks for subclavian or femoral vein catheterization. Cochrane Database Syst Rev 2015; 1 (01) CD011447
- 84 Kupó P, Pap R, Sághy L. et al. Ultrasound guidance for femoral venous access in electrophysiology procedures—systematic review and meta-analysis. J Interv Card Electrophysiol 2020; 59 (02) 407-414
- 85 Delgado V, Ajmone Marsan N, de Waha S. et al; ESC Scientific Document Group. 2023 ESC Guidelines for the management of endocarditis. Eur Heart J 2023; 44 (39) 3948-4042
- 86 Vizzari G, Grasso C, Sardone A. et al. Real-world experience with the new Watchman FLX device: data from two high-volume Sicilian centers. The FLX-iEST registry. Catheter Cardiovasc Interv 2022; 100 (01) 154-160
- 87 Price MJ, Friedman DJ, Du C. et al. Comparative safety of transcatheter LAAO with the first-generation Watchman and next-generation Watchman FLX devices. JACC Cardiovasc Interv 2022; 15 (21) 2115-2123
- 88 Paitazoglou C, Meincke F, Bergmann MW. et al. The ALSTER-FLX registry: 3-month outcomes after left atrial appendage occlusion using a next-generation device, a matched-pair analysis to EWOLUTION. Heart Rhythm 2022; 19 (06) 917-926
- 89 Lakkireddy D, Thaler D, Ellis CR. et al; Amulet IDE Investigators. Outcomes of the roll-in cohort of the Amulet IDE trial of left atrial appendage occlusion. Heart Rhythm O2 2022; 3 (05) 493-500
- 90 Chen S, Chun KRJ, Bordignon S. et al. Left atrial appendage occlusion using LAmbre Amulet and Watchman in atrial fibrillation. J Cardiol 2019; 73 (04) 299-306
- 91 Tilz RR, Fink T, Bartus K. et al. A collective European experience with left atrial appendage suture ligation using the LARIAT+ device. Europace 2020; 22 (06) 924-931
- 92 Betts TR, Grygier M, Nielsen Kudsk JE. et al; FLXibility investigators. Real-world clinical outcomes with a next-generation left atrial appendage closure device: the FLXibility Post-Approval Study. Europace 2023; 25 (03) 914-921
- 93 Bhogal S, Aladin AI, Wermers JP, Morrison N, Gray N, Waksman R. Review of late-breaking trials from CRT 2022. Cardiovasc Revasc Med 2022; 40S: 3-7
- 94 Merdler I, Reddy PK, Bhogal S. et al. Review of late-breaking trials from CRT 2023. Cardiovasc Revasc Med 2023; 53S: S3-S9
- 95 Lakkireddy D, Thaler D, Ellis CR. et al. Amplatzer Amulet left atrial appendage occluder versus Watchman device for stroke prophylaxis (Amulet IDE): a randomized, controlled trial. Circulation 2021; 144 (19) 1543-1552
- 96 Holmes DR, Reddy VY, Turi ZG. et al; PROTECT AF Investigators. Percutaneous closure of the left atrial appendage versus warfarin therapy for prevention of stroke in patients with atrial fibrillation: a randomised non-inferiority trial. Lancet 2009; 374 (9689): 534-542
- 97 Reddy VY, Doshi SK, Sievert H. et al; PROTECT AF Investigators. Percutaneous left atrial appendage closure for stroke prophylaxis in patients with atrial fibrillation: 2.3-year follow-up of the PROTECT AF (Watchman Left Atrial Appendage System for Embolic Protection in Patients with Atrial Fibrillation) trial. Circulation 2013; 127 (06) 720-729
- 98 Bergmann MW, Betts TR, Sievert H. et al. Safety and efficacy of early anticoagulation drug regimens after WATCHMAN left atrial appendage closure: three-month data from the EWOLUTION prospective, multicentre, monitored international WATCHMAN LAA closure registry. EuroIntervention 2017; 13 (07) 877-884
- 99 Berti S, Pastormerlo LE, Rezzaghi M. et al. Left atrial appendage occlusion in high-risk patients with non-valvular atrial fibrillation. Heart 2016; 102 (24) 1969-1973
- 100 Korsholm K, Nielsen KM, Jensen JM, Jensen HK, Andersen G, Nielsen-Kudsk JE. Transcatheter left atrial appendage occlusion in patients with atrial fibrillation and a high bleeding risk using aspirin alone for post-implant antithrombotic therapy. EuroIntervention 2017; 12 (17) 2075-2082
- 101 Landmesser U, Schmidt B, Nielsen-Kudsk JE. et al. Left atrial appendage occlusion with the AMPLATZER Amulet device: periprocedural and early clinical/echocardiographic data from a global prospective observational study. EuroIntervention 2017; 13 (07) 867-876
- 102 Saw J, Tzikas A, Shakir S. et al. Incidence and clinical impact of device-associated thrombus and peri-device leak following left atrial appendage closure with the Amplatzer Cardiac Plug. JACC Cardiovasc Interv 2017; 10 (04) 391-399
- 103 Kar S, Doshi SK, Sadhu A. et al; PINNACLE FLX Investigators. Primary outcome evaluation of a next-generation left atrial appendage closure device: results from the PINNACLE FLX trial. Circulation 2021; 143 (18) 1754-1762
- 104 Ellis CR, Jackson GG, Kanagasundram AN. et al. Left atrial appendage closure in patients with prohibitive anatomy: insights from PINNACLE FLX. Heart Rhythm 2021; 18 (07) 1153-1161
- 105 Korsholm K, Samaras A, Andersen A, Jensen JM, Nielsen-Kudsk JE. The Watchman FLX device: first European experience and feasibility of intracardiac echocardiography to guide implantation. JACC Clin Electrophysiol 2020; 6 (13) 1633-1642
- 106 Paitazoglou C, Bergmann MW, Ince H. et al; theEWOLUTION Investigators. True efficacy of LAA closure: patient outcomes on long-term single-antiplatelet or no therapy: insights from the EWOLUTION registry. J Invasive Cardiol 2022; 34 (05) E348-E355
- 107 Simard T, Jung RG, Lehenbauer K. et al. Predictors of device-related thrombus following percutaneous left atrial appendage occlusion. J Am Coll Cardiol 2021; 78 (04) 297-313
- 108 Cepas-Guillén P, Flores-Umanzor E, Leduc N. et al. Impact of device implant depth after left atrial appendage occlusion. JACC Cardiovasc Interv 2023; 16 (17) 2139-2149
- 109 Saliba WI, Kawai K, Sato Y. et al. Enhanced thromboresistance and endothelialization of a novel fluoropolymer-coated left atrial appendage closure device. JACC Clin Electrophysiol 2023; 9 (8 Pt 2): 1555-1567
- 110 Lakkireddy D, Nielsen-Kudsk JE, Windecker S. et al. Mechanisms, predictors, and evolution of severe peri-device leaks with two different left atrial appendage occluders. Europace 2023; 25 (09) 25
- 111 Della Rocca DG, Murtaza G, Di Biase L. et al. Radiofrequency energy applications targeting significant residual leaks after Watchman implantation: a prospective, multicenter experience. JACC Clin Electrophysiol 2021; 7 (12) 1573-1584
- 112 Chen S, Weise FK, Chun KRJ, Schmidt B. Antithrombotic strategies after interventional left atrial appendage closure: an update. Expert Rev Cardiovasc Ther 2018; 16 (09) 675-678
- 113 Branca L, Tomasoni D, Cimino G. et al. Impact and predictors of device-related thrombus after percutaneous left atrial appendage closure. J Cardiovasc Med (Hagerstown) 2023; 24 (01) 12-19
- 114 Connolly S, Pogue J, Hart R. et al; ACTIVE Writing Group of the ACTIVE Investigators. Clopidogrel plus aspirin versus oral anticoagulation for atrial fibrillation in the Atrial fibrillation Clopidogrel Trial with Irbesartan for prevention of Vascular Events (ACTIVE W): a randomised controlled trial. Lancet 2006; 367 (9526): 1903-1912
- 115 Connolly SJ, Eikelboom J, Joyner C. et al; AVERROES Steering Committee and Investigators. Apixaban in patients with atrial fibrillation. N Engl J Med 2011; 364 (09) 806-817
- 116 Mant J, Hobbs FD, Fletcher K. et al; BAFTA investigators, Midland Research Practices Network (MidReC). Warfarin versus aspirin for stroke prevention in an elderly community population with atrial fibrillation (the Birmingham Atrial Fibrillation Treatment of the Aged Study, BAFTA): a randomised controlled trial. Lancet 2007; 370 (9586): 493-503
- 117 Okumura K, Akao M, Yoshida T. et al; ELDERCARE-AF Committees and Investigators. Low-dose edoxaban in very elderly patients with atrial fibrillation. N Engl J Med 2020; 383 (18) 1735-1745
- 118 Riegler L, Palermi S, Scarafile R. et al. Clinical and multi-modality imaging approach in the selection of patients for left atrial appendage closure. Rev Cardiovasc Med 2021; 22 (04) 1197-1204
- 119 Søndergaard L, Wong YH, Reddy VY. et al. Propensity-matched comparison of oral anticoagulation versus antiplatelet therapy after left atrial appendage closure with WATCHMAN. JACC Cardiovasc Interv 2019; 12 (11) 1055-1063
- 120 Cruz-González I, Trejo-Velasco B. Percutaneous left atrial appendage occlusion in the current practice. Kardiol Pol 2021; 79 (03) 255-268
- 121 Ledwoch J, Sievert K, Boersma LVA. et al; EWOLUTION Investigators. Initial and long-term antithrombotic therapy after left atrial appendage closure with the WATCHMAN. Europace 2020; 22 (07) 1036-1043
- 122 Freeman JV, Higgins AY, Wang Y. et al. Antithrombotic therapy after left atrial appendage occlusion in patients with atrial fibrillation. J Am Coll Cardiol 2022; 79 (18) 1785-1798
- 123 Freeman J, Hsu JC, Kapadia S. et al. Ce-452771–4 outcomes with different postprocedural antithrombotic therapy regimens following left atrial appendage occlusion. Heart Rhythm 2023; 20: S36-S37
- 124 Carvalho PEP, Gewehr DM, Miyawaki IA. et al. Comparison of initial antithrombotic regimens after left atrial appendage occlusion: a systematic review and network meta-analysis. J Am Coll Cardiol 2023; 82 (18) 1765-1773
- 125 Mhanna M, Beran A, Al-Abdouh A. et al. Single versus dual antiplatelet therapy following left atrial appendage occlusion in patients with high bleeding risk. Curr Probl Cardiol 2022; 47 (09) 101269
- 126 Vignali L, Gurgoglione FL, Barocelli F. et al. Looking for optimal antithrombotic strategy after transcatheter left atrial appendage occlusion: a real-world comparison of different antiplatelet regimens. Int J Cardiol 2023; 371: 92-99
- 127 Rodriguez-Gabella T, Nombela-Franco L, Regueiro A. et al. Single antiplatelet therapy following left atrial appendage closure in patients with contraindication to anticoagulation. J Am Coll Cardiol 2016; 68 (17) 1920-1921
- 128 Azienda Ospedaliero Universitaria Maggiore della Carita, Abbott Medical Devices. Head-to-head Comparison of Single Versus Dual Antiplatelet Treatment Strategy After Percutaneous Left Atrial Appendage Closure: A Multicenter, Randomized Study (ARMYDA-AMULET). 2021. Accessed at: https://classic.clinicaltrials.gov/show/NCT05554822
- 129 Cepas-Guillen PL, Flores-Umanzor E, Regueiro A. et al. Low dose of direct oral anticoagulants after left atrial appendage occlusion. J Cardiovasc Dev Dis 2021; 8 (11) 8
- 130 Della Rocca DG, Magnocavallo M, Di Biase L. et al. Half-dose direct oral anticoagulation versus standard antithrombotic therapy after left atrial appendage occlusion. JACC Cardiovasc Interv 2021; 14 (21) 2353-2364
- 131 Freixa X. Apixaban vs Dual Antiplatet Therapy Study After Left Atrial Appendage Occlosure (ADALA). 2019 Accessed at: https://classic.clinicaltrials.gov/show/NCT05632445
- 132 Freixa X, Cruz-González I, Cepas-Guillén P. et al. Low dose direct oral anticoagulation vs. DAPT after LAAO. Euro PCR 2023
- 133 Centre de Recherche de l'Institut Universitaire de Cardiologie et de Pneumologie de Quebec, Institut universitaire de cardiologie et de pneumologie de Québec University Laval. Short-Term Anticoagulation Versus Antiplatelet Therapy for Preventing Device Thrombosis Following Left Atrial Appendage Closure (ANDES). 2018. Accessed at: https://classic.clinicaltrials.gov/show/NCT03568890
- 134 Schmidt B, Nielsen-Kudsk JE, Ellis CR. et al. Incidence, predictors, and clinical outcomes of device-related thrombus in the Amulet IDE trial. JACC Clin Electrophysiol 2023; 9 (01) 96-107
- 135 Dukkipati SR, Kar S, Holmes DR. et al. Device-related thrombus after left atrial appendage closure: incidence, predictors, and outcomes. Circulation 2018; 138 (09) 874-885
- 136 Dukkipati SR, Holmes Jr DR, Doshi SK. et al. Impact of peridevice leak on 5-year outcomes after left atrial appendage closure. J Am Coll Cardiol 2022; 80 (05) 469-483
- 137 Alkhouli M, Du C, Killu A. et al. Clinical impact of residual leaks following left atrial appendage occlusion: insights from the NCDR LAAO registry. JACC Clin Electrophysiol 2022; 8 (06) 766-778
- 138 Sharma SP, Turagam MK, Gopinathannair R. et al. Direct current cardioversion of atrial fibrillation in patients with left atrial appendage occlusion devices. J Am Coll Cardiol 2019; 74 (18) 2267-2274
- 139 Maarse M, Wintgens LIS, Ponomarenko A. et al. Impact of anticoagulation strategy after left atrial appendage occlusion in patients requiring direct current cardioversion. J Cardiovasc Electrophysiol 2021; 32 (03) 737-744
- 140 Joglar JA, Chung MK, Armbruster AL. et al. ACC/AHA/ACCP/HRS guideline for the diagnosis and management of atrial fibrillation: a report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation 2024; 149 (01) e1-e156