
RSS-Feed abonnieren
DOI: 10.1055/a-2657-9236
Radiological Pain Therapy of the Spine: Retrospective Analysis of 2021 DeGIR Registry Data
Artikel in mehreren Sprachen: deutsch | English
- Abstract
- Introduction
- Materials & Methods
- Results
- Discussion
- Limitations
- Conclusions
- Clinical relevance of the study
- Literatur
Abstract
Purpose
To evaluate image-guided pain therapies on the spine based on data collected in the DeGIR quality assurance (QS) registry for the year 2021, in order to analyze the radiological care situation in Germany.
Materials and Methods
A total of 28915 interventions were analyzed from the DeGIR registry’s documented clinical and procedural data for pain management procedures in 2021. The focus was on spine-related therapies, examining the type, location, and methodology of the applied treatments as well as any complications that occurred.
Results
The analysis included 27139 interventions coded as pain management infiltrations in the spinal region. The average patient age was 62 years. Repeat procedures were performed in 4923 cases (29.1%). CT guidance was used in 95.6% of cases. In 15623 interventions (57.6%), local contrast agent was applied for documentation purposes.
Of the procedures, 7848 (28.9%) were performed on joint structures and 19291 (71.1%) on spinal nerves (transforaminal or translaminar); the majority of interventions, 22184 (81.7%), were carried out in the lumbar and sacral sections of the spine.
Complications were documented in 53 cases (0.2%). The vast majority of these were mild complications of categories A or B (49 cases). One death was reported (0.004%). No neuro-cerebral complications were recorded.
Conclusion
The evaluation of the registry data shows a typical distribution pattern of radiological interventional pain therapies on the spine with regard to epidemiological data, localization, and type of therapy. The vast majority of these are performed under CT guidance with very few complications.
Future data collection efforts should aim to include more precise information on patient history, indications, procedural details, and particularly clinical outcome quality.
Key Point
Radiologically guided interventional pain therapies on the spine in Germany are performed safely and, in the vast majority of cases, under CT imaging guidance.
Citation Format
-
Fessl R, Wacker FK, Wilhelm K et al. Radiological Pain Therapy of the Spine: Retrospective Analysis of 2021 DeGIR Registry Data. Rofo 2025; DOI 10.1055/a-2657-9236
Introduction
The prevalence of back pain is high, and in Germany it is reported to be between 30% to 70%. Estimates of lifetime prevalence, i.e. back pain experienced by people at least once in their lifetime, range from 74% to 85%, and 62% of individuals affected are still not pain-free even after 12 months. Back pain, particularly when chronic, can have significant economic consequences. In 2010, back pain was the leading reason for days missed due to incapacity to work and medical rehabilitation for persons insured by German statutory health insurance providers. When individuals are unable to work for a period of more than six months, 60% do not return to work. In 2010, musculoskeletal disorders were the second most common cause of early retirement (pensions due to reduced earning capacity) after mental and behavioral disorders. In 2008, the medical costs of back pain in Germany were estimated at EUR 9 billion in 2008. Indirect costs, e.g. for rehabilitation and early retirement, are estimated at an additional EUR 15 billion [1] [2] [3].
Alongside physical and medication-based therapy approaches, minimally invasive percutaneous spinal therapy procedures are becoming increasingly popular. In Germany, these procedures are performed by interventional specialists in outpatient and inpatient settings, e.g. orthopedics, anesthesiology, neurosurgery, or radiology, and sometimes also general medicine. Complications from these procedures are generally rare, and results are published only in smaller case histories or documented in retrospective cohort studies using primarily fluoroscopy-guided procedures in the US, although relevant and severe complications have also been described [4] [5].
Heterogeneity of the included patient groups, the small number of cases in individual studies, and the lack of differentiation between specific and non-specific causes of pain often prevent reliable conclusions about the effectiveness of the procedures used [6] [7].
The DeGIR-QS-Register is the quality registry of the German Society for Interventional Radiology and Minimally Invasive Therapy (DeGIR). The software program enables users to record all radiological interventions for the purpose of comprehensive quality assurance. Starting in 2005, radiological facilities throughout Germany and Austria have documented their interventions in the central DeGIR quality assurance (QS) registry. Participation in documenting quality information is voluntary. However, it is required for certification of DeGIR/DGNR centers and recognized interdisciplinary vascular centers. The DeGIR-QS-Register contains pseudonymized patient data after consent in accordance with Art. 9 (1) (a) GDPR. Currently, over 220000 procedures are recorded every year. Anonymized data can be exported from the registry to conduct retrospective analyses.
The aim of this analysis is to document the type and number, as well as the adverse effects, of fluoroscopy-guided and CT-guided pain therapies in Germany, using data from 2021 collected in the DeGIR-QS-Register.
Materials & Methods
This retrospective study was conducted in accordance with the Declaration of Helsinki, Section 15 of the Professional Code of Conduct, and in consultation with the responsible ethics committee according to applicable faculty law.
The study is based on retrospective analysis of the pseudonymized clinical and procedural data on pain management interventions documented in the DeGIR registry. For 2021, this included a total of 28,915 data sets from over 300 German hospitals, 27139 of which involved pain management interventions on the spine.
We analyzed the type, location, and methodology of the applied treatments, as well as adverse effects that occurred during fluoroscopy-guided and CT-guided pain management measures on the spine.
Implausible data were excluded after statistical exploration.
Results
Out of 28915 data sets, 27139 were evaluated and coded as pain management infiltrations in the entire spinal region. The data sets not considered involved ganglion blocks (n=661) and peripheral nerve blocks (n=1115).
The 27139 procedures evaluated were performed on a total of 16893 patients, including 8827 female patients (52.3%) and 8,066 male patients (47.7%). The average age was 62 years (6–101). Repeat procedures were performed in 4923 cases (29.1%) ([Table 1]).
As preliminary examinations (sometimes with multiple mentions), an MRI was available at the time of therapy in 16858 cases (62.1%); a CT scan in 10532 cases (38.8%); projection radiography was available in 3,341 cases (12.3%), and no preliminary examination was performed in 1570 cases (5.8%). The procedures were performed on an outpatient basis in 14724 cases (54.3%) and in an inpatient setting in 12415 cases (45.7%).
Contrast agent was administered to document the distribution of medication in 15623 of the procedures (57.6%) and in 12955 of the 19291 spinal nerve procedures (67.2%).
Corticosteroids were used in 23490 cases (86.6%). Local anesthesia was administered in 25811 cases (95.1%).
With regard to the modalities used, 25789 of the procedures were exclusively CT-guided (95.0%), 435 were performed using DSA/fluoroscopy (1.6%), 764 were ultrasound-guided (2.8%), and 5 procedures were performed using MRI imaging guidance (0.02%). A combination of modalities (CT-MRI, CT-ultrasound, CT-DSA) was performed in 146 of the procedures (0.5%). CT was used in 25935 of the cases (95.6%), and fluoroscopy-guided/DSA procedures in 576 cases (2.1%).
With regard to the anatomical target region, the following data were obtained ([Fig. 1]):

-
Joints (facet joints and sacroiliac joint):
-
cervical: 782 (2.9%)
-
thoracic: 173 (0.6%)
-
lumbar and sacral: 6893 (25.4%)
-
-
Spinal nerves (translaminar, transforaminal):
-
cervical: 3655 (13.5%)
-
thoracic: 345 (1.3%)
-
lumbar and sacral: 15291 (56.3%)
-
Joint denervation procedures using radiofrequency ablation were performed in 103 cases (0.4%); in 15 cases using cryotherapy (0.1%), and in 314 cases using alcohol (1.2%).
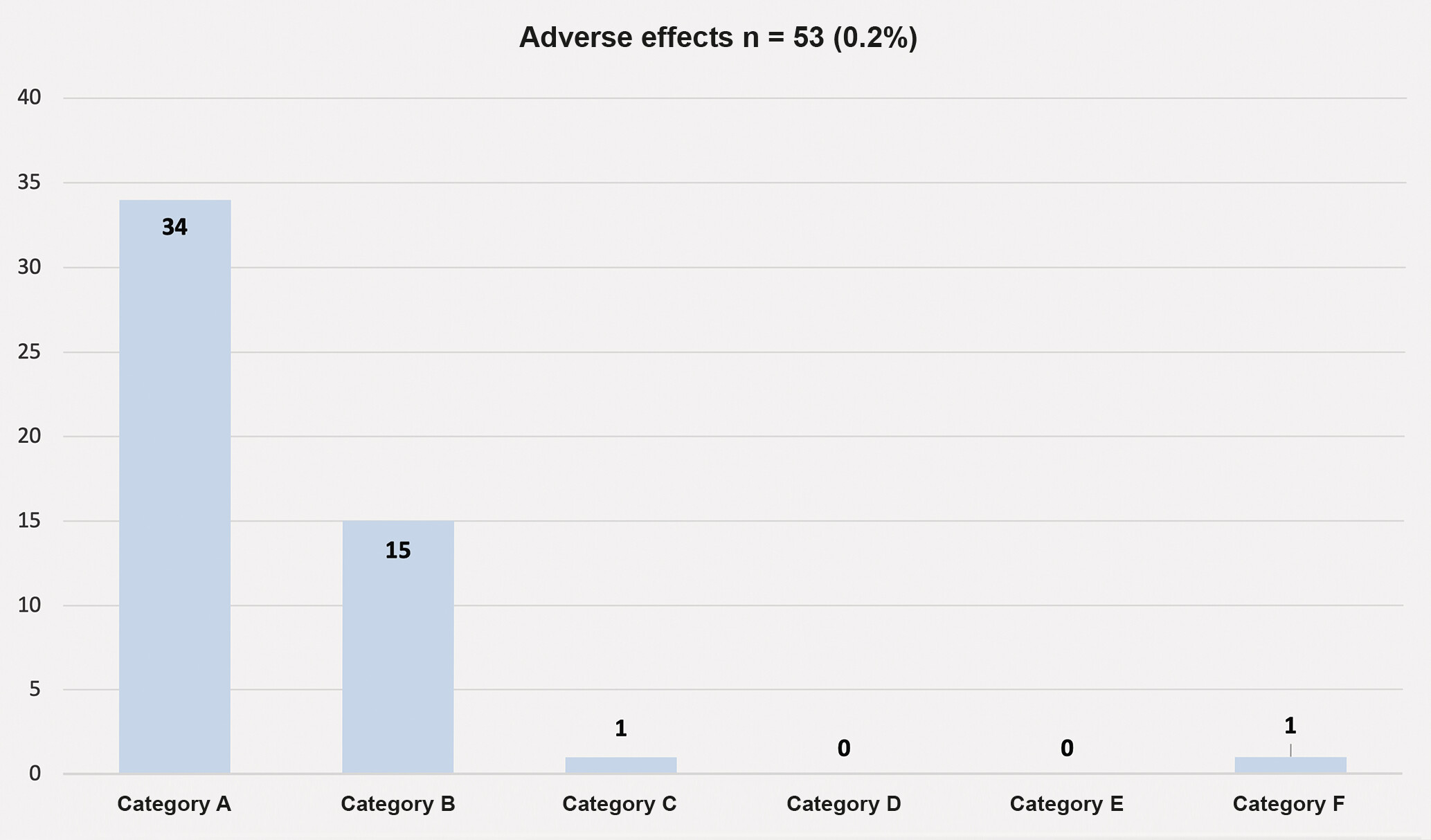
Adverse effects occurred in 53 cases (0.2%), which were classified in five categories (A-F) based on the severity of complications according to the classification system developed by the Cardiovascular and Interventional Radiological Society of Europe (CIRSE) [8]. Category A corresponds to “no need for treatment, no consequences”; category B reflects “symptomatic treatment, overnight observation, if necessary”; category C shows “need for therapy, short hospital stay < 48 hours”; category D indicates “need for greater treatment, unplanned increase in treatment level, extended hospital stay > 48 hours”; category E indicates “permanent damage,” and lastly category F indicates “death”.
Mild cases included 34 cases in category A, 15 cases in category B, and one case in category C. No cases were documented in categories D and E. In category F (fatal), there was one case; no information about category was provided in two cases ([Fig. 2]).
Of the 53 complications documented, nine cases involved interventions using fluoroscopy/DSA (seven of which were category A, one category B, one with no category specified) and one case using ultrasound (category B). Forty-five documented cases used CT imaging guidance.
One complication in category C corresponded to a medication-related side effect, and one complication in category F resulted from a cardiac complication with exitus letalis within 24 hours post-intervention ([Table 2]).
Discussion
Pain originating from the spine, which in the majority of cases is degenerative, is highly prevalent, and it represents a heavy burden for individuals and the economy. In addition to the guideline-compliant indication for specific red flags, for example, in the form of radiculopathies that do not require primary surgery [9] or specific dorsalgia [10], a comprehensive interdisciplinary assessment should be carried out, as recommended by the national care guideline for non-specific low back pain [11], if pain lasts for six weeks in spite of guideline-compliant therapy and positive evidence of risk factors for pain becoming chronic, in order to check the indication for a multimodal therapy program. In this context, injection therapy can also play a major role after conservative measures have been exhausted, particularly when treating degenerative spinal diseases.
Minimally invasive percutaneous pain management procedures on the spine are therefore becoming increasingly important in the broad treatment spectrum. Image-guided injection of analgesic, anti-inflammatory, and anti-edematous preparations at the starting points of nociception improves not only pain management but also supports the differential diagnosis of the cause of pain, for example, helping to identify causes of radicular versus pseudoradicular pain, as well as the nerve root affected in unclear cases. Local anesthesia and corticosteroids are mainly used in the area of pain-causing structures, such as joints, nerve roots, and the entire spinal epidural space. Depending on the clinical situation, transforaminal (PRT) and interlaminar (LESI or epidural flooding) approaches are used for therapies in the epidural space; in the thoracic and lumbar spine, only dorsal or dorsolateral approaches (usually) in prone position are used, while in the cervical spine, ventrolateral and posterolateral approaches in supine and prone positions are used to access the neuroforamen [12]. It should be noted that use of corticoids in the epidural space is an “off-label” therapeutic treatment, but it corresponds to a long-established clinical practice recommended by guidelines [9] [10]. Current guidelines [9] [10] [13] recommend administration of exclusively non-crystalline cortisone preparations, such as dexamethasone for cervical transforaminal injections, because the aggregation of particles in crystalline cortisone can pose a risk of thromboembolic complications – with sometimes catastrophic consequences – in the event of accidental intravascular application.
For injections, radiological imaging techniques such as “landmark-assisted” fluoroscopy are used, possibly with additional digital subtraction technology and computed tomography (CT), as well as ultrasound in a few but increasing number of cases; on rare occasions, MRI is used.
Sufficient evidence exists regarding the effectiveness and accuracy of the two “workhorse” technologies, fluoroscopy and computed tomography. When comparing the two techniques, CT has the advantage of providing a direct visualization of the target tissue and the structures at risk, as well as better contrast resolution under optimized conditions, with comparable radiation exposure for the patient [14] [15] [16] [17] [18] [19] [20]. In German-speaking countries, computed tomography is thus preferred for interventional spinal pain management, particularly in radiological facilities, which is confirmed in 95.6% of cases by analyzing the available DeGIR QS registry data involving CT-guided interventions.
Only 435 of the procedures were performed exclusively using DSA/fluoroscopy (1.6%), and 141 were performed in combination with DSA and CT (0.5%). A total of only 576 were thus performed using fluoroscopy alone or additionally using digital subtraction technology (2.1%).
Adverse effects were documented in 53 cases (0.2%). Of these, 49 cases were mild (category A-B). One complication, category C, corresponded to a medication-related adverse reaction; one complication, category F, corresponded to a cardiac complication with exitus letalis within 24 hours post-intervention (both during CT-guided interventions). It should, however, be noted that it is worth discussing the extent to which the category F complication can be attributed causally to the intervention. There were no relevant neurological/neurocerebral complications. This confirms, in accordance with extensive literature available [21] [22] [23] [24] [25], that interventional pain therapies of the spine are a very low-complication procedure, even in the hands of interventional radiologists. Information on potential infections is not available, as only direct post- or peri-interventional follow-up checks were documented. For the 27139 documented interventions, a worsening of pain symptoms was reported in 60 cases (0.2%); elimination or improvement of pain symptoms was reported in 16714 cases (61.6%); consistent findings were reported for 1626 cases (6%), and no information was provided in 8739 cases (32.2%). Data on pain symptoms during the course of treatment were not logged.
Local injection of contrast agent is used prior to application of medication to ensure correct distribution at the target structure and it is of critical importance due to the anatomical proximity to venous and arterial vessels, particularly in the periradicular area or the epidural space to rule out accidental intravascular application [26] [27] [28] [29] [30]. The data available document contrast administration in only 57.6% of cases overall, and contrast agent was used in only 67.2% of cases in spinal nerve interventions (translaminar or interlaminar). This number is surprisingly low in light of the current literature. Nevertheless, our analysis shows only very low rates of complications and, in particular, there was not a single documented case of a complication induced by accidental intra-arterial administration of medication, such as cerebral thromboembolism or neurological deficits and paraplegia.
Limitations
This retrospective analysis of data from the DeGIR-QS-Register for over 300 hospitals in Germany with 27139 data sets from 2021 is subject to a certain selection bias due to the voluntary nature of the entries.
Because the DeGIR software is a quality assurance tool, some clinical information is not primarily collected. For this reason, the software cannot be used currently to provide a comprehensive clinical analysis. In addition, it is not possible to make any statements about the course of the disease, because not all hospitals are able to collect clinical data from outpatients on a regular basis.
Conclusions
This analysis of data from the DeGIR-QS registry for the year 2021 examined a total of 27139 pain management interventions on the spine, and it shows that image-guided pain therapy on the spine by interventional radiologists is a safe method with very few complications. Computed tomography is used in the vast majority of cases for image control.
It should be noted that, particularly for treatments in the epidural space such as transforaminal (PRT) and interlaminar (LESI or epidural flooding) approaches, it is essential to document that the medication is distributed correctly, excluding intravascular needle placement, at the target structure with contrast agent.
To make further valid clinical statements beyond strictly providing quality assurance for the procedures, more detailed data on the anamnesis, symptoms, indication, implementation, and clinical course are necessary, in order to document pain management interventions on the spine. All of this could, for example, be carried out as part of a prospective registry study.
Clinical relevance of the study
-
Image-guided pain therapies of the spine are conducted safely and with very few complications by interventional radiologists.
-
Computed tomography is the “workhorse” of image-guided pain therapy procedures performed by radiologists.
Conflict of Interest
Robert Fessl: Member of DeGIR Kai Wilhelm: Co-opted member of the DeGIR Executive Board during the period under review (DeGIR representative on the DGNR Executive Board) Frank Wacker: President-elect and current President of DeGIR Jonathan Nadijir: Co-opted member of the DeGIR Executive Board with responsibility for the DeGIR Register Ansgar Berlis: DeGIR membership. President of DGNR during the period under review, currently Past President of DGNR.
Acknowledgement
Many thanks to Dr. Stefan Schiele from the Institute for Mathematics and Statistical Consulting and Prof. Gernot Müller from the University of Augsburg for their support in statistically processing the data sets.
-
Literatur
- 1 Casser HR, Seddigh S, Rauschmann M. Akuter lumbaler Rückenschmerz, Diagnostik, Differenzialdiagnostik und Therapie. Dtsch Ärztebl 2016; 113: 223-234
- 2 von der Lippe E, Krause L, Porst M. et al. Prävalenz von Rücken- und Nackenschmerzen in Deutschland. Ergebnisse der Krankheitslast-Studie BURDEN 2020. J Health Monit 2021; 6: 2-14
- 3 Raspe Heiner, Gesundheitsberichterstattung des Bundes. Robert Koch-Institut in Zusammenarbeit mit dem Statistischen Bundesamt. 2012; 53. DOI: org/10.25646/3164.
- 4 Abrecht CR, Ramsey S, Greenberg P. et al. A Contemporary Medicolegal Analysis of Outpatient Interventional Pain Procedures: 2009–2016. Anesth Analg 2019; 129: 255-262
- 5 Eworuke E, Crisafi L, Liao J. et al. Risk of serious spinal adverse events associated with epidural corticosteroid injections in the Medicare population. Reg Anesth Pain Med 2021; 46: 203-209
- 6 Henschke N, Kuijpers T, Rubinstein SM. et al. Injection therapy and denervation procedures for chronic low-back pain: A systematic review. Eur Urol Focus 2010; 19: 1425-49
- 7 Oliveira CB, Maher CG, Ferreira ML. et al. Epidural corticosteroid injections for lumbosacral radicular pain. Cochrane Database Syst Rev 2020; 4: CD013577
- 8 Filippiadis DK, Pereira PL, Hausegger KA. et al. CIRSE Classification System for Complications’ Reporting: A Project Evaluation Process. Cardiovasc Intervent Radiol 2024; 47: 1160-1162
- 9 S2k-Leitlinie Konservative, operative und rehabilitative Versorgung bei Bandscheibenvorfällen mit radikulärer Symptomatik, AWMF-Registernummer: 187–057.
- 10 DGOU Leitlinie 187–059 – Spezifischer Kreuzschmerz. Deutsche Gesellschaft für Orthopädie und Unfallchirurgie e.V.: Spezifischer Kreuzschmerz: Version 2.0 (March 12, 2024).
- 11 Bundesärztekammer (BÄK), Kassenärztliche Bundesvereinigung (KBV), Arbeitsgemeinschaft der Wissenschaftlichen Medizinischen Fachgesellschaften (AWMF). Nationale VersorgungsLeitlinie Nicht-spezifischer Kreuzschmerz – Langfassung, 2nd edition. Version 1. 2017 AWMF register no.: nvl-007.
- 12 Bise S, Pesque L, Feldis M. et al. Comparison of three CT-guided epidural steroid injection approaches in 104 patients with cervical radicular pain: transforaminal anterolateral, posterolateral, and transfacet indirect. Skeletal Radiol 2018; 47: 1625-1633
- 13 NICE, 2016. Low back pain and sciatica in over 16s: Assessment and management. Invasive treatments. NICE guideline NG59: Methods, evidence and recommendations. London: National Institute for Health and Care Excellence (NICE) 2016;
- 14 Bogdanovic S, Sutter R, Zubler V. Spine injections: The rationale for CT guidance. Skeletal Radiol 2023; 52: 1853-1862
- 15 Dietrich TJ, Peterson CK, Zeimpekis KG. et al. Fluoroscopy-guided versus CT-guided Lumbar Steroid Injections: Comparison of Radiation Exposure and Outcomes. Radiology 2019; 290: 752-759
- 16 Elsholtz FHJ, Kamp JE, Vahldiek JL. et al. Periradicular Infiltration of the Cervical Spine: How New CT Scanner Techniques and Protocol Modifications Contribute to the Achievement of Low-Dose Interventions. Fortschr Röntgenstr 2019; 191: 54-61
- 17 Lindemann C, Strube P, Fisahn C. et al. Next Level in Computed Tomography-Guided Periradicular Infiltration Therapy: Same Efficiency with Less Radiation Exposure. World Neurosurg 2023; 171: e24-e30
- 18 Palmer WE. Spinal injections for pain management. Radiology 2016; 281: 669-688
- 19 Rafati A, Ghanaati H, Asadi B. et al. Outcomes of the Fluoroscopically-Guided vs. Computed-Tomography-Guided Transforaminal Epidural Steroid Injection in Low Back Pain: A Propensity-matched Prospective Cohort. Med J Islam Republ Iran 2023; 37: 23
- 20 Wieschhoff GG, Miskin NP, Kim JS. et al. Radiation dose of fluoroscopy-guided versus ultralow-dose CT-fluoroscopy-guided lumbar spine epidural steroid injections. Skeletal Radiol 2022; 51: 1055-62
- 21 Fenster AJ, Fernandes K, Brook AL. et al. The Safety of CT-Guided Epidural Steroid Injections in an Older Patient Cohort. Pain Physician 2016; 19: E1139-E1146
- 22 Kamp JPM, Bartlett J, Fahmy A. et al. CT‑guided vs. fluoroscopically guided transforaminal epidural steroid injections for lumbar radiculopathy: a comparison of efficacy, safety and cost. Arch Orthop Trauma Surg 2023; 143: 2355-2361
- 23 Amrhein TJ, Parivash SN, Gray L. et al. Incidence of Inadvertent Dural Puncture During CT Fluoroscopy – Guided Interlaminar Epidural Corticosteroid Injections in the Cervical Spine: An Analysis of 974 Cases. AJR Am J Roentgenol 2017; 209: 656-661
- 24 Cotton A, Drapé JL, Sans N. et al. Société d’imagerie musculosquelettique (SIMS), Fédération de radiologie interventionnelle (FRI), and Société française de radiologie (SFR). recommendations for epidural and transforaminal corticosteroid injections. Diagn Interv Imaging 2018; 99: 219-224
- 25 Bise S, Langlet B, Pesquer L. et al. Transforaminal versus interlaminar CT-guided lumbar epidural steroid injections: prospective study of 237 patients with unilateral radicular pain and up to 5 years of follow-up. Skeletal Radiol 2023; 52: 1959-1967
- 26 Kranz PG, Amrhein TJ, Gray L. Incidence of Inadvertent Intravascular Injection during CT Fluoroscopy-guided Epidural Steroid Injections. AJNR Am J Neuroradiol 2015; 36: 1000-1007
- 27 Wald JT, Maus TP, Diehn FE. et al. CT-guided cervical transforaminal epidural steroid injections: Technical insights. J Neuroradiol 2014; 41: 211-215
- 28 Maus T. The Anatomy, Technique, Safety, and Efficacy of Image-guided Epidural Access. Radiol Clin North Am 2024; 62: 199-215
- 29 Rathmell JP, Benzon HT, Dreyfuss P. et al. Safeguards to prevent neurologic complications after epidural steroid injections: consensus opinions from a multidisciplinary working group and national organizations. Anesthesiology 2015; 122: 974-984
- 30 Klessinger S, Wiechert K. Deutsche Wirbelsäulengesellschaft. S3-Leitlinie Epidurale Injektionen bei degenerativen Erkrankungen. Version 01, 2025. https://register.awmf.org/de/leitlinien/detail/151–005
Korrespondenzadresse
Publikationsverlauf
Eingereicht: 31. Mai 2025
Angenommen nach Revision: 11. Juli 2025
Artikel online veröffentlicht:
01. August 2025
© 2025. Thieme. All rights reserved.
Georg Thieme Verlag KG
Oswald-Hesse-Straße 50, 70469 Stuttgart, Germany
-
Literatur
- 1 Casser HR, Seddigh S, Rauschmann M. Akuter lumbaler Rückenschmerz, Diagnostik, Differenzialdiagnostik und Therapie. Dtsch Ärztebl 2016; 113: 223-234
- 2 von der Lippe E, Krause L, Porst M. et al. Prävalenz von Rücken- und Nackenschmerzen in Deutschland. Ergebnisse der Krankheitslast-Studie BURDEN 2020. J Health Monit 2021; 6: 2-14
- 3 Raspe Heiner, Gesundheitsberichterstattung des Bundes. Robert Koch-Institut in Zusammenarbeit mit dem Statistischen Bundesamt. 2012; 53. DOI: org/10.25646/3164.
- 4 Abrecht CR, Ramsey S, Greenberg P. et al. A Contemporary Medicolegal Analysis of Outpatient Interventional Pain Procedures: 2009–2016. Anesth Analg 2019; 129: 255-262
- 5 Eworuke E, Crisafi L, Liao J. et al. Risk of serious spinal adverse events associated with epidural corticosteroid injections in the Medicare population. Reg Anesth Pain Med 2021; 46: 203-209
- 6 Henschke N, Kuijpers T, Rubinstein SM. et al. Injection therapy and denervation procedures for chronic low-back pain: A systematic review. Eur Urol Focus 2010; 19: 1425-49
- 7 Oliveira CB, Maher CG, Ferreira ML. et al. Epidural corticosteroid injections for lumbosacral radicular pain. Cochrane Database Syst Rev 2020; 4: CD013577
- 8 Filippiadis DK, Pereira PL, Hausegger KA. et al. CIRSE Classification System for Complications’ Reporting: A Project Evaluation Process. Cardiovasc Intervent Radiol 2024; 47: 1160-1162
- 9 S2k-Leitlinie Konservative, operative und rehabilitative Versorgung bei Bandscheibenvorfällen mit radikulärer Symptomatik, AWMF-Registernummer: 187–057.
- 10 DGOU Leitlinie 187–059 – Spezifischer Kreuzschmerz. Deutsche Gesellschaft für Orthopädie und Unfallchirurgie e.V.: Spezifischer Kreuzschmerz: Version 2.0 (March 12, 2024).
- 11 Bundesärztekammer (BÄK), Kassenärztliche Bundesvereinigung (KBV), Arbeitsgemeinschaft der Wissenschaftlichen Medizinischen Fachgesellschaften (AWMF). Nationale VersorgungsLeitlinie Nicht-spezifischer Kreuzschmerz – Langfassung, 2nd edition. Version 1. 2017 AWMF register no.: nvl-007.
- 12 Bise S, Pesque L, Feldis M. et al. Comparison of three CT-guided epidural steroid injection approaches in 104 patients with cervical radicular pain: transforaminal anterolateral, posterolateral, and transfacet indirect. Skeletal Radiol 2018; 47: 1625-1633
- 13 NICE, 2016. Low back pain and sciatica in over 16s: Assessment and management. Invasive treatments. NICE guideline NG59: Methods, evidence and recommendations. London: National Institute for Health and Care Excellence (NICE) 2016;
- 14 Bogdanovic S, Sutter R, Zubler V. Spine injections: The rationale for CT guidance. Skeletal Radiol 2023; 52: 1853-1862
- 15 Dietrich TJ, Peterson CK, Zeimpekis KG. et al. Fluoroscopy-guided versus CT-guided Lumbar Steroid Injections: Comparison of Radiation Exposure and Outcomes. Radiology 2019; 290: 752-759
- 16 Elsholtz FHJ, Kamp JE, Vahldiek JL. et al. Periradicular Infiltration of the Cervical Spine: How New CT Scanner Techniques and Protocol Modifications Contribute to the Achievement of Low-Dose Interventions. Fortschr Röntgenstr 2019; 191: 54-61
- 17 Lindemann C, Strube P, Fisahn C. et al. Next Level in Computed Tomography-Guided Periradicular Infiltration Therapy: Same Efficiency with Less Radiation Exposure. World Neurosurg 2023; 171: e24-e30
- 18 Palmer WE. Spinal injections for pain management. Radiology 2016; 281: 669-688
- 19 Rafati A, Ghanaati H, Asadi B. et al. Outcomes of the Fluoroscopically-Guided vs. Computed-Tomography-Guided Transforaminal Epidural Steroid Injection in Low Back Pain: A Propensity-matched Prospective Cohort. Med J Islam Republ Iran 2023; 37: 23
- 20 Wieschhoff GG, Miskin NP, Kim JS. et al. Radiation dose of fluoroscopy-guided versus ultralow-dose CT-fluoroscopy-guided lumbar spine epidural steroid injections. Skeletal Radiol 2022; 51: 1055-62
- 21 Fenster AJ, Fernandes K, Brook AL. et al. The Safety of CT-Guided Epidural Steroid Injections in an Older Patient Cohort. Pain Physician 2016; 19: E1139-E1146
- 22 Kamp JPM, Bartlett J, Fahmy A. et al. CT‑guided vs. fluoroscopically guided transforaminal epidural steroid injections for lumbar radiculopathy: a comparison of efficacy, safety and cost. Arch Orthop Trauma Surg 2023; 143: 2355-2361
- 23 Amrhein TJ, Parivash SN, Gray L. et al. Incidence of Inadvertent Dural Puncture During CT Fluoroscopy – Guided Interlaminar Epidural Corticosteroid Injections in the Cervical Spine: An Analysis of 974 Cases. AJR Am J Roentgenol 2017; 209: 656-661
- 24 Cotton A, Drapé JL, Sans N. et al. Société d’imagerie musculosquelettique (SIMS), Fédération de radiologie interventionnelle (FRI), and Société française de radiologie (SFR). recommendations for epidural and transforaminal corticosteroid injections. Diagn Interv Imaging 2018; 99: 219-224
- 25 Bise S, Langlet B, Pesquer L. et al. Transforaminal versus interlaminar CT-guided lumbar epidural steroid injections: prospective study of 237 patients with unilateral radicular pain and up to 5 years of follow-up. Skeletal Radiol 2023; 52: 1959-1967
- 26 Kranz PG, Amrhein TJ, Gray L. Incidence of Inadvertent Intravascular Injection during CT Fluoroscopy-guided Epidural Steroid Injections. AJNR Am J Neuroradiol 2015; 36: 1000-1007
- 27 Wald JT, Maus TP, Diehn FE. et al. CT-guided cervical transforaminal epidural steroid injections: Technical insights. J Neuroradiol 2014; 41: 211-215
- 28 Maus T. The Anatomy, Technique, Safety, and Efficacy of Image-guided Epidural Access. Radiol Clin North Am 2024; 62: 199-215
- 29 Rathmell JP, Benzon HT, Dreyfuss P. et al. Safeguards to prevent neurologic complications after epidural steroid injections: consensus opinions from a multidisciplinary working group and national organizations. Anesthesiology 2015; 122: 974-984
- 30 Klessinger S, Wiechert K. Deutsche Wirbelsäulengesellschaft. S3-Leitlinie Epidurale Injektionen bei degenerativen Erkrankungen. Version 01, 2025. https://register.awmf.org/de/leitlinien/detail/151–005

