

Subscribe to RSS
DOI: 10.1055/a-2663-7161
Association Between Major Bleeding and In-Hospital Major Adverse Cardiovascular Events After Percutaneous Coronary Intervention in Acute Coronary Syndromes
Authors

Abstract
Background
Major bleeding (MB) is a serious complication in patients with acute coronary syndromes (ACS) undergoing percutaneous coronary intervention (PCI). Although its association with long-term adverse outcomes is well documented, the impact of in-hospital MB on early cardiovascular prognosis remains incompletely characterized.
Objective
To investigate the association between in-hospital MB and major adverse cardiovascular events (MACE) in patients with ACS treated with PCI.
Methods
We conducted a retrospective cohort study on 829 consecutive ACS patients who underwent successful PCI between January 2021 and December 2023. MB was defined as Bleeding Academic Research Consortium (BARC) type 3 or 5 bleeding events. MACE was defined as a composite of all-cause mortality, recurrent myocardial infarction, ischemic stroke, urgent target vessel revascularization, or new-onset/decompensated heart failure with left ventricular ejection fraction (LVEF) <30%. Clinical data and outcomes were extracted from hospital records and independently adjudicated.
Results
MB occurred in 4.5% of patients (n = 37). The incidence of in-hospital MACE was significantly higher among patients with MB compared to those without (40.5% vs. 8.1%, p < 0.001). In multivariate logistic regression, MB was the strongest independent predictor of in-hospital MACE (OR: 12.43, 95% CI: 3.43–44.98, p < 0.001), followed by reduced LVEF (OR per % increase: 0.794, 95% CI: 0.747–0.843, p < 0.001), age, and white blood cell count.
Conclusions
In-hospital MB is a potent and independent predictor of early MACE in patients with ACS undergoing PCI. These findings emphasize the need for careful risk stratification, bleeding prevention strategies, and individualized antithrombotic management in this high-risk population.
Keywords
acute coronary syndrome - percutaneous coronary ıntervention - major bleeding - major adverse cardiovascular events - dual antiplatelet therapy - BARC bleeding criteria - in-hospital outcomesIntroduction
Acute coronary syndrome (ACS) is a major global health burden and among the leading causes of cardiovascular morbidity and mortality. Percutaneous coronary intervention (PCI), in conjunction with dual antiplatelet therapy (DAPT), has significantly improved outcomes in patients with ACS by reducing ischemic complications.[1]
However, the benefits of PCI come at the cost of increased risk of bleeding, particularly in the context of aggressive antithrombotic therapy. Major bleeding (MB), commonly defined by the Bleeding Academic Research Consortium (BARC) criteria as type 3 or above, has been consistently associated with worse clinical outcomes.[2] These include not only increased short-term mortality but also adverse cardiovascular events such as myocardial infarction, stroke, and unplanned revascularization.[3] [4] [5] Several pathophysiological mechanisms have been proposed, including hemodynamic compromise, withdrawal of antiplatelet agents, and inflammatory responses following bleeding events.[6] [7]
Although the link between MB and poor prognosis is well established, it remains unclear whether bleeding is an independent predictor of adverse cardiovascular events or merely a surrogate marker for patient's frailty and comorbidities.[8] [9] Furthermore, much of the current evidence focuses on long-term outcomes, whereas the impact of in-hospital bleeding events on early post-PCI prognosis in patients with ACS is less well-characterized.[10]
This study aims to investigate the association between MB and major adverse cardiovascular events (MACE) in patients with ACS undergoing PCI, thereby providing further insight into the prognostic importance of bleeding during the acute phase of treatment.
Materials and Methods
Study Design and Setting
This retrospective observational cohort study was conducted in the cardiology department of a tertiary care hospital. This study adhered to the principles of the Declaration of Helsinki and was approved by the local institutional ethics committee. Due to the retrospective design of the study, the requirement for informed consent was waived.
Study Population
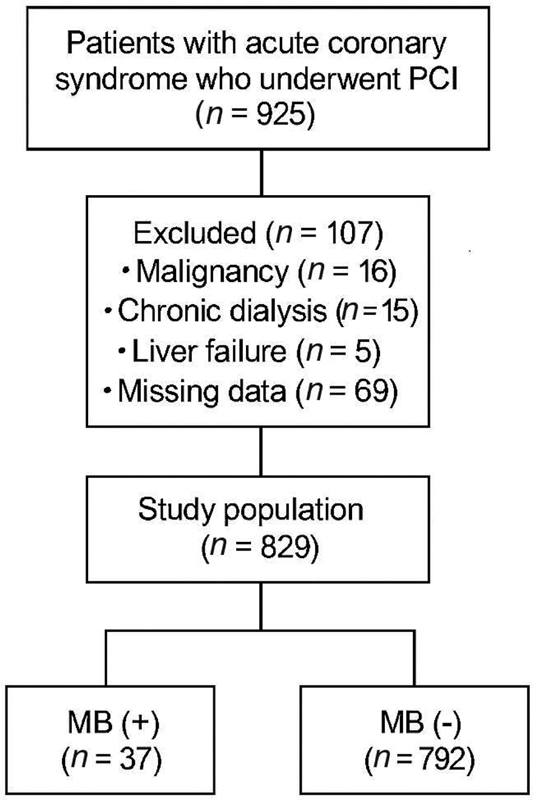
A total of 829 patients aged ≥18 years who were hospitalized with ACS and underwent PCI between January 2021 and December 2023 were included. Patients with incomplete clinical outcome data, active malignancy, end-stage renal disease requiring dialysis, or advanced hepatic dysfunction were excluded from the study. A detailed flowchart of the inclusion and exclusion process is presented in [Fig. 1].
Although patient care during the study period was guided by prior European Society of Cardiology (ESC) recommendations for consistency and clarity, ACS diagnoses in this analysis were retrospectively reviewed and classified according to the 2023 ESC guidelines.[11] The diagnosis of ACS was based on the presence of ischemic chest pain; electrocardiographic changes such as ST-segment elevation, depression, or new left bundle branch block; and/or a dynamic elevation in high-sensitivity cardiac troponin levels. ACS was further classified into ST-elevation myocardial infarction (STEMI), non-ST-elevation myocardial infarction (NSTEMI), or unstable angina, according to the combination of electrocardiographic and biochemical findings. All patients underwent successful PCI during the same index hospitalization, defined as a continuous hospital stay during which the ACS diagnosis was made and treated without inter-hospital transfer or staged procedures beyond the initial admission.
Definitions and Outcomes
MB was defined according to the BARC criteria as type 3 or 5 bleeding events that occurred during the in-hospital period.[2] [12] MACE were defined as a composite of clinically significant outcomes, including all-cause mortality, recurrent myocardial infarction, ischemic stroke, urgent target vessel revascularization, and new-onset or decompensated heart failure with a left ventricular ejection fraction (LVEF) of <30%. Although not included in all MACE definitions across clinical trials, we incorporated new-onset or decompensated heart failure with LVEF <30% to better reflect early post-PCI clinical deterioration in ACS patients. Prior evidence suggests that severe systolic dysfunction is a key prognostic marker in this population, justifying its inclusion in our composite outcome. All clinical events were verified through a detailed review of hospital medical records and independently adjudicated by two experienced cardiologists who were blinded to patient group assignments.
Data Collection
Demographic characteristics, clinical history, vital signs on admission, medication use, and laboratory parameters were extracted from the hospital's electronic medical record system. Echocardiographic data, particularly LVEF, were recorded from the initial transthoracic echocardiography performed during hospitalization. All data were collected and entered into an anonymized database by two independent research assistants.
Statistical Analysis
Statistical analyses were performed using the SPSS version 21.0 software (SPSS Inc., Chicago, IL, USA). Continuous variables were reported as mean ± standard deviation (SD) or median with interquartile range (IQR), depending on the normality of distribution assessed using the Kolmogorov–Smirnov test. Categorical variables are expressed as frequencies and percentages.
Group comparisons were performed using the independent-samples t-test or Mann–Whitney U test for continuous variables and the chi-square or Fisher's exact test for categorical variables. Variables with a p-value <0.05 in univariate analysis were included in a multivariate logistic regression model to identify independent predictors of in-hospital MACE. Results are reported as odds ratios (OR) with 95% confidence intervals (CI). For continuous variables, OR represent the change in the likelihood of the outcome per one-unit increase in the respective predictor variable (e.g., per 1 year increase in age, or per 1% change in LVEF). Statistical significance was set at a two-tailed p-value <0.05.
Results
In total, 829 patients who underwent PCI for ACS were included in this study. The mean age of the study population was 62.0 ± 12.1 years, and 74.9% were male. MB, defined as BARC type ≥3, was observed in 37 patients (4.5%), whereas in-hospital MACE occurred in 79 patients (9.5%).
Comparison According to Major Bleeding Status
Patients who experienced MB were significantly older than those without bleeding (65.8 ± 12.3 vs. 61.7 ± 12.1 years, p = 0.041). Admission heart rate was also higher in the MB(+) group (92.5 ± 18.4 vs. 80.8 ± 13.2 bpm, p < 0.001). C-reactive protein (CRP) levels were higher in the MB(+) group (21.9 [7.2–45] vs. 9.0 [3.3–26.2] mg/L); the difference was statistically significant (p = 0.034). There were no significant differences in sex, blood pressure, hemoglobin level, creatinine level, lipid profile, or ejection fraction between patients with and without bleeding. Notably, the incidence of in-hospital MACE was markedly higher in the MB(+) group (40.5% vs. 8.1%, p < 0.001) ([Table 1]).
Abbreviations: CAD, coronary artery diseases; CRP, C-reactive protein; HDL, high-density lipoprotein; LDL, low-density lipoprotein; MACE, major adverse cardiovascular events.
Note: aContinuous variables are expressed as mean ± standard deviation and compared using the independent-samples t-test or Mann–Whitney U test, as appropriate. Categorical variables were compared using the chi-square or Fisher's exact test.
Comparison According to MACE Status
Compared to patients without MACE, those who experienced MACE were significantly older (68.3 ± 12.6 vs. 61.2 ± 11.8 years, p < 0.001), had higher heart rates at admission (86.0 ± 17.5 vs. 80.9 ± 13.2 bpm, p = 0.016), and higher white blood cell (WBC) counts (12.6 ± 4.9 vs. 10.9 ± 3.6 × 109/L, p < 0.001). Patients in the MACE(+) group also had significantly lower left ventricular ejection fraction (35.3 ± 11.0% vs. 47.5 ± 6.3%, p < 0.001), and elevated serum glucose (149 [114–228] vs. 128 [105–189] mg/dL, p = 0.015) and creatinine levels (1.00 [0.80–1.34] vs. 0.88 [0.74–1.05] mg/dL, p = 0.001). A history of stroke was significantly more frequent in the MACE(+) group (7.6% vs. 1.5%, p < 0.001). The occurrence of MB was substantially higher in patients who developed MACE (19.0% vs. 2.9%, p < 0.001) ([Table 2]).
Abbreviations: CAD, coronary artery diseases; HDL, high-density lipoprotein; LDL, low-density lipoprotein; MACE, major adverse cardiovascular events.
Note: aContinuous variables are presented as mean ± standard deviation and were compared using the independent-samples t-test or the Mann–Whitney U test, depending on data distribution. Categorical variables were compared using the chi-square test or Fisher's exact test, as appropriate.
Multivariate Predictors of In-Hospital MACE
In multivariate logistic regression analysis, MB emerged as the most powerful independent predictor of in-hospital MACE (adjusted OR: 12.43; 95% CI: 3.43–44.98; p < 0.001). In addition, a lower LVEF was independently associated with an increased risk of MACE (OR: 0.794; 95% CI: 0.747–0.843; p < 0.001), indicating a protective effect of preserved cardiac function. Advanced age (OR, 1.054; 95% CI, 1.013–1.096; p = 0.009) and elevated WBC count (OR, 1.125; 95% CI, 1.022–1.239; p = 0.016) were also significantly associated with MACE. Other variables, including serum creatinine level, glucose level, heart rate, and history of stroke, were not statistically significant in the final model ([Table 3]).
Abbreviation: MACE, major adverse cardiovascular events.
Note: aOdds ratios (OR) with 95% confidence intervals (CI) were calculated using multivariate logistic regression analysis.
Discussion
MB has emerged as a critical determinant of outcomes in ACS patients undergoing PCI. In this retrospective cohort study, we demonstrated that MB was significantly associated with an increased risk of in-hospital MACE. These findings reinforce the growing body of evidence that MB is not a benign complication, but rather a marker of heightened vulnerability to a broad range of adverse cardiovascular outcomes—including not only ischemic events such as myocardial infarction and stroke, but also non-ischemic complications like acute decompensated heart failure associated with severely reduced LVEF.[13]
Importantly, we included heart failure with LVEF <30% as part of the MACE definition. This approach was selected based on evidence that impaired left ventricular systolic function particularly below this threshold is strongly associated with in-hospital mortality and early adverse events following PCI. Supporting this, recent studies have highlighted the prognostic value of low LVEF in ACS patients both for ischemic and bleeding complications.[14] Therefore, inclusion of this endpoint enhances the clinical relevance of our composite outcome.
Our study revealed that the incidence of MB was 4.5%, and that these patients exhibited a significantly higher rate of in-hospital MACE than those without bleeding. Although MB was the strongest independent predictor of in-hospital MACE in our study, the wide confidence interval (OR: 12.43, 95% CI: 3.43–44.98) reflects the relatively low number of bleeding events (n = 37, 4.5%), which may have reduced the precision of our effect estimate. This limitation has also been reported in other registries, such as PARIS and TRACER, where MB events were infrequent but highly prognostic. These results are consistent with previous large-scale studies and registries, such as the PARIS registry and the TRACER trial, which reported that bleeding complications independently predicted subsequent myocardial infarction, stroke, and death.[15] [16] The observed association suggests that bleeding exerts pathophysiological effects that extend far beyond simple hemodynamic compromise.[17] [18]
Several interrelated biological mechanisms likely underlie the association between MB and cardiovascular events. First, MB results in acute hypovolemia, which leads to a reduced preload, decreased cardiac output, and hypotension. These hemodynamic changes compromise coronary perfusion, particularly in territories already jeopardized by ACS, potentially triggering myocardial ischemia, infarct extension, or arrhythmic events. Compensatory tachycardia, while attempting to preserve perfusion pressure, paradoxically increases myocardial oxygen demand, thus exacerbating the supply–demand mismatch. In patients with impaired systolic function, even modest drops in perfusion may precipitate decompensated heart failure or cardiogenic shock.[19] [20] [21] [22]
Second, MB often necessitates premature discontinuation of DAPT, particularly P2Y12 inhibitors. This withdrawal removes critical pharmacological protection against platelet aggregation during the early phase post-PCI when the endothelial healing of stents is incomplete. Studies have shown that early cessation of DAPT, particularly within the first 30 days, significantly increases the incidence of stent thrombosis and recurrent myocardial infarction.[23] [24] [25] [26] Although the interruption of DAPT is widely recognized as a mechanism contributing to adverse cardiovascular events following MB, our study did not capture data on antiplatelet therapy discontinuation. Therefore, this proposed pathway should be interpreted cautiously in our context.
Third, MB initiates a systemic inflammatory response characterized by the release of proinflammatory cytokines such as interleukin-6 (IL-6), tumor necrosis factor-alpha (TNF-α), and CRP. These mediators promote leukocyte adhesion, endothelial activation, and increased oxidative stress, all of which contribute to plaque destabilization and a prothrombotic vascular environment.[27] [28] In our study, a trend toward elevated CRP levels in patients with MB supported the role of inflammation as a bridge between bleeding and adverse ischemic outcomes.
Furthermore, hemorrhage induces a hypercoagulable state. Physiological responses aimed at halting bleeding, such as platelet activation and thrombin generation, may inadvertently trigger arterial thrombosis.[29] The vascular endothelium, which normally maintains an antithrombotic balance through nitric oxide (NO) and prostacyclin release, is dysfunctional in the setting of systemic inflammation and hemodynamic stress. Reduced endothelial nitric oxide synthase (eNOS) activity impairs vasodilation and enhances platelet adhesion.[30] Circulating microparticles released in response to vascular injury further amplify coagulation cascades. This pathophysiological milieu creates a window of vulnerability wherein both bleeding and thrombosis can coexist and reinforce one another.
Recent studies, such as that by Yoshii et al, have highlighted the prognostic significance of endothelial dysfunction in patients with ACS and its association with both bleeding risk and cardiovascular death.[31] These data support the hypothesis that bleeding is not merely a complication but also a systemic event that destabilizes vascular integrity and precipitates further cardiovascular deterioration.
When comparing our findings with those in the literature, several similarities and differences emerge. Consistent with previous studies, we found that older age, elevated heart rate at admission, lower LVEF, and higher WBC count were associated with worse outcomes.[5] [32] [33] [34] [35] Elderly patients are particularly vulnerable owing to increased vascular fragility, comorbidities, and diminished compensatory mechanisms. Elevated WBC counts and inflammatory markers not only may reflect systemic stress or occult infection but also likely contribute directly to plaque instability and thrombotic potential.[6]
Our study contributes to the growing recognition of the “risk paradox” phenomenon where patients at high bleeding risk simultaneously harbor high ischemic risk.[36] This dual vulnerability complicates therapeutic decision-making, as intensifying antithrombotic therapy reduces ischemic events but increases bleeding, whereas de-escalation strategies may prevent bleeding, but leave patients exposed to thrombosis. Recent trials, such as MASTER DAPT, have suggested that shorter durations of DAPT may offer a safer balance in select high-risk populations, although careful patient selection remains crucial.[37] [38]
In recent years, platelet function testing (PFT) and biomarker-guided strategies have emerged as valuable tools in tailoring antiplatelet therapy, particularly for patients at increased risk of bleeding.[39] [40] Trials such as TROPICAL-ACS and ARCTIC demonstrated that PFT-guided de-escalation starting with a potent P2Y12 inhibitor like prasugrel or ticagrelor, followed by a switch to clopidogrel based on platelet reactivity can safely reduce bleeding events without increasing ischemic risk.[41] [42] Capranzano and Angiolillo further emphasized that such de-escalation approaches may be particularly beneficial in subgroups such as diabetics, who often exhibit enhanced platelet reactivity.[43] Moreover, current guidelines support individualized DAPT strategies, especially in high bleeding risk populations, highlighting the clinical relevance of incorporating PFT or biomarkers into antithrombotic decision-making. These tools allow clinicians to better balance ischemic and hemorrhagic risks and may improve outcomes in ACS patients following PCI. Future studies may further refine patient selection for PFT-guided strategies and validate their impact on long-term cardiovascular outcomes.
These findings emphasize the need for early identification of bleeding-prone individuals and implementation of individualized treatment strategies. Practical measures include the preferential use of radial arterial access during PCI to minimize access-site bleeding, cautious dosing of antithrombotic agents based on body weight and renal function, and consideration of abbreviated DAPT courses in patients deemed to be at high bleeding risk. In addition, the use of validated bleeding risk scores and endothelial function markers may provide further refinement for clinical risk stratification.
Study Limitations
Our study has some limitations. First, given the observational nature of our study, the associations identified—while statistically significant—do not establish causality and should be interpreted as correlational findings rather than definitive cause–effect relationships. Second, although all bleeding events were classified using the BARC definitions, adjudication was not centralized, which may have led to some degree of misclassification. Third, the lack of post-discharge follow-up data limits our understanding of the long-term implications. Moreover, we did not collect data on DAPT discontinuation following bleeding events, which limits our ability to directly assess this mechanism as a mediator of in-hospital MACE. Additionally, the dual role of LVEF <30% both as a MACE component and an independent predictor could introduce collinearity. However, multicollinearity diagnostics using variance inflation factor (VIF) revealed acceptable levels (VIF <2). Still, the possibility of statistical overlap cannot be fully excluded and warrants further exploration in future prospective cohorts.
Conclusion
In conclusion, MB was strongly and independently associated with an increased risk of in-hospital MACE in patients with ACS undergoing PCI. Multiple interconnected biological mechanisms, including hemodynamic instability, interruption of antithrombotic therapy, systemic inflammation, platelet activation, endothelial dysfunction, and impaired cardiac reserve contribute to this relationship. Recognizing bleeding as a sentinel prognostic event and adopting individualized physiology-informed management strategies are essential steps toward improving early and long-term outcomes in this vulnerable population.
Conflict of Interest
The authors declare that they have no conflict of interest.
-
References
- 1 O'Gara PT, Kushner FG, Ascheim DD. et al. 2013 ACCF/AHA guideline for the management of ST-elevation myocardial infarction. J Am Coll Cardiol 2013; 61 (04) e78-e140
- 2 Mehran R, Rao SV, Bhatt DL. et al. Standardized bleeding definitions for cardiovascular clinical trials: a consensus report from the Bleeding Academic Research Consortium. Circulation 2011; 123 (23) 2736-2747
- 3 Vavalle JP, Rao SV. Impact of bleeding complications on outcomes after PCI. Am J Cardiol 2009; 103 (09) 1204-1209
- 4 Kwok CS, Sirker A, Rawat S. et al. Major bleeding after PCI and mortality. Int J Cardiol 2015; 201: 77-84
- 5 Sun Y, Zhang H, Liu L. et al. In-hospital major bleeding and cardiovascular events in Chinese ACS patients. Thromb Res 2022; 214: 37-43
- 6 Campbell PG, Simon DI. Bleeding events and inflammatory markers. Am J Cardiol 2011; 108 (08) 1105-1111
- 7 Yeh RW, Sidney S, Chandra M, Sorel M, Selby JV, Go AS. Complications and mortality following PCI. Circulation 2012; 125 (09) 1234-1241
- 8 Généreux P, Giustino G, Witzenbichler B. et al. Relation between coronary calcium and bleeding after PCI. JACC Cardiovasc Interv 2014; 7 (11) 1400-1409
- 9 Choi SS, Sergie Z, Mehran R. Impact of in-hospital major bleeding on outcomes in acute coronary syndromes. Curr Opin Cardiol 2012; 27 (06) 669-674
- 10 Mehran R, Pocock S, Nikolsky E. et al. Impact of bleeding on mortality after PCI. Lancet 2012; 379 (9829): 1703-1711
- 11 Byrne RA, Rossello X, Coughlan JJ. et al; ESC Scientific Document Group. 2023 ESC Guidelines for the management of acute coronary syndromes. Eur Heart J 2023; 44 (38) 3720-3826
- 12 Matsuoka Y, Sotomi Y, Hikoso S. et al. The prognostic impact of in-hospital major bleeding and recurrence of myocardial infarction during acute phase after percutaneous coronary intervention for acute myocardial infarction. J Atheroscler Thromb 2024; 31 (02) 158-170
- 13 Mehran R, Baber U, Steg PG. et al. Cessation of dual antiplatelet treatment and cardiac events after PCI. N Engl J Med 2013; 368 (22) 2086-2097
- 14 Iyer M, Shah R, Zheng W. et al. Aetiology and predictors of major bleeding events in patients with heart failure with reduced ejection fraction undergoing percutaneous coronary intervention. Open Heart 2024; 11 (01) e002572
- 15 Sorrentino S, Giustino G, Baber U. et al. Dual antiplatelet therapy cessation and adverse events after drug-eluting stent implantation in patients at high risk for atherothrombosis (from the PARIS registry). Am J Cardiol 2018; 122 (10) 1638-1646
- 16 Valgimigli M, Costa F, Lokhnygina Y. et al. Trade-off of myocardial infarction vs. bleeding types on mortality after acute coronary syndrome: lessons from the Thrombin Receptor Antagonist for Clinical Event Reduction in Acute Coronary Syndrome (TRACER) randomized trial. Eur Heart J 2017; 38 (11) 804-810
- 17 Chhatriwalla AK, Amin AP, Kennedy KF. et al; National Cardiovascular Data Registry. Association between bleeding events and in-hospital mortality after percutaneous coronary intervention. JAMA 2013; 309 (10) 1022-1029 [published correction appears in JAMA. 2013 Aug 14;310(6):647]
- 18 Fu A, Barry Q, Boudreau R. et al. Outcomes of patients with high bleeding risks characteristics presenting with acute coronary syndrome undergoing percutaneous coronary intervention. Eur Heart J 2021; 42 (Suppl. 01) ehab724.1428
- 19 Freemantle N, Calvert M, Wood J, Eastaugh J, Griffin C. Composite outcomes in randomized trials: greater precision but with greater uncertainty?. JAMA 2003; 289 (19) 2554-2559
- 20 Armstrong PW, Westerhout CM, Van de Werf F. et al. Refining clinical trial composite outcomes: an application to the Assessment of the Safety and Efficacy of a New Thrombolytic-3 (ASSENT-3) trial. Am Heart J 2011; 161 (05) 848-854
- 21 Pocock SJ, Ariti CA, Collier TJ, Wang D. The win ratio: a new approach to the analysis of composite endpoints in clinical trials based on clinical priorities. Eur Heart J 2012; 33 (02) 176-182
- 22 Bakal JA, Roe MT, Ohman EM. et al. Applying novel methods to assess clinical outcomes: insights from the TRILOGY ACS trial. Eur Heart J 2015; 36 (06) 385-92a
- 23 Cenko E, Manfrini O, Bugiardini R. Net adverse clinical events with P2Y12 inhibitor therapy in older patients after percutaneous coronary interventions. Atherosclerosis 2024; 390: 117434
- 24 Redfors B, Kirtane AJ, Liu M. et al. Dual antiplatelet therapy discontinuation, platelet reactivity, and adverse outcomes after successful percutaneous coronary intervention. JACC Cardiovasc Interv 2022; 15 (08) 797-806 [published correction appears in JACC Cardiovasc Interv. 2022 Oct 10;15(19):2001]
- 25 Baber U, Dangas G, Chandrasekhar J. et al. Ticagrelor with or without aspirin after PCI. N Engl J Med 2019; 381 (21) 2032-2042
- 26 Kwok CS, Sirker A, Rawat S. et al. Influence of major bleeding after percutaneous coronary intervention on mortality and cardiovascular outcomes. Int J Cardiol 2015; 201: 77-84
- 27 Vinayak M, Cao D, Tanner R. et al. Impact of bleeding risk and inflammation on cardiovascular outcomes after percutaneous coronary intervention. JACC Cardiovasc Interv 2024; 17 (03) 345-355
- 28 Tuomisto K, Jousilahti P, Sundvall J, Pajunen P, Salomaa V. C-reactive protein, interleukin-6 and tumor necrosis factor alpha as predictors of incident coronary and cardiovascular events and total mortality. A population-based, prospective study. Thromb Haemost 2006; 95 (03) 511-518
- 29 Kamphuisen PW, Rosendaal FR, Büller HR. Hemostatic abnormalities and arterial thrombosis. Semin Thromb Hemost 2009; 35 (05) 449-450
- 30 Brenner B, Lisman T. Hemostasis and thrombosis in extreme physiological and pathological conditions. Semin Thromb Hemost 2018; 44 (07) 615-616
- 31 Yoshii S, Nishikawa H, Watanabe K. et al. Endothelial dysfunction predicts bleeding and cardiovascular death in patients with acute coronary syndrome. J Cardiol 2023; 81 (02) 122-128
- 32 Campbell CL, Steinhubl SR, Hooper WC. et al. Bleeding events are associated with an increase in markers of inflammation in acute coronary syndromes: an ACUITY trial substudy. J Thromb Thrombolysis 2011; 31 (02) 139-145
- 33 Yeh RW, Sidney S, Chandra M. et al. Complications and mortality following percutaneous coronary intervention in contemporary practice: results from the NCDR. Circulation 2012; 125 (09) 1234-1241
- 34 Huang L, Zhao Y, Li J. et al. In-hospital major adverse cardiovascular events after primary PCI for STEMI: a real-world multicenter analysis. BMC Cardiovasc Disord 2023; 23: 235
- 35 Généreux P, Witzenbichler B, Weisz G. et al. Incidence, predictors, and impact of bleeding complications after PCI. JACC Cardiovasc Interv 2014; 7 (11) 1400-1409
- 36 Yamamoto K, Natsuaki M, Morimoto T. et al; CREDO-Kyoto PCI/CABG Registry Cohort-3 investigators. Ischemic and bleeding events after first major bleeding event in patients undergoing coronary stent implantation. Am J Cardiol 2022; 162: 13-23
- 37 Valgimigli M, Smits PC, Frigoli E. et al; MASTER DAPT Investigators. Duration of antiplatelet therapy after complex percutaneous coronary intervention in patients at high bleeding risk: a MASTER DAPT trial sub-analysis. Eur Heart J 2022; 43 (33) 3100-3114
- 38 Valgimigli M, Frigoli E, Heg D. et al; MASTER DAPT Investigators. Dual antiplatelet therapy after PCI in patients at high bleeding risk. N Engl J Med 2021; 385 (18) 1643-1655
- 39 Nissen PH, Pedersen OB. Unlocking the potential of microRNA expression: biomarkers for platelet reactivity and coronary artery disease. Semin Thromb Hemost 2025; . Epub ahead of print
- 40 Zhou M, Hou P, Liang Y. et al. Comparison of platelet function tests for long-term cardiovascular events after percutaneous coronary interventions. Semin Thromb Hemost 2025; . Epub ahead of print
- 41 Kang J, Rizas KD, Park KW. et al. Dual antiplatelet therapy de-escalation in acute coronary syndrome: an individual patient meta-analysis. Eur Heart J 2023; 44 (15) 1360-1370
- 42 Lattuca B, Silvain J, Yan Y. et al. Reasons for the failure of platelet function testing to adjust antiplatelet therapy: pharmacodynamic insights from the ARCTIC study. Circ Cardiovasc Interv 2019; 12 (11) e007749
- 43 Capranzano P, Angiolillo DJ. De-escalation of oral P2Y12 inhibitors guided by platelet function testing in ACS patients undergoing PCI: impact of diabetes mellitus. EuroIntervention 2019; 15 (06) e486-e489
Address for correspondence
Publication History
Received: 01 June 2025
Accepted: 22 July 2025
Article published online:
14 August 2025
© 2025. Thieme. All rights reserved.
Georg Thieme Verlag KG
Oswald-Hesse-Straße 50, 70469 Stuttgart, Germany
-
References
- 1 O'Gara PT, Kushner FG, Ascheim DD. et al. 2013 ACCF/AHA guideline for the management of ST-elevation myocardial infarction. J Am Coll Cardiol 2013; 61 (04) e78-e140
- 2 Mehran R, Rao SV, Bhatt DL. et al. Standardized bleeding definitions for cardiovascular clinical trials: a consensus report from the Bleeding Academic Research Consortium. Circulation 2011; 123 (23) 2736-2747
- 3 Vavalle JP, Rao SV. Impact of bleeding complications on outcomes after PCI. Am J Cardiol 2009; 103 (09) 1204-1209
- 4 Kwok CS, Sirker A, Rawat S. et al. Major bleeding after PCI and mortality. Int J Cardiol 2015; 201: 77-84
- 5 Sun Y, Zhang H, Liu L. et al. In-hospital major bleeding and cardiovascular events in Chinese ACS patients. Thromb Res 2022; 214: 37-43
- 6 Campbell PG, Simon DI. Bleeding events and inflammatory markers. Am J Cardiol 2011; 108 (08) 1105-1111
- 7 Yeh RW, Sidney S, Chandra M, Sorel M, Selby JV, Go AS. Complications and mortality following PCI. Circulation 2012; 125 (09) 1234-1241
- 8 Généreux P, Giustino G, Witzenbichler B. et al. Relation between coronary calcium and bleeding after PCI. JACC Cardiovasc Interv 2014; 7 (11) 1400-1409
- 9 Choi SS, Sergie Z, Mehran R. Impact of in-hospital major bleeding on outcomes in acute coronary syndromes. Curr Opin Cardiol 2012; 27 (06) 669-674
- 10 Mehran R, Pocock S, Nikolsky E. et al. Impact of bleeding on mortality after PCI. Lancet 2012; 379 (9829): 1703-1711
- 11 Byrne RA, Rossello X, Coughlan JJ. et al; ESC Scientific Document Group. 2023 ESC Guidelines for the management of acute coronary syndromes. Eur Heart J 2023; 44 (38) 3720-3826
- 12 Matsuoka Y, Sotomi Y, Hikoso S. et al. The prognostic impact of in-hospital major bleeding and recurrence of myocardial infarction during acute phase after percutaneous coronary intervention for acute myocardial infarction. J Atheroscler Thromb 2024; 31 (02) 158-170
- 13 Mehran R, Baber U, Steg PG. et al. Cessation of dual antiplatelet treatment and cardiac events after PCI. N Engl J Med 2013; 368 (22) 2086-2097
- 14 Iyer M, Shah R, Zheng W. et al. Aetiology and predictors of major bleeding events in patients with heart failure with reduced ejection fraction undergoing percutaneous coronary intervention. Open Heart 2024; 11 (01) e002572
- 15 Sorrentino S, Giustino G, Baber U. et al. Dual antiplatelet therapy cessation and adverse events after drug-eluting stent implantation in patients at high risk for atherothrombosis (from the PARIS registry). Am J Cardiol 2018; 122 (10) 1638-1646
- 16 Valgimigli M, Costa F, Lokhnygina Y. et al. Trade-off of myocardial infarction vs. bleeding types on mortality after acute coronary syndrome: lessons from the Thrombin Receptor Antagonist for Clinical Event Reduction in Acute Coronary Syndrome (TRACER) randomized trial. Eur Heart J 2017; 38 (11) 804-810
- 17 Chhatriwalla AK, Amin AP, Kennedy KF. et al; National Cardiovascular Data Registry. Association between bleeding events and in-hospital mortality after percutaneous coronary intervention. JAMA 2013; 309 (10) 1022-1029 [published correction appears in JAMA. 2013 Aug 14;310(6):647]
- 18 Fu A, Barry Q, Boudreau R. et al. Outcomes of patients with high bleeding risks characteristics presenting with acute coronary syndrome undergoing percutaneous coronary intervention. Eur Heart J 2021; 42 (Suppl. 01) ehab724.1428
- 19 Freemantle N, Calvert M, Wood J, Eastaugh J, Griffin C. Composite outcomes in randomized trials: greater precision but with greater uncertainty?. JAMA 2003; 289 (19) 2554-2559
- 20 Armstrong PW, Westerhout CM, Van de Werf F. et al. Refining clinical trial composite outcomes: an application to the Assessment of the Safety and Efficacy of a New Thrombolytic-3 (ASSENT-3) trial. Am Heart J 2011; 161 (05) 848-854
- 21 Pocock SJ, Ariti CA, Collier TJ, Wang D. The win ratio: a new approach to the analysis of composite endpoints in clinical trials based on clinical priorities. Eur Heart J 2012; 33 (02) 176-182
- 22 Bakal JA, Roe MT, Ohman EM. et al. Applying novel methods to assess clinical outcomes: insights from the TRILOGY ACS trial. Eur Heart J 2015; 36 (06) 385-92a
- 23 Cenko E, Manfrini O, Bugiardini R. Net adverse clinical events with P2Y12 inhibitor therapy in older patients after percutaneous coronary interventions. Atherosclerosis 2024; 390: 117434
- 24 Redfors B, Kirtane AJ, Liu M. et al. Dual antiplatelet therapy discontinuation, platelet reactivity, and adverse outcomes after successful percutaneous coronary intervention. JACC Cardiovasc Interv 2022; 15 (08) 797-806 [published correction appears in JACC Cardiovasc Interv. 2022 Oct 10;15(19):2001]
- 25 Baber U, Dangas G, Chandrasekhar J. et al. Ticagrelor with or without aspirin after PCI. N Engl J Med 2019; 381 (21) 2032-2042
- 26 Kwok CS, Sirker A, Rawat S. et al. Influence of major bleeding after percutaneous coronary intervention on mortality and cardiovascular outcomes. Int J Cardiol 2015; 201: 77-84
- 27 Vinayak M, Cao D, Tanner R. et al. Impact of bleeding risk and inflammation on cardiovascular outcomes after percutaneous coronary intervention. JACC Cardiovasc Interv 2024; 17 (03) 345-355
- 28 Tuomisto K, Jousilahti P, Sundvall J, Pajunen P, Salomaa V. C-reactive protein, interleukin-6 and tumor necrosis factor alpha as predictors of incident coronary and cardiovascular events and total mortality. A population-based, prospective study. Thromb Haemost 2006; 95 (03) 511-518
- 29 Kamphuisen PW, Rosendaal FR, Büller HR. Hemostatic abnormalities and arterial thrombosis. Semin Thromb Hemost 2009; 35 (05) 449-450
- 30 Brenner B, Lisman T. Hemostasis and thrombosis in extreme physiological and pathological conditions. Semin Thromb Hemost 2018; 44 (07) 615-616
- 31 Yoshii S, Nishikawa H, Watanabe K. et al. Endothelial dysfunction predicts bleeding and cardiovascular death in patients with acute coronary syndrome. J Cardiol 2023; 81 (02) 122-128
- 32 Campbell CL, Steinhubl SR, Hooper WC. et al. Bleeding events are associated with an increase in markers of inflammation in acute coronary syndromes: an ACUITY trial substudy. J Thromb Thrombolysis 2011; 31 (02) 139-145
- 33 Yeh RW, Sidney S, Chandra M. et al. Complications and mortality following percutaneous coronary intervention in contemporary practice: results from the NCDR. Circulation 2012; 125 (09) 1234-1241
- 34 Huang L, Zhao Y, Li J. et al. In-hospital major adverse cardiovascular events after primary PCI for STEMI: a real-world multicenter analysis. BMC Cardiovasc Disord 2023; 23: 235
- 35 Généreux P, Witzenbichler B, Weisz G. et al. Incidence, predictors, and impact of bleeding complications after PCI. JACC Cardiovasc Interv 2014; 7 (11) 1400-1409
- 36 Yamamoto K, Natsuaki M, Morimoto T. et al; CREDO-Kyoto PCI/CABG Registry Cohort-3 investigators. Ischemic and bleeding events after first major bleeding event in patients undergoing coronary stent implantation. Am J Cardiol 2022; 162: 13-23
- 37 Valgimigli M, Smits PC, Frigoli E. et al; MASTER DAPT Investigators. Duration of antiplatelet therapy after complex percutaneous coronary intervention in patients at high bleeding risk: a MASTER DAPT trial sub-analysis. Eur Heart J 2022; 43 (33) 3100-3114
- 38 Valgimigli M, Frigoli E, Heg D. et al; MASTER DAPT Investigators. Dual antiplatelet therapy after PCI in patients at high bleeding risk. N Engl J Med 2021; 385 (18) 1643-1655
- 39 Nissen PH, Pedersen OB. Unlocking the potential of microRNA expression: biomarkers for platelet reactivity and coronary artery disease. Semin Thromb Hemost 2025; . Epub ahead of print
- 40 Zhou M, Hou P, Liang Y. et al. Comparison of platelet function tests for long-term cardiovascular events after percutaneous coronary interventions. Semin Thromb Hemost 2025; . Epub ahead of print
- 41 Kang J, Rizas KD, Park KW. et al. Dual antiplatelet therapy de-escalation in acute coronary syndrome: an individual patient meta-analysis. Eur Heart J 2023; 44 (15) 1360-1370
- 42 Lattuca B, Silvain J, Yan Y. et al. Reasons for the failure of platelet function testing to adjust antiplatelet therapy: pharmacodynamic insights from the ARCTIC study. Circ Cardiovasc Interv 2019; 12 (11) e007749
- 43 Capranzano P, Angiolillo DJ. De-escalation of oral P2Y12 inhibitors guided by platelet function testing in ACS patients undergoing PCI: impact of diabetes mellitus. EuroIntervention 2019; 15 (06) e486-e489