

Subscribe to RSS
DOI: 10.1055/a-2471-1016
Useful treatment selection strategy for endoscopic hemostasis in colonic diverticular bleeding according to endoscopic findings (with video)
Authors

Abstract
Background and study aims
Direct or indirect clipping and endoscopic band ligation (EBL) are widely used for hemostasis in patients with colonic diverticular bleeding (CDB). However, no treatment selection strategy has been established. This report describes our approach and its outcomes.
Patients and methods
We select direct clipping if the bleeding point is visible and clips could be inserted into the diverticulum. When direct clipping is not feasible, we select EBL as the second choice and indirect clipping as the third. We reviewed data from 192 patients treated with clipping or EBL for definitive CDB with stigmata of recent hemorrhage (SRH) at our hospital between March 2016 and February 2023.
Results
The hemostatic method was clipping in 84 patients (direct, n=78; indirect, n=6) and EBL in 108. The rate of SRH with active bleeding was significantly higher in the EBL group (33.3% vs. 60.2%, p <0.001). Median hemostasis time was significantly shorter in the clipping group (9 min vs. 22 min, P <0.001). There was no significant difference in the 30-day rebleeding rate between clipping and EBL (15.5% vs. 13.0%; P=0.619). There was one case of delayed perforation post-EBL. There were no complications after clipping.
Conclusions
Direct clipping when placement of clips at the bleeding point is feasible and EBL when direct clipping is not feasible is a reasonable strategy in terms of effectiveness, efficiency, and safety. Selection of hemostatic method according to the visual field of SRH and maneuverability of the endoscope allows the advantages of both methods to be realized.
Keywords
Endoscopy Lower GI Tract - Lower GI bleeding - GI surgery - Quality and logistical aspects - Quality managementIntroduction
Colonic diverticular bleeding (CDB) is the most common cause of acute lower gastrointestinal bleeding (ALGIB), and its management is clinically important because severe cases need to be treated by interventional radiology (IVR) or surgery [1] [2]. Endoscopic therapy potentially prevents recurrence of CDB with stigmata of recent hemorrhage (SRH) [3] [4] [5] . Among the various endoscopic therapies for CDB, the clipping technique is commonly used worldwide because of its simplicity, low cost, and theoretical advantage of causing less damage to adjacent tissues [6] [7] [8] [9] [10] [11]. Clipping methods for CDB are classified as direct or indirect [7] [12] [13], whereby direct clipping involves capturing the vessel directly and indirect clipping involves closing the diverticular orifice in a zipper-like manner [9] [10]. A large multicenter cohort study in Japan found that the rebleeding rate was significantly lower after direct clipping than after indirect clipping [14]. However, direct clipping for CDB with active bleeding is challenging and is reported to be less effective because the bleeding point is obscured by blood [14].
Recently, endoscopic band ligation (EBL) has been used for CDB because it is reported to have higher efficacy compared with clipping [8] [15] [16]. For example, a large multicenter cohort study in Japan found that the rebleeding rate was significantly lower after EBL than after clipping and that the results were unchanged in the subgroup of CDB with active bleeding [16]. However, EBL has disadvantages in that the endoscope requires reinsertion for attachment of a ligation device and is associated with a risk of delayed perforation [17] [18] [19].
Based on these results, when direct clip placement at the bleeding point is feasible (e.g., non-active bleeding), direct clipping as the first choice for endoscopic hemostasis is expected to be effective in preventing rebleeding and shorter and safer than EBL. Moreover, EBL as the second choice is expected to be more effective than direct clipping in cases where accurate direct clip placement at the bleeding point is difficult (e.g., active bleeding). If clipping or EBL for CDB can be appropriately selected, we can realize the advantages of both strategies, thereby improving clinical outcomes. However, no studies have evaluated the usefulness of a treatment selection strategy for clipping and EBL in CDB. We hypothesized that direct clipping, which entails precise grasping of the bleeding point of CDB, would be as effective as EBL and subsequently developed the following treatment selection strategy in 2016 when we introduced EBL. At our institution, direct clipping is the first choice if the bleeding point is visible and direct endoclip placement at the bleeding point is possible; if direct clipping is not feasible, EBL is the second choice. In this study, we evaluated the effectiveness of our treatment selection strategy for endoscopic hemostasis in patients with definitive CDB.
Patients and methods
Patients and study design
We retrospectively reviewed the electronic admission and endoscopy databases at Nara City Hospital and identified 391 adult patients who were emergently hospitalized for acute hematochezia between March 2016 and February 2023. Of the 205 patients diagnosed with definitive CDB based on presence of SRH, we analyzed data from 192 patients who were successfully treated by clipping (n=84) or EBL (n=108), ([Fig. 1]). The study protocol was approved by the ethics committee and institutional review board of Nara City Hospital.

Endoscopic procedures and strategy for endoscopic hemostasis (with video)
All patients in this study received standard supportive medical care for acute lower gastrointestinal bleeding, including hemodynamic monitoring and fluid resuscitation. Packed red blood cells were transfused to correct severe anemia if necessary. Bowel preparation with polyethylene glycol or glycerin enema was performed before colonoscopy if possible. All patients underwent colonoscopy with a distal attachment cap and a water-jet device (OFP-2; Olympus Corp., Tokyo, Japan). The most commonly used colonoscope was the PCF-Q260AZI (Olympus Corp.). Colonic diverticula were observed under water immersion to improve endoscopic visualization [20] ([Video 1]: Case 1–3).
Endoscopic hemostasis for colonic diverticular bleeding.Case 1. Direct clipping for colonic diverticular bleeding under water observation.
Case 2. Endoscopic band ligation for active colonic diverticular bleeding.
Case 3. Direct clipping for active colonic diverticular bleeding using a clip device with a re-grasping function.* (*Note: This case was outside the study period.)Video 1
When SRH was identified, we observed the bleeding point and selected the treatment method according to how easily the bleeding point could be visualized and maneuverability of the colonoscope. In principle, the treatment selection policy at our institution is as follows. If the bleeding point is visible and an endoclip insertion is possible, direct clipping is selected as the first choice ([Video 1]: Case 1). If direct clipping is not feasible, EBL is selected as the second choice ([Video 1]: Case 2). If both direct clipping and EBL are difficult, indirect clipping is selected as the third choice. Final treatment selection is made at the discretion of the endoscopist depending on patient comorbidities, ease of insertion of the endoscope, and maneuverability. If initial endoscopic hemostasis fails, additional endoscopic treatment is performed if possible. In this study, patient outcomes were evaluated according to the method that ultimately achieved successful hemostasis ([Fig. 2]).

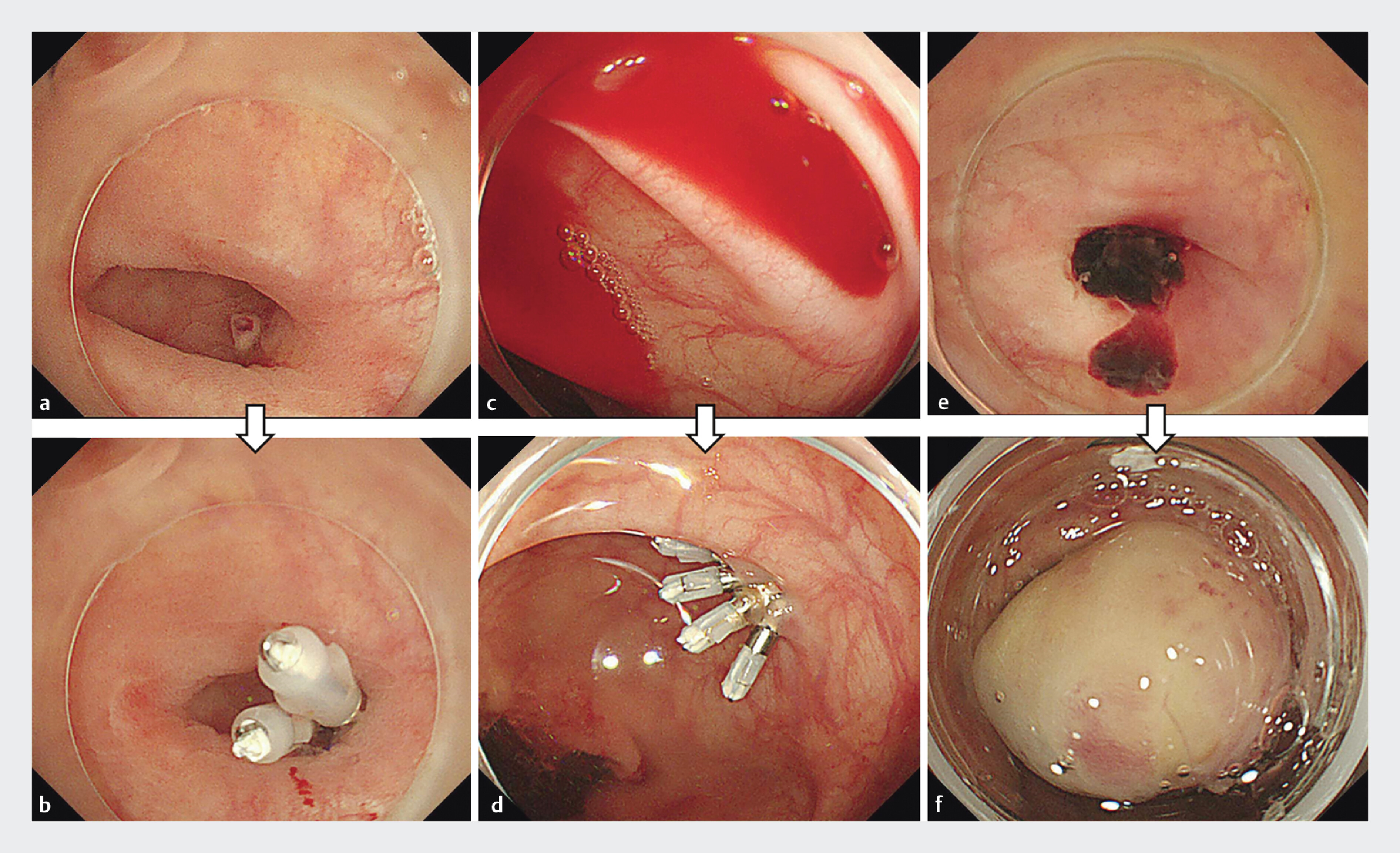
When using the direct clipping method, endoclips (HX-610–090S EZ CLIP; Olympus Corp.) are placed directly on the vessel [12] [13] ([Fig. 3] a, [Fig. 3] b). When using the indirect clipping method, the diverticulum is closed in a zipper-like manner [12] [13] ([Fig. 3] c, [Fig. 3] d). The EBL method for CDB is the same as that reported previously [15] [21]. After the site of bleeding has been marked with endoclips, the colonoscope is removed and then reinserted after attachment of a band ligator device (MD-48912B EBL; Sumitomo Bakelite Company Ltd., Tokyo, Japan). The diverticulum is then pulled into the cup of the endoscopic ligator by suction, and the elastic O-ring is released ([Fig. 3] e, [Fig. 3] f).
Variables investigated
We assessed the clinical data, including baseline characteristics such as age, sex, vital signs on admission, and lifestyle factors as well as presenting symptoms, laboratory data, comorbidities, and medication use. We also reviewed in-hospital examination findings obtained from electronic medical records and endoscopy databases. Comorbidities were assessed using the Charlson Comorbidity Index [22] with the addition of the following four items: hypertension, diabetes mellitus, dyslipidemia, and cerebrovascular or cardiovascular disease. We also evaluated items concerning endoscopic procedures, including type of bowel preparation, use of a distal attachment cap, use of a water-jet device, type and location of SRH, bleeding point in the diverticulum, method of endoscopic hemostasis, and procedure time. SRH was defined as active or non-active bleeding (a densely adherent clot despite vigorous irrigation and/or a visible non-bleeding vessel) seen on colonoscopy [4] [12] ([Fig. 3] a, [Fig. 3] c, [Fig. 3] e). SRH was classified as left-sided (descending colon, sigmoid colon, and rectum) or right-sided (other locations).
Outcomes
The outcome of interest was rebleeding after endoscopic treatment during hospitalization or after discharge. Early rebleeding was defined as rebleeding within 30 days of endoscopic treatment for CDB and late rebleeding as rebleeding within 1 year [12] [23]. Secondary outcomes were need for IVR or surgery after endoscopic treatment, blood transfusion requirement during hospitalization, length of hospital stay, and endoscopy-related outcomes, including type of SRH, bleeding point in the diverticulum, location of SRH, success rate of initial endoscopic hemostasis, and procedure time.
Statistical analysis
Patient characteristics and outcomes were compared between the clipping and EBL groups. Categorical data were compared between the two treatment groups using the chi-squared test or Fisher’s exact test, as appropriate. Continuous data were compared using the Mann-Whitney U test. Propensity score matching (PSM) was used to adjust for differences between the two treatment groups. A logistic regression model was used for propensity score estimation, with EBL as a function of patient baseline characteristics and endoscopic factors. The model included age ≥70 years, sex, and seven factors found to be of at least borderline significance (P <0.10) in univariate analysis ([Table 1]). We performed one-to-one PSM between the clipping and EBL groups, using the nearest neighbor method within a caliper width of 0.2 of the standard deviation of the logit of the propensity score. Before matching, the area under the receiver-operating characteristic curve for propensity scores was 0.734 (95% confidence interval [CI] 0.664–0.803) for EBL. Time-to-event analysis was performed using the Kaplan-Meier method and log-rank test. Statistical analysis was performed using Statistical Package for Social Sciences version 22 (IBM Corp., Armonk, New York, United States). P <0.05 was considered statistically significant.
Results
Patient characteristics
Baseline characteristics of the 192 patients who underwent clipping or EBL for definitive CDB are shown in Supplementary Table 1. The hemostatic method was clipping in 84 patients (direct, n=78; indirect, n=6) and EBL in 108. Baseline characteristics of the unmatched and matched cohorts are presented in [Table 1]. In the unmatched cohort, the clipping and EBL groups showed significant differences (P <0.05) in five variables at baseline, with an absolute standardized difference (ASD) >0.2 for 13 variables. PSM identified 132 patients, comprising 66 pairs from the clipping and EBL groups. The number of variables with an ASD >0.2 was reduced to seven, and baseline characteristics were more balanced in the PSM data.
Endoscopy-related outcomes in our treatment selection strategy
In the unmatched cohort, clipping was selected significantly more frequently than EBL for visible vessels, bleeding at the dome of the diverticulum, and a right-sided diverticulum. However, EBL was selected significantly more frequently than clipping for active bleeding, unconfirmed bleeding point, and for bleeding in the left side of the colon. Total procedure time and time to hemostasis after identification of the SRH was significantly shorter in the clipping group than in the EBL group. These results did not change in the matched cohorts, except for the location of SRH ([Table 2]). Success rates of initial endoscopic hemostasis in direct clipping, indirect clipping, and EBL were 86.4% (76/88), 100% (4/4), and 92.4% (97/105), respectively ([Fig. 2]).
|
Unmatched cohort (N=192) |
Matched cohort (N=132) |
|||||
|
Clipping |
Band ligation |
P value |
Clipping |
Band ligation |
P value |
|
|
Data are shown as the number (percentage) or median (interquartile range). Bold values indicate P <0.05. *The treatment selection policy at our institution is as follows. If the bleeding point is visible and an endoclip insertion is possible, direct clipping is selected as the first choice ([Video 1] : Case 1). If direct clipping is not feasible, band ligation is selected as the second choice ([Video 1] : Case 2). If both direct clipping and band ligation are difficult, indirect clipping is selected as the third choice. †Total procedure time was defined as total time from the start to end of colonoscopy. SRH, stigmata of recent hemorrhage. |
||||||
|
SRH-related outcomes |
||||||
|
||||||
|
28 (33.3) |
65 (60.2) |
<0.001 |
23 (34.8) |
35 (53.0) |
0.035 |
|
43 (51.2) |
24 (22.2) |
<0.001 |
35 (53.0) |
16 (24.2) |
0.001 |
|
13 (15.5) |
19 (17.6) |
0.696 |
8 (12.1) |
15 (22.7) |
0.108 |
|
||||||
|
62 (73.8) |
36 (33.3) |
<0.001 |
48 (72.7) |
23 (34.8) |
<0.001 |
|
6 (7.1) |
4 (3.7) |
0.338 |
5 (7.6) |
(6.1) |
1 |
|
16 (19.0) |
68 (63.0) |
<0.001 |
13 (19.7) |
39 (59.1) |
<0.001 |
|
||||||
|
68 (81.0) |
73 (67.6) |
0.038 |
53 (80.3) |
50 (75.8) |
0.528 |
|
16 (19.0) |
35 (32.4) |
0.038 |
13 (19.7) |
16 (24.2) |
0.528 |
|
Total procedural time,† min |
42.5 (29–62) |
63.5 (47–78) |
<0.001 |
45.5 (29–62) |
66 (47–84) |
<0.001 |
|
Time to hemostasis after identification of SRH, min |
9 (6–14.5) |
22 (14–31.5) |
<0.001 |
9 (6–14) |
21.5 (14–34) |
<0.001 |
Clinical outcomes of clipping and EBL in our treatment selection strategy
In the unmatched cohort, there was no significant differences in early or late rebleeding rate between clipping and EBL (15.5% vs. 13.0%, P=0.619 and 28.6% vs. 27.8%, P=0.903, respectively). Furthermore, there were no significant between-group differences in need for IVR, need for surgery, or length of hospital stay. These results were unchanged in the matched cohort ([Table 3]). Kaplan-Meier analysis revealed no significant difference in likelihood of rebleeding between the two groups during a mean follow-up of 284 days (P=0.938, log-rank test) (Supplementary Fig. 1).
|
Unmatched cohort (N=192) |
Matched cohort (n=132) |
|||||||
|
Clipping |
Band ligation |
Crude OR (95% CI) |
P value |
Clipping |
Band ligation |
Crude OR (95% CI) |
P value |
|
|
Data are shown as the number (percentage) or median (interquartile range). *Treatment selection policy at our institution is as follows. If the bleeding point is visible and endoclip insertion is possible, direct clipping is selected as the first choice ([Video 1] : Case 1). If direct clipping is not feasible, band ligation is selected as the second choice ([Video 1] : Case 2). If both direct clipping and band ligation are difficult, indirect clipping is selected as the third choice. CI, confidence interval; IVR, interventional radiology; NA, not applicable; OR, odds ratio. |
||||||||
|
Rebleeding within 30 days after endoscopic treatment |
13 (15.5) |
14 (13.0) |
0.813 |
0.619 |
10 (15.2) |
10 (15.2) |
1 |
1 |
|
Rebleeding within 1 year after endoscopic treatment |
24 (28.6) |
30 (27.8) |
0.962 |
0.903 |
21 (31.8) |
20 (30.3) |
0.932 |
0.851 |
|
IVR needed after endoscopic treatment |
1 (1.2) |
1 (0.9) |
0.776 |
1.000 |
1 (1.5) |
0 (0) |
NA |
1 |
|
Surgery needed after endoscopic treatment |
0 (0) |
1 (0.9) |
NA |
1.000 |
0 (0) |
0 (0) |
NA |
NA |
|
Blood transfusion requirement during hospitalization |
18 (21.4) |
14 (13.0) |
0.546 |
0.118 |
14 (21.2) |
10 (15.2) |
0.663 |
0.367 |
|
Length of hospital stay, days |
6 (4–8.5) |
5 (4–8) |
NA |
0.079 |
6 (4–9) |
5.5 (4–8) |
NA |
0.593 |
|
Prolonged hospitalization |
38 (45.2) |
41 (38.0) |
0.741 |
0.310 |
31 (47.0) |
30 (45.5) |
0.941 |
0.861 |
Characteristics of patients who underwent endoscopic hemostasis for definitive CDB according to rebleeding status
Baseline characteristics of the rebleeding and non-rebleeding patients who underwent clipping are presented in Supplementary Table 2. Significant differences in current alcohol consumption and type of SRH (active bleeding) were found between the rebleeding and non-bleeding groups. Baseline characteristics in the rebleeding and non-rebleeding patients who underwent EBL are compared in Supplementary Table 3. Significant differences were found between the rebleeding and non-bleeding groups according to whether or not body mass index was ≥25.
Endoscopically relevant adverse events
No endoscopically relevant adverse events (AEs) were observed after clipping. However colonic diverticulitis and perforation developed in one patient (0.93%) following EBL. The patient was a 63-year-old man who presented to our hospital with massive hematochezia. He was taking prednisolone 30 mg and tocilizumab for adult-onset Still’s disease and rivaroxaban for paroxysmal atrial fibrillation. Contrast-enhanced computed tomography (CT) revealed two extravasation sites, one in the sigmoid colon and the other in the descending colon. Emergency colonoscopy showed a diverticulum with an adherent clot in the descending colon but no SRH in the sigmoid colon. EBL was performed for the SRH in the descending colon. No rebleeding was observed after EBL, and the patient was discharged 5 days after treatment. On Day 14 after EBL, the patient was readmitted to our hospital with left lower abdominal pain. Sigmoid colon diverticulitis was diagnosed based on CT and was treated with antibiotics. On Day 19 after EBL, the patient developed severe lower abdominal pain, and colon perforation was diagnosed by CT. Emergency surgery revealed two perforation sites, one in the sigmoid colon and the other in the descending colon. Colonic resection and colostomy were performed.
Discussion
To our knowledge, this is the first study to evaluate the validity of a selection strategy for endoscopic hemostatic methods in CDB according to endoscopic findings for the bleeding point. The main result was that there was no significant difference in terms of bleeding rate (within 30 days or 1 year), need for IVR or surgery, blood transfusion requirement, or length of hospital stay between the clipping group and the EBL group when direct clipping was selected when feasible. Other important findings of this study are as follows. First, unlike in previous studies (Supplementary Table 4), the proportion of patients who underwent direct clipping was high in the overall population as well in the clipping group at 40.6% (78/192) and 92.9% (78/84), respectively. Second, EBL was selected significantly more often for CDB with active bleeding and in the left side of the colon. Third, total procedure time was significantly shorter for the clipping group than for EBL. Fourth, delayed perforation was observed in the EBL group but there were no complications in the clipping group. These findings suggest that the strategy of direct clipping when clip placement at the bleeding point is feasible and EBL when direct clipping is not feasible is reasonable in terms of effectiveness, efficiency, and safety of treatment. Importantly, the cases completed with direct clipping alone when feasible did not negatively affect outcomes. In fact, those cases showed benefits such as reduced procedure time. Also, the extended procedure time with EBL did not compromise clinical outcomes.
Direct clipping was selected for cases in which the view of the bleeding point and endoscopic maneuverability were sufficient to allow direct clip placement at the bleeding point, whereas indirect clipping was rarely selected. Our treatment selection strategy for clipping methods was considered to make clipping more effective and to be the reason why there was no significant difference in rebleeding rate between clipping and EBL. Direct clipping achieves hemostasis by grasping the bleeding point, whereas indirect clipping achieves hemostasis by closing the diverticulum and compressing it with a hematoma. Previous studies have reported that the rebleeding rate is higher with indirect clipping than with direct clipping [13] [14], suggesting that the hemostatic effect of clipping is more effective when the bleeding point is directly grasped. Interestingly, we found no significant difference in early or late rebleeding rates between the clipping and EBL groups. We speculated that this may be because direct clipping blocks blood flow in the vessel, ultimately causing the vessel to disappear. However, the late rebleeding rate was high in both the clipping group (28.6%) and the EBL group (27.8%) in our study, possibly because the rebleeding sites were different from the previously treated sites, as reported previously [12].
We reviewed previous studies investigating the effectiveness of endoscopic clipping and EBL for CDB (Supplementary Table 4) and found a mean early rebleeding rate of 12.3% (186/1512) for EBL, which is similar to our rate of 13.0%. However, the mean early rebleeding rate after clipping was 24.3% (462/1901), which is higher than our rate of 15.5%. It is also noteworthy that the proportion of direct clipping procedures was much higher (92.9%, 78/84) in our study than in previous reports, suggesting that rebleeding after clipping depends on how accurately the clip is placed at the bleeding point.
However, hemostasis with direct clipping may be difficult [21] [24]. Direct clip placement in colonic diverticula may be affected by how endoscopic observation is performed, ease of endoclip insertion, and stability of the endoscope. We attempted to overcome these issues by using underwater observation with a distal attachment cap and a water-jet device [13] [20]. As a result, the proportion of cases in which direct clipping was performed was 40.6% (78/192), which is higher than the 21.4% (360/1679) found in a retrospective analysis of a large multicenter cohort of Japanese patients with definitive CDB [14] [16] . Endoscopic images and video depictions of direct clipping for CDB using underwater observation are available in a recently published series [13] [25] [26].
In our study, rebleeding after clipping was significantly more common in patients with active bleeding during the procedure. We speculated that this may be because active bleeding obscures the bleeding point, making it difficult to accurately grasp the bleeding point for direct clipping. Other studies have also found an association between clipping under conditions with poor visibility, such as active bleeding, and rebleeding [14] [27]. A recently developed novel clip device with a re-grasping function (SureClip; Micro-Tech Co., Nanjing, China) has two advantages. First, the clip can be opened inside the diverticulum and grasp the base of the diverticulum, even if the diverticular orifice is small. Second, grasping can be repeated until hemostasis is confirmed, even if the bleeding point is not visible because of, for example, active bleeding [28]. Direct clipping might be feasible using this device even in active CDB (Video: Case 3). In contrast, no association was found between active bleeding in EBL and rebleeding (Supplementary Table 3). We found EBL to be effective even in patients with active bleeding during EBL, which is consistent with a previous report [16]. A Japanese study based on the Nationwide ALGIB endoscopy dataset [29] found that the 30-day rebleeding rate was significantly higher after direct clipping than after snare or band ligation in right-sided CDB with active bleeding. However, the investigators found no significant difference in 30-day rebleeding rate between ligation and direct clipping in right-sided CDB without active bleeding. These results are in line with our present findings. Therefore, a ligation method such as EBL should be chosen when accurate direct clipping is difficult because of active bleeding.
In our patients, EBL was selected significantly more often for the left side of the colon. Compared with the right side, the left side has a narrower lumen and stronger flexion [30], which reduces the maneuverability of the scope and the visual field [31]. Direct clipping is difficult when scope maneuverability is poor and the field of view is limited. Analysis of the Nationwide ALGIB endoscopy dataset in Japan revealed no association between the 30-day rebleeding rate and the method used for hemostasis (i.e., ligation, direct clipping, or indirect clipping) in left-sided CDB, regardless of active bleeding [29]. However, in view of the potential AEs discussed below, it is reasonable to select direct clipping for the left side of the colon if technically feasible.
EBL can achieve hemostasis even in active CDB, but the procedure time is longer than that with clipping. One case of delayed perforation was observed in our study. In the previously mentioned Japanese study based on the Nationwide ALGIB endoscopy dataset, all cases of delayed perforation occurred after EBL for left-sided CDB [29] . Furthermore, colonic diverticulitis occurred after endoscopic ligation and indirect clipping, but not after direct clipping. Frequency of delayed perforation after EBL has been reported to be as low as 0.31% (2/638) [16] , but all such cases required surgical intervention [17] [18] [19]. Our patient with delayed perforation had perforations at two sites, making it less likely that EBL was the direct cause of the perforation and raising the possibility that medications (prednisolone and tocilizumab) for collagen disease were associated with the perforation [32] [33]. However, when performing endoscopic hemostasis for CDB in patients at high risk of delayed perforation (e.g., those on high-dose steroids [19] or tocilizumab [32] [33]), it may be preferable to choose a treatment modality with a low risk of perforation, such as clipping or injection of a self-assembling peptide material (PuraStat; 3-D Matrix, Tokyo, Japan) [34] . Frequency of diverticulitis after indirect clipping has been reported to be as low as 0.7% [29] , but it is important to consider. We speculate that complete closure of the diverticulum by indirect clipping increases pressure in the diverticulum, which increases risk of bacteremia [35] and diverticulitis. Therefore, from the point of view of AEs, direct clipping should be chosen when clipping is performed.
This study has some limitations. First, it had a retrospective, single-center design and was performed in a Japanese population, so selection bias cannot be excluded. Moreover, although patient characteristics were balanced by PSM, endoscopic findings of SRH differed between the clipping and EBL groups because the hemostatic method was determined based on endoscopic findings at the bleeding point. Therefore, the effectiveness of clipping and EBL could not be directly compared in this study. Multicenter, prospective studies are needed to validate our findings. The study also has some strengths, in that we collected detailed information about, for example, endoscopic findings (e.g., type and location of SRH) and extravasation on CT as well as long-term follow-up data. Moreover, there were few missing values in the data collected.
Conclusions
In conclusion, our results suggest that the endoscopic method for hemostasis in cases of CDB should be determined based on maneuverability of the endoscope, visibility at the bleeding point, and risk of complications. If direct clip placement for the bleeding point is feasible, selection of direct clipping is acceptable. The strategy of selecting clipping or EBL according to visibility at the bleeding point and maneuverability of the endoscope is reasonable in terms of effectiveness, efficiency, and safety of treatment.
Correction: Useful treatment selection strategy for endoscopic hemostasis in colonic diverticular bleeding according to endoscopic findings (with video)
In the above-mentioned article Figure 2 was corrected. This was corrected in the online version on 02.04.2025.
Conflict of Interest
The authors declare that they have no conflict of interest.
-
References
- 1 Sengupta N, Feuerstein JD, Jairath V. et al. Management of patients with acute lower gastrointestinal bleeding: An updated ACG guideline. Am J Gastroenterol 2023; 118: 208-231
- 2 Nagata N, Kobayashi K, Yamauchi A. et al. Identifying bleeding etiologies by endoscopy affected outcomes in 10,342 cases with hematochezia: CODE BLUE-J Study. Am J Gastroenterol 2021; 116: 2222-2234
- 3 Jensen DM, Ohning GV, Kovacs TOG. et al. Natural history of definitive diverticular hemorrhage based on stigmata of recent hemorrhage and colonoscopic Doppler blood flow monitoring for risk stratification and definitive hemostasis. Gastrointest Endosc 2016; 83: 416-423
- 4 Jensen DM, Machicado GA, Jutabha R. et al. Urgent colonoscopy for the diagnosis and treatment of severe diverticular hemorrhage. N Engl J Med 2000; 342: 78-82
- 5 Gobinet-Suguro M, Nagata N, Kobayashi K. et al. Treatment strategies for reducing early and late recurrence of colonic diverticular bleeding based on stigmata of recent hemorrhage: a large multicenter study. Gastrointest Endosc 2022; 95: 1210-1222.e12
- 6 Kumar A, Artifon E, Chu A. et al. Effectiveness of endoclips for the treatment of stigmata of recent hemorrhage in the colon of patients with acute lower gastrointestinal tract bleeding. Dig Dis Sci 2011; 56: 2978-2986
- 7 Kaltenbach T, Watson R, Shah J. et al. Colonoscopy with clipping is useful in the diagnosis and treatment of diverticular bleeding. Clin Gastroenterol Hepatol 2012; 10: 131-137
- 8 Nagata N, Niikura R, Ishii N. et al. Cumulative evidence for reducing recurrence of colonic diverticular bleeding using endoscopic clipping versus band ligation: Systematic review and meta-analysis. J Gastroenterol Hepatol 2021; 36: 1738-1743
- 9 Strate LL, Gralnek IM. ACG Clinical Guideline: Management of patients with acute lower gastrointestinal bleeding. Am J Gastroenterol 2016; 111: 459-474
- 10 Yen EF, Ladabaum U, Muthusamy VR. et al. Colonoscopic treatment of acute diverticular hemorrhage using endoclips. Dig Dis Sci 2008; 53: 2480-2485
- 11 Xavier AT, Campos JF, Robinson L. et al. Endoscopic clipping for gastrointestinal bleeding: emergency and prophylactic indications. Ann Gastroenterol Hepatol 2020; 33: 563-570
- 12 Nagata N, Ishii N, Kaise M. et al. Long-term recurrent bleeding risk after endoscopic therapy for definitive colonic diverticular bleeding: band ligation versus clipping. Gastrointest Endosc 2018; 88: 841-853.e4
- 13 Kishino T, Kanemasa K, Kitamura Y. et al. Usefulness of direct clipping for the bleeding source of colonic diverticular hemorrhage (with videos). Endosc Int Open 2020; 8: E377-E385
- 14 Kishino T, Nagata N, Kobayashi K. et al. Endoscopic direct clipping versus indirect clipping for colonic diverticular bleeding: A large multicenter cohort study. United European Gastroenterol J 2022; 10: 93-103
- 15 Setoyama T, Ishii N, Fujita Y. Enodoscopic band ligation (EBL) is superior to endoscopic clipping for the treatment of colonic diverticular hemorrhage. Surg Endosc 2011; 25: 3574-3578
- 16 Kobayashi K, Nagata N, Furumoto Y. et al. Effectiveness and adverse events of endoscopic clipping versus band ligation for colonic diverticular hemorrhage: a large-scale multicenter cohort study. Endoscopy 2022; 54: 735-744
- 17 Sato Y, Yasuda H, Fukuoka A. et al. Delayed perforation after endoscopic band ligation for colonic diverticular hemorrhage. Clin J Gastroenterol 2020; 13: 6-10
- 18 Tominaga N, Ogata S, Esaki M. Rare complication of endoscopic band ligation for colonic diverticular bleeding. JGH Open 2020; 4: 1244-1245
- 19 Takahashi S, Inaba T, Tanaka N. Delayed perforation after endoscopic band ligation for treatment of colonic diverticular bleeding. Dig Endosc 2016; 28: 484
- 20 Kishino T, Kitaichi T, Kanemasa K. Usefulness of water immersion observations to identify the stigmata of hemorrhage in colonic diverticular bleeding. Dig Endosc 2018; 30: 121-122
- 21 Ishii N, Setoyama T, Deshpande GA. et al. Endoscopic band ligation for colonic diverticular hemorrhage. Gastrointest Endosc 2012; 75: 382-387
- 22 Charlson ME, Pompei P, Ales KL. et al. A new method of classifying prognostic comorbidity in longitudinal studies: development and validation. J Chronic Dis 1987; 40: 373-383
- 23 Nagata N, Ishii N, Manabe N. et al. Guidelines for Colonic Diverticular Bleeding and Colonic Diverticulitis: Japan Gastroenterological Association. Digestion 2019; 99: 1-26
- 24 Ishii N, Hirata N, Omata F. et al. Location in the ascending colon is a predictor of refractory colonic diverticular hemorrhage after endoscopic clipping. Gastrointest Endosc 2012; 76: 1175-1181
- 25 Saito M, Sudo G, Takai S. et al. Direct clipping using underwater inversion method for colonic diverticular bleeding. VideoGIE 2022; 7: 187-189
- 26 Takada J, Arao M, Kojima K. et al. Usefulness of water pressure observation in detection and direct clipping of source of colonic diverticular bleeding. Endoscopy 2023; 55: E753-E754
- 27 Kawanishi K, Kato J, Kakimoto T. et al. Risk of colonic diverticular rebleeding according to endoscopic appearance. Endosc Int Open 2018; 6: E36-E42
- 28 Suzuki S, Esaki M, Ichijima R. Direct clipping method with a repositioning endoscopic clip for colonic diverticular bleeding. Dig Endosc 2020; 32: e67-e68
- 29 Aoki T, Sadashima E, Kobayashi K. et al. High risk stigmata and treatment strategy for acute lower gastrointestinal bleeding: a nationwide study in Japan. Endoscopy 2024; 56: 291-301
- 30 Sadahiro S, Ohmura T, Yamada Y. et al. Analysis of length and surface area of each segment of the large intestine according to age, sex and physique. Surg Radiol Anat 1992; 14: 251-257
- 31 Niikura R, Nagata N, Shimbo T. et al. Colonoscopy can miss diverticula of the left colon identified by barium enema. World J Gastroenterol 2013; 19: 2362-2367
- 32 Strangfeld A, Richter A, Siegmund B. et al. Risk for lower intestinal perforations in patients with rheumatoid arthritis treated with tocilizumab in comparison to treatment with other biologic or conventional synthetic DMARDs. Ann Rheum Dis 2017; 76: 504-510
- 33 Gout T, Ostör AJK, Nisar MK. Lower gastrointestinal perforation in rheumatoid arthritis patients treated with conventional DMARDs or tocilizumab: a systematic literature review. Clin Rheumatol 2011; 30: 1471-1474
- 34 Murakami T, Kamba E, Haga K. et al. Emergency endoscopic hemostasis for gastrointestinal bleeding using a self-assembling peptide: A case series. Medicina 2023; 59
- 35 Kume K, Yamasaki M, Yoshikawa I. Sepsis caused by endoscopic clipping for colonic diverticular bleeding: a rare complication. World J Gastroenterol 2009; 15: 3817-3818
Correspondence
Publication History
Received: 24 June 2024
Accepted after revision: 14 November 2024
Accepted Manuscript online:
21 November 2024
Article published online:
07 January 2025
© 2025. The Author(s). This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial-License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/).
Georg Thieme Verlag KG
Oswald-Hesse-Straße 50, 70469 Stuttgart, Germany
Takaaki Kishino, Yoko Kitamura, Takashi Okuda, Naoki Okamoto, Takayuki Sawa, Maiko Yamakawa, Kazuyuki Kanemasa. Useful treatment selection strategy for endoscopic hemostasis in colonic diverticular bleeding according to endoscopic findings (with video). Endosc Int Open 2025; 13: a24711016.
DOI: 10.1055/a-2471-1016
-
References
- 1 Sengupta N, Feuerstein JD, Jairath V. et al. Management of patients with acute lower gastrointestinal bleeding: An updated ACG guideline. Am J Gastroenterol 2023; 118: 208-231
- 2 Nagata N, Kobayashi K, Yamauchi A. et al. Identifying bleeding etiologies by endoscopy affected outcomes in 10,342 cases with hematochezia: CODE BLUE-J Study. Am J Gastroenterol 2021; 116: 2222-2234
- 3 Jensen DM, Ohning GV, Kovacs TOG. et al. Natural history of definitive diverticular hemorrhage based on stigmata of recent hemorrhage and colonoscopic Doppler blood flow monitoring for risk stratification and definitive hemostasis. Gastrointest Endosc 2016; 83: 416-423
- 4 Jensen DM, Machicado GA, Jutabha R. et al. Urgent colonoscopy for the diagnosis and treatment of severe diverticular hemorrhage. N Engl J Med 2000; 342: 78-82
- 5 Gobinet-Suguro M, Nagata N, Kobayashi K. et al. Treatment strategies for reducing early and late recurrence of colonic diverticular bleeding based on stigmata of recent hemorrhage: a large multicenter study. Gastrointest Endosc 2022; 95: 1210-1222.e12
- 6 Kumar A, Artifon E, Chu A. et al. Effectiveness of endoclips for the treatment of stigmata of recent hemorrhage in the colon of patients with acute lower gastrointestinal tract bleeding. Dig Dis Sci 2011; 56: 2978-2986
- 7 Kaltenbach T, Watson R, Shah J. et al. Colonoscopy with clipping is useful in the diagnosis and treatment of diverticular bleeding. Clin Gastroenterol Hepatol 2012; 10: 131-137
- 8 Nagata N, Niikura R, Ishii N. et al. Cumulative evidence for reducing recurrence of colonic diverticular bleeding using endoscopic clipping versus band ligation: Systematic review and meta-analysis. J Gastroenterol Hepatol 2021; 36: 1738-1743
- 9 Strate LL, Gralnek IM. ACG Clinical Guideline: Management of patients with acute lower gastrointestinal bleeding. Am J Gastroenterol 2016; 111: 459-474
- 10 Yen EF, Ladabaum U, Muthusamy VR. et al. Colonoscopic treatment of acute diverticular hemorrhage using endoclips. Dig Dis Sci 2008; 53: 2480-2485
- 11 Xavier AT, Campos JF, Robinson L. et al. Endoscopic clipping for gastrointestinal bleeding: emergency and prophylactic indications. Ann Gastroenterol Hepatol 2020; 33: 563-570
- 12 Nagata N, Ishii N, Kaise M. et al. Long-term recurrent bleeding risk after endoscopic therapy for definitive colonic diverticular bleeding: band ligation versus clipping. Gastrointest Endosc 2018; 88: 841-853.e4
- 13 Kishino T, Kanemasa K, Kitamura Y. et al. Usefulness of direct clipping for the bleeding source of colonic diverticular hemorrhage (with videos). Endosc Int Open 2020; 8: E377-E385
- 14 Kishino T, Nagata N, Kobayashi K. et al. Endoscopic direct clipping versus indirect clipping for colonic diverticular bleeding: A large multicenter cohort study. United European Gastroenterol J 2022; 10: 93-103
- 15 Setoyama T, Ishii N, Fujita Y. Enodoscopic band ligation (EBL) is superior to endoscopic clipping for the treatment of colonic diverticular hemorrhage. Surg Endosc 2011; 25: 3574-3578
- 16 Kobayashi K, Nagata N, Furumoto Y. et al. Effectiveness and adverse events of endoscopic clipping versus band ligation for colonic diverticular hemorrhage: a large-scale multicenter cohort study. Endoscopy 2022; 54: 735-744
- 17 Sato Y, Yasuda H, Fukuoka A. et al. Delayed perforation after endoscopic band ligation for colonic diverticular hemorrhage. Clin J Gastroenterol 2020; 13: 6-10
- 18 Tominaga N, Ogata S, Esaki M. Rare complication of endoscopic band ligation for colonic diverticular bleeding. JGH Open 2020; 4: 1244-1245
- 19 Takahashi S, Inaba T, Tanaka N. Delayed perforation after endoscopic band ligation for treatment of colonic diverticular bleeding. Dig Endosc 2016; 28: 484
- 20 Kishino T, Kitaichi T, Kanemasa K. Usefulness of water immersion observations to identify the stigmata of hemorrhage in colonic diverticular bleeding. Dig Endosc 2018; 30: 121-122
- 21 Ishii N, Setoyama T, Deshpande GA. et al. Endoscopic band ligation for colonic diverticular hemorrhage. Gastrointest Endosc 2012; 75: 382-387
- 22 Charlson ME, Pompei P, Ales KL. et al. A new method of classifying prognostic comorbidity in longitudinal studies: development and validation. J Chronic Dis 1987; 40: 373-383
- 23 Nagata N, Ishii N, Manabe N. et al. Guidelines for Colonic Diverticular Bleeding and Colonic Diverticulitis: Japan Gastroenterological Association. Digestion 2019; 99: 1-26
- 24 Ishii N, Hirata N, Omata F. et al. Location in the ascending colon is a predictor of refractory colonic diverticular hemorrhage after endoscopic clipping. Gastrointest Endosc 2012; 76: 1175-1181
- 25 Saito M, Sudo G, Takai S. et al. Direct clipping using underwater inversion method for colonic diverticular bleeding. VideoGIE 2022; 7: 187-189
- 26 Takada J, Arao M, Kojima K. et al. Usefulness of water pressure observation in detection and direct clipping of source of colonic diverticular bleeding. Endoscopy 2023; 55: E753-E754
- 27 Kawanishi K, Kato J, Kakimoto T. et al. Risk of colonic diverticular rebleeding according to endoscopic appearance. Endosc Int Open 2018; 6: E36-E42
- 28 Suzuki S, Esaki M, Ichijima R. Direct clipping method with a repositioning endoscopic clip for colonic diverticular bleeding. Dig Endosc 2020; 32: e67-e68
- 29 Aoki T, Sadashima E, Kobayashi K. et al. High risk stigmata and treatment strategy for acute lower gastrointestinal bleeding: a nationwide study in Japan. Endoscopy 2024; 56: 291-301
- 30 Sadahiro S, Ohmura T, Yamada Y. et al. Analysis of length and surface area of each segment of the large intestine according to age, sex and physique. Surg Radiol Anat 1992; 14: 251-257
- 31 Niikura R, Nagata N, Shimbo T. et al. Colonoscopy can miss diverticula of the left colon identified by barium enema. World J Gastroenterol 2013; 19: 2362-2367
- 32 Strangfeld A, Richter A, Siegmund B. et al. Risk for lower intestinal perforations in patients with rheumatoid arthritis treated with tocilizumab in comparison to treatment with other biologic or conventional synthetic DMARDs. Ann Rheum Dis 2017; 76: 504-510
- 33 Gout T, Ostör AJK, Nisar MK. Lower gastrointestinal perforation in rheumatoid arthritis patients treated with conventional DMARDs or tocilizumab: a systematic literature review. Clin Rheumatol 2011; 30: 1471-1474
- 34 Murakami T, Kamba E, Haga K. et al. Emergency endoscopic hemostasis for gastrointestinal bleeding using a self-assembling peptide: A case series. Medicina 2023; 59
- 35 Kume K, Yamasaki M, Yoshikawa I. Sepsis caused by endoscopic clipping for colonic diverticular bleeding: a rare complication. World J Gastroenterol 2009; 15: 3817-3818