

RSS-Feed abonnieren
DOI: 10.1055/s-0037-1602698
Minimally Invasive Biopsies of Deep-Seated Brain Lesions Using Tubular Retractors Under Exoscopic Visualization
Autor*innen
Address for correspondence
Publikationsverlauf
05. November 2016
07. März 2017
Publikationsdatum:
08. Mai 2017 (online)


Abstract
Background and Study Aims/Objective Brain lesions in deep-seated locations can present a surgical challenge. Tissue remains the gold standard for diagnosing these lesions to guide potential adjuvant therapy. These lesions have been traditionally approached by stereotactic needle biopsy, open biopsies through craniotomies, and excisional biopsies. We provide a safe alternative method using tubular retractors under exoscopic visualization for biopsies of deep-seated brain lesions.
Material and Methods All patients who underwent a biopsy with the use of a tubular retractor under exoscopic visualization of a deep-seated lesion from January 2013 to September 2016 were identified prospectively and followed. This was done for patients with lesions where extensive resection was not deemed possible because of eloquent location and/or lack of impact on the natural history of the disease.
Results A total of 11 patients, with an average age (plus or minus standard deviation) of 48.7 ± 18.3 years, underwent biopsies with tubular retractors and exoscopic visualization. The locations included thalamus (n = 3), optic pathway (n = 2), deep cerebellar nuclei (n = 1), centrum semiovale/corpus callosum (n = 4), and multifocal (n = 2). Diagnosis was obtained in all patients: glioblastoma multiforme (n = 3), anaplastic astrocytoma (n = 3), demyelinating disease (n = 2), renal cell cancer (n = 1), and lymphoma (n = 2). In all cases with tumors, the molecular analyses were conducted successfully. On postoperative computed tomography, no patients had notable hematomas and no patients had new deficits.
Conclusion Diagnosing brain lesions is critical for guiding potential adjuvant therapies. When surgical resection is not possible or required, we report the efficacy of a tubular retractor system with exoscopic visualization for the safe access of deep-seated lesions to provide adequate tissue for diagnosis and molecular evaluation.
Introduction
Brain lesions in deep-seated locations present a surgical challenge.[1] [2] [3] [4] In certain situations, extensive surgical resection is not considered appropriate either because resection may not alter the natural history of the disease or may not be possible without causing significant morbidity.[1] [2] [3] [4] However, obtaining tissue for diagnosis is often necessary to guide potential adjuvant therapies including radiation and chemotherapy.[1] [2] [3] [4] The typical approach for obtaining tissue for these lesions involves either burr hole needle biopsies or open biopsies through craniotomies.[1] [2] [3] [4] Needle biopsies provide a scant amount of tissue, making it difficult to establish pathologic diagnoses.[5] [6] [7] [8] [9] [10] Moreover, this lack of tissue often precludes molecular studies and tissue banking for further testing.[5] [6] [7] [8] [9] [10]
For deep-seated lesions, open biopsies through craniotomies require larger openings and have a similar risk profile to craniotomies aiming to achieve extensive resection.[11] [12] We present an alternative minimally invasive technique for performing biopsies via small craniotomies using tubular retractors under exoscopic visualization with the use of an extracorporeal scope. This technique has the advantage of supplying sufficient tissue for diagnosis and further testing, and it may be an alternative to traditional burr hole needle biopsies and open biopsies through craniotomies.
Materials and Methods
Institutional approval was obtained prior to the start of this study (no. 72892).
Patient Selection
All patients who underwent biopsy using minimally invasive surgery with the use of a tubular retractor under exoscopic visualization from January 2013 to September 2016 by the senior authors (K.C. and G.G.) were identified prospectively. This included lesions located in deep-seated areas that include basal ganglia, thalamus, cerebellar peduncles, and hippocampal regions, where extensive resection was not deemed possible because of eloquent location and/or lack of impact on the natural history of the disease. Biopsies were defined as planned subtotal resection of the selected lesion or resection of one lesion in the case of multiple brain lesions. These patients were identified prospectively, and recorded variables included age, gender, tumor location, tumor size, preoperative neurologic function, specimen size, postoperative hematoma (significant being more than punctate), postoperative neurologic function, and follow-up time.
General Treatment Strategy
Patients who presented with deep-seated lesions where a diagnosis was needed and extensive resection was not deemed appropriate either because of surgical morbidity and/or the effects of surgical resection would not change the natural history of the lesion were considered candidates for this approach ([Figs. 1] and [2]). Patients would undergo preoperative magnetic resonance imaging (MRI) 1 to 2 days before surgery. For basal ganglia and thalamic lesions, diffusion tensor images were also typically obtained to understand the location of critical white matter tracts. The trajectory toward the lesion was planned ahead of time and based on causing the least amount of surgical morbidity and avoiding critical white matter tracts. A trans-sulcal route was typically preferred to minimize the amount of injury to the brain parenchyma and to avoid injuring critical white matter tracts.
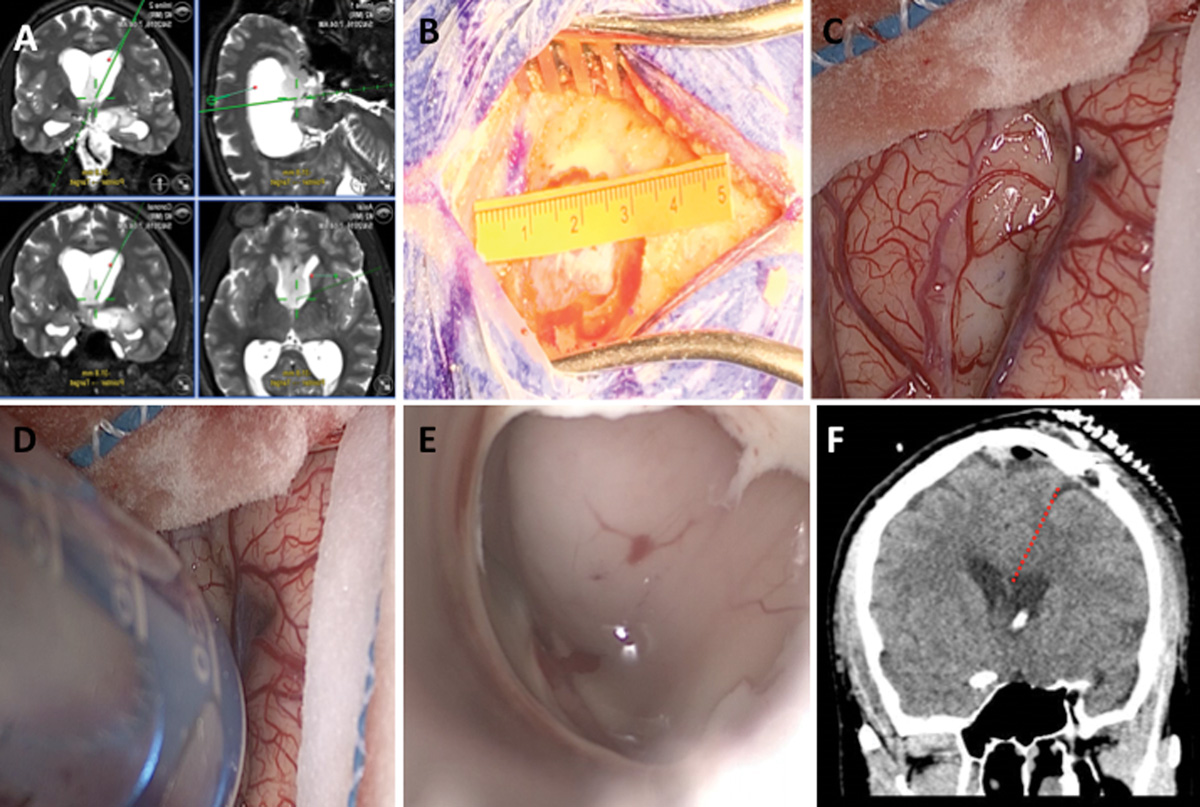

A linear incision measuring 2 to 3 cm was typically done over the planned trajectory based on navigation guidance (Brainlab, Westchester, Illinois, United States) ([Fig. 1B]). A high-speed drill equipped with a perforator was used to make a burr hole, and a craniotome was used to perform a craniotomy measuring ∼ 3 cm in diameter ([Fig. 1B]). The dura was then opened in a cruciate fashion measuring ∼ 1 × 1 cm overlying the desired sulcus ([Fig. 1C]). A 0- or 90-degree exoscope (VITOM; Karl Storz, El Segundo, California, United States) attached to a pneumatic arm (UniArm; Mitaka, Park City, Utah, United States) was used to provide visualization and magnification to open the desired sulcus. Under navigation guidance, a preselected tubular retractor with cannula (BrainPath; NICO, Indianapolis, Indiana, United States) of the desired length to reach the superficial surface of the lesion was passed through the sulcus ([Fig. 1D]).
Once the superficial surface of the lesion was reached, the internal cannula was removed and the exoscope provided visualization ([Fig. 1E]). An exoscopic view is visualization with the use of a scope external to the body. This contrasts with an endoscopic view where visualization is obtained by placing a scope inside the body (i.e., through the nose, into the brain, etc.) ([Fig. 3]). Specimens were then obtained using tumor forceps and/or a side-biting tissue aspiration device (Myriad; NICO). Depending on how much tissue was needed and the location of the tissue, more specimen was obtained and/or the retractor was moved to a different location to obtain more tissue. In circumstances where it was unclear if the retractor was in the desired location, an ultrasound probe (Hitachi Aloka, Wallingford, Connecticut, USA) was passed through the retractor to confirm location. The amount of specimen provided to pathology was measured by the pathologist when placed on a slide prior to freezing.

After resection, the retractor was slowly withdrawn ([Fig. 2D]). Irrigation was used in the cavity to confirm hemostasis. The dura was then closed primarily. The bone flap was replaced with titanium plates. The galea and scalp were closed in standard fashion. Postoperative head computed tomography (CT) was then performed to evaluate unexpected postoperative changes ([Figs. 1F] and [2E]). The patient were observed in the critical care unit overnight and typically discharged on postoperative day 1.
Results
Eleven patients underwent minimally invasive surgery for biopsies using tubular retractors with exoscopic guidance for deep-seated brain lesions from January 2013 to September 2016 ([Table 1]). Six were male and five were female, with an average age (plus or minus standard deviation [SD]) of 48.7 ± 18.3 years. The locations included thalamus in three, optic pathway in two, deep cerebellar nuclei in one, centrum semiovale/corpus callosum in four, and multifocal in two. Four of these patients underwent surgery because there was concern about tumor versus demyelinating/inflammatory disorder, one underwent surgery to evaluate recurrent tumor versus treatment effect for glioblastoma multiforme, and two had presumed lymphoma.
Preoperatively, five patients presented with weakness, four with headaches, two with seizures, and two with vision complaints. The median preoperative tumor volume was 7.2 cm3 (interquartile range [IQR]: 1.3–12.4 cm3), and the median tissue volume delivered to pathology was 0.1 cm3 (IQR: 0.04–0.2 cm3). Diagnosis was obtained in all 11 patients. In all cases with tumors, the molecular analyses were conducted successfully. On postoperative CT, no patients had notable hematomas. The median new postoperative blood in the cavity was 0 cm3 (IQR: 0–0.001 cm3), where six (55%) had no visible blood products. In addition, no patients had new deficits, wound infection, and/or required repeat surgery for more tissue for diagnosis. Patients were followed for an average of 6 months (SD: ± 3 months)
Discussion
In this study, 11 consecutive patients underwent biopsy of deep-seated brain lesions with the use of tubular retractors and exoscopic visualization. We show that this system can be used to obtain tissue samples for deep-seated brain lesions with a 100% diagnostic rate with minimal perioperative morbidity. In all cases, abundant tissue was provided for diagnosis, and in confirmed tumor cases, molecular analyses could be done successfully. No complications including hematomas, new deficit, symptomatic strokes, malignant edema, or repeat surgeries occurred. We present an alternative method that provides more tissue for diagnoses and molecular analyses than needle biopsies and an arguably safer approach than traditional open biopsies for deep-seated lesions. More tissue is often necessary for certain pathologies such as gliomas but unlikely necessary for lymphomas.
Safe and effective access to deep-seated intra-axial brain lesions presents a surgical challenge. Despite advances in imaging modalities, radiographic studies still have up to a 20 to 30% false diagnosis rate.[1] [2] [3] [4] Therefore, tissue remains the gold standard for diagnosis to guide potential adjuvant therapy. These lesions have been traditionally approached by stereotactic needle biopsy or open biopsies through craniotomies.[1] [2] [3] [4] Although needle biopsies have the advantage of minimally traumatizing brain tissue given their small size, their disadvantages include small sample size prone to low diagnostic yield, need for repeat sampling, and lack of necessary tissue for genetic analyses and potential tissue banking.[1] [2] [3] [4] Diagnostic error were as high as 20 to 30% in several series.[1] [2] [3] [4] Moreover, the lack of direct visualization can make it difficult to confirm hemostasis and stop potential bleeding during these procedures, where postoperative bleeding has been reported in up to 9% of stereotactic biopsies.[5] [6] [7] [8] [9] [10] Open biopsies through craniotomies require larger openings than stereotactic biopsies.[11] [12]
Although they can provide a relatively large sample size for pathologic diagnosis, open biopsies for deep-seated lesions are associated with higher rates of surgery-related morbidities due to the need for larger tissue exposure, prolonged retraction of surrounding brain tissue, and more dissection of critical white matter tracts.[11] [12] As compared with needle biopsies, open biopsies are more frequently associated with cerebral edema, infarction, and hemorrhagic transformation.[11] [12] [13] [14] [15] The rates of intracranial hemorrhage vary from 7% to 30% and postoperative seizures in 10 to 20% of open biopsies.[11] [12] [13] [14] [15]
Tubular retractor systems were designed to provide access to deep corridors while limiting associated risks.[16] [17] [18] [19] [20] [21] However, these earlier versions were limited due to the bulk and lack of transparency of the metal or hard plastic retractors.[16] [17] [18] [19] [20] [21] Furthermore, the fixed nature of frame-based stereotactic navigation system was cumbersome and limited the flexibility of the operative field.[16] [17] [18] [19] [20] [21] The system used in this study was a transparent plastic tubular retractor with a diameter that provides safe displacement of white matter tracts.[22] [23] The use of an exoscope, or an extracorporeal scope, provided optimum visualization through this transparent retractor system.[22] [23] This is different than an endoscope because it is placed above the surgical field outside of the surgical cavity, whereas an endoscope is placed within the cavity. By being above the surgical field, an exoscope allows bimanual manipulation, no need to hold the scope because it is attached to a pneumatic arm, and it does not reduce the working corridor.
In addition, an exoscope, as compared with a microscope, provides more operative flexibility and degrees of visualization by having smaller optics, higher magnification ability, and more maneuverability.[22] [23] The retractor itself has a 13.5-mm diameter and its length varies. It has an obturator insert that is gradually tapered and designed to displace, rather than severe, white matter tracts.[22] [23] Traditionally, this has been used for intraparenchymal clot evacuation.[23] [24] [25] More recently, it was also used to resect intra- and periventricular lesions in a multicenter study[22] and for the treatment of ruptured aneurysms, arteriovenous malformations, and cavernomas in case reports.[24] [26] We have expanded the use of this system for biopsies of deep-seated brain lesions.
Our study is the first to describe the use of this technique for accessing deep-seated lesions for biopsies. It provides an alternative to typical burr hole–based needle biopsies and open biopsies through standard craniotomies. The retractor allows safe displacement of critical white matter tracts, and no patients in this study had new deficits. The retractor also provides a corridor for obtaining sufficient tissue for pathologic examinations. The exoscope provides a similar magnification profile as surgical microscopes and allows adequate visualization for lesions located several centimeters away from the surface. Diagnosis was obtained in all cases, and sufficient tissue was available for molecular analyses and tissue banking. In addition, bleeding can be identified and addressed after the retractor is placed and removed. No patients had significant postoperative hemorrhage.
Our study is not without limitations. Patients selected for this technique were subject to bias because they were chosen selectively for this technique. It is not indicated for all deep-seated lesions but can provide an alternative to traditional methods. The study also was not designed to compare this approach with needle biopsies and/or open biopsy techniques. The gold standard would be to do a randomized study comparing different techniques. However, the main goal of this study was to provide proof of principle for the efficacy of this technique with tubular retractors. Extensive surgical resection was not considered for the patients in this series because either it would not affect the natural history of the presumed disease or surgical morbidity would be too high.
Our small sample size also limited detailed statistical analysis and generalizability of the technique. Furthermore, postoperative MRIs were not routinely obtained in the study to evaluate for extent of resection and/or subclinical injury to the surrounding brain tissue using T2 fluid-attenuated inversion recovery and diffusion-weighted image sequences. We typically only obtained postoperative head CTs. However, no patients incurred new deficits or significant parenchymal hematomas, symptomatic strokes, or malignant edema. Our short follow-up period also limits discussion of possible long-term effects and neurologic deficits. Future studies with larger cohorts may better allow the expansion of this technique. Nonetheless, we believe this technique provides a successful means of performing biopsies of deep-seated brain lesions.
Conclusion
Diagnosing brain lesions is critical for guiding potential adjuvant therapies. The gold standard for diagnosing these lesions is to obtain tissue for pathologic evaluation. This can be done either via needle biopsy or open biopsies through craniotomies. When surgical resection is not possible or required, we report the efficacy of using a tubular retractor system with exoscopic visualization for safe access of deep-seated lesions to provide adequate tissue for diagnosis, tissue banking, and molecular evaluation.
Die Autoren geben an, dass kein Interessenkonflikt besteht.
-
References
- 1 Hagen T, Nieder C, Moringlane JR, Feiden W, König J. Correlation of preoperative neuroradiologic with postoperative histologic diagnosis in pathological intracranial processes [in German]. Radiologe 1995; 35 (11) 808-815
- 2 Kim JE, Kim DG, Paek SH, Jung HW. Stereotactic biopsy for intracranial lesions: reliability and its impact on the planning of treatment. Acta Neurochir (Wien) 2003; 145 (07) 547-554 ; discussion 554–555
- 3 Kratimenos GP, Thomas DG. The role of image-directed biopsy in the diagnosis and management of brainstem lesions. Br J Neurosurg 1993; 7 (02) 155-164
- 4 Lunsford LD, Martinez AJ. Stereotactic exploration of the brain in the era of computed tomography. Surg Neurol 1984; 22 (03) 222-230
- 5 Field M, Witham TF, Flickinger JC, Kondziolka D, Lunsford LD. Comprehensive assessment of hemorrhage risks and outcomes after stereotactic brain biopsy. J Neurosurg 2001; 94 (04) 545-551
- 6 Hall WA. The safety and efficacy of stereotactic biopsy for intracranial lesions. Cancer 1998; 82 (09) 1749-1755
- 7 Kulkarni AV, Guha A, Lozano A, Bernstein M. Incidence of silent hemorrhage and delayed deterioration after stereotactic brain biopsy. J Neurosurg 1998; 89 (01) 31-35
- 8 McGirt MJ, Woodworth GF, Coon AL. , et al. Independent predictors of morbidity after image-guided stereotactic brain biopsy: a risk assessment of 270 cases. J Neurosurg 2005; 102 (05) 897-901
- 9 Nishihara M, Sasayama T, Kudo H, Kohmura E. Morbidity of stereotactic biopsy for intracranial lesions. Kobe J Med Sci 2011; 56 (04) E148-E153
- 10 Yu X, Liu Z, Tian Z. , et al. Stereotactic biopsy for intracranial space-occupying lesions: clinical analysis of 550 cases. Stereotact Funct Neurosurg 2000; 75 (2-3): 103-108
- 11 Andrews RJ, Bringas JR. A review of brain retraction and recommendations for minimizing intraoperative brain injury. Neurosurgery 1993; 33 (06) 1052-1063 ; discussion 1063–1064
- 12 Zhong J, Dujovny M, Perlin AR, Perez-Arjona E, Park HK, Diaz FG. Brain retraction injury. Neurol Res 2003; 25 (08) 831-838
- 13 Burns JD, Cadigan RO, Russell JA. Evaluation of brain biopsy in the diagnosis of severe neurologic disease of unknown etiology. Clin Neurol Neurosurg 2009; 111 (03) 235-239
- 14 Hawasli AH, Buckley RT, Gao F. , et al. Biopsy of the superficial cortex: predictors of effectiveness and outcomes. Neurosurgery 2013; 73 (02) 224-231 ; discussion 231–232; quiz 232
- 15 Schuette AJ, Taub JS, Hadjipanayis CG, Olson JJ. Open biopsy in patients with acute progressive neurologic decline and absence of mass lesion. Neurology 2010; 75 (05) 419-424
- 16 Barlas O. A simple stereotactic retractor for use with the Leksell system. Neurosurgery 1994; 34 (02) 380-381
- 17 Kelly PJ. Future perspectives in stereotactic neurosurgery: stereotactic microsurgical removal of deep brain tumors. J Neurosurg Sci 1989; 33 (01) 149-154
- 18 Kelly PJ, Goerss SJ, Kall BA. The stereotaxic retractor in computer-assisted stereotaxic microsurgery. Technical note. J Neurosurg 1988; 69 (02) 301-306
- 19 Moshel YA, Link MJ, Kelly PJ. Stereotactic volumetric resection of thalamic pilocytic astrocytomas. Neurosurgery 2007; 61 (01) 66-75 ; discussion 75
- 20 Otsuki T, Jokura H, Yoshimoto T. Stereotactic guiding tube for open-system endoscopy: a new approach for the stereotactic endoscopic resection of intra-axial brain tumors. Neurosurgery 1990; 27 (02) 326-330
- 21 Ross DA. A simple stereotactic retractor for use with the Leksell stereotactic system. Neurosurgery 1993; 32 (03) 475-476 ; discussion 476
- 22 Eliyas JK, Glynn R, Kulwin CG. , et al. Minimally invasive transsulcal resection of intraventricular and periventricular lesions through a tubular retractor system: multicentric experience and results. World Neurosurg 2016; 90: 556-564
- 23 Labib MA, Shah M, Kassam AB. , et al. The safety and feasibility of image-guided BrainPath-mediated transsulcul hematoma evacuation: a multicenter study. Neurosurgery 2016
- 24 Ding D, Starke RM, Crowley RW, Liu KC. Endoport-assisted microsurgical resection of cerebral cavernous malformations. J Clin Neurosci 2015; 22 (06) 1025-1029
- 25 Przybylowski CJ, Ding D, Starke RM, Webster Crowley R, Liu KC. Endoport-assisted surgery for the management of spontaneous intracerebral hemorrhage. J Clin Neurosci 2015; 22 (11) 1727-1732
- 26 Chen CJ, Caruso J, Starke RM. , et al. Endoport-assisted microsurgical treatment of a ruptured periventricular aneurysm. Case Rep Neurol Med 2016; 2016: 8654262
Address for correspondence
-
References
- 1 Hagen T, Nieder C, Moringlane JR, Feiden W, König J. Correlation of preoperative neuroradiologic with postoperative histologic diagnosis in pathological intracranial processes [in German]. Radiologe 1995; 35 (11) 808-815
- 2 Kim JE, Kim DG, Paek SH, Jung HW. Stereotactic biopsy for intracranial lesions: reliability and its impact on the planning of treatment. Acta Neurochir (Wien) 2003; 145 (07) 547-554 ; discussion 554–555
- 3 Kratimenos GP, Thomas DG. The role of image-directed biopsy in the diagnosis and management of brainstem lesions. Br J Neurosurg 1993; 7 (02) 155-164
- 4 Lunsford LD, Martinez AJ. Stereotactic exploration of the brain in the era of computed tomography. Surg Neurol 1984; 22 (03) 222-230
- 5 Field M, Witham TF, Flickinger JC, Kondziolka D, Lunsford LD. Comprehensive assessment of hemorrhage risks and outcomes after stereotactic brain biopsy. J Neurosurg 2001; 94 (04) 545-551
- 6 Hall WA. The safety and efficacy of stereotactic biopsy for intracranial lesions. Cancer 1998; 82 (09) 1749-1755
- 7 Kulkarni AV, Guha A, Lozano A, Bernstein M. Incidence of silent hemorrhage and delayed deterioration after stereotactic brain biopsy. J Neurosurg 1998; 89 (01) 31-35
- 8 McGirt MJ, Woodworth GF, Coon AL. , et al. Independent predictors of morbidity after image-guided stereotactic brain biopsy: a risk assessment of 270 cases. J Neurosurg 2005; 102 (05) 897-901
- 9 Nishihara M, Sasayama T, Kudo H, Kohmura E. Morbidity of stereotactic biopsy for intracranial lesions. Kobe J Med Sci 2011; 56 (04) E148-E153
- 10 Yu X, Liu Z, Tian Z. , et al. Stereotactic biopsy for intracranial space-occupying lesions: clinical analysis of 550 cases. Stereotact Funct Neurosurg 2000; 75 (2-3): 103-108
- 11 Andrews RJ, Bringas JR. A review of brain retraction and recommendations for minimizing intraoperative brain injury. Neurosurgery 1993; 33 (06) 1052-1063 ; discussion 1063–1064
- 12 Zhong J, Dujovny M, Perlin AR, Perez-Arjona E, Park HK, Diaz FG. Brain retraction injury. Neurol Res 2003; 25 (08) 831-838
- 13 Burns JD, Cadigan RO, Russell JA. Evaluation of brain biopsy in the diagnosis of severe neurologic disease of unknown etiology. Clin Neurol Neurosurg 2009; 111 (03) 235-239
- 14 Hawasli AH, Buckley RT, Gao F. , et al. Biopsy of the superficial cortex: predictors of effectiveness and outcomes. Neurosurgery 2013; 73 (02) 224-231 ; discussion 231–232; quiz 232
- 15 Schuette AJ, Taub JS, Hadjipanayis CG, Olson JJ. Open biopsy in patients with acute progressive neurologic decline and absence of mass lesion. Neurology 2010; 75 (05) 419-424
- 16 Barlas O. A simple stereotactic retractor for use with the Leksell system. Neurosurgery 1994; 34 (02) 380-381
- 17 Kelly PJ. Future perspectives in stereotactic neurosurgery: stereotactic microsurgical removal of deep brain tumors. J Neurosurg Sci 1989; 33 (01) 149-154
- 18 Kelly PJ, Goerss SJ, Kall BA. The stereotaxic retractor in computer-assisted stereotaxic microsurgery. Technical note. J Neurosurg 1988; 69 (02) 301-306
- 19 Moshel YA, Link MJ, Kelly PJ. Stereotactic volumetric resection of thalamic pilocytic astrocytomas. Neurosurgery 2007; 61 (01) 66-75 ; discussion 75
- 20 Otsuki T, Jokura H, Yoshimoto T. Stereotactic guiding tube for open-system endoscopy: a new approach for the stereotactic endoscopic resection of intra-axial brain tumors. Neurosurgery 1990; 27 (02) 326-330
- 21 Ross DA. A simple stereotactic retractor for use with the Leksell stereotactic system. Neurosurgery 1993; 32 (03) 475-476 ; discussion 476
- 22 Eliyas JK, Glynn R, Kulwin CG. , et al. Minimally invasive transsulcal resection of intraventricular and periventricular lesions through a tubular retractor system: multicentric experience and results. World Neurosurg 2016; 90: 556-564
- 23 Labib MA, Shah M, Kassam AB. , et al. The safety and feasibility of image-guided BrainPath-mediated transsulcul hematoma evacuation: a multicenter study. Neurosurgery 2016
- 24 Ding D, Starke RM, Crowley RW, Liu KC. Endoport-assisted microsurgical resection of cerebral cavernous malformations. J Clin Neurosci 2015; 22 (06) 1025-1029
- 25 Przybylowski CJ, Ding D, Starke RM, Webster Crowley R, Liu KC. Endoport-assisted surgery for the management of spontaneous intracerebral hemorrhage. J Clin Neurosci 2015; 22 (11) 1727-1732
- 26 Chen CJ, Caruso J, Starke RM. , et al. Endoport-assisted microsurgical treatment of a ruptured periventricular aneurysm. Case Rep Neurol Med 2016; 2016: 8654262