

Subscribe to RSS
DOI: 10.1055/a-2802-3753
Clinical Heterogeneity and Prognostic Impact of Disseminated Intravascular Coagulation in Critically Ill Patients: A Large-Scale Retrospective Study
Authors

Abstract
Background
Disseminated intravascular coagulation (DIC) is a serious condition characterized by systemic coagulation activation leading to thrombotic and hemorrhagic complications. Although the characteristics of DIC vary depending on the underlying cause, studies directly comparing coagulation/fibrinolysis laboratory findings across a wide range of underlying diseases are limited.
Objective
We investigated the characteristics of coagulation/fibrinolysis laboratory results, the frequency of DIC, and the impact of DIC on patient prognosis across various underlying diseases in a critical care setting.
Methods
This was a single-center retrospective observational study of 1,665 critically ill patients admitted between January 1, 2010, and December 21, 2022. Patients were categorized based on underlying diseases, which included out-of-hospital cardiac arrest, sepsis, trauma, burn, and heat stroke. We retrospectively collected data on background, DIC scores, laboratory results, and in-hospital mortality rates of patients.
Results
Significant heterogeneity in coagulation/fibrinolysis laboratory findings was observed, with all findings differing based on the underlying disease (p < 0.001). For example, patients with trauma-associated DIC showed significantly elevated D-dimer and fibrin/fibrinogen degradation product levels, while those with burn-associated DIC tended to have high platelet counts and a rapid decrease in antithrombin activity following admission. Among all underlying diseases, the development of DIC was associated with an increase in in-hospital mortality. This association was particularly strong in patients with trauma or burns.
Conclusion
The coagulation/fibrinolysis laboratory findings, along with the clinical trajectory of DIC, exhibit remarkable heterogeneity depending on the precipitating cause. Development of DIC in patients with burn or trauma is strongly associated with increased in-hospital mortality.
Introduction
Disseminated intravascular coagulation (DIC) is a complex pathophysiological process characterized by the systemic activation of coagulation, leading to both thrombotic and hemorrhagic complications. It is associated with various underlying conditions, where it significantly increases mortality.[1] [2] [3] [4] [5] Based on the underlying conditions, DIC manifests differently, with two main identified phenotypes: the thrombotic and fibrinolytic phenotypes.[4] [5] [6] [7]
Previous studies evaluated the variability of coagulation/fibrinolysis laboratory parameters in patients with DIC owing to underlying diseases such as sepsis, solid tumors, and hematologic malignancies and found that the balance between coagulation and fibrinolytic activation differed between sepsis and hematologic malignancy.[8] [9] [10] Furthermore, antithrombin (AT) activity levels were lower, while fibrinogen levels were higher in patients with septic DIC than in those with DIC caused by other underlying diseases. Recently, using the Japanese Diagnosis Procedure Combination database, a nationwide administrative database that integrates patient diagnosis and procedure data for hospital reimbursement, it was reported that the clinical symptoms of bleeding and organ failure in patients with DIC may not be associated with the different phenotypes or underlying disorders associated with DIC.[11] However, the laboratory results were not evaluated in this study. Studies examining the characteristics of coagulation/fibrinolysis laboratory results associated with specific underlying diseases of DIC are limited.
Therefore, in the present study, we investigated the characteristics of coagulation/fibrinolysis laboratory results in patients with DIC, the frequency of DIC, and the impact of DIC on patient prognosis across various underlying diseases in critical care settings.
Materials and Methods
Study Design and Patients
This study was approved by the Institutional Review Board of the Ethics Committee of Hokkaido University Hospital (no. 024-0247, approved November 12, 2024) and was conducted in accordance with the Declaration of Helsinki. The need for written informed consent was waived because of the retrospective design of the study.
This single-center, retrospective observational study was performed in the emergency and critical care center at Hokkaido University Hospital, a tertiary emergency institution. As a tertiary emergency institute, the center received patients with a wide range of severe conditions. Our study thoroughly reviewed all patients admitted to our center between January 1, 2010, and December 21, 2022, and included those with underlying disease, including cardiogenic out-of-hospital cardiac arrest (OHCA), severe sepsis,[12] [13] severe trauma with Injury Severity Score[14] ≥ 9, severe burn, accidental hypothermia, heat stroke, cerebral hemorrhage, and subarachnoid hemorrhage. These underlying diseases were selected due to their relatively high admission numbers at our institute. The patients were divided into groups based on their underlying disease.
We retrospectively collected the patient background information, including age, sex, DIC score based on DIC diagnostic criteria established by the Japanese Association for Acute Medicine,[15] Systemic Inflammatory Response Syndrome (SIRS) score,[12] laboratory results, and in-hospital mortality, based on electronic medical records.
Primary and Secondary Outcomes
The primary outcome of the study was in-hospital mortality, and secondary outcomes were laboratory heterogeneity and DIC frequency.
Statistical Analysis
All data were presented as numbers (percentages) or medians (interquartile ranges), as appropriate. Continuous variables were compared among groups using the Kruskal–Wallis test. To evaluate the differences in laboratory results among groups, standardized mean differences were calculated. Logistic regression analysis was used to evaluate the influence of DIC score and concomitant DIC on mortality. To account for potential separation issues and to reduce small-sample bias in the logistic regression models to evaluate the influence of concomitant DIC on mortality, we employed Firth's penalized likelihood approach. Missing variable data on day 2 or 3 were imputed using the last observation carried forward method. All statistical analyses and calculations were performed using SPSS software (version 26; SPSS Inc., Chicago, Illinois, United States).
Results
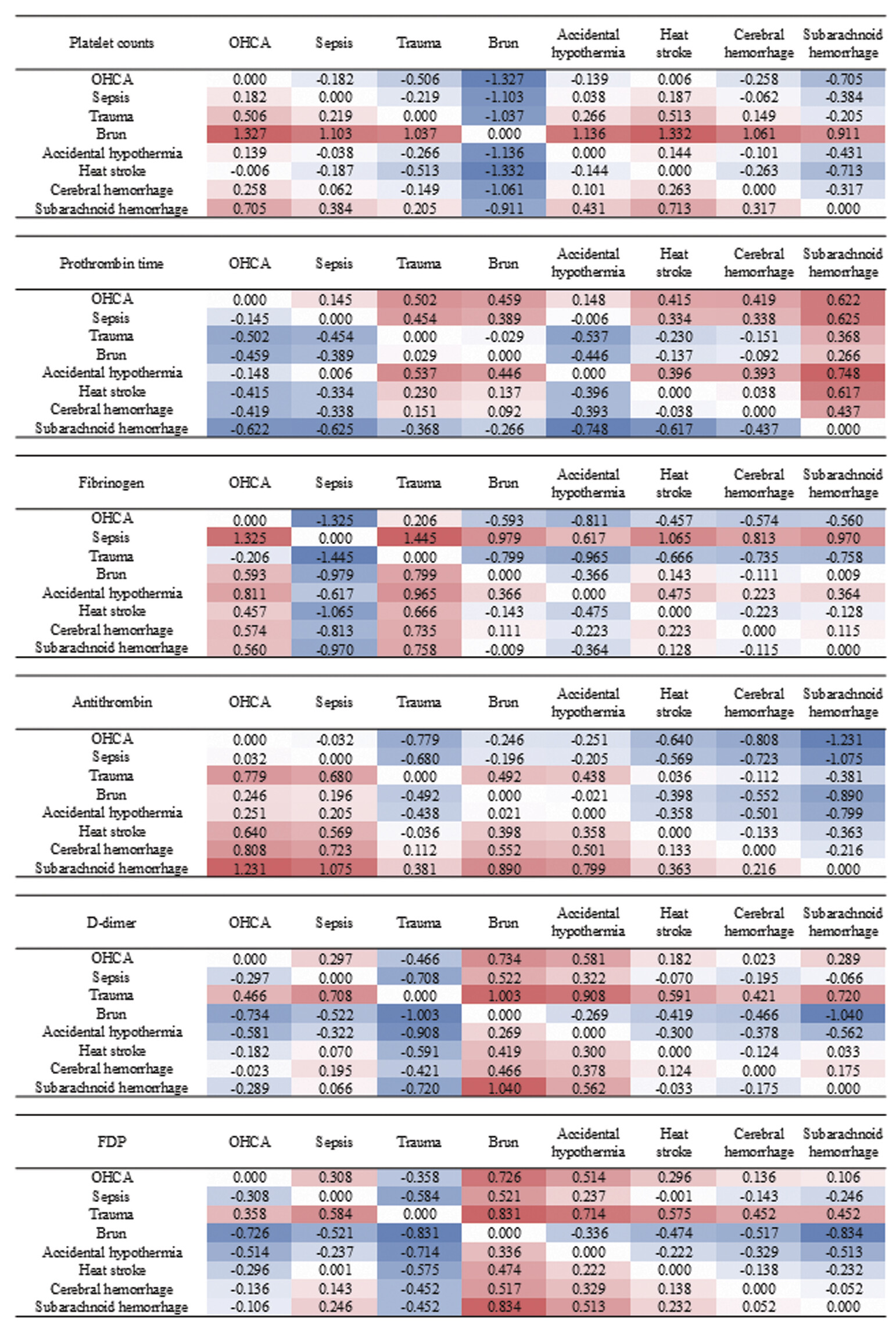
During the study period, 1,726 patients with targeted underlying diseases were admitted. Because some variables used to calculate the DIC scores on day 1 (on arrival at the emergency department [ED]) were missing, 61 patients were excluded. Finally, 1,665 patients were included in this study. [Table 1] summarizes the characteristics of patients with and without DIC upon arrival at the ED. Most underlying diseases in the patients were OHCA, sepsis, and trauma. Seventy-five percent of patients were complicated by DIC upon arrival. [Table 2] presents the characteristics of the patients with DIC on arrival at the ED in each group. Box plots of coagulation/fibrinolysis laboratory results in patients with DIC upon arrival at the ED are presented in [Fig. 1]. Even under the same conditions, patients who presented with DIC upon arrival at the ED exhibited different results of all coagulation/fibrinolysis tests depending on the underlying disease (p < 0.001, Kruskal–Wallis test). [Fig. 2] presents the standardized mean differences in coagulation/fibrinolysis laboratory results between the two groups in patients with DIC upon arrival at the ED. Platelet counts in patients with burn-associated DIC were higher than those in other patients. Prothrombin time was slightly prolonged in patients with DIC associated with OHCA, sepsis, and accidental hypothermia compared with patients in other groups. Fibrinogen levels were higher in patients with DIC associated with sepsis, whereas AT activity was lower in patients with DIC associated with OHCA, sepsis, burn, and accidental hypothermia than in other patients. D-dimer and FDP levels were higher in patients with trauma-associated DIC, and in contrast, lower levels were observed in burn- and accidental hypothermia-associated DIC patients compared with those in other patients.
Abbreviations: ALT, alanine aminotransferase; APTT, activated partial thromboplastin time; AST, aspartate aminotransferase; DIC, disseminated intravascular coagulation; FDP, fibrin/fibrinogen degradation products; LDH, lactate dehydrogenase; OHCA, out-of-hospital cardiac arrest; SIRS, systemic inflammatory response syndrome; γ-GTP, γ-glutamyl transpeptidase.
Abbreviations: APTT, activated partial thromboplastin time; DIC, disseminated intravascular coagulation; FDP, fibrin/fibrinogen degradation products; OHCA, out-of-hospital cardiac arrest; SIRS, systemic inflammatory response syndrome.

[Fig. 3] presents the changes in coagulation/fibrinolysis laboratory results during the first 3 days after admission in patients with DIC upon arrival at the ED. The changes in the coagulation/fibrinolysis laboratory parameters varied according to the underlying diseases. In patients with burn-associated DIC, platelet count and AT activity rapidly decreased. Platelet counts rapidly decreased, and prothrombin time was prolonged after admission, in patients with DIC associated with heat stroke. In patients with DIC associated with sepsis, fibrinogen levels were high upon arrival at the ED and were further elevated, whereas in patients with trauma-associated DIC, D-dimer and FDP levels were remarkably high upon arrival, which rapidly decreased thereafter (statistical evaluations were not performed for [Fig. 3]).

[Table 3] shows the association between DIC upon arrival at the ED and in-hospital mortality for each underlying disease. For all underlying diseases, the mortality rate increased with increasing DIC score. Among the patients with trauma and heat stroke, no deaths occurred in those without DIC on arrival at the ED. [Fig. 4] presents the changes in the frequency of DIC in each underlying disease during the first 3 days after admission. In patients with DIC associated with trauma and accidental hypothermia, the frequency of DIC decreased rapidly (statistical evaluations were not performed for [Fig. 4]). [Table 4] shows the association between changes in DIC from day 1 to 3 and in-hospital mortality in each underlying disease. Irrespective of the underlying disease, patients in whom DIC persisted from day 1, on arrival at ED, to day 3, exhibited high in-hospital mortality rates. However, even if DIC was present on day 1, an improvement in DIC was associated with a lower mortality rate.
Abbreviations: DIC, disseminated intravascular coagulation; OHCA, out-of-hospital cardiac arrest.
Note: The odds ratio was not adjusted for any covariates.

Abbreviations: DIC, disseminated intravascular coagulation; OHCA, out-of-hospital cardiac arrest.
Note: The odds ratio was not adjusted for any covariates.
Discussion
In this retrospective study of 1,665 critically ill patients, we examined how DIC characteristics and outcomes vary across a broad range of underlying conditions. Our findings highlight the remarkable heterogeneity in the laboratory findings and clinical trajectory of DIC depending on the precipitating cause. Patients with burn-associated DIC showed higher platelet counts upon arrival at the ED than those with DIC associated with other underlying diseases. Patients with DIC associated with OHCA, sepsis, and accidental hypothermia exhibited prolonged prothrombin time, whereas levels of fibrinogen were higher in patients with DIC associated with sepsis compared to those in other patients. AT activity in patients with DIC associated with OHCA, sepsis, burn, and accidental hypothermia was lower than that in other patients. D-dimer and FDP levels in patients with DIC due to trauma were higher than in other patients, while in patients with DIC associated with burn and accidental hypothermia were lower than those with other diseases. Development of DIC upon arrival at the ED in patients with burn and trauma was strongly associated with in-hospital mortality compared with other underlying diseases. Regardless of the underlying disease, in patients with persistent DIC, the in-hospital mortality rates were higher compared with those of other patients.
Across various underlying diseases, the development of DIC is associated with increased mortality and adverse events. Moreover, the incidence of DIC increases with the severity of the underlying disease.[1] [2] [3] [4] [5] In the present study, the development of DIC upon arrival at the ED and its persistence were associated with increased mortality for all underlying diseases, provided the development of DIC was associated with the severity of underlying diseases. However, the effects of DIC on mortality differed markedly. In burn and trauma, DIC was associated with markedly increased mortality, although the frequency of DIC was low in patients with burn in our cohort. However, sepsis-associated DIC, despite being the most investigated DIC among various underlying diseases, was associated with only a slight increase in mortality. In our institute, sepsis-associated DIC is frequently treated with AT concentrates and/or recombinant thrombomodulin. These anti-DIC treatments might mitigate the effects of DIC on mortality in patients with sepsis. Although the development of DIC correlates with the severity of the underlying disease, the impact of DIC on mortality varies significantly depending on the nature of the disease. Furthermore, no previous studies have described the differences in the effect of DIC on mortality among various underlying diseases.
DIC is associated with various underlying diseases[1] [2] [3] [4] [5] and presents differently based on these conditions.[4] [5] [6] [7] However, studies directly comparing the characteristics of coagulation/fibrinolysis laboratory findings for DIC depending on the underlying disease are limited. Although various underlying conditions can trigger DIC in critical care settings, previous reports have only compared the characteristics of coagulation/fibrinolysis laboratory findings in DIC associated with sepsis, solid tumors, and hematologic malignancy. In the present study, the characteristics of DIC associated with sepsis upon arrival to the ED included prolonged prothrombin time, increased fibrinogen levels, and decreased AT activity. Increased fibrinogen levels and decreased AT activity, which are induced by persistent severe inflammation, have been reported in previous studies.[8] [9] [10] These changes may also be caused by sustained inflammatory responses.[16] [17]
Trauma-associated DIC is classified as a fibrinolytic phenotype and is characterized by elevated D-dimer and FDP levels.[4] [5] [6] [18] In the present study, patients with trauma-associated DIC exhibited a marked increase in D-dimer and FDP levels upon arrival at the ED, attributable to fibrinolytic activation following stimulation of coagulation. Furthermore, the fibrinogen levels in patients with trauma-associated DIC were lower than those in patients with DIC associated with other underlying diseases. The low fibrinogen level is one of the characteristics of DIC with a fibrinolytic phenotype. However, although trauma-associated DIC is associated with hemorrhagic complications,[4] [5] [6] [18] low platelet counts and prolonged prothrombin time were not observed on arrival at the ED, which aligns with a previous report.[19] Additionally, the frequency of DIC rapidly decreased from day 1, on arrival at the ED, to day 3 compared to that of DIC associated with other underlying conditions.
In patients with severe burns, DIC is strongly associated with poor outcomes.[20] [21] [22] However, no studies have described the characteristics of burn-associated DIC in the early phases of burn. In the present study, the most characteristic feature of patients with burn-associated DIC was the change in platelet count. Platelet counts in patients with burn-associated DIC did not decrease upon arrival at the ED, but subsequently declined rapidly. Furthermore, a rapid decrease in AT activity from day 1 to 2 is characteristic of burn-associated DIC. These changes have been reported in patients with severe burns regardless of the presence or absence of DIC.[23] [24] [25] These phenomena are likely influenced by hemoconcentration due to increased vascular permeability following severe burn, as well as the diluting effect of fluid administration.[25]
Hypothermia induces coagulation disorders in various clinical settings by inhibiting coagulation enzymatic reactions[26] and causing platelet dysfunction.[27] Conversely, it has been reported that hypothermia-induced platelet aggregation can cause microvascular thrombosis.[28] However, usually, accidental hypothermia is promptly rewarmed after arrival at the ED. Therefore, the coagulation disorder is promptly improved, similar to our observations. In this study, most patients with accidental hypothermia were elderly and developed the condition indoors, analogous to the previous registry study in Japan.[29] The characteristics of coagulation/fibrinolysis abnormalities in accidental hypothermia may differ between indoor and outdoor occurrences.[30]
In the present study, the information on anti-DIC treatments was not collected. In our institute, we often administered AT concentrates and/or recombinant thrombomodulin in patients with sepsis-associated DIC. These treatments might improve the deterioration of platelet counts and AT activity in patients with sepsis-associated DIC after admission.[31] [32] In patients with severe trauma, tranexamic acid is usually administered after admission. Tranexamic acid might promptly suppress the fibrinolysis activation and early decreases in D-dimer and FDP levels. However, in severe trauma, the fibrinolysis activation was previously reported to be physiologically and rapidly suppressed by plasminogen activator inhibitor-1, regardless of whether tranexamic acid was administered.[33] [34] Furthermore, these anti-DIC treatments may improve in-hospital mortality rates in patients with DIC.[35] [36] [37] [38] [39]
The present study has some limitations. First, this was a single-center retrospective study. Therefore, although a relatively large number of patients were included, generalizability may be limited. Second, molecular markers such as the thrombin- AT complex and plasmin–antiplasmin complex were not measured. To evaluate the DIC phenotype in detail, measuring these molecular markers must be considered. However, these molecular markers are not routinely measured in clinical practice. In the present study, we identified the various characteristics of DIC associated with each underlying disease using standard coagulation/fibrinolysis laboratory results. Third, severity levels were inconsistent among the underlying diseases. However, we have compared the characteristics of DIC across underlying diseases, achieving a degree of uniformity in severity associated with DIC. Fourth, the information on anti-DIC treatments was not collected in the present study. Anti-DIC treatments may affect the changes in coagulation/fibrinolysis laboratory results and in-hospital mortality after admission. However, anti-DIC treatment had no effect on the coagulation/fibrinolysis laboratory results on arrival at the ED.
In conclusion, significant heterogeneity was observed in the coagulation/fibrinolysis laboratory findings, as well as in the clinical progression of DIC, depending on the underlying cause. Notably, the development of DIC upon arrival at the ED in patients with burn and trauma was strongly associated with higher in-hospital mortality compared to other underlying diseases. These findings may suggest that the type and importance of treatment for DIC could vary depending on the underlying disease.
What Is known about this topic?
-
Disseminated intravascular coagulation (DIC) is a critical condition characterized by the systemic activation of coagulation, leading to thrombotic as well as hemorrhagic complications.
-
The pathophysiology of DIC varies depending on the underlying cause, with two main phenotypes identified as thrombotic and fibrinolytic.
-
However, previous studies focused on a limited number of diseases, and a comprehensive comparison of coagulation/fibrinolysis findings across a wide range of critical illnesses remains lacking.
What does this paper add?
-
This study revealed significant heterogeneity in the coagulation/fibrinolysis laboratory findings across various underlying diseases, including trauma, burn, sepsis, heat stroke, and out-of-hospital cardiac arrest.
-
We identified that trauma- and burn-associated DIC on arrival at the emergency department were particularly strongly linked to an increase in in-hospital mortality compared to other underlying diseases.
-
Improvement rates for DIC also showed heterogeneity, with trauma- and accidental hypothermia-associated DIC improving more rapidly than other medical conditions.
Contributors' Statement
M. Hayamizu contributed to data curation, investigation, and writing—review and editing. M. Hayakawa contributed to conceptualization, formal analysis, methodology, project administration, resources, supervision, visualization, and writing—review. and editing. Both authors approved the final manuscript.
Conflict of Interest
The authors declare that they have no conflict of interest.
Ethical Approval
This study was approved by the Institutional Review Board of the Ethics Committee of Hokkaido University Hospital (no. 024-0247, approved November 12, 2024) and was conducted in accordance with the Declaration of Helsinki. The need for written informed consent was waived because of the retrospective design of the study.
-
References
- 1 Levi M, Sivapalaratnam S. Disseminated intravascular coagulation: an update on pathogenesis and diagnosis. Expert Rev Hematol 2018; 11 (08) 663-672
- 2 Levi M, de Jonge E, van der Poll T, ten Cate H. Disseminated intravascular coagulation. Thromb Haemost 1999; 82 (02) 695-705
- 3 Iba T, Levi M, Thachil J, Levy JH. Disseminated intravascular coagulation: the past, present, and future considerations. Semin Thromb Hemost 2022; 48 (08) 978-987
- 4 Gando S, Levi M, Toh CH. Disseminated intravascular coagulation. J Intensive Care 2025; 13 (01) 32
- 5 Iba T, Levy JH, Maier CL. et al. Updated definition and scoring of disseminated intravascular coagulation in 2025: communication from the ISTH SSC Subcommittee on Disseminated Intravascular Coagulation. J Thromb Haemost 2025; 23 (07) 2356-2362
- 6 Wada T, Gando S. Phenotypes of disseminated intravascular coagulation. Thromb Haemost 2024; 124 (03) 181-191
- 7 Asakura H. Classifying types of disseminated intravascular coagulation: clinical and animal models. J Intensive Care 2014; 2 (01) 20
- 8 Takahashi H, Tatewaki W, Wada K, Hanano M, Shibata A. Thrombin vs. plasmin generation in disseminated intravascular coagulation associated with various underlying disorders. Am J Hematol 1990; 33 (02) 90-95
- 9 Kawasugi K, Wada H, Hatada T. et al; Japanese Society of Thrombosis Hemostasis/DIC Subcommittee. Prospective evaluation of hemostatic abnormalities in overt DIC due to various underlying diseases. Thromb Res 2011; 128 (02) 186-190
- 10 Asakura H, Ontachi Y, Mizutani T. et al. An enhanced fibrinolysis prevents the development of multiple organ failure in disseminated intravascular coagulation in spite of much activation of blood coagulation. Crit Care Med 2001; 29 (06) 1164-1168
- 11 Ohbe H, Yamakawa K, Taniguchi K. et al. Underlying disorders, clinical phenotypes, and treatment diversity among patients with disseminated intravascular coagulation. JMA J 2020; 3 (04) 321-329
- 12 Bone RC, Balk RA, Cerra FB. et al; The ACCP/SCCM Consensus Conference Committee. American College of Chest Physicians/Society of Critical Care Medicine. Definitions for sepsis and organ failure and guidelines for the use of innovative therapies in sepsis. Chest 1992; 101 (06) 1644-1655
- 13 Levy MM, Fink MP, Marshall JC. et al. SCCM/ESICM/ACCP/ATS/SIS International Sepsis Definitions Conference. Crit Care Med 2001; 2003: 31
- 14 Baker SP, O'Neill B, Haddon Jr W, Long WB. The injury severity score: a method for describing patients with multiple injuries and evaluating emergency care. J Trauma 1974; 14 (03) 187-196
- 15 Gando S, Saitoh D, Ogura H. et al; Japanese Association for Acute Medicine Disseminated Intravascular Coagulation (JAAM DIC) Study Group. Natural history of disseminated intravascular coagulation diagnosed based on the newly established diagnostic criteria for critically ill patients: results of a multicenter, prospective survey. Crit Care Med 2008; 36 (01) 145-150
- 16 Aibiki M, Fukuoka N, Umakoshi K, Ohtsubo S, Kikuchi S. Serum albumin levels anticipate antithrombin III activities before and after antithrombin III agent in critical patients with disseminated intravascular coagulation. Shock 2007; 27 (02) 139-144
- 17 Luyendyk JP, Schoenecker JG, Flick MJ. The multifaceted role of fibrinogen in tissue injury and inflammation. Blood 2019; 133 (06) 511-520
- 18 Hayakawa M. Pathophysiology of trauma-induced coagulopathy: disseminated intravascular coagulation with the fibrinolytic phenotype. J Intensive Care 2017; 5: 14
- 19 Hayakawa M, Gando S, Ono Y, Wada T, Yanagida Y, Sawamura A. Fibrinogen level deteriorates before other routine coagulation parameters and massive transfusion in the early phase of severe trauma: a retrospective observational study. Semin Thromb Hemost 2015; 41 (01) 35-42
- 20 Lavrentieva A, Kontakiotis T, Bitzani M. et al. Early coagulation disorders after severe burn injury: impact on mortality. Intensive Care Med 2008; 34 (04) 700-706
- 21 Lippi G, Ippolito L, Cervellin G. Disseminated intravascular coagulation in burn injury. Semin Thromb Hemost 2010; 36 (04) 429-436
- 22 Zhang TN, Ba T, Li F. et al. Coagulation dysfunction of severe burn patients: a potential cause of death. Burns 2023; 49 (03) 678-687
- 23 Cato LD, Wearn CM, Bishop JRB, Stone MJ, Harrison P, Moiemen N. Platelet count: a predictor of sepsis and mortality in severe burns. Burns 2018; 44 (02) 288-297
- 24 Niedermayr M, Schramm W, Kamolz L. et al. Antithrombin deficiency and its relationship to severe burns. Burns 2007; 33 (02) 173-178
- 25 Osuka A, Ishihara T, Shimizu K, Shintani A, Ogura H, Ueyama M. Natural kinetics of blood cells following major burn: impact of early decreases in white blood cells and platelets as prognostic markers of mortality. Burns 2019; 45 (08) 1901-1907
- 26 Rohrer MJ, Natale AM. Effect of hypothermia on the coagulation cascade. Crit Care Med 1992; 20 (10) 1402-1405
- 27 Wallner B, Schenk B, Hermann M. et al. Hypothermia-associated coagulopathy: a comparison of viscoelastic monitoring, platelet function, and real time live confocal microscopy at low blood temperatures, an in vitro experimental study. Front Physiol 2020; 11: 843
- 28 Lindenblatt N, Menger MD, Klar E, Vollmar B. Sustained hypothermia accelerates microvascular thrombus formation in mice. Am J Physiol Heart Circ Physiol 2005; 289 (06) H2680-H2687
- 29 Matsuyama T, Morita S, Ehara N. et al. Characteristics and outcomes of accidental hypothermia in Japan: the J-point registry. Emerg Med J 2018; 35 (11) 659-666
- 30 Fujimoto Y, Matsuyama T, Morita S. et al. Indoor versus outdoor occurrence in mortality of accidental hypothermia in Japan: the J-point registry. Ther Hypothermia Temp Manag 2020; 10 (03) 159-164
- 31 Kobayashi T, Mikami R, Hayakawa M. Association between recombinant human soluble thrombomodulin administration dosages and mortality in patients with sepsis-induced disseminated intravascular coagulation. Thromb J 2025; 23 (01) 101
- 32 Iba T, Saitoh D, Wada H, Asakura H. Efficacy and bleeding risk of antithrombin supplementation in septic disseminated intravascular coagulation: a secondary survey. Crit Care 2014; 18 (05) 497
- 33 Hayakawa M, Tsuchida T, Honma Y. et al. Fibrinolytic system activation immediately following trauma was quickly and intensely suppressed in a rat model of severe blunt trauma. Sci Rep 2021; 11 (01) 20283
- 34 Gando S, Hayakawa M. Pathophysiology of trauma-induced coagulopathy and management of critical bleeding requiring massive transfusion. Semin Thromb Hemost 2016; 42 (02) 155-165
- 35 Hayakawa M, Kudo D, Saito S. et al. Antithrombin supplementation and mortality in sepsis-induced disseminated intravascular coagulation: a multicenter retrospective observational study. Shock 2016; 46 (06) 623-631
- 36 Hayakawa M, Yamakawa K, Saito S. et al; Japan Septic Disseminated Intravascular Coagulation (JSEPTIC DIC) study group. Recombinant human soluble thrombomodulin and mortality in sepsis-induced disseminated intravascular coagulation. A multicentre retrospective study. Thromb Haemost 2016; 115 (06) 1157-1166
- 37 Takahashi Y, Hayakawa M, Itagaki Y, Ono K, Kudo D, Kushimoto S. Coagulopathy as a predictor of the effectiveness of tranexamic acid in severe blunt trauma: a multicenter retrospective study. Thromb J 2025; 23 (01) 37
- 38 Yamakawa K, Okamoto K, Seki Y. et al; Committee of the Clinical Practice Guidelines for Management of Disseminated Intravascular Coagulation 2024, the Japanese Society on Thrombosis and Hemostasis. Clinical practice guidelines for management of disseminated intravascular coagulation in Japan 2024. Part 1: sepsis. Int J Hematol 2025; 121 (05) 592-604
- 39 Hayakawa M, Seki Y, Ikezoe T. et al; Committee of the Clinical Practice Guidelines for Disseminated Intravascular Coagulation 2024, the Japanese Society on Thrombosis, Hemostasis. Clinical practice guidelines for management of disseminated intravascular coagulation in Japan 2024: part 4-trauma, burn, obstetrics, acute pancreatitis/liver failure, and others. Int J Hematol 2025; 121 (05) 633-652
- 40 Cohen J. Statistical Power Analysis for the Behavioural Sciences, 2nd Edn. Hillside, NJ: Lawrence Erlbaum Associates; 1988. : pp. 25-27
Correspondence
Publication History
Received: 06 October 2025
Accepted: 31 January 2026
Article published online:
12 February 2026
© 2026. The Author(s). This is an open access article published by Thieme under the terms of the Creative Commons Attribution License, permitting unrestricted use, distribution, and reproduction so long as the original work is properly cited. (https://creativecommons.org/licenses/by/4.0/)
Georg Thieme Verlag KG
Oswald-Hesse-Straße 50, 70469 Stuttgart, Germany
-
References
- 1 Levi M, Sivapalaratnam S. Disseminated intravascular coagulation: an update on pathogenesis and diagnosis. Expert Rev Hematol 2018; 11 (08) 663-672
- 2 Levi M, de Jonge E, van der Poll T, ten Cate H. Disseminated intravascular coagulation. Thromb Haemost 1999; 82 (02) 695-705
- 3 Iba T, Levi M, Thachil J, Levy JH. Disseminated intravascular coagulation: the past, present, and future considerations. Semin Thromb Hemost 2022; 48 (08) 978-987
- 4 Gando S, Levi M, Toh CH. Disseminated intravascular coagulation. J Intensive Care 2025; 13 (01) 32
- 5 Iba T, Levy JH, Maier CL. et al. Updated definition and scoring of disseminated intravascular coagulation in 2025: communication from the ISTH SSC Subcommittee on Disseminated Intravascular Coagulation. J Thromb Haemost 2025; 23 (07) 2356-2362
- 6 Wada T, Gando S. Phenotypes of disseminated intravascular coagulation. Thromb Haemost 2024; 124 (03) 181-191
- 7 Asakura H. Classifying types of disseminated intravascular coagulation: clinical and animal models. J Intensive Care 2014; 2 (01) 20
- 8 Takahashi H, Tatewaki W, Wada K, Hanano M, Shibata A. Thrombin vs. plasmin generation in disseminated intravascular coagulation associated with various underlying disorders. Am J Hematol 1990; 33 (02) 90-95
- 9 Kawasugi K, Wada H, Hatada T. et al; Japanese Society of Thrombosis Hemostasis/DIC Subcommittee. Prospective evaluation of hemostatic abnormalities in overt DIC due to various underlying diseases. Thromb Res 2011; 128 (02) 186-190
- 10 Asakura H, Ontachi Y, Mizutani T. et al. An enhanced fibrinolysis prevents the development of multiple organ failure in disseminated intravascular coagulation in spite of much activation of blood coagulation. Crit Care Med 2001; 29 (06) 1164-1168
- 11 Ohbe H, Yamakawa K, Taniguchi K. et al. Underlying disorders, clinical phenotypes, and treatment diversity among patients with disseminated intravascular coagulation. JMA J 2020; 3 (04) 321-329
- 12 Bone RC, Balk RA, Cerra FB. et al; The ACCP/SCCM Consensus Conference Committee. American College of Chest Physicians/Society of Critical Care Medicine. Definitions for sepsis and organ failure and guidelines for the use of innovative therapies in sepsis. Chest 1992; 101 (06) 1644-1655
- 13 Levy MM, Fink MP, Marshall JC. et al. SCCM/ESICM/ACCP/ATS/SIS International Sepsis Definitions Conference. Crit Care Med 2001; 2003: 31
- 14 Baker SP, O'Neill B, Haddon Jr W, Long WB. The injury severity score: a method for describing patients with multiple injuries and evaluating emergency care. J Trauma 1974; 14 (03) 187-196
- 15 Gando S, Saitoh D, Ogura H. et al; Japanese Association for Acute Medicine Disseminated Intravascular Coagulation (JAAM DIC) Study Group. Natural history of disseminated intravascular coagulation diagnosed based on the newly established diagnostic criteria for critically ill patients: results of a multicenter, prospective survey. Crit Care Med 2008; 36 (01) 145-150
- 16 Aibiki M, Fukuoka N, Umakoshi K, Ohtsubo S, Kikuchi S. Serum albumin levels anticipate antithrombin III activities before and after antithrombin III agent in critical patients with disseminated intravascular coagulation. Shock 2007; 27 (02) 139-144
- 17 Luyendyk JP, Schoenecker JG, Flick MJ. The multifaceted role of fibrinogen in tissue injury and inflammation. Blood 2019; 133 (06) 511-520
- 18 Hayakawa M. Pathophysiology of trauma-induced coagulopathy: disseminated intravascular coagulation with the fibrinolytic phenotype. J Intensive Care 2017; 5: 14
- 19 Hayakawa M, Gando S, Ono Y, Wada T, Yanagida Y, Sawamura A. Fibrinogen level deteriorates before other routine coagulation parameters and massive transfusion in the early phase of severe trauma: a retrospective observational study. Semin Thromb Hemost 2015; 41 (01) 35-42
- 20 Lavrentieva A, Kontakiotis T, Bitzani M. et al. Early coagulation disorders after severe burn injury: impact on mortality. Intensive Care Med 2008; 34 (04) 700-706
- 21 Lippi G, Ippolito L, Cervellin G. Disseminated intravascular coagulation in burn injury. Semin Thromb Hemost 2010; 36 (04) 429-436
- 22 Zhang TN, Ba T, Li F. et al. Coagulation dysfunction of severe burn patients: a potential cause of death. Burns 2023; 49 (03) 678-687
- 23 Cato LD, Wearn CM, Bishop JRB, Stone MJ, Harrison P, Moiemen N. Platelet count: a predictor of sepsis and mortality in severe burns. Burns 2018; 44 (02) 288-297
- 24 Niedermayr M, Schramm W, Kamolz L. et al. Antithrombin deficiency and its relationship to severe burns. Burns 2007; 33 (02) 173-178
- 25 Osuka A, Ishihara T, Shimizu K, Shintani A, Ogura H, Ueyama M. Natural kinetics of blood cells following major burn: impact of early decreases in white blood cells and platelets as prognostic markers of mortality. Burns 2019; 45 (08) 1901-1907
- 26 Rohrer MJ, Natale AM. Effect of hypothermia on the coagulation cascade. Crit Care Med 1992; 20 (10) 1402-1405
- 27 Wallner B, Schenk B, Hermann M. et al. Hypothermia-associated coagulopathy: a comparison of viscoelastic monitoring, platelet function, and real time live confocal microscopy at low blood temperatures, an in vitro experimental study. Front Physiol 2020; 11: 843
- 28 Lindenblatt N, Menger MD, Klar E, Vollmar B. Sustained hypothermia accelerates microvascular thrombus formation in mice. Am J Physiol Heart Circ Physiol 2005; 289 (06) H2680-H2687
- 29 Matsuyama T, Morita S, Ehara N. et al. Characteristics and outcomes of accidental hypothermia in Japan: the J-point registry. Emerg Med J 2018; 35 (11) 659-666
- 30 Fujimoto Y, Matsuyama T, Morita S. et al. Indoor versus outdoor occurrence in mortality of accidental hypothermia in Japan: the J-point registry. Ther Hypothermia Temp Manag 2020; 10 (03) 159-164
- 31 Kobayashi T, Mikami R, Hayakawa M. Association between recombinant human soluble thrombomodulin administration dosages and mortality in patients with sepsis-induced disseminated intravascular coagulation. Thromb J 2025; 23 (01) 101
- 32 Iba T, Saitoh D, Wada H, Asakura H. Efficacy and bleeding risk of antithrombin supplementation in septic disseminated intravascular coagulation: a secondary survey. Crit Care 2014; 18 (05) 497
- 33 Hayakawa M, Tsuchida T, Honma Y. et al. Fibrinolytic system activation immediately following trauma was quickly and intensely suppressed in a rat model of severe blunt trauma. Sci Rep 2021; 11 (01) 20283
- 34 Gando S, Hayakawa M. Pathophysiology of trauma-induced coagulopathy and management of critical bleeding requiring massive transfusion. Semin Thromb Hemost 2016; 42 (02) 155-165
- 35 Hayakawa M, Kudo D, Saito S. et al. Antithrombin supplementation and mortality in sepsis-induced disseminated intravascular coagulation: a multicenter retrospective observational study. Shock 2016; 46 (06) 623-631
- 36 Hayakawa M, Yamakawa K, Saito S. et al; Japan Septic Disseminated Intravascular Coagulation (JSEPTIC DIC) study group. Recombinant human soluble thrombomodulin and mortality in sepsis-induced disseminated intravascular coagulation. A multicentre retrospective study. Thromb Haemost 2016; 115 (06) 1157-1166
- 37 Takahashi Y, Hayakawa M, Itagaki Y, Ono K, Kudo D, Kushimoto S. Coagulopathy as a predictor of the effectiveness of tranexamic acid in severe blunt trauma: a multicenter retrospective study. Thromb J 2025; 23 (01) 37
- 38 Yamakawa K, Okamoto K, Seki Y. et al; Committee of the Clinical Practice Guidelines for Management of Disseminated Intravascular Coagulation 2024, the Japanese Society on Thrombosis and Hemostasis. Clinical practice guidelines for management of disseminated intravascular coagulation in Japan 2024. Part 1: sepsis. Int J Hematol 2025; 121 (05) 592-604
- 39 Hayakawa M, Seki Y, Ikezoe T. et al; Committee of the Clinical Practice Guidelines for Disseminated Intravascular Coagulation 2024, the Japanese Society on Thrombosis, Hemostasis. Clinical practice guidelines for management of disseminated intravascular coagulation in Japan 2024: part 4-trauma, burn, obstetrics, acute pancreatitis/liver failure, and others. Int J Hematol 2025; 121 (05) 633-652
- 40 Cohen J. Statistical Power Analysis for the Behavioural Sciences, 2nd Edn. Hillside, NJ: Lawrence Erlbaum Associates; 1988. : pp. 25-27