

Subscribe to RSS
DOI: 10.1055/s-0041-1734374
Challenges in Image-Guided Drainage of Infected Pleural Collections: A Review
Authors


Abstract
Infected pleural fluid collections (IPFCs) commonly occur as a part of bacterial, fungal, or tubercular pneumonia or due to involvement of pleura through hematogenous route. Management requires early initiation of therapeutic drugs, as well as complete drainage of the fluid, to relieve patients' symptoms and prevent pleural fibrosis. Image-guided drainage plays an important role in achieving these goals and improving outcomes. Intrapleural fibrinolytic therapy (IPFT) is also a vital component of the management. The concepts of image-guided drainage procedures, IPFT, and nonexpanding lung are discussed in this review.
Introduction
Infected pleural fluid collections (IPFCs) can be the result of various organisms, the most frequent being bacterial or mycobacterial (tubercular), much less frequently fungal, and are rare in viral infections. This article focuses on IPFCs associated with bacterial pneumonia. In other forms of IPFCs caused by organisms, such as tuberculosis/fungi, basic presentation and treatment remain the same but recommendations may vary in terms of time of intervention. IPFCs associated with bacterial pneumonia may develop in the setting of community-acquired pneumonia (CAP), as well in hospital-acquired pneumonia (HAP). Pneumonia can be complicated by parapneumonic effusion, complicated parapneumonic effusion (CPE), or empyema which are defined subsequently. However, there are a significant number of cases of empyema or CPE that do not have an underlying pneumonia. Moreover, their bacteriologic spectra are not always similar. Other possible causes of empyema include hematogenous spread of infection and contiguous spread from subdiaphragmatic pathologies and trauma.[1] [2] [3] [4]
Management of CPE or empyema requires early and complete drainage, not only to relieve the patient's symptoms but also to prevent long-term complications of pleural fibrosis, resulting in compromised pulmonary function. Notable existing guidelines in terms of management include those of the British Thoracic Society (BTS)[5] and American Academy for Thoracic Surgeons (AATS).[6] The purpose of this review is to highlight key concepts and knowledge essential for optimal interventional radiology (IR) management of CPEs and empyema, to improve short- and long-term patient outcomes.
Diagnosis and Terminology
A concept that needs to be understood is that not all infected pleural fluid collections are empyemas. These could also be complicated parapneumonic/synpneumonic effusions. The differences between these two entities are illustrated in [Table 1].[7] [8] [9] [10] Further, terms which are employed are related to the clinical settings in which the empyema occurs. These are very similar to the settings of the underlying pneumonia. For example, CPE occurs as a complication of CAP, while health care associated empyema (HCAE) is associated with HAP.
While the detection of IPFCs is largely clinical ± imaging based, the diagnosis of empyema versus CPE relies largely on the pleural fluid aspiration. Pleural effusions associated with an underlying pneumonia should have a diagnostic tap, if the pneumonia does not respond to 48 to 72 hours of antibiotic treatment.[5] [11] A diagnostic tap should also be performed if a patient with sepsis has a pleural fluid of >10-mm thickness on chest radiograph/ultrasound or >20 mm on computed tomography (CT)[6]; or in elderly patients. The aspirated fluid may be serous/serosanguinous or frank pus. The analysis of pleural fluid has two components: biochemical and microbiological.
Biochemical analysis depends on pleural fluid pH, glucose, and lactate dehydrogenase (LDH). It should be kept in mind that the yield of pleural fluid in cases of CPE may only be approximately 50%, whereas blood cultures are reported to have higher yield. Whenever possible, blood culture specimens should also be obtained. Several ways have been described to enhance the microbiological yield of pleural fluid, such as direct inoculation of the pleural fluid, into a blood culture bottle after aspiration at the bedside. Another method is adopting Polymerase chain reaction (PCR) technique for pleural fluid samples/biopsy. This is especially useful for anaerobes. However, since the microbiological confirmation rate is markedly low, empiric antibiotic therapy is often started depending on the specific clinical scenario. Microbiological analysis of empyema/CPE fluid may yield variable bacteriologic spectra. While Streptococcus predominates the CAP fluid, methicillin-resistant Staphylococcus aureus (MRSA) and gram negative and anaerobic bacteria constitute a large part in HCAE.[10] [12] [13]
Imaging of Infected Pleural Fluid Collections
While the complete discussion of this topic is beyond the scope of this review, imaging is critical in detection, quantification, guiding drainage, and follow-up.
Quantification of Pleural Fluid Collection
Quantification of pleural fluid guides the decision for drainage. Pleural effusions can be quantified on ultrasound and CT using various methods which are summarized in [Table 2]. On ultrasound, the Goecke 2 formula measured in erect position of the patient is reported to most closely correlate with actual fluid drained. Ultrasonography (USG) image is obtained keeping probe longitudinally oriented along dorsolateral/posterolateral aspect of chest wall, and craniocaudal extent (X) and the lung base to middiaphragm distance (LDD)/subpulmonary height is measured. Volume of effusion is measured using formula “estimated volume (EV) mL = (X + LDD) × 70”[14] ([Fig. 1A–D]).
Abbreviations: AP, anteroposterior; CT, computed tomography; IPFC, infected pleural fluid collection; LDD, lung to diaphragm distance; USG, ultrasonography.

Computed tomography: one method is to measure anteroposterior (AP) depth at the midclavicular line on axial CT image where the maximum fluid is seen and quantify according to [Table 2] ( [Fig. 1E] ). Another method is to divide hemithorax in a quartile wherein first AP quartile represents 0 to 25% fluid occupying the hemithorax and suggest effusions are small, second AP quartile represents 25 to 50% effusions that are moderate, and third 50 to 75% or fourth 75 to 100% AP-quartile effusions are large[15] ( [Fig. 1F] ). CT volumetry software tool may also be used for estimation.
Staging of Infected Pleural Fluid Collection
Empyema is diagnosed on CT when there is a pleural fluid collection with enhancing visceral and parietal pleural layers, giving rise to “split pleura sign.” Classically, IPFC has been divided into three stages; exudative phase, fibrinopurulent stage, and empyema stage.[16] CT findings indicating the stages[17] are shown in [Table 3] and [Fig. 2] . CPE on USG may appear as clear fluid or fluid with fine internal echoes and on CT may show early pleural thickening.
Abbreviations: CT, computed tomography; IPFC, infected pleural fluid collection.

However, the imaging findings may not always correspond to empyema in pleural fluid analysis. The final diagnosis is made by thoracentesis. Sinusoid sign on USG represents the appearance of wavy pattern on M-mode demonstrated when the visceral and parietal pleura are separated by free fluid ( [Fig. 3] ). It may be absent when there is a dense or multiseptated collection.

Management
Management of IPFCs has two main modalities: surgery and percutaneous intervention (tube drainage and intrapleural fibrinolytic therapy [IPFT]). Most available literature suggests surgery as the second line management option, after failure of conservative management or tube thoracostomy. Exceptions to this are presence of sepsis or septic shock or a suspected lung abscess. Very few trials analyzed the efficacy of upfront minimally invasive video-assisted thoracic surgery (VATS) in comparison to tube drainage.[18] This article will describe the interventional management: goals of treatment are two folds, relieving sepsis and preventing long-term complications (e.g., fibrosis and trapped lung).
Time to Intervene
Timing and nature of surgery is beyond the scope of this article. Interventional management is discussed here. However, not every parapneumonic effusion needs drainage. If the effusion is mild and the patient is responding to antibiotics, it should not be drained. Unlike diagnostic tap, no volume cut-off is available for IPFT.
Parapneumonic effusion has classically been described to evolve through three stages: exudative, fibrinopurulent, and organizing.[19] The time duration of each stage is variable, and delay in thoracentesis may result in increased morbidity. The diagnostic thoracentesis should be performed proactively in the earliest suspicion of nonresponse to antibiotics (see “Diagnosis and Terminology”). Similarly, a tube thoracostomy should also be performed at an early stage of the disease, so as to avoid subsequent complications.[20] [21]
Tube Drainage
While surgical drainage enables one to use larger bore tubes (up to 32–40 Fr), image-guided drainage is typically described to suffer from the drawback of smaller size of the tubes. Though there is no consensus on the size of the optimal chest tube for drainage, for most IPFCs, a small-bore catheter of size 10 to 14 F will be adequate. With the advances in percutaneous drainage tube technology, larger bore tubes, even up to 32 Fr (Thal-Quick, Cook Medical, United States),[22] are now available and can be used for thick stubborn collection not responding to small bore catheter drainage. In cases with rib crowding, it is advisable to measure the intercostal space and calculate tube size accordingly. Pigtail catheter is commonly preferred due to the presence of multiple side holes. Malecot catheter is also another preferred self-retaining drainage catheter.
Technique principles of standard trocar and Seldinger's techniques of tube insertions are similar to all drainage procedures elsewhere in the body. Complete discussion of the techniques is beyond the scope of this review. A few points specific to thoracic drainage are emphasized. Standard site of catheter insertion is along the midaxillary line in fifth or sixth intercostal space and direction of insertion being superior to inferior. However in case of loculated effusions, such universal approach will have to be modified according to site of loculation. Care should be taken that no air is introduced into the pleural space during entire procedure and use of three ways are helpful. After the catheter is placed, it should be connected to an underwater seal drainage bag. USG along with fluoroscopy is a good combination modality for guiding the procedure. CT also can be adapted accordingly, especially in case of rib crowding and when USG visualization is poor.
Outcome of empyema having frank pus vis-a-vis CPE may not be largely different. Whereas it has been demonstrated that frank pus does not essentially imply a tube thoracostomy failure, absence of pus is usually associated with a good outcome of tube thoracostomy.[21] [22] [23] [24] [25] [26] Larger bore tubes have higher pain scores but offer no additional advantage in terms of prevention of surgical intervention or mortality.
Catheter removal: although literature states, for removal of tube, the output volume to be 200 ml/day in general,[27] the decision of tube removal in clinical practice is based on combination of factors such as radiological reduction in size of pleural fluid collection, clinical resolution of sepsis, and fever with no significant drainage output for 48 to 72 hours. Hence, the catheter can be retained even with output <200 mL/day, as several of these collections do not have large volumes.
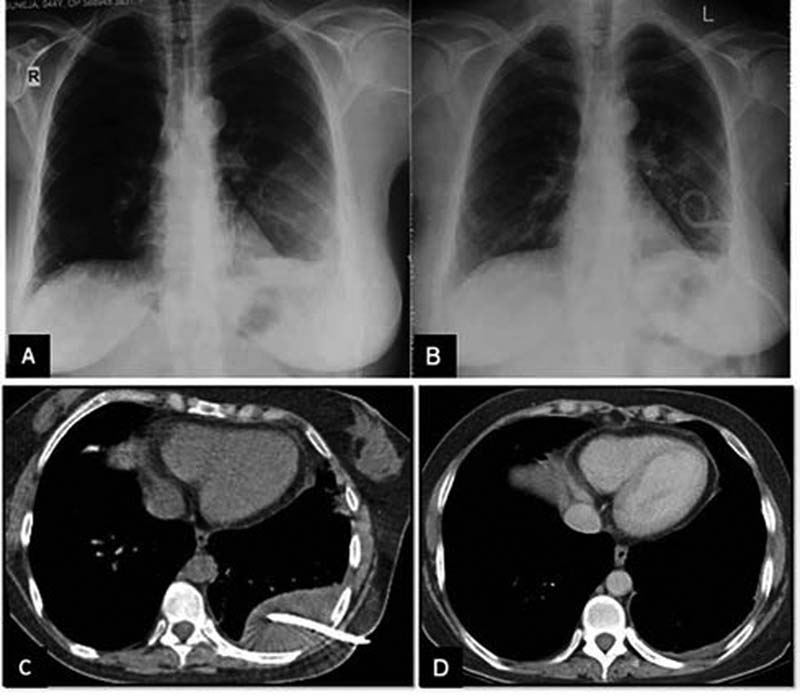
Reasons for inadequate drainage include thick, viscous collection and presence of loculations. Postinsertion monitoring consists of output monitoring, checking for any tube kink and regular flushing of the tube. Simple saline irrigation has been proven to be useful.[28] It has been found superior to tube drainage alone. Thrice daily irrigation with 200 mL of saline for 3 days is recommended.[28] Due to improper fixing or accidental misplacement, there may be tube displacement ( [Fig. 4] ). Repeat chest X-ray (CXR) can be helpful. In the authors' experience, a low-dose CT can be used in the follow-up before repositioning of catheters.

Intrapleural Fibrinolytic Therapy
While IPFT forms an important component in the management of IPFCs, their use is very variable among institutions. This topic will be discussed under the following headings: Indications, choice of pharmacologic agent, benefits, adverse effects, and cost-effectiveness issues.
Indications
The primary indication for IPFT is organizing phase of empyema with loculations and fibrin deposition which may not resolve completely with tube thoracostomy alone; resulting in nonexpansion of underlying lung. IPFT aims to lyse the loculations caused by fibrin deposition.
Choice of Pharmacologic Agent
Streptokinase/urokinase are the pharmacologic agents used in the earlier trial (multicenter intrapleural sepsis trial [MIST] 1). In comparison to placebo, they were not found to have any improved outcome (in terms of death, surgical referral or duration of hospital stay). Tissue plasminogen activator (tPA) acts by virtue of its fibrinolytic property. It can either be used alone or in combination with other agents. The viscosity of empyema fluid is caused by extracellular DNA. Deoxyribonuclease (DNase) is another agent which acts by degrading them. Also, they help destroy bacterial biofilm. DNase is reported to increase the efficacy of streptokinase or tPA. A combination of tPA and DNase was reported to be more effective than any other combinations with respect to a reduction of surgical referral and morbidity.
Frequency and Dosage
Various recommendations exist, ranging from 2 to 100 mg of tPA,[29] [30] for dwell time varying from 30 minutes to 4 hours.[31] [32] MIST2 trial recommends twice daily administration of a dose of 10 mg of tPA and 5 mg of DNase; instilled sequentially with a gap of 2 hours. Individual dwell time for each agent is 1 hour. In case of simultaneous administration of two agents; a dwell time of 2 hours should be allowed. The duration of treatment is also not uniform, and mostly individualized. However, a duration of 3 days is recommended by MIST2 trial; and any prolongation of treatment duration does not lead to improved outcome.
Benefits
Improved outcome of tube drainage in terms of reduced rate of surgical intervention and death ( [Fig. 5] ).
Adverse Effects
Intrapleural administration of tPA does not cause systemic bleeding because they do not have significant systemic absorption. However, they can cause local (pleural) hemorrhage, especially at a higher dose. The maximum safe dose is variable according to different studies, ranging from 20 to 100 mg. Intrapleural hemorrhage is mostly treatable with conservative measures and stoppage of IPFT. Anaphylaxis to streptokinase is also a documented adverse effect which can be life threatening.
Cost-Effectiveness Issues
IPFT reduces the rates of surgical referral and, therefore, the surgical cost. However, the additional period of hospital stay and the cost of fibrinolytics should also be taken into consideration. A recent meta-analysis did not show any benefit of IPFT in terms of duration of hospital stay.[33] This is more relevant in resource-constrained countries like India.
The summary of the pharmacologic agents and their dosage is further listed in [Table 4].
Abbreviations: DNase, deoxyribonuclease; IPFC, infected pleural fluid collection; tPA, tissue plasminogen activator.
Important Trials on Intrapleural Fibrinolytic Therapy
The topic of the efficacy of IPFT is a matter of perpetual confusion. Several large studies/trials have taken place in the last few decades, a few of them are being discussed hereinafter.
Multicenter Intrapleural Sepsis Trials 1 and 2
These two large trials originated from the United Kingdom. MIST1 trial was conducted between 1999 and 2002 on 454 patients, with the objective of establishing the efficacy and safety of intrapleural streptokinase in patients of empyema and CPE. This study concluded that intrapleural streptokinase did not improve mortality, rate of surgery or length of the hospital stay, and was associated with significant adverse effects.[24] MIST2 trial, conducted from 2005 to 2008, evaluated the efficacy of other intrapleural fibrinolytic agents (tPA and DNase) on 210 patients ([Supplementary Table S1]; available in the online version). This trial had four arms (tPA alone, DNase alone, combination, and placebo). The investigators concluded that intrapleural t-PA–DNase therapy improved fluid drainage and reduced the frequency of surgical referral, and hospital stay. Treatment with DNase alone or t-PA alone was ineffective.[25] Another meta-analysis comparing IPFT with placebo reported that IPFT reduces the need for surgical referral and low risk of overall mortality.[34] A flowchart summarizing the indications for various intervention steps is depicted in [Fig. 6]:

Special Situations
Bronchopleural Fistula
Bronchopleural fistula (BPF) can develop after lung resections (commoner) and as a complication of necrotizing pneumonia (rare). The incidences of BPF after pulmonary resections have reduced with the advent of good antibiotics. The reported incidence of BPF is higher in cases of pneumonectomy rather than lobectomy. Several other factors govern the risk of developing a postoperative BPF.
A necrotizing pneumonia can occasionally give rise to BPF ( [Fig. 7] ). Long-term tube thoracostomy is recommended. A word of caution worth mentioning is that in empyema associated with BPF, IPFT is contraindicated. Studies have demonstrated the utility of apposing the serratus anterior muscle in the chest cavity for the closure of fistula during thoracoscopic debridement in children.[35]

Unexpandable Lung
Unexpandable lung is a term used to define the condition when the visceral and parietal pleura do not appose even after adequate pleural fluid drainage. It can occur as a result of empyema, CPE, malignant pleural effusion, uremic effusion, hemothorax, and radiation-induced or pleurodesis-induced pleural damage.
The underlying mechanism of nonexpansion of lung can be as follows:
-
Central obstruction of the subtending bronchus ( [Fig. 8A] ).
-
Prolonged atelectasis which leads to inadequate subsequent expansion ( [Fig. 8B] ).
-
Thick pleural peel which hinders proper apposition of pleural layers ([Fig. 8C] and [D] ).

It is important to understand the difference between two terminologies used in relation to nonexpansion of the lung, “lung entrapment” and “trapped lung.” Failure of apposition of pleural layers can be seen either during an active pleural inflammatory process (or malignancy) or in healed diseases where there is no active inflammation. The term “lung entrapment” is used when active inflammation is present while “trapped lung” is used in cases of healed infections. ([Fig. 9])

[Fig. 10] describes the pathogenesis and clinical manifestations of these two entities. Pleural manometry is useful in differentiating these two entities. Ultrasound demonstrates an absence of normal “sinusoid sign” in both these situations. CT is crucial in identifying the cause of nonexpansion.

The clinical manifestations arise out of the inability of the lung to expand. When a large amount of pleural fluid is drained, and yet the lung cannot expand, it creates a characteristic sharp pain. This pain has been typically described to resolve after injection of air into the pleural space (“therapeutic pneumothorax”). In case of a more pronounced negative intrapleural pressure, small peripheral airways may rupture, leading to pneumothorax (“pneumothorax-ex-vacuo”). This pneumothorax is usually asymptomatic, as it is actually a way to normalize the negative pressure within the pleural cavity. Reexpansion pulmonary edema is also a dreaded complication of excessive pleural fluid drainage in the background of an unexpandable lung.
Empyema in Children
Incidence of CPE and empyema in children is lower than in adults. However, these are different from the adult counterpart, both in terms of epidemiology, as well as management strategies.
First, decision of tube thoracostomy is usually based on clinical (failure to respond to appropriate antibiotic treatment) and imaging parameters. CT is not routinely recommended. A baseline CT may be performed. However, USG is preferred for monitoring. Echogenic contents, debris, loculations, and pleural thickening should call for escalation of management. In follow-up, USG is preferred as ultrasonographic visualization is much better in children owing to thinner chest wall musculature.
Second, the procedure of tube drainage should always be performed under proper sedation (in older children) and general anesthesia (in case of very small children). In case of procedure under sedation in an interventional radiology suite, proper patient monitoring should be ensured.
Third, there is no consensus recommendation regarding the optimal tube size in children. Several large studies have produced conflicting reports.[35] [36] [37] [38] In a large single-center study from the United Kingdom,[39] smaller bore tubes were recommended in children. The advantages include superior patient comfort, less pain and reduced hospital stay. The same study has recommended a size of 8.5 Fr for older children,[39] and even smaller bore tubes in younger children.
Lastly, several technical nuances are worth noting in pediatric procedures. Single step trocar technique is often preferred over Seldinger's technique in children.[37] The aspiration of pleural fluid should be gradual (maximum: 10 mL/kg) to avoid reexpansion pulmonary edema. In children, adhesive devices are preferred over sutures. Fibrinolytic dosage is also different in children. The recommended dose is 10,000 U urokinase diluted in 10 mL of normal saline in infants and 40,000 U urokinase in 40 mL of normal saline in older children. A dwell time of 4 hours should be followed by an 8-hour drainage at a negative suction of 10 to 20 cm H2O.
Summary of Guidelines
Several guidelines are available regarding diagnosis, management, and pharmacologic choices in IPFCs. Herein, we shall summarize the salient points from the AATS guidelines ([Table 5]).
Abbreviations: AATS, American Academy for Thoracic Surgeons; BPF, bronchopleural fistula; CAP, community-acquired pneumonia; CPE, complicated parapneumonic effusion; CT, computed tomography; CXR, chest X-ray; HAP, hospital-acquired pneumonia; LDH, lactate dehydrogenase; LOE, level of evidence; USG, ultrasonography; VATS, video-assisted thoracic surgery;
a This remains a matter of debate; as several prominent trials (e.g., multicenter intrapleural sepsis trial 2) advocate the use of IPFT to improve outcome and avoid surgery. In practice, it largely depends on multiple factors as follows: (1) institutional protocol; (2) availability of experienced thoracic surgeon for decortication which is a major surgical procedure; (3) availability of appropriate surgical infrastructure, especially in emergency hours; (4) patient suitability for undergoing a major surgical procedure; and (5) experience of the interventional radiology team.
b Choosing an optimum tube size in children is also a controversial topic (discussed in detail above).
Conclusion
IPFCs, secondary to pyogenic infections, require early complete drainage of the fluid in addition to systemic drugs. Image-guided drainage along with IPFT plays an important role in improving outcomes.
Conflict of interest
There are no financial or nonfinancial conflicts.
-
References
- 1 Light RW. Pleural Diseases. 6th ed. India: Wolters Kluwer 2019
- 2 Scarci M, Abah U, Solli P. et al. EACTS expert consensus statement for surgical management of pleural empyema. Eur J Cardiothorac Surg 2015; 48 (05) 642-653
- 3 Zahid I, Routledge T, Billè A, Scarci M. What is the best treatment of postpneumonectomy empyema?. Interact Cardiovasc Thorac Surg 2011; 12 (02) 260-264
- 4 Balfour-Lynn IM, Abrahamson E, Cohen G. et al. Paediatric Pleural Diseases Subcommittee of the BTS Standards of Care Committee. BTS guidelines for the management of pleural infection in children. Thorax 2005; 60 (Suppl. 01) i1-i21
- 5 Davies HE, Davies RJ, Davies CW, Group BPDG. BTS Pleural Disease Guideline Group. Management of pleural infection in adults: British Thoracic Society Pleural Disease Guideline 2010. Thorax 2010; 65 (Suppl. 02) ii41-ii53
- 6 Shen KR, Bribriesco A, Crabtree T. et al. The American Association for Thoracic Surgery consensus guidelines for the management of empyema. J Thorac Cardiovasc Surg 2017; 153 (06) e129-e146
- 7 Colice GL, Curtis A, Deslauriers J. et al. Medical and surgical treatment of parapneumonic effusions : an evidence-based guideline. Chest 2000; 118 (04) 1158-1171
- 8 Light RW. A new classification of parapneumonic effusions and empyema. Chest 1995; 108 (02) 299-301
- 9 Pine JR, Hollman JL. Elevated pleural fluid pH in Proteus mirabilis empyema. Chest 1983; 84 (01) 109-111
- 10 Micek ST, Dunne M, Kollef MH. Pleuropulmonary complications of Panton-Valentine leukocidin-positive community-acquired methicillin-resistant Staphylococcus aureus: importance of treatment with antimicrobials inhibiting exotoxin production. Chest 2005; 128 (04) 2732-2738
- 11 El AA Solh, Alhajjhasan A, Ramadan FH, Pineda LA. A comparative study of community- and nursing home-acquired empyema thoracis. J Am Geriatr Soc 2007; 55 (11) 1847-1852
- 12 Maskell NA, Batt S, Hedley EL, Davies CW, Gillespie SH, Davies RJ. The bacteriology of pleural infection by genetic and standard methods and its mortality significance. Am J Respir Crit Care Med 2006; 174 (07) 817-823
- 13 Lin YC, Chen HJ, Liu YH, Shih CM, Hsu WH, Tu CY. A 30-month experience of thoracic empyema in a tertiary hospital: emphasis on differing bacteriology and outcome between the medical intensive care unit (MICU) and medical ward. South Med J 2008; 101 (05) 484-489
- 14 Ibitoye BO, Idowu BM, Ogunrombi AB, Afolabi BI. Ultrasonographic quantification of pleural effusion: comparison of four formulae. Ultrasonography 2018; 37 (03) 254-260
- 15 Moy MP, Levsky JM, Berko NS, Godelman A, Jain VR, Haramati LB. A new, simple method for estimating pleural effusion size on CT scans. Chest 2013; 143 (04) 1054-1059
- 16 Ahmed AE, Yacoub TE. Empyema thoracis. Clin Med Insights Circ Respir Pulm Med 2010; 4: 1-8
- 17 Naranje P, Guleria R. Imaging of infections of pleura and chest wall. In: Bhalla AS, Jana M, eds. Clinicoradiological Series: Imaging of Chest Infections. Delhi, India: JP Brothers Medical Publishers 2018: 385-404
- 18 Subotic D, Lardinois D, Hojski A. Minimally invasive thoracic surgery for empyema. Breathe (Sheff 2018; 14 (04) 302-310
- 19 Andrews NC, Parker EF, Shaw RR, Wilson J, Webb WR. Management of nontuberculous empyema: a statement of the subcommittee on surgery. Am Rev Respir Dis 1962 85: 935-936
- 20 Heffner JE, McDonald J, Barbieri C, Klein J. Management of parapneumonic effusions. An analysis of physician practice patterns. Arch Surg 1995; 130 (04) 433-438
- 21 Ashbaugh DG. Empyema thoracis. Factors influencing morbidity and mortality. Chest 1991; 99 (05) 1162-1165
- 22 Corso RM, Agnoletti V, Piraccini E, Lupi C, Gambale G. Wire-guided chest tube placement in the intensive care unit. Anaesth Intensive Care 2012; 40 (06) 1071-1072
- 23 Davies CW, Kearney SE, Gleeson FV, Davies RJ. Predictors of outcome and long-term survival in patients with pleural infection. Am J Respir Crit Care Med 1999; 160 (5, pt 1) 1682-1687
- 24 Maskell NA, Davies CW, Nunn AJ. et al. First Multicenter Intrapleural Sepsis Trial (MIST1) Group. U.K. Controlled trial of intrapleural streptokinase for pleural infection. N Engl J Med 2005; 352 (09) 865-874
- 25 Rahman NM, Maskell NA, West A. et al. Intrapleural use of tissue plasminogen activator and DNase in pleural infection. N Engl J Med 2011; 365 (06) 518-526
- 26 Rahman NM, Maskell NA, Davies CW. et al. The relationship between chest tube size and clinical outcome in pleural infection. Chest 2010; 137 (03) 536-543
- 27 Havelock T, Teoh R, Laws D, Gleeson F, Group BPDG. BTS Pleural Disease Guideline Group. Pleural procedures and thoracic ultrasound: British Thoracic Society Pleural Disease Guideline 2010. Thorax 2010; 65 (Suppl. 02) ii61-ii76
- 28 Hooper CE, Edey AJ, Wallis A. et al. Pleural irrigation trial (PIT): a randomised controlled trial of pleural irrigation with normal saline versus standard care in patients with pleural infection. Eur Respir J 2015; 46 (02) 456-463
- 29 Skeete DA, Rutherford EJ, Schlidt SA, Abrams JE, Parker LA, Rich PB. Intrapleural tissue plasminogen activator for complicated pleural effusions. J Trauma 2004; 57 (06) 1178-1183
- 30 Thommi G, Nair CK, Aronow WS, Shehan C, Meyers P, McLeay M. Efficacy and safety of intrapleural instillation of alteplase in the management of complicated pleural effusion or empyema. Am J Ther 2007; 14 (04) 341-345
- 31 Heimes J, Copeland H, Lulla A. et al. The use of thrombolytics in the management of complex pleural fluid collections. J Thorac Dis 2017; 9 (05) 1310-1316
- 32 Popowicz N, Bintcliffe O, De Fonseka D. et al. Dose de-escalation of intrapleural tissue plasminogen activator therapy for pleural infection. the alteplase dose assessment for pleural infection therapy project. Ann Am Thorac Soc 2017; 14 (06) 929-936
- 33 Redden MD, Chin TY, van Driel ML. Surgical versus non-surgical management for pleural empyema. Cochrane Database Syst Rev 2017; 3: CD010651
- 34 Altmann ES, Crossingham I, Wilson S, Davies HR. Intra-pleural fibrinolytic therapy versus placebo, or a different fibrinolytic agent, in the treatment of adult parapneumonic effusions and empyema. Cochrane Database Syst Rev 2019; 2019 (10) CD002312
- 35 Jester I, Nijran A, Singh M, Parikh DH. Surgical management of bronchopleural fistula in pediatric empyema and necrotizing pneumonia: efficacy of the serratus anterior muscle digitation flap. J Pediatr Surg 2012; 47 (07) 1358-1362
- 36 Pierrepoint MJ, Evans A, Morris SJ, Harrison SK, Doull IJ. Pigtail catheter drain in the treatment of empyema thoracis. Arch Dis Child 2002; 87 (04) 331-332
- 37 Thomson AH, Hull J, Kumar MR, Wallis C, Balfour IM Lynn. Randomised trial of intrapleural urokinase in the treatment of childhood empyema. Thorax 2002; 57 (04) 343-347
- 38 Petel D, Li P, Emil S. Percutaneous pigtail catheter versus tube thoracostomy for pediatric empyema: A comparison of outcomes. Surgery 2013; 154 (04) 655-660 discussion 660–661
- 39 Lewis MR, Micic TA, Doull IJM, Evans A. Real-time ultrasound-guided pigtail catheter chest drain for complicated parapneumonic effusion and empyema in children - 16-year, single-centre experience of radiologically placed drains. Pediatr Radiol 2018; 48 (10) 1410-1416
Address for correspondence
Publication History
Article published online:
12 October 2021
© 2021. Indian Society of Vascular and Interventional Radiology. This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial-License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/).
Thieme Medical and Scientific Publishers Pvt. Ltd.
A-12, 2nd Floor, Sector 2, Noida-201301 UP, India
-
References
- 1 Light RW. Pleural Diseases. 6th ed. India: Wolters Kluwer 2019
- 2 Scarci M, Abah U, Solli P. et al. EACTS expert consensus statement for surgical management of pleural empyema. Eur J Cardiothorac Surg 2015; 48 (05) 642-653
- 3 Zahid I, Routledge T, Billè A, Scarci M. What is the best treatment of postpneumonectomy empyema?. Interact Cardiovasc Thorac Surg 2011; 12 (02) 260-264
- 4 Balfour-Lynn IM, Abrahamson E, Cohen G. et al. Paediatric Pleural Diseases Subcommittee of the BTS Standards of Care Committee. BTS guidelines for the management of pleural infection in children. Thorax 2005; 60 (Suppl. 01) i1-i21
- 5 Davies HE, Davies RJ, Davies CW, Group BPDG. BTS Pleural Disease Guideline Group. Management of pleural infection in adults: British Thoracic Society Pleural Disease Guideline 2010. Thorax 2010; 65 (Suppl. 02) ii41-ii53
- 6 Shen KR, Bribriesco A, Crabtree T. et al. The American Association for Thoracic Surgery consensus guidelines for the management of empyema. J Thorac Cardiovasc Surg 2017; 153 (06) e129-e146
- 7 Colice GL, Curtis A, Deslauriers J. et al. Medical and surgical treatment of parapneumonic effusions : an evidence-based guideline. Chest 2000; 118 (04) 1158-1171
- 8 Light RW. A new classification of parapneumonic effusions and empyema. Chest 1995; 108 (02) 299-301
- 9 Pine JR, Hollman JL. Elevated pleural fluid pH in Proteus mirabilis empyema. Chest 1983; 84 (01) 109-111
- 10 Micek ST, Dunne M, Kollef MH. Pleuropulmonary complications of Panton-Valentine leukocidin-positive community-acquired methicillin-resistant Staphylococcus aureus: importance of treatment with antimicrobials inhibiting exotoxin production. Chest 2005; 128 (04) 2732-2738
- 11 El AA Solh, Alhajjhasan A, Ramadan FH, Pineda LA. A comparative study of community- and nursing home-acquired empyema thoracis. J Am Geriatr Soc 2007; 55 (11) 1847-1852
- 12 Maskell NA, Batt S, Hedley EL, Davies CW, Gillespie SH, Davies RJ. The bacteriology of pleural infection by genetic and standard methods and its mortality significance. Am J Respir Crit Care Med 2006; 174 (07) 817-823
- 13 Lin YC, Chen HJ, Liu YH, Shih CM, Hsu WH, Tu CY. A 30-month experience of thoracic empyema in a tertiary hospital: emphasis on differing bacteriology and outcome between the medical intensive care unit (MICU) and medical ward. South Med J 2008; 101 (05) 484-489
- 14 Ibitoye BO, Idowu BM, Ogunrombi AB, Afolabi BI. Ultrasonographic quantification of pleural effusion: comparison of four formulae. Ultrasonography 2018; 37 (03) 254-260
- 15 Moy MP, Levsky JM, Berko NS, Godelman A, Jain VR, Haramati LB. A new, simple method for estimating pleural effusion size on CT scans. Chest 2013; 143 (04) 1054-1059
- 16 Ahmed AE, Yacoub TE. Empyema thoracis. Clin Med Insights Circ Respir Pulm Med 2010; 4: 1-8
- 17 Naranje P, Guleria R. Imaging of infections of pleura and chest wall. In: Bhalla AS, Jana M, eds. Clinicoradiological Series: Imaging of Chest Infections. Delhi, India: JP Brothers Medical Publishers 2018: 385-404
- 18 Subotic D, Lardinois D, Hojski A. Minimally invasive thoracic surgery for empyema. Breathe (Sheff 2018; 14 (04) 302-310
- 19 Andrews NC, Parker EF, Shaw RR, Wilson J, Webb WR. Management of nontuberculous empyema: a statement of the subcommittee on surgery. Am Rev Respir Dis 1962 85: 935-936
- 20 Heffner JE, McDonald J, Barbieri C, Klein J. Management of parapneumonic effusions. An analysis of physician practice patterns. Arch Surg 1995; 130 (04) 433-438
- 21 Ashbaugh DG. Empyema thoracis. Factors influencing morbidity and mortality. Chest 1991; 99 (05) 1162-1165
- 22 Corso RM, Agnoletti V, Piraccini E, Lupi C, Gambale G. Wire-guided chest tube placement in the intensive care unit. Anaesth Intensive Care 2012; 40 (06) 1071-1072
- 23 Davies CW, Kearney SE, Gleeson FV, Davies RJ. Predictors of outcome and long-term survival in patients with pleural infection. Am J Respir Crit Care Med 1999; 160 (5, pt 1) 1682-1687
- 24 Maskell NA, Davies CW, Nunn AJ. et al. First Multicenter Intrapleural Sepsis Trial (MIST1) Group. U.K. Controlled trial of intrapleural streptokinase for pleural infection. N Engl J Med 2005; 352 (09) 865-874
- 25 Rahman NM, Maskell NA, West A. et al. Intrapleural use of tissue plasminogen activator and DNase in pleural infection. N Engl J Med 2011; 365 (06) 518-526
- 26 Rahman NM, Maskell NA, Davies CW. et al. The relationship between chest tube size and clinical outcome in pleural infection. Chest 2010; 137 (03) 536-543
- 27 Havelock T, Teoh R, Laws D, Gleeson F, Group BPDG. BTS Pleural Disease Guideline Group. Pleural procedures and thoracic ultrasound: British Thoracic Society Pleural Disease Guideline 2010. Thorax 2010; 65 (Suppl. 02) ii61-ii76
- 28 Hooper CE, Edey AJ, Wallis A. et al. Pleural irrigation trial (PIT): a randomised controlled trial of pleural irrigation with normal saline versus standard care in patients with pleural infection. Eur Respir J 2015; 46 (02) 456-463
- 29 Skeete DA, Rutherford EJ, Schlidt SA, Abrams JE, Parker LA, Rich PB. Intrapleural tissue plasminogen activator for complicated pleural effusions. J Trauma 2004; 57 (06) 1178-1183
- 30 Thommi G, Nair CK, Aronow WS, Shehan C, Meyers P, McLeay M. Efficacy and safety of intrapleural instillation of alteplase in the management of complicated pleural effusion or empyema. Am J Ther 2007; 14 (04) 341-345
- 31 Heimes J, Copeland H, Lulla A. et al. The use of thrombolytics in the management of complex pleural fluid collections. J Thorac Dis 2017; 9 (05) 1310-1316
- 32 Popowicz N, Bintcliffe O, De Fonseka D. et al. Dose de-escalation of intrapleural tissue plasminogen activator therapy for pleural infection. the alteplase dose assessment for pleural infection therapy project. Ann Am Thorac Soc 2017; 14 (06) 929-936
- 33 Redden MD, Chin TY, van Driel ML. Surgical versus non-surgical management for pleural empyema. Cochrane Database Syst Rev 2017; 3: CD010651
- 34 Altmann ES, Crossingham I, Wilson S, Davies HR. Intra-pleural fibrinolytic therapy versus placebo, or a different fibrinolytic agent, in the treatment of adult parapneumonic effusions and empyema. Cochrane Database Syst Rev 2019; 2019 (10) CD002312
- 35 Jester I, Nijran A, Singh M, Parikh DH. Surgical management of bronchopleural fistula in pediatric empyema and necrotizing pneumonia: efficacy of the serratus anterior muscle digitation flap. J Pediatr Surg 2012; 47 (07) 1358-1362
- 36 Pierrepoint MJ, Evans A, Morris SJ, Harrison SK, Doull IJ. Pigtail catheter drain in the treatment of empyema thoracis. Arch Dis Child 2002; 87 (04) 331-332
- 37 Thomson AH, Hull J, Kumar MR, Wallis C, Balfour IM Lynn. Randomised trial of intrapleural urokinase in the treatment of childhood empyema. Thorax 2002; 57 (04) 343-347
- 38 Petel D, Li P, Emil S. Percutaneous pigtail catheter versus tube thoracostomy for pediatric empyema: A comparison of outcomes. Surgery 2013; 154 (04) 655-660 discussion 660–661
- 39 Lewis MR, Micic TA, Doull IJM, Evans A. Real-time ultrasound-guided pigtail catheter chest drain for complicated parapneumonic effusion and empyema in children - 16-year, single-centre experience of radiologically placed drains. Pediatr Radiol 2018; 48 (10) 1410-1416