

Subscribe to RSS
DOI: 10.1055/a-2648-6856
Extravasation of Intraarticular Fluid Injection Following Canine Elbow Arthroscopy: A Cadaveric Study
Authors

Abstract
Objective
To investigate extravasation of contrast media injected intraarticularly, either immediately following elbow arthroscopy or after arthrocentesis using computed tomographic (CT) imaging at different time points.
Study Design
Cadaveric dog model.
Methods
A total of 16 elbows of eight canine cadavers (median age 10.2 years, 5.6 to 16.8 years; median weight 35.0 kg, 26.0 to 42.0 kg) were randomly assigned to the arthroscopy group with the contralateral elbow as control. Right after elbow arthroscopy, both elbows were injected with 2.5 mL contrast fluid. Elbow CT scans were obtained at seven time points. To detect a possible loss of contrast medium from the joint, both the total volume and intensity of the contrast fluid were measured intra- and extraarticularly using rendering software. To compare volume and intensity of contrast fluid, a simple linear model and a linear mixed effect model were used.
Results
The total volume of contrast-enhanced fluid was increased (avg. difference: 5115 mm3; linear model std. estimate: 1.69, std. error 0.10) and the total intensity decreased (avg. difference: 1330 Hounsfield Units; linear model std. estimate: −1.66, std. error 0.11) in the arthroscopy group compared with the control. Neither total volume nor total intensity of contrast-enhanced fluid changed significantly within 15 minutes.
Conclusion
Extravasation of intraarticular injected contrast fluid after elbow arthroscopy without a significant effect of time could be shown. Injection of liquid therapeutics, e.g., orthobiologics, at a later point after arthroscopy should be considered.
Introduction
Arthroscopy is one of the most frequently used diagnostic tools for elbow pathology in dogs.[1] [2] [3] Besides its significance as a diagnostic tool, arthroscopy also offers the opportunity of minimally invasive surgical treatment for many pathologic conditions of the elbow joint.[4] [5]
Agents like local anesthetics,[6] [7] [8] opioids,[6] [9] glucocorticoids,[10] [11] [12] hyaluronic acid,[10] [13] [14] and also biological active agents such as platelet-rich plasma[10] [13] [15] [16] and stem cells[14] [17] are injected into affected joint(s). Although some surgeons perform joint injections immediately after the arthroscopic procedure, others prefer to inject at a later time point, because they speculate that, although arthroscopy is considered to be minimally invasive, the portals required for elbow arthroscopy might allow for leakage of the injected agent into the periarticular tissues, diminishing its intraarticular therapeutic potential.
In veterinary medicine Blumhagen and colleagues evaluated the effect of arthroscopy on extravasation scores after contrast fluid injection in a cadaveric dog model.[18] In their work they could not show a significant effect of an arthroscopy treatment on extravasation scores in 3D-CT models compared with an arthrocentesis control group. They also compared the effect of different volumes of injected contrast fluid and could show increased extravasation scores in the 4 mL versus the 2 mL group, regardless of arthroscopy treatment or arthrocentesis.[18]
However, other veterinary and human studies have shown significant extravasation of irrigation fluid during arthroscopic procedures, making extravasation of intraarticular administered fluids likely.[19] [20] [21] [22] The question also arises as to what effect a longer observation period could have on possible extravasation of intraarticular injected fluids. The purpose of this cadaveric study was to investigate extravasation of contrast media injected intraarticularly, either immediately following elbow arthroscopy or after simple arthrocentesis using computed tomographic (CT) imaging of the elbow region at different time points.
Our hypothesis was that there is a significantly increased extravasation of contrast media in the arthroscopy group compared with the arthrocentesis group, which increases gradually over the various time points.
Materials and Methods
Dogs with body weight >20 kg, humanely euthanized in accordance with current international guidelines for animal welfare (EU Convention on the protection of animals revised directive 86/609/EEC) for reasons unrelated to this study, were potential candidates. With the owner's consent, they were screened for any form of elbow pathology, based on orthogonal radiographs, and subsequently frozen at −20°C, if they showed no abnormal finding. Prior to further processing, the cadavers were thawed for 48 h at room temperature. For each specimen, the determination of whether the left or right elbow joint would be assigned to the arthroscopy group (group 1) or the arthrocentesis group (group 2) was made through a random assignment process using a coin toss. Regardless of the group assignment, both elbow joints were clipped as for a standard arthroscopic procedure. For elbow arthroscopy, the dogs were positioned in lateral recumbency, with the elbow joint to be operated on at the edge of the table. Elbow arthroscopy was performed using the standard medial portals and a 1.9-mm needle arthroscope and a 2.4-mm arthroscopic sleeve (NanoScope, Arthrex Inc., Naples, FL 34108, USA).[23] To achieve a permanent flow of fluid, a 1-L Ringer infusion solution (Ringer-Infusionslösung B. Braun, B. Braun Melsungen AG, 34209 Melsungen, Germany) was connected to the arthroscopic sleeve using an infusion set (Infusionsset, Eickemeyer-Medizintechnik für Tierärzte KG, 78532 Tuttlingen, Germany) and a pressure cuff (Metpak, Rudolf Riester GmbH, 72417 Jungingen, Germany). A 20-gauge hypodermic needle was placed into the olecranon fossa as an egress cannula (Hypodermic Needle; Covetrus BV, 5431 SLCuijk, Netherlands). The pressure of the system was kept constant between 40 and 50 mmHg during the arthroscopy.[5] [18] [23] After intraarticular placement of the camera, the instrument portal was established under visual control, just caudal to the medial collateral ligament. After gentle enlargement of the working portal with a curved mosquito forceps, an arthroscopic palpation hook was inserted and routine exploration of the joint was performed, including palpation of the medial joint structures. All arthroscopic procedures, including arthrocentesis and portal placing, were performed by a board-certified surgeon (P.S.).[1] At the end of the diagnostic arthroscopy and following removal of the scope, the arthroscopic sleeve, and the palpation hook, aspiration of the remaining irrigation fluid from within the joint was performed via the egress cannula placed into the olecranon fossa. Subsequently, 2.5 mL of undiluted contrast media (Xenetix ® 300; 300 mg Iod/mL, Guerbet, Roissy CdG Cedex, France) were injected via the same needle using a 3-mL syringe (Omnifix® Luer Solo 3 mL, REF 4616025V, B. Braun Melsungen AG, 34209 Melsungen, Germany), ensuring true intraarticular contrast media application. After this, the dogs were turned onto the opposite side and arthrocentesis at exactly the corresponding location as the para anconeal egress cannula on the arthroscopy side was performed. Intraarticular needle placement was confirmed by aspiration of synovial fluid and 2.5 mL of contrast media were injected into the joint. Without further delay, axial CT imaging (SOMATOM go.now, Siemens, Erlangen, Germany) of both elbow joints was acquired (KVP 130 V; mA 160; 0.6 mm slice thickness; 0.30 mm increment). To allow for standardized imaging of all investigated elbow joints, the cadavers were positioned in dorsal recumbency, with both front limbs in parallel and the elbow joints at 135 degrees, using a custom-made positioning device ([Fig. 1]). Time between injection of contrast media after arthroscopy as well as arthrocentesis and the start of CT scanning was recorded for every specimen.
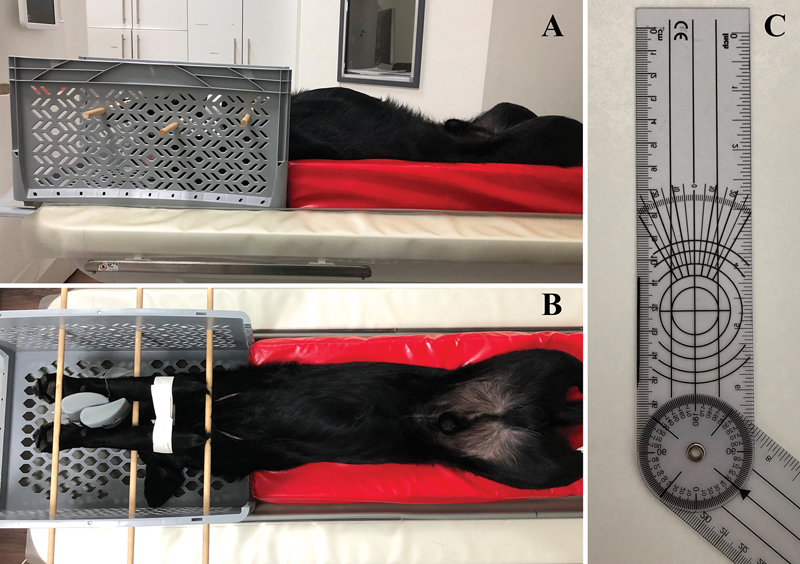
To allow monitoring of contrast medium leakage over time, consecutive scans were performed at seven predefined time points: T0, T1 (T0 + 2 minutes), T2 (T0 + 4 minutes), T3 (T0 + 6 minutes), T4 (T0 + 8 minutes), T5 (T0 + 10 minutes), and T6 (T0 + 15 minutes). These time intervals were chosen to investigate whether a possible extravasation occurs exclusively just after the operation or also in the further short-term course. To detect a possible loss of contrast medium from the joint, both the total volume and the total intensity of the contrast medium-enhanced fluid were measured both intra- and extraarticularly. For each elbow scan, one single investigator (L.R.) calculated 3D renderings of the intraarticular and extracapsular contrast media–enhanced fluid, using the open-source software ITK-SNAP (Version 3.8.0, July 22, 2022).[24] [25] [26] This was performed in a nonrandomized and nonblinded manner. In each cross-sectional image, the intra- and extraarticular contrast media–enhanced fluid was manually segmented using the software's internal brush tool. The visual difference in image contrast between soft tissues, the contrast media–enhanced fluid, and bone structures was used to delineate the region of interest. Finally, the volume (mm3) of the segmented intra- and extraarticular contrast media–enhanced fluid, as well as its mean intensity (Hounsfield Units, HU), was calculated from the voxel volumes segmented in the outlined manner. This process was performed for each elbow, in each specimen, and at all seven time points. The volumes segmented in this way represent the sum of intraarticular and extraarticular contrast medium–enhanced fluid. In the same way, the segmented intensity represents the intensity for the entire measured volume, including intraarticular and extraarticular contrast-enhanced fluid. To simplify the phrasing in the following, the terms volume and intensity of the contrast medium–enhanced fluid represent the sum of intraarticular and extraarticular volume and the corresponding intensity. The two segmented contrast media–enhanced fluid volumes of each specimen at a certain time point were labeled accordingly as arthroscopy (AS) in green, or arthrocentesis (AC) in yellow ([Fig. 2]).

Data Analysis
The effect of the arthroscopy treatment on fluid volume and fluid intensity was first tested using two separate linear models, with time as a covariate. For each model, we tested for the significance of the treatment variable using likelihood ratio tests, which consisted in comparing the goodness of fit of models fitted with or without the variable. Linear mixed effect models were then performed to further test for potential basal differences among dogs in fluid volume and intensity, with arthroscopy treatments and time as fixed effects and the specimen ID as a random effect. Large random effect variance would indicate large variance among dogs in their basal fluid intensity or volume. P-values lower than 0.05 indicated statistically significant results. Statistical analyses were performed using R and the lme4 package.[27] Response variables were standardized prior to analyses.
Results
A total of eight dogs, meeting the inclusion criteria, were included in the study. The median age of the dog was 10.2 years (5.6 to 16.8 years) and the median weight was 35.0 kg (26.0 to 42.0 kg). There were two females, two males, three neutered females, and one neutered male. Breeds are shown in [Supplementary Table S1] (available in the online version only). As a result of randomization, arthroscopy was performed on six right and two left elbow joints. The average time interval between the intraarticular application of the contrast agent and the start of the CT scans (T0) was 10 minutes (SD 2).
The volume of contrast media–enhanced fluid measured over all seven time points was considerably larger in the arthroscopy group compared with the arthrocentesis group (likelihood ratio test: volume χ2 = 144.6, df = 1, p-value < 0.0001) with an average of 11,663 mm3 (S.D. 221.13) of fluid in the arthroscopy group and 6,548 mm3 (S.D. 108.23) in the arthrocentesis group. On average volume was greater by 5,115 mm3 in the arthroscopy group (linear model standardized estimate: 1.69, std. error 0.10) ([Table 1] and [Supplementary Fig. S1], available in the online version only).
Abbreviations: Int., intensity in Hounsfield Units; min., minutes; T, time point (0 to 6) in minutes; Vol., volume in mm3.
The intensity of the contrast media–enhanced fluid measured across all seven time points was significantly lower in the arthroscopy group (mean: 739.33 HU, SD: 246.68) compared with the arthrocentesis group (mean: 2069.60 HU, SD: 605.34), as indicated by a likelihood ratio test (χ2 = 135.9, df = 1, p < 0.0001). On average, the measured intensity of contrast media–enhanced fluid was lower by 1,330 HU in the arthroscopy group (linear model standardized estimate: −1.66, std. error 0.11) ([Table 1] and [Supplementary Fig. S2], available in the online version only).
There was no significant change in the measured volume or intensity of contrast media–enhanced fluid over the study period of 15 minutes, for either the arthroscopy or the arthrocentesis group (likelihood ratio test: volume χ2 = 1.69, df = 6, p-value = 0.94, intensity χ2 = 0.63, df = 6, p-value = 0.99) ([Table 1], [Figs. 3] and [4]).


Linear mixed effect models revealed high variance among dogs and high consistency within each dog regarding how they responded to the treatment, in both contrast media–enhanced fluid volume (random intercept variance effect: 0.1044, corresponding to a 0.35 intraclass correlation) and intensity (random intercept variance effect: 0.2457, corresponding to a 0.74 intraclass correlation) ([Supplementary Fig. S1] and [S2], available in the online version only). Mixed effect model estimates for the effect of the arthroscopy treatment on fluid volume and intensity are remarkably close to estimates of simpler linear models, with smaller estimated standard deviations in mixed effect models (volume: mixed model standardized estimate: 1.69, std. error 0.08; intensity: mixed model standardized estimate: −1.67, std. error 0.05), arguing for a strong effect of arthroscopy on fluid volume and intensity in linear mixed effect models.
Discussion
In our study setup, a significant extravasation of contrast medium was observed in the arthroscopy group, which supports the first hypothesis. However, the second hypothesis was not confirmed, as neither the intensity of the contrast medium–enhanced fluid nor the volume changed within the first 15 minutes following application.
In the control group, the contrast agent was clearly delineated from the surrounding periarticular tissue in the CT images and showed a high intensity in all cases. It can be assumed that the injected contrast agent remains condensed inside the capsular space leaving the joint capsule intact. If, on the other hand, the distribution pattern of the contrast agent in the arthroscopy group is compared with the control group, no clear delineation and a diffuse spread in the periarticular tissue was observed. As a result, the measured fluid volume increases and the measured fluid intensity decreases.
Since, as in the study of Blumhagen and colleagues, applied irrigation fluid was removed after the arthroscopy and the contrast medium was only administered afterwards, it can be assumed that the increase in volume and the decrease in intensity are caused by the contrast medium leaking out of the intraarticular space and spreading into the periarticular tissue.[18] Extravasation of irrigation fluid is a well-described phenomenon during and after arthroscopy in both humans and dogs.[19] [20] [21] In human orthopedic traumatology, the so-called saline load test is used to visualize even small traumatic joint capsule injuries.[28] [29] [30] A defined amount of sterile saline solution is injected into the affected joint to show leakage of this fluid, which would indicate a lesion of the joint capsule. This procedure has been shown to have a high sensitivity and a high specificity.[28] [29] [30] The extravasation of fluids during saline load test and during irrigation in arthroscopic procedures through lesions of the joint capsule support our hypothesis that a leakage of fluids through the arthroscopic ports occurs.
The decrease in the intensity of the contrast medium in the arthroscopy group can be explained in a similar way. Although the contrast fluid in the control group remains condensed in the joint space and therefore no dilution occurs, in the arthroscopy group, there is a loss of intensity due to extravasation and associated increase in volume due to a higher distribution between the surrounding soft tissues. In addition, a certain dilutional effect on the injected contrast agent, which decreased the intensity in the arthroscopy group, cannot be excluded. Both the intraarticular synovium and the irrigation fluid applied during arthroscopy may cause such a dilutional effect. In both human and veterinary studies, synovial and effusion fluid was removed by puncture prior to injection of contrast medium for CT arthrography.[31] [32] [33] Despite this procedure, Samii and colleagues[33] noted that it was probably not possible to remove all of the fluid and that this could have led to a potential dilutional effect of the contrast medium, resulting in poorer contrast medium resolution. However, since a dilutional effect by synovia should also influence the intensity in the control group to the same extent, no influence on the results of the study should be expected. After the arthroscopic procedure, care was taken to evacuate the joint via arthrocentesis under visual control to the best possible extent. Investigating the possible dilutional effect of irrigation fluids after arthroscopy, Stopka and colleagues evaluated intraarticular injected trypan blue solution in a human knee cadaveric model.[34] After a routine arthroscopic exploration, an attempt was made to remove all irrigation fluid from the joint via the empty arthroscopy cannula by moving the joint and massaging the fluid out before the solution was injected. After several range of motions, samples of the intraarticular fluid were obtained and spectometrically analyzed and revealed a dilutional effect of approximately 27%.[34] Considering the results of our study with a percentage decrease in intensity by 64.3%, the demonstrated dilutional effect is approximately twice as high as described by Stopka and colleagues, confirming the hypothesis of dilution due to extravasation.
It is difficult to say why in our experiment the dilutional effect is almost twice as large, especially since we also tried to remove the irrigation fluid before injection. Possible explanations are that the removal of irrigation fluid was not effective enough in our study and that the measurement methods are different as in the mentioned study only the intraarticular fluid concentration was compared with the original solution. In our case, however, all contrast fluid, including the extracapsular component, was also measured, so that not only a dilutional effect due to remaining irrigation fluid, but also a dilutional effect due to distribution into the surrounding tissue was taken into account.
With our manual measurement of the intra- and extracapsular contrast agent, we observed that in some areas there is an overlap in the intensities measured in HU between the different tissues and the diluting contrast fluid. When trying to automatically calculate the contrast agent volumes based on defined thresholds of HU values, there were frequent errors compared with the manual measurements in our work. Unintentional additions as well as subtractions of areas were observed in the automated procedure compared with the manual method. This observation in our study could explain the different results compared with the work of Blumhagen and colleagues which used an automated procedure.[18]
Various therapeutic agents such as local anesthetics, or orthobiologics, e.g., platelet-rich plasma, have been described for intraarticular application. Several studies describing a positive effect of local anesthetics injected intraarticularly after arthroscopy.[6] [7] [8] One possible explanation is that local anesthetics can still achieve an adequate effect after extravasation due to resorption in the surrounding tissues. This might be different for specific agents in the treatment of osteoarthritis. The use of orthobiologics for the therapy of cartilage lesions or osteoarthritis shows good medium- to long-term effects in dogs.[10] [13] [16] [35] [36] As far as the mechanism of action of platelet-rich plasma is understood, it locally stimulates a variety of processes that promote tissue healing, such as cell recruitment and angiogenesis, via various growth factors.[37] [38] [39] Due to these effects in the area of the affected lesion, local application at an appropriate concentration appears to be indicated even if, according to the current literature, no clear statements can be made about specific concentrations.[37] Taking these considerations into account and given the dilution effect of the contrast medium–enhanced fluid volume of 64.3%, the question must be asked whether enough of the therapeutic fluid remains at the desired location and if an effective concentration can be achieved with an injection immediately after elbow arthroscopy. In a recent study by Scharpf and Theyse, no significant clinical effect was observed following intraarticular injection of autologous conditioned plasma (ACP) after elbow arthroscopy and subtotal coronoidectomy compared with a control group with injection of a placebo.[40] Future studies should evaluate which concentrations of platelet-rich plasma are needed intraarticularly to achieve an adequate effect level. Until then injection of orthobiologics might be considered at a later time point.
The fact that neither intensity nor volume changed significantly over the course of the various measurement points indicates that the main effect of extravasation already occurred directly at time point T0. The causative extravasation therefore occurred directly after the arthroscopy and injection of contrast media. One possible explanation as to why even more fluid did not escape from the joints over the further course of time could be a lack of movement. In an in vivo scenario, there would most likely be even more extravasation due to the movement of the joints.
Our results also revealed high variance among dogs in each treatment group but high consistency in how each dog responded to the treatment. This means that dogs which showed higher fluid volume or intensity in the control group also showed higher fluid volume and intensity in the arthroscopy group. We speculate that the physiology of the dogs has an influence on the measured volumes and intensities but does not influence the ratio of extravasation.
Several limitations must be considered when interpreting the results of this study. First, the ex-vivo character of this study does not allow direct translation to the clinical field. The use of elbow joints of previously frozen cadaveric dogs might have compromised the integrity of the joint capsule. However, as the same dogs were used as their control, expected compromises to the joint capsule should occur to the same amount in the control group. As the use of thawed joints showed no adverse effects in the work of Samii and colleagues and Gendler and colleagues with an similar setup, we estimate the risk for effects in our study to be low.[33] [41] As previously discussed joint movement after injection could have a significant effect on extravasation and should therefore be considered in future studies.[18] [34] Since the contrast medium was administered without monitoring the application pressure and without blinding, this aspect could also represent a limitation. As the injection was easy and without resistance in all cases, an effect on increased extravasation due to increased application pressures appears to be low. But a certain variance in the application pressures during manual administration cannot be ruled out. Also, the widening of the arthroscopic ports with mosquito forceps may have contributed to an increased risk of extravasation. But as this is common practice in many institutions and is a described technique in the literature, we wanted to include this effect in our study setup.[18] [23] How great the effect of the widening really contributes to leakage cannot be clearly stated at this point. Future studies should evaluate whether there is a difference between widening and non-widening of arthroscopic portals. In addition, the pressure of 40 to 50 mmHg used for irrigation during arthroscopy can be criticized as relatively high. These pressures are described in the literature and are commonly used in practice, and we therefore wanted to consider the possible effects of these pressures in our experimental setup.[5] [18] [23] Whether there is a possible influence of different irrigation pressures on the extravasation behavior is beyond the scope of this study. Lastly, all CT measurements were performed by a single, non-blinded investigator, which might have caused a certain degree of bias.
Conclusion
In conclusion, we were able to show a significant extravasation of intraarticularly injected contrast fluid after arthroscopy by means of an increased volume and a decreased intensity in this cadaveric model. No significant effect of time on the contrast fluid volume and intensity could be shown. Injection of liquid therapeutics, e.g., orthobiologics, at a later time point after arthroscopy should be considered.
Conflict of Interest
P.A.S. works as consultant for Arthrex VetSystems. P.B. works as consultant for Arthrex VetSystems. M.G. works as a senior data scientist at the Swiss Data Science Center.
Notes
The abstract was presented at the annual ECVS meeting 2023 in Cracow, 01.07.2023 ( https://doi.org/10.1111/vsu.13989 ).
Authors' Contribution
L.R. contributed to compilation of all data, interpretation and processing of the data, drafting and revision of the manuscript; participation in the conception and design of the study. M.G. contributed in performing statistical analyses and produced illustrations. P.B. contributed to the design of the study, provided scientific, in-line editing of the manuscript. P.A.S. contributed to study idea, design of the study, was responsible for the arthroscopic procedures, oversaw data collection, interpreted data, and provided scientific, in-line editing of the manuscript.
-
References
- 1 Van Ryssen B, van Bree H, Simoens P. Elbow arthroscopy in clinically normal dogs. Am J Vet Res 1993; 54 (01) 191-198
- 2 Botazzoli AF, Ferraresi F, Travetti O, Martini FM, Mortellaro CM, Di Giancamillo M. Elbow dysplasia and lesions of the medial coronoid process: correlation between tomographic and arthroscopic findings in thirty cases. Vet Res Commun 2008; 32 (Suppl. 01) S247-S249
- 3 Goldhammer MA, Smith SH, Fitzpatrick N, Clements DN. A comparison of radiographic, arthroscopic and histological measures of articular pathology in the canine elbow joint. Vet J 2010; 186 (01) 96-103
- 4 Meyer-Lindenberg A, Langhann A, Fehr M, Nolte I. Arthrotomy versus arthroscopy in the treatment of the fragmented medial coronoid process of the ulna (FCP) in 421 dogs. Vet Comp Orthop Traumatol 2003; 16 (04) 204-210
- 5 van Bree HJJ, Van Ryssen B. Diagnostic and surgical arthroscopy in osteochondrosis lesions. Vet Clin North Am Small Anim Pract 1998; 28 (01) 161-189
- 6 Gurney MA, Rysnik M, Comerford EJ, Cripps PJ, Iff I. Intra-articular morphine, bupivacaine or no treatment for postoperative analgesia following unilateral elbow joint arthroscopy. J Small Anim Pract 2012; 53 (07) 387-392
- 7 Dutton TAG, Gurney MA, Bright SR. Intra-articular mepivacaine reduces interventional analgesia requirements during arthroscopic surgery in dogs. J Small Anim Pract 2014; 55 (08) 405-408
- 8 Kim JH, Seok SH, Park TY. et al. Analgesic effect of intra-articular ropivacaine injection after arthroscopic surgery on the shoulder joint in dogs. Vet Med (Praha) 2018; 63 (11) 513-521
- 9 Sammarco JL, Conzemius MG, Perkowski SZ, Weinstein MJ, Gregor TP, Smith GK. Postoperative analgesia for stifle surgery: a comparison of intra-articular bupivacaine, morphine, or saline. Vet Surg 1996; 25 (01) 59-69
- 10 Franklin SP, Cook JL. Prospective trial of autologous conditioned plasma versus hyaluronan plus corticosteroid for elbow osteoarthritis in dogs. Can Vet J 2013; 54 (09) 881-884
- 11 Alves JC, Santos A, Jorge P, Lavrador C, Carreira LM. The intra-articular administration of triamcinolone hexacetonide in the treatment of osteoarthritis. Its effects in a naturally occurring canine osteoarthritis model. PLoS ONE. 2021; 16 (01) e0245553
- 12 Tellegen A, Beukers M, Rudnik-Jansen I. et al. Intra-articular slow-release triamcinolone acetonide from polyesteramide microspheres as a treatment for osteoarthritis. Pharmaceutics 2021; 13 (03) 372
- 13 Alves JC, Santos A, Jorge P, Lavrador C, Carreira LM. Intraarticular triamcinolone hexacetonide, stanozolol, Hylan G-F 20 and platelet concentrate in a naturally occurring canine osteoarthritis model. Sci Rep 2021; 11 (01) 3118
- 14 Kim S, Elam L, Johnson V. et al. Intra-articular injections of allogeneic mesenchymal stromal cells vs. high molecular weight hyaluronic acid in dogs with osteoarthritis: exploratory data from a double-blind, randomized, prospective clinical trial. Front Vet Sci 2022; 9: 890704
- 15 Fahie MA, Ortolano GA, Guercio V. et al. A randomized controlled trial of the efficacy of autologous platelet therapy for the treatment of osteoarthritis in dogs. J Am Vet Med Assoc 2013; 243 (09) 1291-1297
- 16 Vilar JM, Manera ME, Santana A. et al. Effect of leukocyte-reduced platelet-rich plasma on osteoarthritis caused by cranial cruciate ligament rupture: a canine gait analysis model. PLoS One 2018; 13 (03) e0194752
- 17 Kim SE, Pozzi A, Chern YJ. et al. Intra-articular umbilical cord derived mesenchymal stem cell therapy for chronic elbow osteoarthritis in dogs: double-blinded, placebo-controlled clinical trial. Front Vet Sci 2019; 6: 474
- 18 Blumhagen EM, Spector DI, Fischetti AJ. Impact of arthroscopy on post-procedure intra-articular elbow injections: a cadaveric study. Vet Surg 2024; 53 (06) 988-998
- 19 Borgeat A, Bird P, Ekatodramis G, Dumont C. Tracheal compression caused by periarticular fluid accumulation: a rare complication of shoulder surgery. J Shoulder Elbow Surg 2000; 9 (05) 443-445
- 20 Lo IKY, Burkhart SS. Immediate postoperative fluid retention and weight gain after shoulder arthroscopy. Arthroscopy 2005; 21 (05) 605-610
- 21 Capito NM, Smith MJ, Stoker AM, Werner N, Cook JL. Hyperosmolar irrigation compared with a standard solution in a canine shoulder arthroscopy model. J Shoulder Elbow Surg 2015; 24 (08) 1243-1248
- 22 Beale BS, Hulse DA, Schulz KS, Whitney WO. Chapter 1 - History of arthroscopy. In: Beale BS, Hulse DA, Schulz KS, Whitney WO. eds. Small Animal Arthroscopy. W.B. Saunders; 2003: 1-3
- 23 Beale BS, Hulse DA, Schulz KS, Whitney WO. Chapter 4 - Arthroscopically assisted surgery of the elbow joint. In: Beale BS, Hulse DA, Schulz KS, Whitney WO. eds. Small Animal Arthroscopy. W.B. Saunders; 2003: 51-79
- 24 ITK-SNAP. Accessed July 22, 2022 at: www.itksnap.org
- 25 Yushkevich PA, Piven J, Hazlett HC. et al. User-guided 3D active contour segmentation of anatomical structures: significantly improved efficiency and reliability. Neuroimage 2006; 31 (03) 1116-1128
- 26 Smolders LA, Knell SC, Park B, Pozzi A, Meij BP, Steffen F. The effects of foraminotomy and intervertebral distraction on the volume of the lumbosacral intervertebral neurovascular foramen: an ex vivo study. Vet J 2020; 256: 105435
- 27 Bates D, Mächler M, Bolker B, Walker S. Fitting linear mixed-effects models using lme4. J Stat Softw 2015; 67 (01) 1-48
- 28 Konda SR, Davidovitch RI, Egol KA. Computed tomography scan to detect traumatic arthrotomies and identify periarticular wounds not requiring surgical intervention: an improvement over the saline load test. J Orthop Trauma 2013; 27 (09) 498-504
- 29 Kupchick TD, Yousif MJ, Colen AJ, Fenkell BR, Faulkner AM. Detection of traumatic elbow arthrotomies: computed tomography scan vs. saline load test. J Shoulder Elbow Surg 2020; 29 (09) 1869-1875
- 30 Konda SR, Howard D, Davidovitch RI, Egol KA. The saline load test of the knee redefined: a test to detect traumatic arthrotomies and rule out periarticular wounds not requiring surgical intervention. J Orthop Trauma 2013; 27 (09) 491-497
- 31 Vande Berg BC, Lecouvet FE, Poilvache P, Dubuc JE, Maldague B, Malghem J. Anterior cruciate ligament tears and associated meniscal lesions: assessment at dual-detector spiral CT arthrography. Radiology 2002; 223 (02) 403-409
- 32 Vande Berg BC, Lecouvet FE, Poilvache P, Maldague B, Malghem J. Spiral CT arthrography of the knee: technique and value in the assessment of internal derangement of the knee. Eur Radiol 2002; 12 (07) 1800-1810
- 33 Samii VF, Dyce J, Pozzi A. et al. Computed tomographic arthrography of the stifle for detection of cranial and caudal cruciate ligament and meniscal tears in dogs. Vet Radiol Ultrasound 2009; 50 (02) 144-150
- 34 Stopka SS, Wilson GL, Pearsall AW. Dilution effect of intra-articular injection administered after knee arthroscopy. J Surg Orthop Adv 2015; 24 (04) 209-212
- 35 Cook JL, Smith PA, Bozynski CC. et al. Multiple injections of leukoreduced platelet rich plasma reduce pain and functional impairment in a canine model of ACL and meniscal deficiency. J Orthop Res 2016; 34 (04) 607-615
- 36 Alves JC, Santos A, Jorge P. Platelet-rich plasma therapy in dogs with bilateral hip osteoarthritis. BMC Vet Res 2021; 17 (01) 207
- 37 Nguyen RT, Borg-Stein J, McInnis K. Applications of platelet-rich plasma in musculoskeletal and sports medicine: an evidence-based approach. PM R 2011; 3 (03) 226-250
- 38 Sánchez M, Anitua E, Orive G, Mujika I, Andia I. Platelet-rich therapies in the treatment of orthopaedic sport injuries. Sports Med 2009; 39 (05) 345-354
- 39 Bosch G, Moleman M, Barneveld A, van Weeren PR, van Schie HTM. The effect of platelet-rich plasma on the neovascularization of surgically created equine superficial digital flexor tendon lesions. Scand J Med Sci Sports 2011; 21 (04) 554-561
- 40 Scharpf M, Theyse LFH. Assessment of outcome of arthroscopic subtotal coronoidectomy in treating medial coronoid disease and effect of concurrent autologous conditioned plasma in dogs using force plate analysis. Vet Comp Orthop Traumatol 2024; 37 (02) 83-89
- 41 Gendler A, Keuler NS, Schaefer SL. Computed tomographic arthrography of the normal canine elbow. Vet Radiol Ultrasound 2015; 56 (02) 144-152
Address for correspondence
Publication History
Received: 17 October 2024
Accepted: 18 June 2025
Article published online:
16 July 2025
© 2025. The Author(s). This is an open access article published by Thieme under the terms of the Creative Commons Attribution License, permitting unrestricted use, distribution, and reproduction so long as the original work is properly cited. (https://creativecommons.org/licenses/by/4.0/)
Georg Thieme Verlag KG
Oswald-Hesse-Straße 50, 70469 Stuttgart, Germany
-
References
- 1 Van Ryssen B, van Bree H, Simoens P. Elbow arthroscopy in clinically normal dogs. Am J Vet Res 1993; 54 (01) 191-198
- 2 Botazzoli AF, Ferraresi F, Travetti O, Martini FM, Mortellaro CM, Di Giancamillo M. Elbow dysplasia and lesions of the medial coronoid process: correlation between tomographic and arthroscopic findings in thirty cases. Vet Res Commun 2008; 32 (Suppl. 01) S247-S249
- 3 Goldhammer MA, Smith SH, Fitzpatrick N, Clements DN. A comparison of radiographic, arthroscopic and histological measures of articular pathology in the canine elbow joint. Vet J 2010; 186 (01) 96-103
- 4 Meyer-Lindenberg A, Langhann A, Fehr M, Nolte I. Arthrotomy versus arthroscopy in the treatment of the fragmented medial coronoid process of the ulna (FCP) in 421 dogs. Vet Comp Orthop Traumatol 2003; 16 (04) 204-210
- 5 van Bree HJJ, Van Ryssen B. Diagnostic and surgical arthroscopy in osteochondrosis lesions. Vet Clin North Am Small Anim Pract 1998; 28 (01) 161-189
- 6 Gurney MA, Rysnik M, Comerford EJ, Cripps PJ, Iff I. Intra-articular morphine, bupivacaine or no treatment for postoperative analgesia following unilateral elbow joint arthroscopy. J Small Anim Pract 2012; 53 (07) 387-392
- 7 Dutton TAG, Gurney MA, Bright SR. Intra-articular mepivacaine reduces interventional analgesia requirements during arthroscopic surgery in dogs. J Small Anim Pract 2014; 55 (08) 405-408
- 8 Kim JH, Seok SH, Park TY. et al. Analgesic effect of intra-articular ropivacaine injection after arthroscopic surgery on the shoulder joint in dogs. Vet Med (Praha) 2018; 63 (11) 513-521
- 9 Sammarco JL, Conzemius MG, Perkowski SZ, Weinstein MJ, Gregor TP, Smith GK. Postoperative analgesia for stifle surgery: a comparison of intra-articular bupivacaine, morphine, or saline. Vet Surg 1996; 25 (01) 59-69
- 10 Franklin SP, Cook JL. Prospective trial of autologous conditioned plasma versus hyaluronan plus corticosteroid for elbow osteoarthritis in dogs. Can Vet J 2013; 54 (09) 881-884
- 11 Alves JC, Santos A, Jorge P, Lavrador C, Carreira LM. The intra-articular administration of triamcinolone hexacetonide in the treatment of osteoarthritis. Its effects in a naturally occurring canine osteoarthritis model. PLoS ONE. 2021; 16 (01) e0245553
- 12 Tellegen A, Beukers M, Rudnik-Jansen I. et al. Intra-articular slow-release triamcinolone acetonide from polyesteramide microspheres as a treatment for osteoarthritis. Pharmaceutics 2021; 13 (03) 372
- 13 Alves JC, Santos A, Jorge P, Lavrador C, Carreira LM. Intraarticular triamcinolone hexacetonide, stanozolol, Hylan G-F 20 and platelet concentrate in a naturally occurring canine osteoarthritis model. Sci Rep 2021; 11 (01) 3118
- 14 Kim S, Elam L, Johnson V. et al. Intra-articular injections of allogeneic mesenchymal stromal cells vs. high molecular weight hyaluronic acid in dogs with osteoarthritis: exploratory data from a double-blind, randomized, prospective clinical trial. Front Vet Sci 2022; 9: 890704
- 15 Fahie MA, Ortolano GA, Guercio V. et al. A randomized controlled trial of the efficacy of autologous platelet therapy for the treatment of osteoarthritis in dogs. J Am Vet Med Assoc 2013; 243 (09) 1291-1297
- 16 Vilar JM, Manera ME, Santana A. et al. Effect of leukocyte-reduced platelet-rich plasma on osteoarthritis caused by cranial cruciate ligament rupture: a canine gait analysis model. PLoS One 2018; 13 (03) e0194752
- 17 Kim SE, Pozzi A, Chern YJ. et al. Intra-articular umbilical cord derived mesenchymal stem cell therapy for chronic elbow osteoarthritis in dogs: double-blinded, placebo-controlled clinical trial. Front Vet Sci 2019; 6: 474
- 18 Blumhagen EM, Spector DI, Fischetti AJ. Impact of arthroscopy on post-procedure intra-articular elbow injections: a cadaveric study. Vet Surg 2024; 53 (06) 988-998
- 19 Borgeat A, Bird P, Ekatodramis G, Dumont C. Tracheal compression caused by periarticular fluid accumulation: a rare complication of shoulder surgery. J Shoulder Elbow Surg 2000; 9 (05) 443-445
- 20 Lo IKY, Burkhart SS. Immediate postoperative fluid retention and weight gain after shoulder arthroscopy. Arthroscopy 2005; 21 (05) 605-610
- 21 Capito NM, Smith MJ, Stoker AM, Werner N, Cook JL. Hyperosmolar irrigation compared with a standard solution in a canine shoulder arthroscopy model. J Shoulder Elbow Surg 2015; 24 (08) 1243-1248
- 22 Beale BS, Hulse DA, Schulz KS, Whitney WO. Chapter 1 - History of arthroscopy. In: Beale BS, Hulse DA, Schulz KS, Whitney WO. eds. Small Animal Arthroscopy. W.B. Saunders; 2003: 1-3
- 23 Beale BS, Hulse DA, Schulz KS, Whitney WO. Chapter 4 - Arthroscopically assisted surgery of the elbow joint. In: Beale BS, Hulse DA, Schulz KS, Whitney WO. eds. Small Animal Arthroscopy. W.B. Saunders; 2003: 51-79
- 24 ITK-SNAP. Accessed July 22, 2022 at: www.itksnap.org
- 25 Yushkevich PA, Piven J, Hazlett HC. et al. User-guided 3D active contour segmentation of anatomical structures: significantly improved efficiency and reliability. Neuroimage 2006; 31 (03) 1116-1128
- 26 Smolders LA, Knell SC, Park B, Pozzi A, Meij BP, Steffen F. The effects of foraminotomy and intervertebral distraction on the volume of the lumbosacral intervertebral neurovascular foramen: an ex vivo study. Vet J 2020; 256: 105435
- 27 Bates D, Mächler M, Bolker B, Walker S. Fitting linear mixed-effects models using lme4. J Stat Softw 2015; 67 (01) 1-48
- 28 Konda SR, Davidovitch RI, Egol KA. Computed tomography scan to detect traumatic arthrotomies and identify periarticular wounds not requiring surgical intervention: an improvement over the saline load test. J Orthop Trauma 2013; 27 (09) 498-504
- 29 Kupchick TD, Yousif MJ, Colen AJ, Fenkell BR, Faulkner AM. Detection of traumatic elbow arthrotomies: computed tomography scan vs. saline load test. J Shoulder Elbow Surg 2020; 29 (09) 1869-1875
- 30 Konda SR, Howard D, Davidovitch RI, Egol KA. The saline load test of the knee redefined: a test to detect traumatic arthrotomies and rule out periarticular wounds not requiring surgical intervention. J Orthop Trauma 2013; 27 (09) 491-497
- 31 Vande Berg BC, Lecouvet FE, Poilvache P, Dubuc JE, Maldague B, Malghem J. Anterior cruciate ligament tears and associated meniscal lesions: assessment at dual-detector spiral CT arthrography. Radiology 2002; 223 (02) 403-409
- 32 Vande Berg BC, Lecouvet FE, Poilvache P, Maldague B, Malghem J. Spiral CT arthrography of the knee: technique and value in the assessment of internal derangement of the knee. Eur Radiol 2002; 12 (07) 1800-1810
- 33 Samii VF, Dyce J, Pozzi A. et al. Computed tomographic arthrography of the stifle for detection of cranial and caudal cruciate ligament and meniscal tears in dogs. Vet Radiol Ultrasound 2009; 50 (02) 144-150
- 34 Stopka SS, Wilson GL, Pearsall AW. Dilution effect of intra-articular injection administered after knee arthroscopy. J Surg Orthop Adv 2015; 24 (04) 209-212
- 35 Cook JL, Smith PA, Bozynski CC. et al. Multiple injections of leukoreduced platelet rich plasma reduce pain and functional impairment in a canine model of ACL and meniscal deficiency. J Orthop Res 2016; 34 (04) 607-615
- 36 Alves JC, Santos A, Jorge P. Platelet-rich plasma therapy in dogs with bilateral hip osteoarthritis. BMC Vet Res 2021; 17 (01) 207
- 37 Nguyen RT, Borg-Stein J, McInnis K. Applications of platelet-rich plasma in musculoskeletal and sports medicine: an evidence-based approach. PM R 2011; 3 (03) 226-250
- 38 Sánchez M, Anitua E, Orive G, Mujika I, Andia I. Platelet-rich therapies in the treatment of orthopaedic sport injuries. Sports Med 2009; 39 (05) 345-354
- 39 Bosch G, Moleman M, Barneveld A, van Weeren PR, van Schie HTM. The effect of platelet-rich plasma on the neovascularization of surgically created equine superficial digital flexor tendon lesions. Scand J Med Sci Sports 2011; 21 (04) 554-561
- 40 Scharpf M, Theyse LFH. Assessment of outcome of arthroscopic subtotal coronoidectomy in treating medial coronoid disease and effect of concurrent autologous conditioned plasma in dogs using force plate analysis. Vet Comp Orthop Traumatol 2024; 37 (02) 83-89
- 41 Gendler A, Keuler NS, Schaefer SL. Computed tomographic arthrography of the normal canine elbow. Vet Radiol Ultrasound 2015; 56 (02) 144-152