

Subscribe to RSS
DOI: 10.1055/a-2650-6754
Resolution of Symptomatic Intracranial Hypertension Following Resection of Tentorial Meningioma Compressing the Dominant Transverse Sinus
Authors


Abstract
Background
Symptomatic intracranial hypertension is a rare presentation of meningiomas associated with compression and/or invasion of the dural venous sinuses. Establishing a clear link between tumor-induced venous outflow obstruction and elevated intracranial pressure is essential to determine the appropriate management strategy.
Case Description
A 59-year-old female presented with headaches, imbalance, pulsatile tinnitus, and horizontal binocular diplopia secondary to bilateral abducens nerve dysfunction in the setting of a small tentorial meningioma compressing the dominant right transverse sinus. Venous manometry demonstrated elevated sinus pressures and a large pressure gradient across the lesion. Microsurgical resection improved the caliber of the transverse sinus and normalized intracranial pressures without the need for permanent venous stent placement.
Conclusion
Tentorial meningiomas infrequently result in venous outflow obstruction and symptomatic intracranial hypertension. Thorough workup including diagnostic angiography, venous manometry, and temporary stenting can be used to confirm the diagnosis. Surgical resection with or without permanent stent placement can restore venous drainage and alleviate debilitating symptoms.
Keywords
tentorial meningioma - intracranial hypertension - venous manometry - venous outflow obstruction - elevated intracranial pressure - transverse sinusIntroduction
Symptomatic intracranial hypertension caused by compression and/or invasion of the dural venous sinuses is an uncommon presentation of intracranial meningiomas.[1] Tentorial meningiomas exerting mass effect on the transverse–sigmoid complex can result in venous outflow obstruction and elevated intracranial pressure (ICP).[2] For small tentorial meningiomas, establishing a causal link between sinus compression, elevated ICPs, and associated symptomatology is critical for rationalizing surgical intervention over surveillance. In this report, we describe the case of a 59-year-old female who presented with symptomatic intracranial hypertension secondary to extrinsic compression of the dominant transverse sinus by a small tentorial meningioma. Venous manometry revealed a large pressure gradient across the lesion, and expansion of a temporary venous stent-retriever improved sinus caliber at the site of focal stenosis. Microsurgical resection restored normal sinus pressures and resolved the patient's debilitating symptoms without the need for permanent stenting.
Case Presentation
A 59-year-old female was evaluated for progressive horizontal binocular diplopia, imbalance, occipital headaches, and pulsatile tinnitus. Diplopia was present for about 10 years and had been managed with prism glasses. Over several months prior to presentation, her diplopia rapidly worsened and she developed new progressive positional headaches exacerbated by bending over and lying flat. Neuro-ophthalmologic examination revealed incomitant esotropia that increased in right and left gazes, as well as trace abduction deficits in each eye suggestive of bilateral abducens nerve dysfunction. Fundoscopic examination showed no frank papilledema. Visual acuity, color vision, and visual field testing were normal. Additional workup included negative serum acetylcholine receptor antibody testing, normal single fiber orbicularis oculi muscle electromyography, and normal repetitive nerve stimulation studies. Intracranial hypertension symptoms did not improve after several weeks of acetazolamide therapy.
MRI of the head with and without intravenous contrast demonstrated bilateral optic nerve sheath tortuosity and dilation, unobstructed cerebrospinal fluid (CSF) pathways without ventriculomegaly, and a small tentorial meningioma (1.7 × 1.7 × 1.4 cm) compressing the dominant right transverse sinus at the proximal transverse–sigmoid junction associated with subtotal transverse sinus occlusion without clear intraluminal invasion ([Fig. 1A]–[C]).

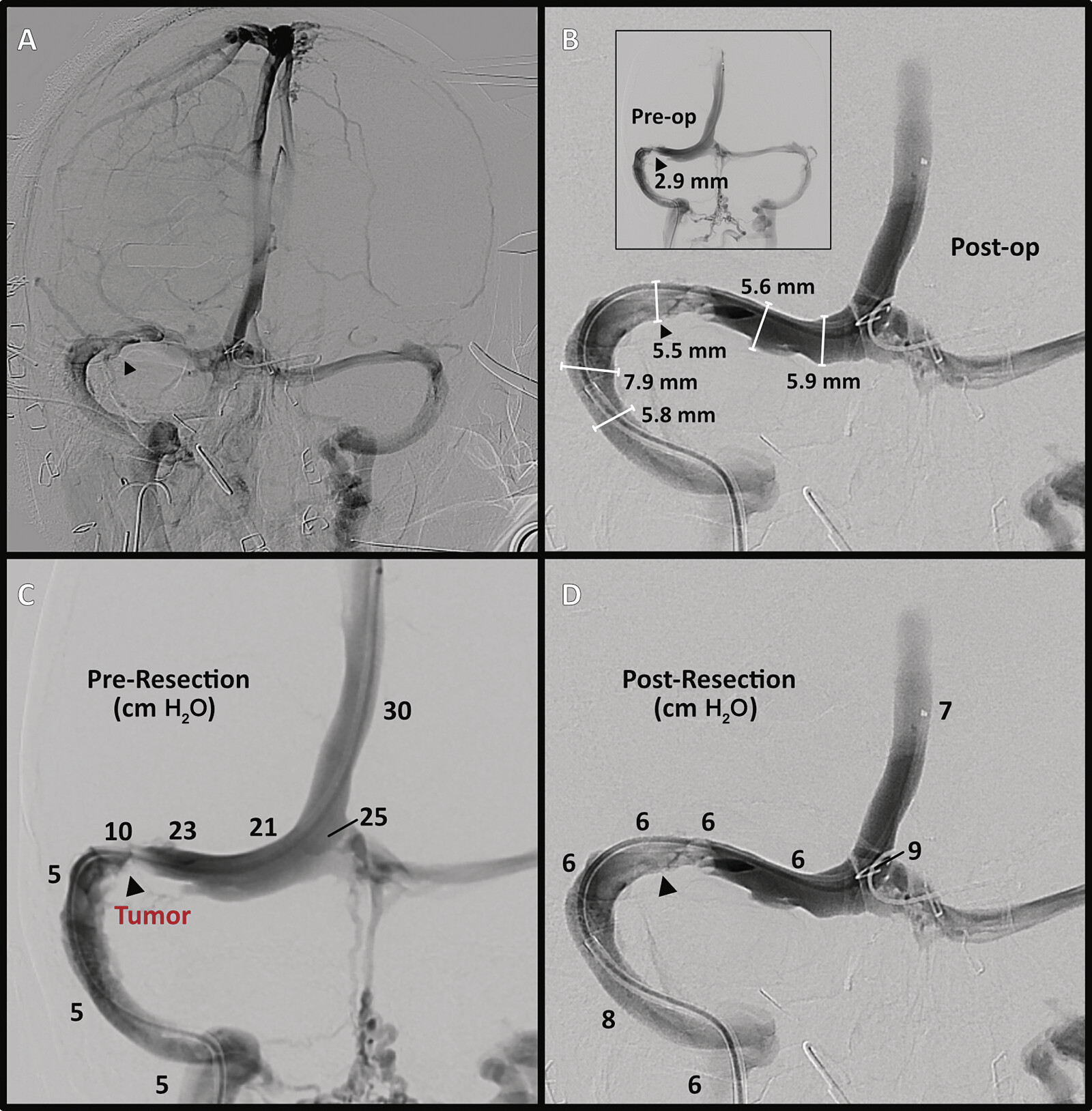
To investigate a potential link between sinus outflow obstruction and intracranial hypertension, the patient underwent lumbar puncture (LP), angiography, venous manometry, and temporary stent-retriever placement. LP opening pressure (OP) was elevated (40–45 cm H2O). Venous-phase 3D rotational angiography demonstrated a dominant right transverse sinus, focal stenosis at the site of meningioma compression, and engorgement of the cavernous sinus and occipital condylar plexus ([Fig. 1D]–[G]). Venous manometry revealed a large pressure gradient across the lesion at the proximal aspect of the transverse–sigmoid junction ([Table 1]). Expansion of a temporary stent-retriever (Tigertriever 21, Rapid Medical, Yokneam, Israel) resulted in improved vessel caliber (2.9 to 5.7 mm), with reversion to original diameter after relaxation ([Fig. 1H], [I]).
Abbreviations: IJ, internal jugular; SS, sigmoid sinus; SSS, superior sagittal sinus; TS, transverse sinus.
After thorough discussion of treatment options including ventriculoperitoneal shunting and venous sinus stenting without tumor resection, the patient consented to undergo retrosigmoid craniotomy for tumor excision followed by intraoperative angiography and repeat manometry. The procedure was performed in a hybrid operating suite equipped with biplanar fluoroscopy. A lumbar drain was placed to facilitate CSF drainage throughout the case. Arterial and venous access was obtained via the right radial artery (5-Fr sheath) and antecubital vein (6-Fr sheath), respectively. The patient was positioned laterally with the head rotated to bring the right post-auricular region to the apex of the field. An inverted U-shaped incision was planned using a combination of Medtronic StealthStation and augmented reality-based neuronavigation (Hoth Intelligence, Philadelphia, PA) ([Fig. 2]). A generous myocutaneous flap was reflected inferiorly to expose the right subocciput. A retrosigmoid craniotomy was fashioned to unroof the transverse–sigmoid junction. The C-shaped dural leaflet was flapped superiorly toward the transverse sinus.

Under the operating microscope ([Supplementary Video 1]), the tentorial meningioma was identified and carefully dissected from the surrounding cerebellum. The tumor was internally debulked and de-vascularized at its base with care to preserve the patency of the transverse sinus. A small focus of possible microscopic tumor infiltration into the sinus was explored, but ultimately, entry into the sinus was deemed unnecessary. Intraoperative venous angiography after tumor resection demonstrated sinus patency, improved venous drainage, and restoration of normal sinus diameter ([Fig. 3A], [B]). Manometry revealed normalization of venous sinus pressures ([Table 1]; [Fig. 3C], [D]), obviating the need for permanent stenting. After watertight dural closure, the bone flap was replaced, the incision was closed, and the lumbar drain was removed.
Postoperative recovery was uneventful. MRI of the head with and without contrast (postoperative day 1; POD1) demonstrated complete resection of enhancing tumor and preserved sinus patency ([Fig. 4]). She was discharged home on POD2. She experienced gradual resolution of her debilitating headaches, balance issues, and pulsatile tinnitus. Acetazolamide was successfully weaned off. By 3-month follow-up her binocular diplopia significantly improved, esotropia improved, and ocular motility was normal bilaterally, all suggesting improved abducens nerve function. Repeat MRI at 3 months revealed continued sinus patency and no evidence of tumor recurrence. Pathology was consistent with WHO grade I meningioma.

The participants and any identifiable individuals consented to publication of his/her image. The patient consented to publication of his/her image. Institutional review was not required for this case presentation as per institutional policy.
Discussion
Although meningiomas frequently associate with the dural venous sinuses, their indolent growth typically permits the gradual maturation of venous collaterals that compensate for obstructed or even occluded sinuses. Previous reports of tumor-induced venous outflow obstruction resulting in symptomatic intracranial hypertension are rare.[1] [3] [4] [5] [6] [7] [8] [9] [10] This case illustrates diagnostic and technical nuances involved in managing this unusual presentation. First, convincing evidence favoring the uncommon diagnosis of tumor-induced venous hypertension over more common entities (e.g., idiopathic intracranial hypertension, migraine, etc.) should be pursued. Cheyuo et al[6] were the first to use venous manometry to demonstrate a pressure gradient across a segment of the sigmoid sinus compressed externally by a meningioma. This adjunct proved essential in our case given the small size of the meningioma and the partial sinus patency demonstrated on preoperative imaging. Second, selection of the optimal treatment strategy must consider factors such as venous drainage pattern and degree of sinus invasion. Most patients exhibit asymmetric flow through the transverse–sigmoid system, and surgical manipulation of the dominant side is typically avoided, especially when the sinus is partially patent.[11] Recently, dural sinus stenting has been used to restore venous drainage in patients with tumor-induced outflow obstruction,[12] [13] although studies with long-term follow-up demonstrate that patients often require repeat intervention to maintain stent patency.[14] In our case, a temporary stent-retriever was used to confirm that normal sinus caliber could be restored with stenting, but we ultimately opted for upfront surgical resection given the accessibility of the tumor, the extrinsic source of compression without clear intraluminal extension, and the patient's preference for resection. Finally, our case illustrates the utility of the hybrid operating suite, which would have facilitated permanent stenting had post-resection angiography revealed persistent obstruction and elevated pressures.
Conclusion
Symptomatic intracranial hypertension is a rare presentation of meningiomas associated with compression and/or invasion of the dural venous sinuses. Adjudicating between definitive resection and less-invasive alternatives requires assessment of the severity of the venous outflow obstruction, its potential reversibility, and the anticipated risks of sinus injury from surgical manipulation. In well-selected patients, tumor resection to relieve sinus obstruction can normalize ICPs and resolve associated symptoms.
Conflict of Interest
The authors declare that they have no conflict of interest.
Contributors' Statement
S.B.T., D.Y., and V.M.S. contributed to the conception of the study. S.B.T., R.R., R.J., and V.M.S. were involved in the literature review and drafting of the manuscript. All authors participated in the interpretation of data and reviewed and approved the final version of the manuscript.
-
References
- 1 Hartmann AJPW, Latting MW, Lee MS. et al. Papilloedema from dural venous sinus compression by meningiomas. Neuroophthalmology 2018; 43 (03) 171-179
- 2 Maiuri F, Di Martino G, Vergara P, Mariniello G. Meningiomas of the transverse—sigmoid sinus junction area. Br J Neurosurg 2011; 25 (04) 492-496
- 3 Healy A, Singh U, Bhatia SS, Lai N, Lui F. Increased intracranial pressure due to transverse sinus compression by a meningioma en plaque. Cureus 2023; 15 (01) e33487
- 4 Amuluru K, Al-Mufti F, Shah M, Prestigiacomo CJ, Liu JK, Gandhi CD. Acquired sinus pericranii due to parasagittal meningiomatous invasion of the superior sagittal sinus and bilateral transverse sinuses. World Neurosurg 2017; 98: 872.e5-872.e9
- 5 Chausson N, Bocquet J, Aveillan M. et al. Intracranial hypertension caused by a meningioma compressing the transverse sinus. J Clin Neurosci 2010; 17 (12) 1589-1592
- 6 Cheyuo C, Rosen CL, Rai A, Cifarelli CP, Qaiser R. Venous manometry as an adjunct for diagnosis and multimodal management of intracranial hypertension due to meningioma compressing sigmoid sinus. Cureus 2019; 11 (06) e4953
- 7 Mariniello G, Giamundo A, Donzelli R. et al. Intracranial hypertension due to meningioma of the unique transverse sinus. Neuroradiol J 2013; 26 (02) 209-212
- 8 Sumi K, Otani N, Mori F, Yamamuro S, Oshima H, Yoshino A. Venous hypertension caused by a meningioma involving the sigmoid sinus: case report. BMC Neurol 2021; 21 (01) 119
- 9 Kim AW, Trobe JD. Syndrome simulating pseudotumor cerebri caused by partial transverse venous sinus obstruction in metastatic prostate cancer. Am J Ophthalmol 2000; 129 (02) 254-256
- 10 Sharma N, Hitti FL, Liu G, Grady MS. Pseudotumor cerebri comorbid with meningioma: a review and case series. Surg Neurol Int 2018; 9: 130
- 11 Maiuri F, Donzelli R, Pagano S, Mariniello G. The management of the venous sinuses during surgery for posterior fossa meningiomas. World Neurosurg 2019; 125: 357-363
- 12 White TG, Chen A, Dalal S. et al. Treatment of tumor-induced cerebral venous sinus stenosis: technical note and review of the literature. Interv Neuroradiol 2024; 15910199241267341. Epub ahead of print
- 13 Ahmed G, Abou-Foul M, Sage W, McConachie N. Endovascular stenting for cerebral venous sinus stenosis secondary to meningioma invasion. Neuroradiology 2024; 66 (05) 817-824
- 14 Higgins JNP, Kirollos SRW, Helmy A. et al. Technical considerations and long-term results of endovascular venous stenting to control venous hypertension from meningiomas invading intracranial venous sinuses. J Neurosurg 2023; 140 (03) 826-838
Address for correspondence
Publication History
Received: 16 May 2025
Accepted: 22 June 2025
Article published online:
22 July 2025
© 2025. The Author(s). This is an open access article published by Thieme under the terms of the Creative Commons Attribution License, permitting unrestricted use, distribution, and reproduction so long as the original work is properly cited. (https://creativecommons.org/licenses/by/4.0/)
Georg Thieme Verlag KG
Oswald-Hesse-Straße 50, 70469 Stuttgart, Germany
-
References
- 1 Hartmann AJPW, Latting MW, Lee MS. et al. Papilloedema from dural venous sinus compression by meningiomas. Neuroophthalmology 2018; 43 (03) 171-179
- 2 Maiuri F, Di Martino G, Vergara P, Mariniello G. Meningiomas of the transverse—sigmoid sinus junction area. Br J Neurosurg 2011; 25 (04) 492-496
- 3 Healy A, Singh U, Bhatia SS, Lai N, Lui F. Increased intracranial pressure due to transverse sinus compression by a meningioma en plaque. Cureus 2023; 15 (01) e33487
- 4 Amuluru K, Al-Mufti F, Shah M, Prestigiacomo CJ, Liu JK, Gandhi CD. Acquired sinus pericranii due to parasagittal meningiomatous invasion of the superior sagittal sinus and bilateral transverse sinuses. World Neurosurg 2017; 98: 872.e5-872.e9
- 5 Chausson N, Bocquet J, Aveillan M. et al. Intracranial hypertension caused by a meningioma compressing the transverse sinus. J Clin Neurosci 2010; 17 (12) 1589-1592
- 6 Cheyuo C, Rosen CL, Rai A, Cifarelli CP, Qaiser R. Venous manometry as an adjunct for diagnosis and multimodal management of intracranial hypertension due to meningioma compressing sigmoid sinus. Cureus 2019; 11 (06) e4953
- 7 Mariniello G, Giamundo A, Donzelli R. et al. Intracranial hypertension due to meningioma of the unique transverse sinus. Neuroradiol J 2013; 26 (02) 209-212
- 8 Sumi K, Otani N, Mori F, Yamamuro S, Oshima H, Yoshino A. Venous hypertension caused by a meningioma involving the sigmoid sinus: case report. BMC Neurol 2021; 21 (01) 119
- 9 Kim AW, Trobe JD. Syndrome simulating pseudotumor cerebri caused by partial transverse venous sinus obstruction in metastatic prostate cancer. Am J Ophthalmol 2000; 129 (02) 254-256
- 10 Sharma N, Hitti FL, Liu G, Grady MS. Pseudotumor cerebri comorbid with meningioma: a review and case series. Surg Neurol Int 2018; 9: 130
- 11 Maiuri F, Donzelli R, Pagano S, Mariniello G. The management of the venous sinuses during surgery for posterior fossa meningiomas. World Neurosurg 2019; 125: 357-363
- 12 White TG, Chen A, Dalal S. et al. Treatment of tumor-induced cerebral venous sinus stenosis: technical note and review of the literature. Interv Neuroradiol 2024; 15910199241267341. Epub ahead of print
- 13 Ahmed G, Abou-Foul M, Sage W, McConachie N. Endovascular stenting for cerebral venous sinus stenosis secondary to meningioma invasion. Neuroradiology 2024; 66 (05) 817-824
- 14 Higgins JNP, Kirollos SRW, Helmy A. et al. Technical considerations and long-term results of endovascular venous stenting to control venous hypertension from meningiomas invading intracranial venous sinuses. J Neurosurg 2023; 140 (03) 826-838