

RSS-Feed abonnieren
DOI: 10.1055/a-2651-4971
Interpregnancy Interval as a Determinant of Outcome in Women with Prophylactic Cerclage Following Preterm Birth or Late Miscarriage
Artikel in mehreren Sprachen: English | deutschAutor*innen

Abstract
Background
Patients with a history of late miscarriage or preterm birth in a previous pregnancy may have a cerclage with total cervical closure (TCC) in a subsequent pregnancy to increase the likelihood of term delivery. This analysis investigates whether the interpregnancy interval influences the outcome of the subsequent pregnancy.
Methods
In a retrospective cohort of 131 women who received a prophylactic cerclage with TCC following late miscarriage or preterm birth, the impact of the interpregnancy interval on pregnancy outcome was evaluated. Women were divided into three interpregnancy interval groups (0–6, 6–12, and > 12 months). Outcomes assessed included late miscarriage, preterm birth (stratified by gestational age), term birth (≥ 37+0 weeks of gestation), and neonatal parameters (Apgar scores, umbilical cord pH, birth weight, and admission to the neonatal intensive care unit [NICU]).
Results
An interpregnancy interval of more than 12 months was associated with the highest rate of term deliveries (85.4%) and the best neonatal outcomes overall. This group had the lowest NICU admission rates, the highest birth weights, and the best Apgar scores. Very early preterm births (< 28+0 weeks) were observed more frequently in the shorter interval groups. Umbilical artery pH showed no correlation with the interpregnancy interval.
Conclusion
A longer interpregnancy interval of more than 12 months was associated with a higher rate of deliveries ≥ 37+0 weeks and improved fetal outcomes in women with prophylactic cerclage and TCC after prior preterm birth or late miscarriage. In contrast, very early preterm births (< 28+0 weeks) occurred more often with shorter intervals.
Keywords
cerclage - interpregnancy interval - premature birth - cervical insufficiency - late miscarriageIntroduction
Late miscarriage or preterm birth is a significant emotional and physical burden for affected women [1] [2].
The wish to have another pregnancy, especially after suffering the loss of a child, is often very strong. For many women, the previous pregnancy shows them just how strong their wish is to have a child [3].
Counseling patients after late miscarriage or preterm birth is important but often challenging, as the wish to quickly start a subsequent pregnancy can be very strong. Recommendations on the optimal interval until starting a subsequent pregnancy are inconsistent and depend on the treating physician or the patient’s individual situation.
After a live birth, the WHO recommends leaving an interval of at least 24 months before the next conception to reduce the risk of maternal and neonatal complications. In contrast, the American College of Obstetricians and Gynecologists (ACOG) considers an interval of at least six months to be sufficient but advises against an interpregnancy interval of less than six months. The ACOG also emphasizes the importance of individual counseling about the risk of having another pregnancy before 18 months have expired since the last pregnancy. Several studies and meta-analyses have reported a correlation between a short interpregnancy interval of less than 6 months and a higher risk of low birth weight, preterm birth and intrauterine or neonatal death [4] [5] [6].
When treating high-risk pregnant women with a medical history of preterm birth, the main aim is to increase the probability of a birth at term. Prophylactic (primary) cerclage with or without additional TCC may be considered for patients with a prior history of late miscarriage or preterm birth. If the cervical length late in the first trimester or early in the second trimester of pregnancy is unremarkable, a surgical procedure can be carried out to mechanically stabilize the cervix. This is an effective established approach. Several studies and meta-analyses have shown that cerclage can significantly reduce the risk of repeat late miscarriage or preterm birth [7] [8].
The most common surgical cerclage techniques are McDonald cerclage and Shirodkar cerclage. It is not clear which of these surgical techniques is more effective [9] [10] [11].
A secondary cerclage may be considered in addition to primary cerclage in high-risk patients if the cervix decreases to less than 25 mm.
According to the S2k-guideline “Prevention and Therapy of Preterm Birth” issued by the DGGG (2022), vaginal microbiological diagnostic tests are recommended for pregnant women with a relevant medical history to identify asymptomatic bacterial or mycotic infections at an early stage and prevent ascending infection as a potential cause of preterm birth [12]. Such infections are considered potential contributors to late miscarriage and preterm birth. If the test findings are pathological, targeted antibiotic or antimycotic therapy must be administered prior to carrying out the cerclage. A vaginal microbiome dominated by Lactobacillus species is considered protective, while bacterial dysbiosis, especially bacterial vaginosis, is associated with a higher risk of spontaneous preterm birth [13].
Patients and Methods
Study design and population
A retrospective analysis of patient data from the Gynecology Department of the University Hospital Freiburg was carried out. Women with an adverse obstetric medical history, defined as late miscarriage or preterm birth who underwent prophylactic cerclage with TCC late in the first trimester or early in the second trimester of pregnancy were included in the study.
Diagnosis and preoperative preparation
Prior to placement of the cerclage, a microbiological vaginal swab was taken from all patients. If the findings were unsuspicious, the surgical procedure was performed shortly thereafter. If pathological microorganisms were identified, targeted antibiotic therapy was initiated based on the antibiogram. Cerclage and TCC were carried out after the conclusion of antibiotic treatment irrespective of whether microbiological eradication was confirmed or not.
Surgical technique
Surgical cerclage was carried out using the McDonald technique as it is the preferred procedure used in the investigating hospital because the department has many years of experience with this technique. Non-absorbable polyfilament suture material was used for mechanical stabilization of the cervix. TCC was additionally carried out using absorbable sutures.
Assignment into groups based on the interpregnancy interval
Patients were divided into three groups based on the interval between the previous and the subsequent (current) pregnancy:
-
Group 1: interpregnancy interval of 0 to 6 months
-
Group 2: interpregnancy interval of 6 to 12 months
-
Group 3: interpregnancy interval of > 12 months
Primary endpoint: time of delivery
Primary endpoint was the time of delivery divided into:
-
Term birth: from 37+0 GW
-
Preterm birth: between 23+5 and 37+0 GW, subdivided further into:
-
23+5 to 28+0 GW
-
28+1 to 32+0 GW
-
32+1 to 37+0 GW
-
-
Late miscarriage: prior to 23+5 GW
Secondary endpoints: neonatal outcome
Secondary endpoints for fetal outcome included:
-
birth weight
-
Apgar score at 1, 5 and 10 minutes
-
umbilical cord pH
-
admission to the NICU
This retrospective data analysis is a non-interventional study. The Ethics Committee of Albert Ludwig University Freiburg approved the study (vote no. 24-1552-S1-retro).
Statistical analysis
Fisher’s exact test for r×c contingency tables was used for the statistical analysis of correlations between interpregnancy interval and pregnancy outcome as it provides robust results even for small samples [14].
Shapiro-Wilk test was used to evaluate infant parameters (birth weight, Apgar scores, umbilical cord pH) for normal distribution [15]. Non-parametric tests for birth weight and Apgar scores were done as these parameters were not normally distributed.
-
Comparison of groups: Kruskal-Wallis test [16].
-
Correlations: Spearman’s rank correlation
-
Umbilical cord pH was evaluated using one-way analysis of variance (ANOVA).
A significance level of α = 0.05 was set for all statistical tests.
Results
The analysis initially included 138 patients. Seven patients had to be excluded because of missing data, meaning that the final evaluation included a total of 131 patients.
The distribution of interpregnancy intervals was as follows:
-
10 patients had an interval of 0–6 months,
-
25 patients had an interval of 6–12 months,
-
96 patients had an interval of > 12 months.
Patient demographic data
There were only slight differences between the three groups with regard to age and medical history. Patients with an interval of more than 12 months tended to have a higher number of gravidities (median 3.5) and more late miscarriages and preterm births. The mean age in all groups was 32 years ([Table 1]).
Primary endpoint: time of delivery in the three groups
Preterm births depend on the interpregnancy interval and gestational age
A total of 131 patients who had prophylactic cerclage and TCC after previous late miscarriage or preterm birth were divided into three groups, based on the interpregnancy interval since the previous pregnancy: Group 1 (0–6 months, n = 10), Group 2 (6–12 months, n = 25) and Group 3 (> 12 months, n = 96) ([Fig. 1]).

Time of delivery and distribution of preterm births
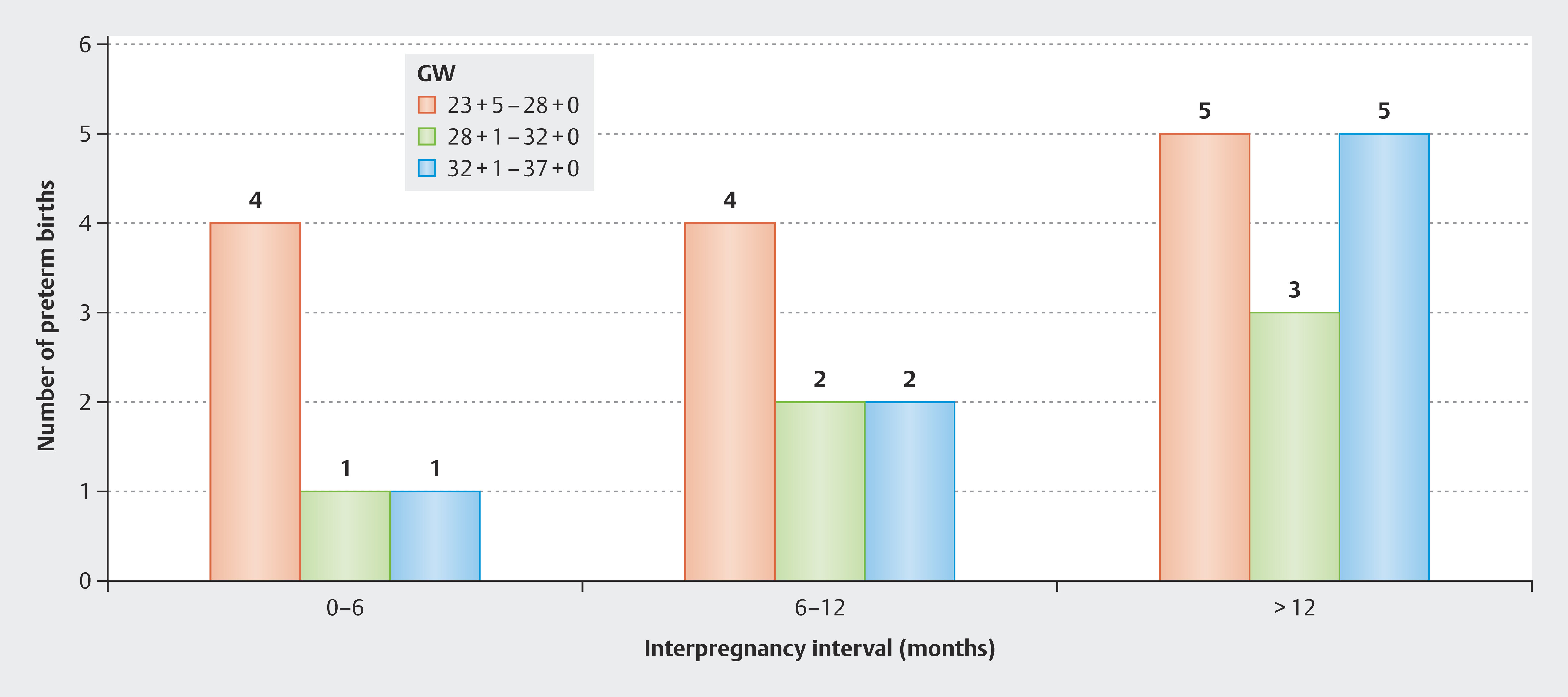
A late miscarriage was recorded for 10% (1/10) of women in Group 1; 60% (6/10) had a preterm birth, four of which were extremely preterm births (< 28+0 GW), one was a severe (28+1–32+0 GW) and was a moderate/late preterm birth (32+1–36+6 GW). 30% (3/10) of women achieved a term birth ≥ 37+0 GW.
In Group 2, 4% (1/25) of women had a late miscarriage, 32% (8/25) had a preterm birth (four < 28+0 GW, two between 28+1 and 32+0 GW, two between 32+1 and 36+6 GW). 64% (16/25) had a term birth.
The late miscarriage rate in Group 3 was 1% (1/96) and the preterm birth rate was 13.5% (13/96). The distribution of preterm births was five < 28+0 GW, three between 28+1 and 32+0 GW and five between 32+1 and 36+6 GW. The term birth rate was 85.4% (82/96) ([Fig. 2]).
Correlation between interpregnancy interval and pregnancy outcome
The frequency of late miscarriages, preterm births and term births varied significantly, depending on the interpregnancy interval (p < 0.001; Fisher’s exact test). A longer interval was associated with a significantly lower preterm birth rate and a higher rate of term births.
Secondary endpoints: neonatal parameters depending on the interpregnancy interval
The analysis of neonatal parameters showed differences between groups with different interpregnancy intervals.
Apgar scores differed significantly depending on the interpregnancy interval. The group with an interval of 0–6 months showed the greatest variability between scores and had the lowest Apgar scores, especially Apgar scores at one minute (p = 0.02). Apgar scores of the group with an interval of 6–12 months were more stable and median scores at 5 and 10 minutes were higher (p = 0.03 and p = 0.04, respectively). The highest and most stable Apgar scores were observed in the group with an interpregnancy interval of more than 12 months, with little variation and almost constantly high values at all time points (p < 0.01).
Birth weight varied significantly depending on the interpregnancy interval. The neonates with the lowest birth weights were in the group with an interpregnancy interval of 0–6 months, with a wide range of birth weights including several birth weights under 2500 g (p = 0.01). The birth weights in the group with an interval of 6–12 months were higher and the variability was lower (p = 0.02). The highest birth weights were observed in the group with an interval of more than 12 months, with most birth weights closely grouped around the median and only a few infants with a birth weight < 2500 g (p < 0.01).
There were no significant differences in umbilical cord pH values between groups, which indicates that umbilical cord pH was not affected by the interpregnancy interval.
The longer the interpregnancy interval between the previous and the subsequent pregnancy, the fewer neonates required admission to the NICU. In the group with an interval of 0–6 months, 44.4% (4/9) of neonates were admitted to the NICU; in the group with an interval of 6–12 months 33.3% (8/24) required admission, and in the group with an interval of more than 12 months 10.6% (10/94) of neonates were transferred to the NICU. Only live births are included in these figures; late miscarriages were not included. No information about admission to the NICU was available for one of the patients in group 3 (interval > 12 months) ([Fig. 3]).

Discussion
For patients who have had a late miscarriage or preterm birth, the overriding aim in a subsequent pregnancy is to maximize the probability of a term birth. Early structured interpregnancy counseling is essential.
Patients should be informed that a short interval between a previous pregnancy and the next pregnancy is associated with a higher risk of adverse pregnancy outcomes and neonatal complications [17] [18].
Cerclage placement is a key element in the preventive care of women with a high risk of late miscarriage or preterm birth. Depending on the individual risk constellation, cerclage may be carried out as a primary or secondary procedure, with or without additional TCC. Cerclage is used as a mechanical means of stabilizing the cervix and is an established procedure to treat cervical insufficiency or a sonographically shortened cervix.
TCC was additionally carried out to prevent ascending infection as infection is a relevant pathomechanism for spontaneous late miscarriage and preterm birth. The original TCC procedure was first described by Szendi in the 1960s and was developed further by Erich Saling. The concept consists of complete closure of the cervical canal to avoid bacterial colonization of intrauterine structures [19] [20] [21]. Up to now, the potential benefit of TCC has been described primarily in retrospective case series. In a prospective study of births after a combination of McDonald cerclage and TCC, Zayyan et al. reported a term birth rate of 92% in a group of patients with recurrent pregnancy loss in the second trimester [22]. Braun and Klockenbusch discussed the benefit of TCC in the context of a multistage prevention concept, especially combined with cerclage and pessaries, although their assessment was primarily based on clinical experience and has not yet been confirmed in prospective randomized studies [23].
In our patient cohort, all patients with a medical history of late miscarriage or preterm birth underwent cerclage with TCC. The decision for this combined procedure was based on the risk profiles of the individual patients and the infection-related hypothesis that additional mechanical closure could effectively prevent ascending infection. As there was no comparison group without TCC, our data does not permit reliable statements to be made about the effectiveness of TCC in isolation.
International recommendations, including those of the WHO, advise women to have an interpregnancy interval of at least six months after a miscarriage. No specific recommendations have been issued for pregnancies which ended in preterm birth. The WHO recommends an interval of at least 24 months after any live birth before the next conception. However, the AWMF S2k-guideline on the prevention of preterm birth (2022) advocates an 18-month interval between two pregnancies.
Our data show that an interval of more than 12 months after late miscarriage or preterm birth is associated with a significantly higher rate of term births and better neonatal outcomes. The highest rate of births ≥ 37+0 GW (85.4%) was recorded in the group with an interpregnancy interval of > 12 months. The neonates in this group had higher birth weights, better Apgar scores and the lowest rate of admissions to the NICU compared to the other groups. These findings are in accordance with existing recommendations which view longer interpregnancy intervals as protective. Good neonatal outcomes showed a clear association with being born at term.
Our analysis clearly showed that the length of the interpregnancy interval affects the gestational age of preterm births. In the group with the shortest interpregnancy interval (0–6 months), two thirds of preterm births occurred at a very early gestational age (< 28+0 GW). Preterm births increasingly shifted to the later weeks of gestation in the groups with longer interpregnancy intervals. This finding is clinically important as extremely preterm births are associated with significantly higher neonatal morbidity and mortality rates.
The close correlation between gestational age and neonatal outcome is well documented. The earlier the birth, the higher the risk of low birth weight, poor Apgar scores and the need for intensive medical care. It appears that the interpregnancy interval is a significant, modifiable risk factor. Women with a medical history of cervical insufficiency and previous preterm birth could benefit from receiving targeted information on planning the interval between pregnancies as this could lead to better outcomes.
Our findings are supported by recent meta-analyses. A network meta-analysis by Wen et al. (2025) identified an interval of between 24 and 29 months as particularly protective against preterm birth [24]. A systematic dose-response meta-analysis by Ni et al. (2023) showed that both very short (< 6 months) and very long intervals (≥ 60 months) were associated with an increased risk of preterm birth, low birth weight, and stillbirth [25].
In accordance with the recommendations of the current S2k-guideline, a microbiological smear was taken from all patients prior to cerclage placement for the early identification of potentially pathogenic bacteria. If the results of the smear were pathological, targeted antibiotic therapy based on the antibiogram was administered prior to the surgical procedure. The aim of this preintervention diagnosis was to minimize the risk of ascending infection and thereby prevent complications such as preterm birth or late miscarriage.
A significant limitation of our analysis was that in the majority of patients, the previous pregnancy (miscarriage or preterm birth) occurred outside our institution. Most of the women were referred to us for counseling and cerclage placement by external hospitals. In many cases, we therefore did not have reliable information about the precise cause of the previous pregnancy loss, for example, whether it was caused by infection, premature rupture of membranes or silent cervical dilation. But this information would have been essential to be able to better estimate the individual risk of preterm birth and initiate more targeted preventive measures.
An imbalance in the composition of the vaginal microbiome with reduced dominance of Lactobacillus is known to be a relevant risk factor for spontaneous preterm birth. A network meta-analysis identified Lactobacillus crispatus as a protective marker, while a dysbiotic microbiome profile significantly increased the risk of preterm birth [26]. It has not yet been conclusively determined whether a short interpregnancy interval directly results in the development of microbial dysbiosis or whether dysbiosis is the result of incomplete postpartum regeneration of the vaginal microbiome.
Recent studies have shown, however, that microbial changes such as bacterial vaginosis can persist postpartum over a period of several weeks to months, and this appears to be especially clinically relevant for short interpregnancy intervals [27] [28]. A longer interval between pregnancies might therefore not just promote uterine recovery but could also contribute to restabilizing the vaginal microbiome. This could reduce the risk of ascending infection, last miscarriage, and preterm birth. These associations emphasize the importance of carrying out microbiological tests and providing high-risk patients with individual counseling on optimal interpregnancy intervals.
Conclusion
The analysis shows that an interpregnancy interval of > 12 months after late miscarriage or preterm birth in patients who had cerclage and TCC increases the probability of a term birth. As neonatal outcomes are significantly affected by gestational age at delivery, an interpregnancy interval of > 12 months was found to be associated with higher birth weights, better Apgar scores, and lower admission rates to the NICU.
These results underscore the importance of leaving longer intervals between pregnancies. The recommendation to have an interpregnancy interval of > 12 months is an important part of individual counseling provided to patients with an adverse obstetric history.
Conflict of Interest
The authors declare that they have no conflict of interest.
-
References/Literatur
- 1 Bouras G, Dannheim I, Horsch A. Preterm birth and maternal psychological health. J Health Psychol 2015; 20: 1388-1396
- 2 Lothrop H. Gute Hoffnung, jähes Ende: Fehlgeburt, Totgeburt und Verluste in der frühen Lebenszeit. Begleitung und neue Hoffnung für Eltern. Vollständig überarbeitete Neuausgabe. München: Kösel-Verlag; 2016
- 3 Fernández-Basanta S, Dahl-Cortizo C, Coronado C. et al. Pregnancy after perinatal loss: A meta-ethnography from a women’s perspective. Midwifery 2023; 124: 103762
- 4 World Health Organization. Report of a WHO technical consultation on birth spacing: Geneva, Switzerland, 13–15 June 2005. Geneva: World Health Organization; 2006. Zugriff am 22. August 2025 unter: https://www.who.int/publications/i/item/924159484X
- 5 American College of Obstetricians and Gynecologists, Society for Maternal-Fetal Medicine. Obstetric Care Consensus No. 8: Interpregnancy Care. Obstet Gynecol 2019; 133: e51-e72
- 6 Wang Y, Zeng C, Chen Y. et al. Short interpregnancy interval can lead to adverse pregnancy outcomes: A meta-analysis. Front Med (Lausanne) 2022; 9: 922053
- 7 Chan S, Dong X. Effectiveness of Prophylactic Transvaginal Cervical Cerclage in Improving Clinical Outcomes among Pregnant Women with Cervical Insufficiency: Meta-Analysis. Open J Intern Med 2024; 14: 228-246
- 8 Giouleka S, Boureka E, Tsakiridis I. et al. Cervical Cerclage: A comprehensive Review of Major Guideline. Obstet Gynecol Surv 2023; 78: 544-553
- 9 Issah A, Diacci R, Williams KP. et al. McDonald versus Shirodkar cerclage technique in women requiring a prophylactic cerclage: a systematic review and meta-analysis protocol. Syst Rev 2021; 10: 130
- 10 McDonald IA. Suture of the cervix for inevitable miscarriage. J Obstet Gynaecol Br Emp 1957; 64: 346-350
- 11 Shirodkar VN. A new method of operative treatment for habitual abortion in the second trimester of pregnancy. Antiseptic 1955; 52: 299
- 12 Berger R, Abele H, Bahlmann F. et al. Prevention and Therapy of Preterm Birth. Guideline of the DGGG, OEGGG and SGGG (S2k-Level, AWMF Registry Number 015/025, September 2022) – Part 1. Geburtshilfe Frauenheilkd 2023; 83: 547-568
- 13 Kindinger LM, MacIntyre DA, Lee YS. et al. Relationship between vaginal microbial dysbiosis, inflammation, and pregnancy outcomes in cervical cerclage. Sci Transl Med 2016; 8: 350ra102
- 14 Mehta CR, Patel NR. A network algorithm for performing Fisher’s exact test in r×c contingency tables. J Am Stat Assoc 1983; 78: 427-434
- 15 Shapiro SS, Wilk MB. An analysis of variance test for normality (complete samples). Biometrika 1965; 52: 591-611
- 16 Kruskal WH, Wallis WA. Use of ranks in one-criterion variance analysis. J Am Stat Assoc 1952; 47: 583-621
- 17 Conde-Agudelo A, Rosas-Bermúdez A, Kafury-Goeta AC. Birth spacing and risk of adverse perinatal outcomes: a meta-analysis. JAMA 2006; 295: 1809-1813
- 18 Tanigawa K, Ikehara S, Cui M. et al. Association Between Interpregnancy Interval and Risk of Preterm Birth and Its Modification by Folate Intake: The Japan Environment and Children's Study. J Epidemiol 2023; 33: 113-119
- 19 Saling E. Der frühe totale Muttermundverschluss zur Vermeidung habitueller Aborte und Frühgeburten. Z Geburtsh Perinat 1981; 185: 259-261
- 20 Saling E, Schumacher E. Der operative Totale Muttermund-Verschluss (TMV). Z Geburtshilfe Neonatol 1996; 200: 82-87
- 21 Szendi B. Vollständiges Zusammennähen des äußeren Muttermundes auf blutigem Wege zur Verhinderung von fortgeschrittenem Abortus und Frühgeburten. Zentralbl Gynakol 1961; 83: 1083-1087
- 22 Zayyan M, Suhyb SR, Laurel NO. The Use of Total Cervical Occlusion along with McDonald Cerclage in Patients with Recurrent Miscarriage or Preterm Deliveries. Oman Med J 2012; 27: 63-65
- 23 Braun J, Klockenbusch W. Nutzen von Pessar, Cerclage und Muttermundverschluss für das Überleben von Frühgeborenen. Geburtshilfe Frauenheilkd 2016; 76: 942-945
- 24 Wen X, Liang W, Zhai J. et al. The association between interpregnancy intervals and preterm birth: a systematic review and meta-analysis. BMC Pregnancy Childbirth 2025; 25: 226
- 25 Ni W, Gao X, Su X. et al. Birth spacing and risk of adverse pregnancy and birth outcomes: A systematic review and dose-response meta-analysis. Acta Obstet Gynecol Scand 2023; 102: 1618-1633
- 26 Gudnadottir U, Debelius J, Du J. et al. The vaginal microbiome and the risk of preterm birth: a systematic review and network meta-analysis. Sci Rep 2022; 12: 7926
- 27 Odogwu NM. Role of short interpregnancy interval, birth mode, birth practices, and the post-partum vaginal microbiome in preterm birth. Front Reprod Health 2023; 4: 1082199
- 28 Costello EK, DiGiulio DB, Robaczewska A. et al. Abrupt perturbation and delayed recovery of the vaginal ecosystem following childbirth. Nat Commun 2023; 14: 4141
Correspondence
Publikationsverlauf
Eingereicht: 02. Mai 2025
Angenommen nach Revision: 07. Juli 2025
Artikel online veröffentlicht:
29. August 2025
© 2025. The Author(s). This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial-License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/).
Georg Thieme Verlag KG
Oswald-Hesse-Straße 50, 70469 Stuttgart, Germany
-
References/Literatur
- 1 Bouras G, Dannheim I, Horsch A. Preterm birth and maternal psychological health. J Health Psychol 2015; 20: 1388-1396
- 2 Lothrop H. Gute Hoffnung, jähes Ende: Fehlgeburt, Totgeburt und Verluste in der frühen Lebenszeit. Begleitung und neue Hoffnung für Eltern. Vollständig überarbeitete Neuausgabe. München: Kösel-Verlag; 2016
- 3 Fernández-Basanta S, Dahl-Cortizo C, Coronado C. et al. Pregnancy after perinatal loss: A meta-ethnography from a women’s perspective. Midwifery 2023; 124: 103762
- 4 World Health Organization. Report of a WHO technical consultation on birth spacing: Geneva, Switzerland, 13–15 June 2005. Geneva: World Health Organization; 2006. Zugriff am 22. August 2025 unter: https://www.who.int/publications/i/item/924159484X
- 5 American College of Obstetricians and Gynecologists, Society for Maternal-Fetal Medicine. Obstetric Care Consensus No. 8: Interpregnancy Care. Obstet Gynecol 2019; 133: e51-e72
- 6 Wang Y, Zeng C, Chen Y. et al. Short interpregnancy interval can lead to adverse pregnancy outcomes: A meta-analysis. Front Med (Lausanne) 2022; 9: 922053
- 7 Chan S, Dong X. Effectiveness of Prophylactic Transvaginal Cervical Cerclage in Improving Clinical Outcomes among Pregnant Women with Cervical Insufficiency: Meta-Analysis. Open J Intern Med 2024; 14: 228-246
- 8 Giouleka S, Boureka E, Tsakiridis I. et al. Cervical Cerclage: A comprehensive Review of Major Guideline. Obstet Gynecol Surv 2023; 78: 544-553
- 9 Issah A, Diacci R, Williams KP. et al. McDonald versus Shirodkar cerclage technique in women requiring a prophylactic cerclage: a systematic review and meta-analysis protocol. Syst Rev 2021; 10: 130
- 10 McDonald IA. Suture of the cervix for inevitable miscarriage. J Obstet Gynaecol Br Emp 1957; 64: 346-350
- 11 Shirodkar VN. A new method of operative treatment for habitual abortion in the second trimester of pregnancy. Antiseptic 1955; 52: 299
- 12 Berger R, Abele H, Bahlmann F. et al. Prevention and Therapy of Preterm Birth. Guideline of the DGGG, OEGGG and SGGG (S2k-Level, AWMF Registry Number 015/025, September 2022) – Part 1. Geburtshilfe Frauenheilkd 2023; 83: 547-568
- 13 Kindinger LM, MacIntyre DA, Lee YS. et al. Relationship between vaginal microbial dysbiosis, inflammation, and pregnancy outcomes in cervical cerclage. Sci Transl Med 2016; 8: 350ra102
- 14 Mehta CR, Patel NR. A network algorithm for performing Fisher’s exact test in r×c contingency tables. J Am Stat Assoc 1983; 78: 427-434
- 15 Shapiro SS, Wilk MB. An analysis of variance test for normality (complete samples). Biometrika 1965; 52: 591-611
- 16 Kruskal WH, Wallis WA. Use of ranks in one-criterion variance analysis. J Am Stat Assoc 1952; 47: 583-621
- 17 Conde-Agudelo A, Rosas-Bermúdez A, Kafury-Goeta AC. Birth spacing and risk of adverse perinatal outcomes: a meta-analysis. JAMA 2006; 295: 1809-1813
- 18 Tanigawa K, Ikehara S, Cui M. et al. Association Between Interpregnancy Interval and Risk of Preterm Birth and Its Modification by Folate Intake: The Japan Environment and Children's Study. J Epidemiol 2023; 33: 113-119
- 19 Saling E. Der frühe totale Muttermundverschluss zur Vermeidung habitueller Aborte und Frühgeburten. Z Geburtsh Perinat 1981; 185: 259-261
- 20 Saling E, Schumacher E. Der operative Totale Muttermund-Verschluss (TMV). Z Geburtshilfe Neonatol 1996; 200: 82-87
- 21 Szendi B. Vollständiges Zusammennähen des äußeren Muttermundes auf blutigem Wege zur Verhinderung von fortgeschrittenem Abortus und Frühgeburten. Zentralbl Gynakol 1961; 83: 1083-1087
- 22 Zayyan M, Suhyb SR, Laurel NO. The Use of Total Cervical Occlusion along with McDonald Cerclage in Patients with Recurrent Miscarriage or Preterm Deliveries. Oman Med J 2012; 27: 63-65
- 23 Braun J, Klockenbusch W. Nutzen von Pessar, Cerclage und Muttermundverschluss für das Überleben von Frühgeborenen. Geburtshilfe Frauenheilkd 2016; 76: 942-945
- 24 Wen X, Liang W, Zhai J. et al. The association between interpregnancy intervals and preterm birth: a systematic review and meta-analysis. BMC Pregnancy Childbirth 2025; 25: 226
- 25 Ni W, Gao X, Su X. et al. Birth spacing and risk of adverse pregnancy and birth outcomes: A systematic review and dose-response meta-analysis. Acta Obstet Gynecol Scand 2023; 102: 1618-1633
- 26 Gudnadottir U, Debelius J, Du J. et al. The vaginal microbiome and the risk of preterm birth: a systematic review and network meta-analysis. Sci Rep 2022; 12: 7926
- 27 Odogwu NM. Role of short interpregnancy interval, birth mode, birth practices, and the post-partum vaginal microbiome in preterm birth. Front Reprod Health 2023; 4: 1082199
- 28 Costello EK, DiGiulio DB, Robaczewska A. et al. Abrupt perturbation and delayed recovery of the vaginal ecosystem following childbirth. Nat Commun 2023; 14: 4141


