

Subscribe to RSS
DOI: 10.1055/s-0041-1740258
Engaging Housestaff as Informatics Collaborators: Educational and Operational Opportunities
Authors
Funding No funding sources were utilized for this work.

Abstract
Background In academic hospitals, housestaff (interns, residents, and fellows) are a core user group of clinical information technology (IT) systems, yet are often relegated to being recipients of change, rather than active partners in system improvement. These information systems are an integral part of health care delivery and formal efforts to involve and educate housestaff are nascent.
Objective This article develops a sustainable forum for effective engagement of housestaff in hospital informatics initiatives and creates opportunities for professional development.
Methods A housestaff-led IT council was created within an academic medical center and integrated with informatics and graduate medical education leadership. The Council was designed to provide a venue for hands-on clinical informatics educational experiences to housestaff across all specialties.
Results In the first year, five housestaff co-chairs and 50 members were recruited. More than 15 projects were completed with substantial improvements made to clinical systems impacting more than 1,300 housestaff and with touchpoints to nearly 3,000 staff members. Council leadership was integrally involved in hospital governance committees and became the go-to source for housestaff input on informatics efforts. Positive experiences informed members' career development toward informatics roles. Key lessons learned in building for success are discussed.
Conclusion The council model has effectively engaged housestaff as learners, local champions, and key informatics collaborators, with positive impact for the participating members and the institution. Requiring few resources for implementation, the model should be replicable at other institutions.
Keywords
stakeholder engagement - graduate medical education - quality improvement - program evaluationBackground and Significance
In academic medical centers, clinical informaticians advance care through development of clinical information systems (CIS) and training the next generation of clinicians in informatics. Since formally becoming a subspecialty in 2011, clinical informatics (CI) fellowship programs have been established as a training pathway for physicians.[1] However, health informatics is a required skill for all 21st century clinicians,[2] and thus there is a need for informatics experiences for all postgraduate trainees.[3] Previously described educational initiatives have focused on brief trainings on informatics,[4] [5] [6] [7] but few institutions have engaged housestaff in hands-on experiential informatics training or formalized educational programs.[7] [8] [9] [10] Early career exposure to informatics can support professional development in the field, addressing unmet need for these skilled physicians in the health care workforce.
Housestaff are a core user group of CIS—spending much of their workday interacting with the electronic health record (EHR),[11] [12] picture archiving and communication systems, and other clinical communication tools—which makes them well positioned to be key contributors to informatics improvement initiatives.[8] [13] As frontline clinicians working in both ambulatory and inpatient settings across multiple teams, housestaff have first-hand knowledge of complex and varied workflows and have a vested interest in identifying, implementing, and improving patient care and system usability.[8] [14] [15] [16] Despite these opportunities, housestaff are an underutilized resource, often relegated to being recipients of system changes, rather than primary drivers and champions.
Although multiple models may be successful in engaging housestaff in hospital informatics,[4] [7] [8] [9] [10] we report here on a novel housestaff-organized and -led information technology (IT) council format that has fostered opportunities for housestaff to collaborate in operational roles and to learn CI through hands-on real-world experiences.
Principles, Structure, and Functions of a Housestaff IT Council
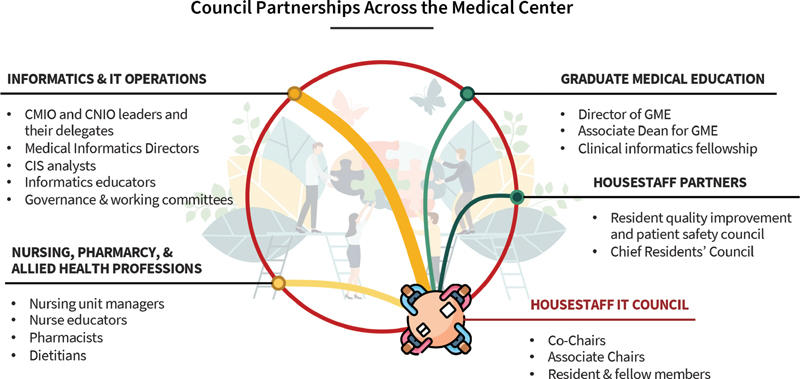
In February 2020, the Housestaff Information Technology Enhancement Council was created at Stanford Health Care, a tertiary/quaternary care academic hospital system in Palo Alto, California, United States. The Council's structure and integration with key informatics leadership ([Fig. 1]) was modeled after the experiences of our authors (J.S., I.J.) at prior institutions,[13] [17] as well as on the Medical Informatics Directors Working Group, a faculty group operating under the direction of the Chief Medical Information Officer (CMIO). Guiding goals for the Council are described in [Table 1].
Leadership of the Council is divided into domains managed by associate Chairs including the EHR, non-EHR hospital technology (e.g., the secure clinical text messaging platform), and a housestaff-directed IT resource Web site. Those individuals chosen for Council leadership commit to a minimum of a 1-year term during which they are primarily responsible for directing Council activities in their respective domain and leading relevant project teams; participating in hospital IT governance; and attending all Council meetings. To foster a culture of inclusion, collaboration, and transparency, becoming a Council member, by self-subscribing to the mailing list and/or attending meetings, is open to any individual in the hospital's housestaff community. Barriers to participation were intentionally minimized as all members and hospital partners volunteered their time.
The Council is supported by the offices of the CMIO, Chief Nursing Informatics Officer (CNIO), and Graduate Medical Education (GME). Collaboration between the Council and hospital informatics teams occurs formally through monthly Council meetings as well as informally via email and other communications. Additionally, Council leadership regularly participates in various hospital committees, including the Medical Informatics Directors Working Group, the Clinical Decision Support group, the inpatient orderset review committee, and the secure chat steering committee. The Council also partners with the informatics education team for onboarding of new housestaff. This bidirectional participation ensures that housestaff voices continue to be integrated within hospital initiatives.
For the hour-long Council meetings, held monthly after clinic hours, we developed a productive and sustainable format with slides prepared in advance: (1) education and system updates from hospital informaticians and informatics educators; (2) stakeholder presentations on specific projects to obtain feedback from the Council and its partners; (3) updates from the Associate Chairs on domain-specific initiatives; and (4) announcements and next steps from the co-Chairs. In addition to the Council's leadership, general housestaff members, CI fellows, and individuals within the hospital informatics leadership—including the CMIO, associate CMIO, CNIO, and designated representatives for physicians, nurses, pharmacists, informatics educators, and EHR analysts—routinely attend.
Results
In its first 12 months, the two founding co-Chairs recruited 4 associate Chairs as well as 55 housestaff members. The subspecialties represented among inaugural Council leaders included anesthesia, endocrinology, internal medicine, otolaryngology, and urology. A CI fellow was also recruited in the first year. General members similarly represented a broad range of clinical specialties.
The Council successfully completed more than 15 projects of varying scale with substantial improvements made to clinical systems impacting more than 1,300 housestaff and with touchpoints to nearly 3,000 staff members in its first year. Selected projects are described in [Table 2]. These projects have filled gaps in existing resources and training, targeted improvements to drivers of housestaff frustration, and addressed common needs across specialties. Projects were selected based on housestaff motivation and requests by hospital partners.
Abbreviations: CMIO, Chief Medical Information Officer; CNIO, Chief Nursing Informatics Officer; EHR, electronic health record; GME, Graduate Medical Education; IT, information technology; MAR, medical administration record; QI, quality improvement.
One Council-led endeavor involved the inpatient secure text messaging platform, utilized daily by more than 12,000 users. As daily users, the Council identified solutions to errors in clinician and patient identification and lack of message prioritization amidst a high volume of incoming messages. After analyzing real-world communications to derive performance metrics that could enable tracking of subsequent improvements, members collaborated with technical analysts to design solutions (e.g., linkage of user roles in the EHR to the messaging platform) and presented at governance committees to propose sociotechnical changes (e.g., updated communication protocols).
Another gap filled by the Council was communicating IT changes to housestaff. The Council developed a monthly email newsletter and a new Web site (hitec.stanford.edu) to provide content in a relevant, accessible manner ([Fig. 2]). Within 9 months, the Web site's traffic increased to over 200 visitors per month, approximately 15% of all housestaff. Partnership with the informatics education team harmonized efforts to ensure all users of CIS were adequately informed.

Leadership across the hospital has increasingly approached the Council for guidance regarding technology impacting housestaff. For example, a team from pharmacy, nutrition, and nursing sought feedback on an initiative to add tube feeding to the medication administration record. Council leadership has also been invited to serve on multiple hospital informatics task forces and governance committees.
Discussion
Implementation of a housestaff IT council at an academic medical center has been the foundation for a rich collaboration between housestaff and hospital informatics ([Fig. 1]). Informal feedback has demonstrated strong bidirectional enthusiasm for the Council model, noting both the short- and long-term value for participating housestaff, informatics leadership, and the CIS user community. The Council provided a mechanism by which informatics leadership could readily obtain housestaff feedback on new initiatives, whereas housestaff realized a forum to drive CI improvement efforts.
The Council was formed to address the lack of a housestaff-driven forum dedicated to hospital informatics at the authors' institution. Although existing housestaff leadership groups such as the Resident Safety Council and Chief Residents' Council occasionally touched on IT issues, informatics was not their primary focus. Additionally, fellows are traditionally excluded from many housestaff groups but are an integral part of the Council.
Pursuit of projects spanning quick wins to long-term efforts rapidly demonstrated the Council's contributions to the hospital's CIS. Housestaff became engaged champions, promoting the hospital's informatics goals among their peers. Motivated by their positive experiences to date, all of the Council's inaugural leadership intends to pursue operational informatics roles in their careers, including one pursuing CI fellowship and one accepting an industry position developing clinical technology.
Facilitators of and Barriers to Success
We identified several factors that contributed to the success of this initiative. First, from the initial inception of the Council, senior informatics leaders at our organization dedicated time and effort to attend meetings, provide mentorship, and be vocal advocates for the Council throughout the medical center. Their support strengthened a nascent institutional culture by affirming that housestaff are key stakeholders with significant ability to contribute to institutional projects. Second, we found that structured and inclusive monthly meetings involving housestaff, hospital informaticians, and other partners fostered a productive workspace for these activities. Regular meetings promoted project accountability and momentum, while the inclusive format facilitated collaborative discussion and feedback. Third, the Council's housestaff leadership was committed to the longevity of the initiative by establishing strong partnerships with informatics leaders, the CI fellowship, and the office for GME, as well as engaging their housestaff colleagues within and outside of the Council. These relationships built a strong foundation for the Council to actively exist in the organization long after the founding members have graduated.
In contrast to the New EHR Resident Development Squad at the Children's Hospital of Pennsylvania,[8] our model was designed for longitudinal housestaff engagement in CI and IT projects wherein the Council not only provides feedback but also serves as a partner and driver throughout the development and implementation pathway. Additionally, our Council is open to participation from housestaff of all residency and fellowship training programs. The Resident Informaticist Program at the University of California, Los Angeles[10] delivered outstanding impact by having each resident participant complete an informatics project while receiving formalized informatics education from their faculty. However, this model requires extensive financial and time investments from the institution, faculty partners, and the residents themselves, which may not be feasible at all institutions. By contrast, our model is sustained by time volunteered by housestaff and hospital partners without formal funding or protected time. Council proposals are considered equally by the IT department as those from other groups. Our Council model relies on team-based project completion, which more readily accommodates the housestaff's limited free time and varying schedules as well as requiring limited resources to set up and maintain, and so should be readily adaptable to the resources available across different institutions.
There have been some barriers encountered by the Council to date. One key challenge was that, although planning began in November 2019, the first group-wide meeting in February 2020 coincided with the cessation of in-person extracurricular activities due to the COVID-19 pandemic. In the first year of the Council, all meetings thus were held virtually. Although the virtual format limited the development of interpersonal relationships to some extent, it also enabled higher rates of participation from a group that notoriously has little free time. Additionally, COVID-19 has limited the bandwidth of the IT teams, delaying implementation of several projects from the Council, although relationships developed through the Council facilitated short-tracking of several simple improvements. Another important barrier is that the associated children's hospital has a separate IT and leadership structure. Although most housestaff rotate through both settings, housestaff in pediatrics and obstetrics have had less opportunity to get involved with IT projects because, to date, informatics representation has only been from the adult hospital organization. To address this, the Council is inclusive of housestaff in pediatrics specialties and is planning to involve children's hospital informatics efforts in its second year.
Limitations
There are also some limitations of the Council model described here that are worthy of mention. As a young initiative, it remains too early to assess its long-term impact. Yet, our early experiences are promising and have demonstrated clear improvements to our CIS. Mechanisms to sustain housestaff participation in the Council will be essential, as others have reported.[8] [9] The Council plans to solicit new housestaff membership during CIS onboarding training and integrate CI fellows into the leadership structure annually. Some may raise concerns about housestaff having sufficient time and energy to devote to these efforts; our experience suggests that a clear mission, regular meeting cadences, appropriate project scoping, and continued support from experienced leadership help retain and grow housestaff participation despite their multiple clinical and professional demands. While our Council model has worked well at our institution due to support and engagement by a strong group of CI leadership, it may not translate as well to other institutions where the culture is more siloed or that lack a strong informatics infrastructure with resources to iterate and enhance existing systems.
Future Directions
Future directions for the Council include extending the scope to include the associated colocated children's hospital and/or other major affiliate hospitals through which housestaff rotate, developing a longitudinal portfolio of projects, and formalizing educational opportunities for housestaff members. Additionally, we hope to continue to contribute academically to the field of CI with follow-up work on Council projects, such as technology-enabled intrahospital communication; formal evaluation of sustainability as members graduate; and the impact of the Council not only on IT projects but also housestaff well-being.
Conclusion
The integration of a housestaff IT council with hospital informatics leadership has effectively engaged housestaff as learners, champions, and key collaborators in an academic medical center's informatics operations. This partnership has created substantial operational gains for the institution while simultaneously providing unique educational and professional growth opportunities for residents and fellows. Creating an avenue for housestaff to influence the hospital system's informatics system also facilitates physician-driven innovation, thereby mitigating housestaff frustration and improving patient care. We hope that our experiences may serve as a blueprint for development of similar programs at other institutions.
Clinical Relevance Statement
-
Housestaff are a core user group of clinical information systems but are an underutilized resource for system improvement. A housestaff-led IT council created an effective forum for their engagement and substantial contributions to an academic hospital's informatics priorities.
-
The proposed housestaff IT council format can be implemented with minimal costs or resources and is inclusive of trainees at all levels and of all specialties, but requires the active engagement of and championing by informatics leadership (e.g., CMIO, CNIO) at the institution.
-
Longitudinal, hands-on participation in clinical informatics initiatives creates diverse learning opportunities for the personal and professional development of housestaff, and may encourage and support a career pathway with informatics leadership roles.
Multiple Choice Questions
-
Why are housestaff strong partners in a hospital's clinical informatics efforts?
-
They are heavy users of the clinical information systems.
-
They work in multiple practice settings.
-
They have professional interest in informatics leadership.
-
They are motivated to improve the work environment for their peers.
-
All of the above.
Correct Answer: Correct choice is (e) All of the above. All of the listed choices are examples of why housestaff provide value to a hospital's clinical informatics initiatives and why housestaff choose to participate in these initiatives.
-
-
Which of the following is not a key facilitator of the housestaff IT council as described?
-
Direct support of hospital informatics leadership.
-
Direct support of the office for Graduate Medical Education.
-
Structured informatics education for housestaff members.
-
Active engagement in hands-on operational informatics activities.
Correct Answer: Correct choice is (c) Structure informatics education for housestaff members. Although structured education could be beneficial, as has been reported at other institutions, structured education was not incorporated in the housestaff IT council described in this article.
-
-
Which of the following are potential positive outcomes of a housestaff IT council?
-
Decreased clinician IT-related burnout.
-
Increasing the pool of practicing physician informaticists.
-
Improving communication between hospital informatics leadership and housestaff.
-
Improving communication among physicians, nurses, and other allied health professionals involved in patient care.
-
All of the above.
Correct Answer: Correct choice is (e) All of the above. All of the listed items were positive results obtained by implementation of the housestaff IT council as described. There is the potential for positive impact to housestaff participants; hospital leadership; and non-participating housestaff, nurses and other allied health professionals.
-
Conflict of Interest
None declared.
Acknowledgments
We wish to thank Stanford Health Care informatics leadership including Christopher Sharp, MD (CMIO) and Gretchen Brown, MSN, RN (CNIO) for their support of this initiative. We also wish to thank the physicians, nurses, pharmacists, IT professionals, and many others who have worked collaboratively with the Housestaff IT Council.
Protection of Human and Animal Subjects
The Stanford University Institutional Review Board granted exempt status to this work under the grounds of quality improvement.
* These authors contributed equally to this work as first authors.
** These authors contributed equally to this work.
-
References
- 1 Longhurst CA, Pageler NM, Palma JP. et al. Early experiences of accredited clinical informatics fellowships. J Am Med Inform Assoc 2016; 23 (04) 829-834
- 2 Fridsma DB. Health informatics: a required skill for 21st century clinicians. BMJ 2018; 362: k3043
- 3 Leung TI, Chen JH. Clinical Informatics: Journeys into an Emerging Subspecialty. SGIM Forum. 2017;40(7): 1–2
- 4 Henricks WH, Karcher DS, Harrison JH. et al. Pathology informatics essentials for residents: a flexible informatics curriculum linked to Accreditation Council for Graduate Medical Education milestones. J Pathol Inform 2016; 7: 27
- 5 Lyu HG, Doherty GM, Landman AB. Surgical informatics: defining the role of informatics in the current surgical training paradigm. J Surg Educ 2020; 77 (01) 9-12
- 6 Torous J, Chan S, Luo J, Boland R, Hilty D. Clinical informatics in psychiatric training: preparing today's trainees for the already present future. Acad Psychiatry 2018; 42 (05) 694-697
- 7 Vitiello E, Kane M, Hutto A, Hall A. Building for the future: the creation of a residency training track to foster innovation through clinical informatics in psychiatry. J Am Med Inform Assoc 2020; 27 (11) 1747-1751
- 8 Mai MV, Luo BT, Orenstein EW, Luberti AA. A model for clinical informatics education for residents: addressing an unmet need. Appl Clin Inform 2018; 9 (02) 261-267
- 9 Quirós FGB, Baum A, Lira A. Active participation and engagement of residents in clinical informatics. Appl Clin Inform 2019; 10 (01) 38-39
- 10 Singer JS, Cheng EM, Baldwin K, Pfeffer MA, Committee UHPI. UCLA Health Physician Informaticist Committee. The UCLA Health Resident Informaticist Program - a novel clinical informatics training program. J Am Med Inform Assoc 2017; 24 (04) 832-840
- 11 Holmgren AJ, Lindeman B, Ford EW. Resident physician experience and duration of electronic health record use. Appl Clin Inform 2021; 12 (04) 721-728
- 12 Sinha A, Stevens LA, Su F, Pageler NM, Tawfik DS. Measuring electronic health record use in the pediatric ICU using audit-logs and screen recordings. Appl Clin Inform 2021; 12 (04) 737-744
- 13 Brindamour L, Tess A. Resident Information Systems Committee (RISC). Beth Israel Deaconess Medical Center Quality Improvement Symposium. 2019. Boston, MA:
- 14 Kohn MS, Topaloglu U, Kirkendall ES, Dharod A, Wells BJ, Gurcan M. Creating learning health systems and the emerging role of biomedical informatics. Learn Health Syst 2021;
- 15 Martikainen S, Kaipio J, Lääveri T. End-user participation in health information systems (HIS) development: physicians' and nurses' experiences. Int J Med Inform 2020; 137: 104117
- 16 Subash M, Sakumoto M, Bass J. et al. The emerging role of clinical informatics fellows in service learning during the COVID-19 pandemic. J Am Med Inform Assoc 2021; 28 (03) 487-493
- 17 Shenson JA, Adams RC, Ahmed ST, Spickard A. Formation of a new entity to support effective use of technology in medical education: the Student Technology Committee. JMIR Med Educ 2015; 1 (02) e9
Address for correspondence
Publication History
Received: 24 August 2021
Accepted: 20 October 2021
Article published online:
08 December 2021
© 2021. Thieme. All rights reserved.
Georg Thieme Verlag KG
Rüdigerstraße 14, 70469 Stuttgart, Germany
-
References
- 1 Longhurst CA, Pageler NM, Palma JP. et al. Early experiences of accredited clinical informatics fellowships. J Am Med Inform Assoc 2016; 23 (04) 829-834
- 2 Fridsma DB. Health informatics: a required skill for 21st century clinicians. BMJ 2018; 362: k3043
- 3 Leung TI, Chen JH. Clinical Informatics: Journeys into an Emerging Subspecialty. SGIM Forum. 2017;40(7): 1–2
- 4 Henricks WH, Karcher DS, Harrison JH. et al. Pathology informatics essentials for residents: a flexible informatics curriculum linked to Accreditation Council for Graduate Medical Education milestones. J Pathol Inform 2016; 7: 27
- 5 Lyu HG, Doherty GM, Landman AB. Surgical informatics: defining the role of informatics in the current surgical training paradigm. J Surg Educ 2020; 77 (01) 9-12
- 6 Torous J, Chan S, Luo J, Boland R, Hilty D. Clinical informatics in psychiatric training: preparing today's trainees for the already present future. Acad Psychiatry 2018; 42 (05) 694-697
- 7 Vitiello E, Kane M, Hutto A, Hall A. Building for the future: the creation of a residency training track to foster innovation through clinical informatics in psychiatry. J Am Med Inform Assoc 2020; 27 (11) 1747-1751
- 8 Mai MV, Luo BT, Orenstein EW, Luberti AA. A model for clinical informatics education for residents: addressing an unmet need. Appl Clin Inform 2018; 9 (02) 261-267
- 9 Quirós FGB, Baum A, Lira A. Active participation and engagement of residents in clinical informatics. Appl Clin Inform 2019; 10 (01) 38-39
- 10 Singer JS, Cheng EM, Baldwin K, Pfeffer MA, Committee UHPI. UCLA Health Physician Informaticist Committee. The UCLA Health Resident Informaticist Program - a novel clinical informatics training program. J Am Med Inform Assoc 2017; 24 (04) 832-840
- 11 Holmgren AJ, Lindeman B, Ford EW. Resident physician experience and duration of electronic health record use. Appl Clin Inform 2021; 12 (04) 721-728
- 12 Sinha A, Stevens LA, Su F, Pageler NM, Tawfik DS. Measuring electronic health record use in the pediatric ICU using audit-logs and screen recordings. Appl Clin Inform 2021; 12 (04) 737-744
- 13 Brindamour L, Tess A. Resident Information Systems Committee (RISC). Beth Israel Deaconess Medical Center Quality Improvement Symposium. 2019. Boston, MA:
- 14 Kohn MS, Topaloglu U, Kirkendall ES, Dharod A, Wells BJ, Gurcan M. Creating learning health systems and the emerging role of biomedical informatics. Learn Health Syst 2021;
- 15 Martikainen S, Kaipio J, Lääveri T. End-user participation in health information systems (HIS) development: physicians' and nurses' experiences. Int J Med Inform 2020; 137: 104117
- 16 Subash M, Sakumoto M, Bass J. et al. The emerging role of clinical informatics fellows in service learning during the COVID-19 pandemic. J Am Med Inform Assoc 2021; 28 (03) 487-493
- 17 Shenson JA, Adams RC, Ahmed ST, Spickard A. Formation of a new entity to support effective use of technology in medical education: the Student Technology Committee. JMIR Med Educ 2015; 1 (02) e9