
Subscribe to RSS
DOI: 10.1055/s-0040-1716760
Nonoperative Treatment for Displaced Proximal Humeral Fractures in Elderly Patients: Correlation Between Deviations and Clinical Outcomes[*]
Article in several languages: português | English
Abstract
Objectives To describe the functional result of the conservative treatment of displaced proximal humerus fractures (PHF) using the American Shoulder and Elbow Surgeons (ASES) score after 12 months and assess whether the different initial classifications and radiographic measurements are related to clinical results.
Methods Forty patients > 60 years old, with displaced PHUs submitted to conservative treatment were evaluated at standardized times (3, 6, and 12 months). The American Society of Shoulder and Elbow Surgeons (ASES), Constant-Murley and Single Assessment Numeric Evaluation (SANE) scales were used as clinical outcomes. Radiographic variables included the Neer and Resch classifications, the presence and displacement of tuberosity fracture, metaphyseal comminution, medial periosteal lesion, and angular and translational deviations of the head in the coronal and sagittal plane.
Results The result of the ASES score was 77.7 ± 23.2 for the whole sample, the mean absolute values of the Constant-Murley score were 68.7 ± 16 and 82.6% for the scale relative to the contralateral side. The SANE scale at 12 months was 84.8 ± 19. We observed that the severity of the Neer classification and the coronal plane angular deviation (measured by the head-shaft angle) and the presence of fractures in both tuberosities negatively influenced the ASES score after 12 months of treatment.
Conclusion Nonoperative treatment of displaced proximal humerus fractures in elderly patients results in good clinical results. Clinical results are negatively influenced by the angular deviation of the humeral head and the presence of fractures of the greater and lesser tubercles, as well as by the Neer classification.
Introduction
Osteoporosis-related fractures affect ∼ 2 million people per year in the United States, and proximal humeral fractures (PHFs) account for 10% of these injuries.[1] Recent studies revealed that nonoperative treatment outcomes are similar to those obtained with surgery, regardless of the age and fracture pattern of the patient.[2] [3]
However, there are still controversies about the main fracture patterns benefiting from surgical treatment and little evidence regarding prognostic radiographic parameters for nonoperative treatment.
The Neer, Arbeitsgemeinschaft für Osteosynthesefragen (AO) and binary classification systems have low reliability and add little to the therapeutic decision-making process.[4] [5] [6] Previous studies demonstrate that functional outcomes are influenced by several fracture-related features that are not evaluated by these classification systems, such as medial metaphyseal comminution,[7] deviation type and degree in coronal and sagittal views, and bone loss due to impaction.[8] Other prognostic factors are related to the patient and the injury, such as age, osteoporosis and time from fracture to treatment.[9] [10]
Few studies evaluate different radiographic criteria to predict functional outcomes from the nonoperative treatment of deviated PHF.[8] [11] [12] [13] [14] [15] In addition, no previous study evaluates the Resch criteria and other radiographic variables in PHF prognosis.
The primary objective of the present study is to describe functional outcomes from the nonoperative treatment of deviated PHFs using the American Shoulder and Elbow Surgeons (ASES) score at a 12-month follow-up. The secondary objective is to evaluate whether different classification systems and initial radiographic measurements are related to worse outcomes according to the ASES score.
Methods
Study design
We conducted a prospective study involving 40 patients with deviated PHFs submitted to nonoperative treatment. The patients belong to a randomized study and were treated from February 2016 to October 2018 at a single center. The protocol was approved by the Ethics Committee of our service under the opinion number 1.266.876.
Subjects
The inclusion criteria were age ≥ 60 years, trauma within the last 30 days and PHF with surgical neck involvement and at least one of the following parameters: head-diaphysis angle with ≥ 20° deviation (in varus or valgus); head-to-shaft translation > 1 cm (in frontal or sagittal view) and greater and/or lesser tubercle fracture with > 0.5 cm deviation. Two physicians specialized in shoulder and elbow surgery evaluated these criteria before the patient was included in the study.
Dislocation-fractures, fractures with no contact between the humeral head and the diaphysis, and bilateral fractures were not included. Patients with ipsilateral or contralateral upper limb fractures, neurological injuries diagnosed at physical examination, other fractures in the affected limb, pathological fractures, bilateral fractures, previous surgery on the affected shoulder or previous full-thickness tear of one of the rotator cuff tendons were not included in the present study.
Intervention
The nonoperative treatment consisted of velpeau sling use and early rehabilitation. No patient underwent closed reduction. Analgesia was standardized with dipyrone (500 mg; one tablet every 8 hours for 10 days), codeine (30 mg; one tablet every 6 hours for 7 days and then as required, according to pain) and paracetamol (500 mg; one tablet each 8 hours for 10 days).
Guidance to sling use was standardized and each patient received a printed leaflet containing the rehabilitation guidelines described below after inclusion in the study. Home exercises were personally guided by a physical therapist on the 1st day of inclusion in the study.
Elbow, wrist, and hand movements started on the 1st day of inclusion in the study. Sleeping position, personal hygiene, and feeding modes were advised. Home cervical, scapular, elbow, wrist, and hand exercises were oriented on the 1st day of inclusion in the study; pendulum exercises were added on the 7th day. In 15 days, passive shoulder exercises for lifting, abduction and rotation were started. After 30 days, active-resisted elbow exercises, active-assisted and active-free shoulder exercises, as well as isometric exercises for the rotator cuff, the deltoid and the scapular girdle were started as tolerated by the patients. Active-resisted exercises for the rotator cuff, the deltoid and the scapular girdle began at the 45th day. The maximum time indicated for sling use was 30 days after the fracture.
Outcomes
The primary outcome consisted in clinical evaluation using the ASES score 12 months after the fracture. Secondary outcomes were the following: Constant-Murley score, both in absolute values and relative values for the contralateral limb (CRI) and the Single Assessment Numeric Evaluation (SANE) score. Scores were assessed at 3, 6 and 12 months after the fracture. Clinical scores were applied by an evaluator who did not participate in the physical rehabilitation or clinical follow-up of the patients.
Radiographs were obtained in four views, including the AP (anteroposterior) view, Y lateral view, axillary view and Velpeau views, whenever tolerated by the patient. Images were evaluated using the institutional image storage system (iSite enterprise 4.1, Phillips, Amsterdam, Netherlands). All patients underwent a computed tomography (CT) scan before study inclusion. The CT results complemented the definition of radiographic fracture variables, such as classifications and deviation features. Two orthopedists, members of the Brazilian Shoulder and Elbow Society, with 11 and 12 years of experience, evaluated all images and consensually determined ratings. The measurements used in the study were taken by one of these evaluators.
An ultrasound examination was performed 6 months after the fracture to assess rotator cuff integrity. Ultrasounds were obtained at the radiology department of the institution by the musculoskeletal radiologist team using a Logiq E9 device (GE Healthcare, Waukesha, WI, USA) with an ML6-15 linear transducer (6- to 15-MHz linear, ML-6-15, GE Healthcare, Waukesha, USA). Findings related to rotator cuff tendons were classified according to the full-thickness tear of one or more tendons.
Complications were noted according to their occurrence, and their total number was recorded separately for each individual patient. Vicious consolidation was not deemed a complication. The need for surgical approach and the type of surgery performed were also recorded. The following complications were analyzed as binary variables (present or absent) and were considered present if identified at any time during treatment: recurrent pain with functional limitations requiring additional treatment (clinical or surgical therapy) after 1 year of treatment; fracture-related clinical complication or treatment requiring hospitalization; death related to the fracture or treatment; re-fractures: shoulder stiffness, defined by decreased shoulder range of motion with sustained functional limitation 6 months after the fracture; complex regional pain syndrome; heterotopic ossification; glenohumeral osteoarthritis; and osteonecrosis of the humeral head and pseudoarthrosis, defined by the lack of consolidation 1 year after the fracture. Ancillary tests (CT, magnetic resonance imaging [MRI] or electroneuromyography) were requested per clinical suspicion.
Analyzed variables
The analyzed clinical variables were the following: gender, side, dominance, smoking status, diabetes, time until the beginning of rehabilitation, rehabilitation duration and number of sessions.
Radiographic variables included Neer and Resch classification systems and presence of tuberosity fracture (regardless of deviation), metaphyseal comminution, and medial periosteal lesion. Several radiographic parameters of fracture deviation were evaluated. The head-shaft angle was assessed as previously published.[16] Greater tuberosity deviation was evaluated according to the distance from the apex of the humeral head at a AP (anteroposterior) view radiograph. The lesser tuberosity was evaluated on axillary or velpeau views if the fragment was deviated. Other measures were taken in relation to fragment deviation. All measures were categorized into three levels according to previously established criteria. [Table 1] describes all analyzed radiographic variables.
|
Metaphyseal comminution |
|---|
|
No |
|
Yes |
|
Medial periosteal lesion |
|
No |
|
Yes |
|
Tuberosity fracture |
|
No tuberosity fracture |
|
Greater tuberosity fracture |
|
Lesser and greater tuberosities fracture |
|
Greater tuberosity deviation |
|
Up to 2 mm inferior to the top of the humeral head |
|
Up to 2 mm superior to the top of the humeral head |
|
Over 2 mm from the top of the humeral head |
|
Lesser tuberosity deviation |
|
Up to 2 mm |
|
2 to 5 mm |
|
> 5 mm |
|
Diaphyseal head angle, front view |
|
125° to 150° |
|
110° to 124° or 151° to 165° |
|
< 110° or >166° |
|
Diaphyseal head angle, lateral view |
|
No deviation |
|
Moderate (0-20°) |
|
Severe (> 45°) |
|
Diaphyseal deviation, front view |
|
Up to 5 mm |
|
5 to 10 mm |
|
> 10 mm |
|
Diaphyseal deviation, lateral view |
|
Up to 5 mm |
|
5 to 10 mm |
|
> 10 mm |
Statistical analysis
Due to the sample size, nonparametric tests were used regardless of data normality. Continuous variables were presented as mean and standard deviation (SD), median and interquartile range values. Categorical values were shown as absolute and percentage values. The sample was calculated for convenience and cases were included sequentially.
Functional scores before and after treatment were compared using Wilcoxon tests. Kruskal-Wallis tests were performed for univariate analyzes of radiographic variables, and the Friedman test was used for post-hoc analysis.
Data was analyzed in IBM SPSS Statistics for Windows, Version 20.0 (IBM Corp., Armonk, NY, USA) adopting a 5% significance level.
Results
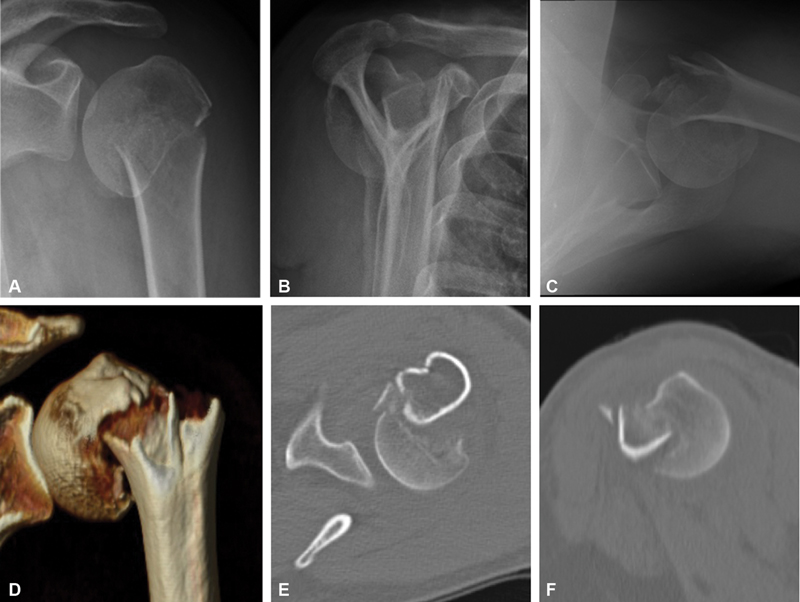
Forty-five patients were included for nonoperative treatment. Five patients did not show up for the first assessment at 3 months, with complete loss to follow-up. Forty patients with a complete 12-month follow-up were included at the final evaluation. [Table 2] shows general sample data. Most patients were female, with a mean age of 69 ± 6 years old. [Figures 1], [2] and [3] show radiographic and clinical outcomes from one patient. The mean time until the beginning of physical therapy was 21 ± 12 days; the mean duration of rehabilitation was 111 ± 51 days, with 18 ± 10 sessions. The mean ASES score in patients who started physical therapy more than 15 days after the fracture was 72 ± 25 points, whereas patients who started rehabilitation within 15 days presented a mean ASES score of 79.9 ± 23.4 points.
|
n |
% |
|
|---|---|---|
|
Gender |
||
|
Male |
7 |
17.5 |
|
Female |
33 |
82.5 |
|
Side |
||
|
Right |
13 |
32.5 |
|
Left |
27 |
67.5 |
|
Dominant side affected? |
||
|
Yes |
15 |
37.5 |
|
No |
25 |
62.5 |
|
Smoking |
||
|
No |
31 |
77.5 |
|
Smoker |
7 |
17.5 |
|
Former smoker |
2 |
5.0 |
|
Diabetes |
||
|
No |
30 |
75.0 |
|
Yes, non-insulin-dependent |
8 |
20.0 |
|
Yes, insulin-dependent |
2 |
5.0 |


The ASES score at 12 months was 77.7 ± 23.2 points for the entire sample, improving over time. At 12 months, the mean absolute Constant-Murley score was 68.7 ± 16 points, with 82.6% for the contralateral side. The SANE score at 12 months was 84.8 ± 19 points. [Table 3] shows clinical outcomes.
|
n |
Mean |
Standard deviation |
Median |
IQR |
|
|---|---|---|---|---|---|
|
ASES |
|||||
|
3 months |
39 |
57.7 |
24.5 |
56.3 |
42.8 |
|
6 months |
39 |
71.6 |
24.3 |
80.7 |
36.0 |
|
12 months |
40 |
77.7 |
23.2 |
85.2 |
40.1 |
|
SANE |
|||||
|
3 months |
39 |
66.2 |
22.6 |
70.0 |
40.0 |
|
6 months |
39 |
82.2 |
19.4 |
85.0 |
22.5 |
|
12 months |
40 |
84.8 |
19.0 |
90.0 |
20.0 |
|
Constant-Murley |
|||||
|
3 months |
39 |
55.6 |
16.7 |
60.0 |
31.0 |
|
6 months |
40 |
64.8 |
15.9 |
68.5 |
28.5 |
|
12 months |
40 |
68.7 |
16.0 |
72.0 |
24.0 |
|
Relative Constant score for the contralateral limb |
|||||
|
6 months |
39 |
80.1% |
18.7% |
87.2% |
37.8% |
|
12 months |
39 |
82.6% |
23.6% |
89.5% |
31.3% |
Ultrasonography was performed in 37 patients (92.5%). Full-thickness tears of the rotator cuff were observed in eight subjects. The mean ASES score in patients presenting cuff tear was 76.9 ± 24.0 points at 12 months, with no statistically significant difference compared with patients with no cuff injuries (p = 0.188).
Eight patients (20%) had complications, including 4 cases of osteonecrosis (10%), 2 cases of pseudarthrosis (5%) and 2 cases of persistent stiffness (5%). No patient chose for a surgical approach to treat complications. [Figure 3] shows an osteonecrosis case and [Figure 4] demonstrates a pseudoarthrosis case. The mean ASES score in patients with complications was 53.8 ± 23.0 points.

The analysis of radiographic variables revealed the negative influence of the following parameters on the clinical outcome according to the ASES score at 12 months: severity according to the Neer classification and angular deviation at the coronal plane (measured by the head-diaphysis angle) and tuberosity fracture. The remaining radiographic variables did not influence functional outcomes according to the ASES score. [Table 4] shows a subgroup analysis for the main variables of the present study.
|
ASES score at 12 months |
|||||
|---|---|---|---|---|---|
|
Mean |
Standard deviation |
Median |
IQR |
p-value |
|
|
Neer classification |
|||||
|
2 parts |
88.4 |
15.4 |
94.2 |
19.9 |
|
|
3 parts |
79.0 |
21.5 |
85.2 |
32.3 |
|
|
4 parts |
61.0 |
28.3 |
47.5 |
56.0 |
0.031 |
|
Diaphyseal head angle, coronal view |
|||||
|
125° to 150° |
93.4 |
7.8 |
96.3 |
11.9 |
|
|
110° to 124° or 151° a 165° |
74.5 |
25.2 |
78.4 |
45.4 |
|
|
< 110° or >166° |
64.3 |
25.0 |
56.5 |
48.2 |
0.004 |
|
Angular deviation, coronal view |
|||||
|
Minimal deviation |
84.7 |
20.4 |
93.8 |
26.1 |
|
|
Severe valgus (>166°) |
60.0 |
22.3 |
58.1 |
41.9 |
|
|
Severe varus (<110°) |
66.2 |
27.1 |
56.5 |
54.9 |
0.034 |
|
Tuberosity fracture |
|||||
|
No tuberosity fracture |
84.7 |
19.7 |
94.2 |
38.4 |
|
|
Greater tuberosity fracture |
82.8 |
20.3 |
88.1 |
27.5 |
|
|
Lesser and greater tuberosities fracture |
61.5 |
26.9 |
50.4 |
54.6 |
0.031 |
|
Resch classification |
|||||
|
1 |
94.2 |
6.4 |
95.9 |
12.6 |
|
|
2 |
88.1 |
16.8 |
88.1 |
NA |
|
|
3 |
64.4 |
27.1 |
61.5 |
53.0 |
|
|
4 |
76.2 |
23.7 |
84.9 |
44.8 |
0.052 |
|
Metaphyseal comminution |
|||||
|
No |
75.8 |
23.7 |
85.4 |
49.7 |
|
|
Yes |
77.7 |
25.2 |
85.0 |
36.7 |
0.570 |
|
Medial periosteal lesion |
|||||
|
No |
82.9 |
22.3 |
93.2 |
27.3 |
|
|
Yes |
71.6 |
24.7 |
78.5 |
51.7 |
0.168 |
Discussion
Our results demonstrate that even fractures with significant tuberosity or humeral head deviation can be treated nonoperatively. The Constant-Murley score for the contralateral side was 82.6%, consistent with other studies on nonoperative treatment,[8] [11] [12] [13] [14] as well as with the surgical treatment using arthroplasty or locked plate fixation.[17] [18] [19] [20] Subjective scores (i.e., ASES and SANE) were similar to those reported in systematic reviews.[2] Our results reinforce findings from the Proximal Fracture of the Humerus Evaluation by Randomization (PROFHER) study and a Cochrane systematic review demonstrating that nonoperative treatment can provide good functional outcomes even in deviated fractures.[2] [3]
In a systematic review, Sabharwal et al.[21] obtained similar clinical outcomes with both treatments. However, these authors demonstrated that, in more complex, four-part fractures, the surgical treatment resulted in better clinical outcomes and a lower rate of complications. They highlighted the need for future studies with specific fracture subtypes.
Few investigations evaluated the influence of the classification and deviation criteria defined by Neer on the nonoperative treatment of PHF.[8] [14] Although routinely used as criteria to indicate surgical treatment, a 45° angular deviation, 1 cm translational deviation and 0.5 cm tuberosity deviation were arbitrarily defined, as explained by Neer himself in 2002.[22]
Our secondary objective was to evaluate not only the deviation criteria described by Neer, but also several other radiographic parameters. The classification recently described by Resch et al.[23] has better inter- and intraobserver reliability when compared with the Neer system, but its potential in determining prognosis has not been evaluated yet.[6]
Univariate analyses revealed statistically significant, clinically relevant differences for some radiographic variables, mainly angular deviation, assessed by the head-diaphysis angle, and greater and lesser tuberosity fracture, regardless of its deviation. The mean ASES score in patients with greater and lesser tuberosity fractures was 23 points, a clinically significant relevant finding. Patients with deviated, four-part fractures according to Neer presented worse outcomes, consistent with Yüksel et al.;[14] however, there was no statistically significant difference in two- or three-part fractures.
The head-diaphysis angle may be difficult to be evaluated on radiographs of acute fractures and presents variable interobserver correlation.[16] [24] Nevertheless, with an adequate radiographic standardization and the potential use of CT scans, the head-diaphysis angle is an important parameter to aid the decision-making process, as it directly influences clinical outcomes. Patients with < 110° or > 166° had 29 points less on the ASES score when compared with subjects with minimal angular deviation (125° to 150°). Yüksel et al.[14] did not observe such influence on the Constant-Murley score, with similar results between valgus or varus impacted fractures < 110°.
Comparing only the mean head-diaphysis angles can lead to incorrect interpretations when fractures with varus and valgus deviation are included, as it approximates figures from opposite ends. The categorized analysis, such as the one performed in our study, or separated by valgus or varus deviations, avoids evaluation bias. In contrast to Court-Brown et al.,[12] in our sample, subjects with deviated fractures in severe valgus (> 166°) had lower ASES scores compared to those with severe varus (< 110°), but there was no statistically significant difference. Consistent with our findings, Foruria et al.[8] demonstrated that valgus impacted fractures had a three-fold higher risk of worsening 10 points on the Disability of Arm, Shoulder, and Hand (DASH) score when compared with varus impacted injuries.
Other factors did not show a statistically significant difference. The most prominent factor was the presence or absence of metaphyseal comminution, medial periosteal lesion, and deviations at the sagittal plane. Some studies[25] [26] observed worse outcomes regarding stability after plate fixation in patients with posteromedial metaphyseal comminution, but no study has evaluated the importance of this finding in the nonoperative treatment.
We were unable to detect a statistically significant difference in functional scores for the classification described by Resch et al.[23] Nevertheless, mean values for subtypes in valgus (type 3) and varus (type 4) were lower than types 1 and 2.
Rehabilitation-related variables showed no difference in subgroup analyzes either for time until the start of rehabilitation and its total duration and number of sessions.
As for rotator cuff injuries, there was no relationship between injury and worse clinical outcomes. Although we did not include patients with previous rotator cuff injury, it is possible that some cases were asymptomatic lesions, explaining the high rate observed in our sample. In addition, ultrasound scans in patients with fracture sequelae may be less accurate due to mobility limitations or deformities.
Rotator cuff tears did not influence the clinical outcome according to the ASES score in our sample.
Our study has some limitations. Since the sample size is relatively small for multivariate analysis, these radiographic factors were submitted to a univariate analysis, which can increase the risk of confounding factors. However, this is a homogeneous sample consisting of patients with similar features.
As positive points, this is a prospective clinical and radiographic evaluation, in standardized times, with an evaluator who did not participate in the study and did not follow-up the patients. All fractures included had significant deviations, which could be considered an indication for surgical treatment; there were no fractures with no or minimal deviation in this investigation. Our results can assist the decision-making process between non-operative and surgical treatment for some specific patterns of PHFs.
Conclusion
Nonoperative treatment of deviated PHFs in elderly patients had good clinical outcomes. These outcomes were negatively influenced by the Neer classification, the angular deviation of the humeral head and the presence of greater and lesser tuberosities fractures.
Conflito de Interesses
Os autores declaram não haver conflito de interesses.
Dr. Gracitelli relata honorários pessoais da Arthrex, fora do trabalho submetido.
Financial Support
There was no financial support from public, commercial, or non-profit sources.
* Study developed at the Instituto de Ortopedia e Traumatologia, Hospital das Clínicas, Faculdade de Medicina, Universidade de São Paulo, São Paulo, SP, Brazil.
-
Referências
- 1 Palvanen M, Kannus P, Niemi S, Parkkari J. Update in the epidemiology of proximal humeral fractures. Clin Orthop Relat Res 2006; 442 (442) 87-92
- 2 Handoll HHG, Brorson S. Interventions for treating proximal humeral fractures in adults. Cochrane Database Syst Rev 2015; (11) CD000434
- 3 Rangan A, Handoll H, Brealey S. et al. PROFHER Trial Collaborators. Surgical vs nonsurgical treatment of adults with displaced fractures of the proximal humerus: the PROFHER randomized clinical trial. JAMA 2015; 313 (10) 1037-1047
- 4 Majed A, Macleod I, Bull AMJ. et al. Proximal humeral fracture classification systems revisited. J Shoulder Elbow Surg 2011; 20 (07) 1125-1132
- 5 Bernstein J, Adler LM, Blank JE, Dalsey RM, Williams GR, Iannotti JP. Evaluation of the Neer system of classification of proximal humeral fractures with computerized tomographic scans and plain radiographs. J Bone Joint Surg Am 1996; 78 (09) 1371-1375
- 6 Gracitelli MEC, Dotta TAG, Assunção JH. et al. Intraobserver and interobserver agreement in the classification and treatment of proximal humeral fractures. J Shoulder Elbow Surg 2017; 26 (06) 1097-1102
- 7 Krappinger D, Bizzotto N, Riedmann S, Kammerlander C, Hengg C, Kralinger FS. Predicting failure after surgical fixation of proximal humerus fractures. Injury 2011; 42 (11) 1283-1288
- 8 Foruria AM, de Gracia MM, Larson DR, Munuera L, Sanchez-Sotelo J. The pattern of the fracture and displacement of the fragments predict the outcome in proximal humeral fractures. J Bone Joint Surg Br 2011; 93 (03) 378-386
- 9 Südkamp NP, Audigé L, Lambert S, Hertel R, Konrad G. Path analysis of factors for functional outcome at one year in 463 proximal humeral fractures. J Shoulder Elbow Surg 2011; 20 (08) 1207-1216
- 10 Siebenbürger G, Van Delden D, Helfen T, Haasters F, Böcker W, Ockert B. Timing of surgery for open reduction and internal fixation of displaced proximal humeral fractures. Injury 2015; 46 (Suppl. 04) S58-S62
- 11 Court-Brown CM, Garg A, McQueen MM. The translated two-part fracture of the proximal humerus. Epidemiology and outcome in the older patient. J Bone Joint Surg Br 2001; 83 (06) 799-804
- 12 Court-Brown CM, McQueen MM. The impacted varus (A2.2) proximal humeral fracture: prediction of outcome and results of nonoperative treatment in 99 patients. Acta Orthop Scand 2004; 75 (06) 736-740
- 13 Court-Brown CM, Cattermole H, McQueen MM. Impacted valgus fractures (B1.1) of the proximal humerus. The results of non-operative treatment. J Bone Joint Surg Br 2002; 84 (04) 504-508
- 14 Yüksel HY, Yılmaz S, Akşahin E, Celebi L, Muratli HH, Biçimoğlu A. The results of nonoperative treatment for three- and four-part fractures of the proximal humerus in low-demand patients. J Orthop Trauma 2011; 25 (10) 588-595
- 15 Hanson B, Neidenbach P, de Boer P, Stengel D. Functional outcomes after nonoperative management of fractures of the proximal humerus. J Shoulder Elbow Surg 2009; 18 (04) 612-621
- 16 Malavolta EA, Assunção JH, Pagotto RA. et al. The rotation of the humeral head does not alter radiographic evaluation of the head-shaft angle. J Shoulder Elbow Surg 2016; 25 (04) 543-547
- 17 Miyazaki AN, Fregoneze M, Santos PD. et al. Results of open reduction and internal fixation of severe fractures of the proximal humerus in elderly patients. Rev Bras Ortop 2014; 49 (01) 25-30
- 18 Gracitelli MEC, Lobo FL, Ferreira GMA. et al. Outcomes evaluation of locking plate osteosynthesis in displaced fractures of the proximal humerus. Rev Bras Ortop 2013; 48 (06) 491-499
- 19 Ferrel JR, Trinh TQ, Fischer RA. Reverse total shoulder arthroplasty versus hemiarthroplasty for proximal humeral fractures: a systematic review. J Orthop Trauma 2015; 29 (01) 60-68
- 20 Brandão BL, Amaral MVG, Cohen M. et al. Treatment of complex acute proximal humerus fractures using hemiarthroplasty. Rev Bras Ortop 2013; 48 (01) 29-35
- 21 Sabharwal S, Patel NK, Griffiths D, Athanasiou T, Gupte CM, Reilly P. Trials based on specific fracture configuration and surgical procedures likely to be more relevant for decision making in the management of fractures of the proximal humerus: Findings of a meta-analysis. Bone Joint Res 2016; 5 (10) 470-480
- 22 Neer II CS. Four-segment classification of proximal humeral fractures: purpose and reliable use. J Shoulder Elbow Surg 2002; 11 (04) 389-400
- 23 Resch H, Tauber M, Neviaser RJ. et al. Classification of proximal humeral fractures based on a pathomorphologic analysis. J Shoulder Elbow Surg 2016; 25 (03) 455-462
- 24 Assunção JH, Malavolta EA, Beraldo RA, Gracitelli MEC, Bordalo-Rodrigues M, Ferreira Neto AA. Impact of shoulder rotation on neck-shaft angle: A clinical study. Orthop Traumatol Surg Res 2017; 103 (06) 865-868
- 25 Osterhoff G, Hoch A, Wanner GA, Simmen HP, Werner CML. Calcar comminution as prognostic factor of clinical outcome after locking plate fixation of proximal humeral fractures. Injury 2012; 43 (10) 1651-1656
- 26 Ponce BA, Thompson KJ, Raghava P. et al. The role of medial comminution and calcar restoration in varus collapse of proximal humeral fractures treated with locking plates. J Bone Joint Surg Am 2013; 95 (16) e113 , 1–7
Endereço para correspondência
Publication History
Received: 07 March 2020
Accepted: 06 July 2020
Article published online:
02 November 2020
© 2020. Sociedade Brasileira de Ortopedia e Traumatologia. This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commecial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/)
Thieme Revinter Publicações Ltda.
Rua do Matoso 170, Rio de Janeiro, RJ, CEP 20270-135, Brazil
-
Referências
- 1 Palvanen M, Kannus P, Niemi S, Parkkari J. Update in the epidemiology of proximal humeral fractures. Clin Orthop Relat Res 2006; 442 (442) 87-92
- 2 Handoll HHG, Brorson S. Interventions for treating proximal humeral fractures in adults. Cochrane Database Syst Rev 2015; (11) CD000434
- 3 Rangan A, Handoll H, Brealey S. et al. PROFHER Trial Collaborators. Surgical vs nonsurgical treatment of adults with displaced fractures of the proximal humerus: the PROFHER randomized clinical trial. JAMA 2015; 313 (10) 1037-1047
- 4 Majed A, Macleod I, Bull AMJ. et al. Proximal humeral fracture classification systems revisited. J Shoulder Elbow Surg 2011; 20 (07) 1125-1132
- 5 Bernstein J, Adler LM, Blank JE, Dalsey RM, Williams GR, Iannotti JP. Evaluation of the Neer system of classification of proximal humeral fractures with computerized tomographic scans and plain radiographs. J Bone Joint Surg Am 1996; 78 (09) 1371-1375
- 6 Gracitelli MEC, Dotta TAG, Assunção JH. et al. Intraobserver and interobserver agreement in the classification and treatment of proximal humeral fractures. J Shoulder Elbow Surg 2017; 26 (06) 1097-1102
- 7 Krappinger D, Bizzotto N, Riedmann S, Kammerlander C, Hengg C, Kralinger FS. Predicting failure after surgical fixation of proximal humerus fractures. Injury 2011; 42 (11) 1283-1288
- 8 Foruria AM, de Gracia MM, Larson DR, Munuera L, Sanchez-Sotelo J. The pattern of the fracture and displacement of the fragments predict the outcome in proximal humeral fractures. J Bone Joint Surg Br 2011; 93 (03) 378-386
- 9 Südkamp NP, Audigé L, Lambert S, Hertel R, Konrad G. Path analysis of factors for functional outcome at one year in 463 proximal humeral fractures. J Shoulder Elbow Surg 2011; 20 (08) 1207-1216
- 10 Siebenbürger G, Van Delden D, Helfen T, Haasters F, Böcker W, Ockert B. Timing of surgery for open reduction and internal fixation of displaced proximal humeral fractures. Injury 2015; 46 (Suppl. 04) S58-S62
- 11 Court-Brown CM, Garg A, McQueen MM. The translated two-part fracture of the proximal humerus. Epidemiology and outcome in the older patient. J Bone Joint Surg Br 2001; 83 (06) 799-804
- 12 Court-Brown CM, McQueen MM. The impacted varus (A2.2) proximal humeral fracture: prediction of outcome and results of nonoperative treatment in 99 patients. Acta Orthop Scand 2004; 75 (06) 736-740
- 13 Court-Brown CM, Cattermole H, McQueen MM. Impacted valgus fractures (B1.1) of the proximal humerus. The results of non-operative treatment. J Bone Joint Surg Br 2002; 84 (04) 504-508
- 14 Yüksel HY, Yılmaz S, Akşahin E, Celebi L, Muratli HH, Biçimoğlu A. The results of nonoperative treatment for three- and four-part fractures of the proximal humerus in low-demand patients. J Orthop Trauma 2011; 25 (10) 588-595
- 15 Hanson B, Neidenbach P, de Boer P, Stengel D. Functional outcomes after nonoperative management of fractures of the proximal humerus. J Shoulder Elbow Surg 2009; 18 (04) 612-621
- 16 Malavolta EA, Assunção JH, Pagotto RA. et al. The rotation of the humeral head does not alter radiographic evaluation of the head-shaft angle. J Shoulder Elbow Surg 2016; 25 (04) 543-547
- 17 Miyazaki AN, Fregoneze M, Santos PD. et al. Results of open reduction and internal fixation of severe fractures of the proximal humerus in elderly patients. Rev Bras Ortop 2014; 49 (01) 25-30
- 18 Gracitelli MEC, Lobo FL, Ferreira GMA. et al. Outcomes evaluation of locking plate osteosynthesis in displaced fractures of the proximal humerus. Rev Bras Ortop 2013; 48 (06) 491-499
- 19 Ferrel JR, Trinh TQ, Fischer RA. Reverse total shoulder arthroplasty versus hemiarthroplasty for proximal humeral fractures: a systematic review. J Orthop Trauma 2015; 29 (01) 60-68
- 20 Brandão BL, Amaral MVG, Cohen M. et al. Treatment of complex acute proximal humerus fractures using hemiarthroplasty. Rev Bras Ortop 2013; 48 (01) 29-35
- 21 Sabharwal S, Patel NK, Griffiths D, Athanasiou T, Gupte CM, Reilly P. Trials based on specific fracture configuration and surgical procedures likely to be more relevant for decision making in the management of fractures of the proximal humerus: Findings of a meta-analysis. Bone Joint Res 2016; 5 (10) 470-480
- 22 Neer II CS. Four-segment classification of proximal humeral fractures: purpose and reliable use. J Shoulder Elbow Surg 2002; 11 (04) 389-400
- 23 Resch H, Tauber M, Neviaser RJ. et al. Classification of proximal humeral fractures based on a pathomorphologic analysis. J Shoulder Elbow Surg 2016; 25 (03) 455-462
- 24 Assunção JH, Malavolta EA, Beraldo RA, Gracitelli MEC, Bordalo-Rodrigues M, Ferreira Neto AA. Impact of shoulder rotation on neck-shaft angle: A clinical study. Orthop Traumatol Surg Res 2017; 103 (06) 865-868
- 25 Osterhoff G, Hoch A, Wanner GA, Simmen HP, Werner CML. Calcar comminution as prognostic factor of clinical outcome after locking plate fixation of proximal humeral fractures. Injury 2012; 43 (10) 1651-1656
- 26 Ponce BA, Thompson KJ, Raghava P. et al. The role of medial comminution and calcar restoration in varus collapse of proximal humeral fractures treated with locking plates. J Bone Joint Surg Am 2013; 95 (16) e113 , 1–7



