

Subscribe to RSS
DOI: 10.1055/s-0042-106210
Follow-up Reality for Breast Cancer Patients – Standardised Survey of Patients and Physicians and Analysis of Treatment Data
Nachsorgerealität von Brustkrebspatientinnen – standardisierte Befragung von Patientinnen und Ärzten sowie Analyse der BehandlungsdatenAuthors
Correspondence
Publication History
received 03 March 2016
revised 08 April 2016
accepted 08 April 2016
Publication Date:
19 May 2016 (online)

Abstract
Introduction: Currently, about 360 000 breast cancer patients who could, after completion of their primary therapy, take advantage of follow-up options are living in Germany. Up to now very little is known about the extent to which the available options are used and as to how the follow-up reality is experienced and evaluated. Thus, an explorative examination among the patients and their physicians was undertaken. Patients and Methods: All patients who underwent surgery in a certified breast centre between 2007 and 2013 received a standardised questionnaire; at the same time the physicians responsible for the follow-up were invited to answer a standardised questionnaire. Results: 920 patients (response rate: 61 %) with a median age of 65 years (32–95) could be analysed. 99 % of the participants stated that they regularly attended follow-ups. The personal contact with the physician (mean value: 4.4) and the reassurance that the cancer disease had not recurred (mean value: 4.5) were described on a scale of 0 to 5 to be two of the most important factors of the follow-up. Deficits were expressed with regard to psychosocial care (70 %) and the perception and treatment of physical complaints (55 %). In addition, 105 physicians returned completed questionnaires (response rate: 12 %). For asymptomatic patients the physicians performed the following examinations most frequently: anamnesis (92 %), physical examination (87 %) as well as laboratory tests (63 %) and tumour marker determinations (40 %). Conclusion: On the whole it became clear that the vast majority of the patients took advantage of the follow-up options. From the patientʼs perspective the importance of the follow-up lies in contact to the physician and the comforting assurance that the breast cancer has not relapsed. Deficits are seen in the psychosocial care and the perception and treatment of physical impairments. Not recommended examinations were employed by a significant proportion of the surveyed physicians.
Zusammenfassung
Einleitung: In Deutschland leben etwa 360 000 Brustkrebspatientinnen, die, nach Abschluss ihrer Primärtherapie, Nachsorgeangebote in Anspruch nehmen können. Bisher ist nur wenig darüber bekannt, inwieweit die vorhandenen Angebote genutzt werden und wie die Nachsorgerealität erlebt und beurteilt wird. Hierzu wurde eine explorative Untersuchung mit Patientinnen und Ärzten durchgeführt. Patientinnen und Methoden: Alle Patientinnen, die zwischen 2007–2013 in einem zertifizierten Brustzentrum operiert wurden, erhielten einen standardisierten Fragebogen; gleichzeitig wurden nachsorgende Ärzte zur Beantwortung eines standardisierten Fragebogens eingeladen. Ergebnisse: 920 Patientinnen (Response-Rate: 61 %) mit einem medianen Alter von 65 Jahren (32–95) konnten analysiert werden. 99 % der Befragten gaben an, regelmäßig zur Nachsorge zu gehen. Der persönliche Kontakt zum Arzt (Mittelwert: 4,4) und die Rückversicherung, dass die Krebserkrankung nicht rezidiviert ist (Mittelwert: 4,5), wurden auf einer Skala von 0 bis 5 als 2 der wichtigsten Nachsorgequalitäten beschrieben. Defizite wurden bez. der psychosozialen Betreuung (70 %) und der Wahrnehmung und Behandlung körperlicher Beschwerden (55 %) geäußert. Zusätzlich beantworteten 105 Ärzte einen Fragebogen (Response-Rate: 12 %). Bei asymptomatischen Patientinnen führten die befragten Ärzte folgende Untersuchungen am häufigsten durch: Anamnese (92 %), körperliche Untersuchung (87 %) sowie Labor (63 %) und Tumormarkerbestimmung (40 %). Schlussfolgerung: Insgesamt wird deutlich, dass eine überwältigende Mehrheit der Patientinnen das Nachsorgeangebot nutzt. Aus der Patientenperspektive liegt die Bedeutung der Nachsorge vor allem im Arztkontakt und in der beruhigenden Rückversicherung, dass die Brustkrebserkrankung nicht rezidiviert ist. Defizite zeigen sich in der psychosozialen Betreuung und in der Wahrnehmung und Behandlung körperlicher Beschwerden. Nicht empfohlene Untersuchungen werden von einem signifikanten Anteil der befragten Ärzte eingesetzt.
Introduction
Early diagnosis and improved therapeutic options have led to better survival rates for breast cancer patients [1], [2], [3], [4], [5]. In Germany at present about 360 000 patients are living in the phase after completed primary therapy [6], [7], and take advantage of the ever increasing number of follow-up options [2], [8].
Under follow-up (aftercare) we mean in general the structured, regular control of asymptomatic patients after a potentially curative tumour therapy [9], [10]. The 2013 revision of the guidelines of the American Society of Clinical Oncology (ASCO) and the currently valid S3 guidelines recommend for all breast cancer patients a personal consultation and physical examination at intervals of 3 to 12 months as well as an annual mammography [11], [12]. Routine blood tests, imaging procedures, except for mammography, and determination of tumour markers, on the other hand, are not recommended for asymptomatic patients [11], [12].
From the point of view of both the patients and the physicians, the main purpose of follow-up is the early detection of local recurrences [2]. In a meta-analysis of over 5000 patients, however, it was shown that only 40 % of the isolated loco-regional recurrences in asymptomatic patients were detected during routine examinations [13], this has often led to the value of follow-up being questioned [14]. Also the detection of asymptomatic distant metastases is not a priority target of follow-up since there is no evidence from randomised studies that an early palliative intervention leads to a longer survival [9], [15], [16]. After completion of the initial breast cancer therapy the focus lies, above all, on the recognition and adequate treatment of long-term toxicities and side effects of the therapy [8], [17], [18], [19], the detection of derivatives of the primary tumour [18], support in the psychosocial field [8] and in continuous motivation to comply with the adjuvant systemic therapy regularly [12].
In the present contribution we have assessed the subjective appraisals of the afflicted patients and the responsible physicians. Our aim was to examine the follow-up situation from various perspectives and to uncover content correlations. The methodological approach was explorative, specific hypotheses were not examined.
Materials and Methods
Methods of the patient survey
All breast cancer patients who were operated in a certified breast cancer centre (Breast Centre Marienhof, Koblenz) between 2007 and 2013 were identified and personally approached in writing. The letter, signed by the treating physician, explained the aims and methodological procedures of the survey and provided information on the handling of personal data. Reminders were not sent after the first letter, nor were the patients contacted personally or by telephone. A stamped and addressed envelope was provided for the patients to return the completed questionnaire at no cost to themselves. The data were entered via machine by a service provider and checked for completeness.
The scannable, standardised questionnaire was evaluated in a pre-test and its content covered the following points: adjuvant therapies received, participation in clinical trials, utilisation of follow-up options, evaluation of follow-up intervals and duration, motivation to participate in follow-up examinations, distress in connection with the follow-up appointments, wishes and suggestions about follow-up and sociodemographic characteristics.
In addition, the medical treatment parameters of all patients were extracted from the patient records and transferred to a database. In this way, the treatment data of responders and non-responders could be compared and checked for systematic selection effects.
Methods of the physician survey
Physicians from a regional database who regularly receive invitations to participate in gynaeco-oncological further training events were also contacted in writing and invited to complete a scannable questionnaire. Reminders were again not sent to this group. Participating physicians could return the completed questionnaire in anonymous form by means of the supplied stamped and addressed envelope; these data were also entered via machine.
The previously evaluated questionnaire covered the following contents: medical setting, coordination of follow-up, performed or prescribed follow-up examinations, judgement of the recommended follow-up duration and intensity as well as of the aims and content of the follow-up.
In the questionnaires, treating physicians and patients evaluated several statements on the subject of follow-up using a 6-point scale with the endpoints “0” “not correct at all” or, respectively, “not at all important” and “5” “fully correct” or, respectively “very important”.
Statistical considerations
Statistical analyses were performed with the help of SPSS 19. Frequencies and statistical measures of location were calculated as were mean values for interval-scaled data and median values for ordinally scaled data.
The analyses were done almost exclusively on a descriptive level. Assessment of statistical significance was performed with the help of the t test for independent samples.
A calculation of case numbers was not done on account of the explorative character of the investigation.
Data protection and ethical vote
The ethics commission of the Chamber of Medicine of Rhineland Palatinate has given its approval for this project. The patients have declared their agreement to the scientific utilisation of their pseudo-anonymised data.
Results
Non-responder analysis
N = 1520 female patients were approached, 920 returned the complete questionnaire (response rate 61 %). The non-responders were on average 66.5 years old and thus about 2 years older than the responders (p = 0.002). 54 % of the non-responders had undergone breast-conserving operations, in comparison to 51 % of the responders.
Results of the patient survey
At the time of the survey the average age of the 920 patients was 64.4 years (standard deviation: 11.4 years). The time period between the last operation and the survey amounted to 3.7 years on average (standard deviation: 2.0 years). For 82 % of the patients the systemic therapy consisted of radiotherapy, 79 % received an anti-hormonal therapy, 6 % a neoadjuvant and 43 % adjuvant chemotherapy. At the time of the survey 58 % were still under therapy, mostly anti-hormonal (94 %). 11 % reported that they had participated in a clinical trial within the framework of their treatment, namely 16 % of the under 60 and 7 % of the over 70 year olds. The patient characteristics are presented in [Table 1].
|
Gender |
|
|
n = 920 (100 %) |
|
Age at the time of the survey |
|
|
64.4 years (11.4 years) |
|
UICC stage |
|
|
n = 444 (48 %) |
|
n = 329 (36 %) |
|
n = 81 (9 %) |
|
n = 66 (7 %) |
|
Year of the last OP |
|
|
n = 219 (24 %) |
|
n = 366 (40 %) |
|
n = 319 (35 %) |
|
n = 16 (2 %) |
|
Adjuvant therapies (multiple answers possible) |
|
|
n = 755 (82 %) |
|
n = 731 (79 %) |
|
n = 58 (6 %) |
|
n = 395 (43 %) |
|
Therapy at the time of the survey |
|
|
n = 502 (58 %) |
|
n = 371 (42 %) |
|
Participation in clinical trials according to subgroup |
|
|
n = 97 (11 %) |
|
n = 52 (16 %) |
|
n = 25 (9 %) |
|
n = 20 (7 %) |
|
Health insurance |
|
|
n = 720 (78 %) |
|
n = 171 (19 %) |
|
n = 29 (3 %) |
94 % of the patients were still in the follow-up phase at the time of the survey, 5 % had already finished the follow-up phase. Nine of the participants (1 %) had never taken part in a follow-up option: 0.3 % of the under 70 and 2.3 % of the over 70 year olds. Four of the 9 patients had specifically decided against the follow-up options.
Gynaecologists were involved in 97 % of the follow-up procedures, 65 % additionally mentioned radiologists. Oncologist (17 %) and general practitioners (16 %) on the other hand were less strongly involved. A physical examination (93 %) and mammography (90 %) constituted the basis of the follow-up, in addition sonography of the breast or, respectively, axilla (81 %) and laboratory tests (56 %) were mentioned as diagnostic procedures that had been employed at least once per patient.
The current examination interval was considered to be “perfect” by 93 % of the participants. The 12-month interval was somewhat more critically assessed in comparison with the 6- and 3-month intervals: 87 % considered it to be “just right”, in contrast, for 5 % it was too short and for 9 % too long.
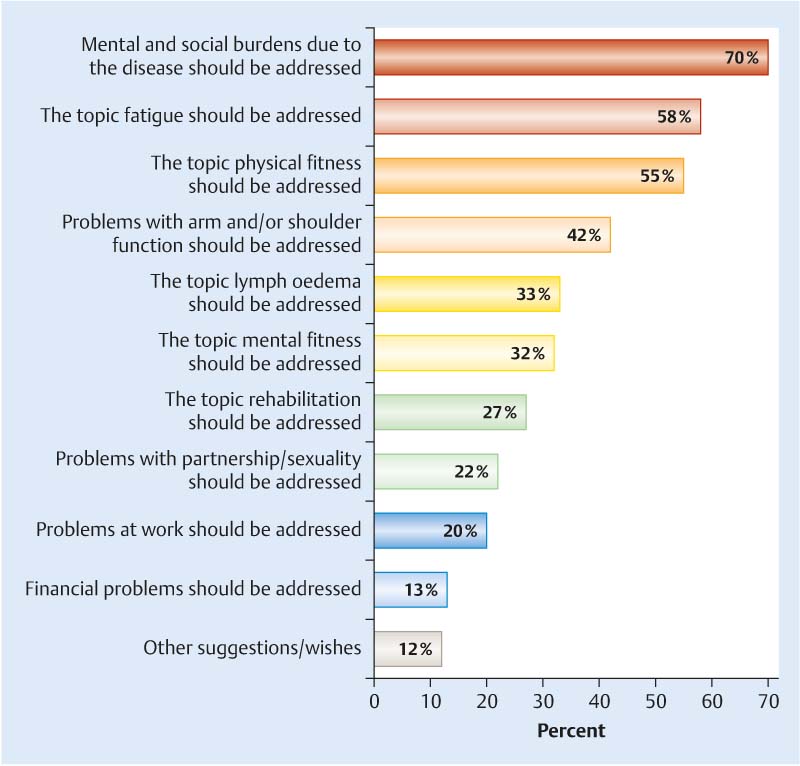
The mean values of the assessed statements showed that the follow-up was considered to be important for the patientʼs own health (4.7) and that an unremarkable result has a comforting effect (4.5). The majority considered themselves to be optimally managed (4.4) or, respectively, well cared for (4.4) and appreciated the contact with their physician (4.4). The average values of the individual items are presented in [Table 2]. Deficits were expressed with regard to psychosocial care (70 %) and the detection and treatment of physical complaints (55 %) ([Fig. 1]).
|
Mean value |
Number of cases |
Standard deviation |
|
|---|---|---|---|
|
The questions on the topic follow-up were answered with the help of a 6-point scale with the endpoints “not at all correct” (0) to “fully correct” (5). |
|||
|
Follow-up gives me a secure feeling of being healthy. |
4.3 |
886 |
1.13 |
|
For me contact with the physician is important in the follow-up. |
4.4 |
861 |
1,12 |
|
For me the follow-up is a troublesome burden that I must endure. |
0.8 |
781 |
1,48 |
|
An unremarkable follow-up result is comforting for me. |
4.5 |
857 |
1.14 |
|
Follow-up appointments already mean stress for me. |
2.1 |
807 |
1.88 |
|
I feel well cared for in the follow-up sessions. |
4.4 |
876 |
1.13 |
|
I feel optimally managed in the follow-up sessions. |
4.4 |
867 |
1.03 |
|
Follow-up is important for me and my health. |
4.7 |
876 |
0.84 |
|
Mental and psychological consequences of the disease are given adequate consideration in the follow-up. |
2.7 |
781 |
1.86 |
Considering all patients together, follow-up appointments were associated with a mean stress level of 2.1. The mean burden recorded with the help of a distress thermometer achieved a value of 4. On applying the usual cut-off value of ≥ 5 [20], 45 % of the patients experienced above average stress before a follow-up appointment. Radiological examinations, in comparison to other follow-up appointments, were considered to be especially stressful (median 5 vs. median 3). In these cases uncertainty or even anxiety about the examination result created distress (64 %).
Results of the physician survey
Of the 905 physicians approached, 105 returned the completed questionnaire (response rate 12 %). On average each of the participating physicians managed 10 follow-up patients per year (between 0 and 350), further characteristics of the participating physicians are given in [Table 3]. In 51 % of the institutions there was a fixed follow-up scheme, a written follow-up plan on the other hand in merely 14 %. An overview of the employed examination methods is given in [Table 4]; anamnesis (92 %) and physical examinations (87 %) were of central importance for almost all of the participating physicians. 88 % considered the recommended follow-up intervals to be “exactly right”, even if it was departed from in 5 % of patients (median). Altogether, the participants were satisfied with the international guidelines (3.5), although the recommended duration was considered to be too short by 38 %. From the physicianʼs point of view the most important aspects of follow-up are the early detection of recurrences and secondary tumours (4.8), calming the patient or reducing her anxiety (4.7), treatment of side effects of the therapy (4.5) and support in cases of psychosocial stress (4.5). The mean values for the individual items are listed in [Table 5].
|
Specialty |
|
|
n = 54 (51 %) |
|
n = 31 (30 %) |
|
n = 8 (8 %) |
|
n = 6 (6 %) |
|
n = 4 (4 %) |
|
n = 2 (2 %) |
|
Main focus of work |
|
|
n = 96 (92 %) |
|
n = 2 (2 %) |
|
n = 6 (6 %) |
|
Number of follow-up patients personally managed per year |
|
|
n = 28 (30 %) |
|
n = 28 (30 %) |
|
n = 23 (25 %) |
|
n = 13 (14 %) |
|
Anamnesis |
n = 84 (92 %) |
|
Physical examination |
n = 79 (87 %) |
|
Laboratory test/blood chemistry |
n = 57 (63 %) |
|
Sonography of the breasts |
n = 45 (49 %) |
|
Mammography |
n = 41 (45 %) |
|
Sonography of the liver |
n = 41 (45 %) |
|
Determination of tumour markers |
n = 36 (40 %) |
|
Sonography of the axilla |
n = 35 (38 %) |
|
X-ray of the thorax |
n = 19 (21 %) |
|
Bone scintigraphy |
n = 13 (14 %) |
|
MRI |
n = 10 (11 %) |
|
CT |
n = 8 (9 %) |
|
PET/PET-CT |
n = 1 (1 %) |
|
Other examinations |
n = 7 (8 %) |
|
Mean value |
Number of cases |
Standard deviation |
|
|---|---|---|---|
|
The importance of the individual aspects was reported with the help of a 6-point scale with endpoints “not at all important” (0) to “very important” (5). |
|||
|
Early detection of local recurrences and secondary tumours |
4.8 |
93 |
0.72 |
|
Early detection of distant metastases |
4.4 |
93 |
1.07 |
|
Quality assurance for the primary therapy |
4.4 |
90 |
0.88 |
|
Calming/reducing the patientsʼ anxiety |
4.7 |
94 |
0.53 |
|
Suggestions in life-style questions |
4.1 |
94 |
0.91 |
|
Support in smoking cessation |
3.5 |
93 |
1.32 |
|
Discussion and support in cases of mental/psychosocial stress |
4.5 |
94 |
0.68 |
|
Consultations on the topic fatigue |
4.2 |
94 |
0.84 |
|
Help in socio-medical/socio-legal problems |
3.9 |
94 |
1.01 |
|
Consultations on partnership and sexuality problems |
3.9 |
94 |
1.08 |
|
Detection and treatment of side effects of therapy |
4.5 |
92 |
0.69 |
|
Information/support in cases of surgical interventions to improve the cosmetic results of breast surgery |
3.8 |
94 |
1.13 |
|
Recognition of family risks and, if necessary, proposal of prevention options |
4.1 |
92 |
0.89 |
|
Monitoring the compliance/adherence with adjuvant therapies |
4.0 |
91 |
0.93 |
|
Recognition and, if necessary, treatment of long-term toxicities of the therapy |
4.2 |
92 |
0.82 |
The highest agreements from the side of the physicians were reached for the following statements: “the follow-up should be more individualised and risk adapted” (3.8), “the conversation between physician and patient is the most important aspect of the follow-up” (3.8) and “follow-up examinations are not adequately reimbursed” (3.8). An overview of the mean values is given in [Table 6].
|
Mean value |
Number of cases |
Standard deviation |
|
|---|---|---|---|
|
The agreement with statements on the topic follow-up of the individual aspects was reported with the help of a 6-point scale with endpoints “do not agree at all” (0) to “agree completely” (5). |
|||
|
The data upon which the follow-up recommendations are based are out of date. |
2.9 |
83 |
1.22 |
|
The follow-up should be more individualised and risk adapted. |
3.8 |
89 |
1.11 |
|
There are other useful measures that are not recommended in the current guidelines. |
3.1 |
84 |
1.24 |
|
The majority of the patients are not satisfied with the follow-up in its present form. |
1.5 |
88 |
1.33 |
|
From the medical point of view an adequate adjuvant therapy is more important than the follow-up. |
2.1 |
85 |
1.42 |
|
Follow-up examinations are not adequately reimbursed. |
3.8 |
83 |
1.14 |
|
The conversation between physician and patient is the most important aspect of the follow-up. |
3.8 |
90 |
1.05 |
|
Patients often wish for a more intensive follow-up than that recommended in the guidelines. |
3.3 |
88 |
1.40 |
Discussion
The follow-up of breast cancer patients operates in a complex area of conflict between expectations and desires from the point of view of the patients, interdisciplinary medical activities and clear guideline recommendations whereby their medical efficacy remains uncertain [21].
The expectations of the patients with regard to the duration and frequency of follow-ups vary dramatically [22]. In a discrete choice experiment, the patients preferred follow-up intervals of 3 months [23]; in another survey one third did not want to return to the hospital at all after they had been informed just how rarely metastases were detected during routine clinical examinations [22]. In our study the great majority of the surveyed patients were satisfied with the duration and intervals of the follow-up. Merely 9 % of the patients who were followed-up only once per year considered that the interval was too long. However, for 5 % it was even too short which is possibly indicative of a certain follow-up weariness. Our data support the conclusion that the heterogeneous expectations and preferences of the patients with regard to the length and intensity should be taken seriously and that personalised follow-ups would have the potential for a significant improvement in patient satisfaction [23]. In addition, the individual recurrence risk should be taken into consideration because the current follow-up intensity is not differentiated on the basis of the tumour biology [24].
Only little is known about the actual conduct of clinical experts and whether or not they act in accord with the guidelines [24]. In our survey numerous not recommended diagnostic procedures were mentioned and employed by a significant proportion of the participants. In this respect blood and/or laboratory tests (63 %), the determination of tumour markers (40 %) and sonographic examinations of the liver (45 %) are of primary interest. These results are in agreement with a current study in which the use of not recommended diagnostic procedures was frequently seen in follow-up patients; 55 % underwent a not recommended imaging procedure and 79 % at least one not recommended biomarker test [25]. The results of other studies revealed that 97 % of all patients underwent a physical examination and that mammography was not employed as frequently as is recommended [26], [27]. In numerous studies reported in the literature it is consistently seen that the actual use of mammography is too low over the entire study period [18], [28] and is offset against the routine use of not recommended examination methods [24], [25], [29].
In the light of the observed over- or underuse of diagnostic methods, we can only speculate about the motivations of the patients and their physicians in the face of the available evidence from prospective studies [30], [31], [32]. Attempts at explanations from the patientʼs point of view are the reduced concern with regard to the risk of breast cancer, other medical needs, or a low perception of the usefulness of follow-up [18]. A general dissatisfaction with the international guidelines among the participating physicians cannot be deduced although one can certainly imagine a more individual and risk-adapted procedure. Finally, the physicians are also influenced by the expectations of their patients. In a patient survey it was mentioned that one of the most important activities of the physician was not to follow the symptom-oriented follow-up guidelines [7]. In several studies the patients also preferred a more intensive follow-up scheme [2], [24], [29], [33] and tighter controls [34].
The needs and preferences of the patients are thus in contradiction to the available evidence concerning the efficacy of follow-up examinations [33]. The fact that patients believe that they have a better chance of survival through more tests and the early detection of metastases and recurrences [29], however, does mean that they have not been adequately informed of the basic aims of the follow-up [33].
In conclusion, the question therefore arises about the function and practical implementation of the follow-up options. Since the incidence of local recurrences is low, huge efforts have to be made in routine follow-up to achieve the early diagnosis of a very small number of curable local recurrences [13]. This clearly illustrates the discrepancy between the expectations of the patients and the physiciansʼ possibilities who consider the central reassurance desired by the patients that the disease has not recurred to be unrealistic [2]. Follow-up should thus be more than solely the detection of recurrences [21], [35]. After completion of their primary therapy and also under an adjuvant therapy patients often suffer from somatic and mental complaints, lymph oedemas, fatigue, polyneuropathies and need support in their social and professional fields [19]. The feeling of security of an active treatment and its associated supportive milieu [1] is lost and its place taken by a real anxiety of recurrence, this should be adequately addressed in a comprehensive and personalised follow-up.
This was also apparent in the present study because a significant proportion of the participating patients reported on deficits in psychosocial care and in the appreciation and treatment of physical complaints in the framework of the follow-up. However, for a structured further treatment and follow-up and the thus associated emotional relief on the patient side, the physicians require sufficient time that is currently not appropriately reimbursed. By means of the follow-up appointments contact with the physician is maintained so that long-term sequelae of disease and therapy can be managed adequately. Follow-up also serves for quality assurance of the primary therapy and supports the consequent continuation of adjuvant anti-HER2- and/or anti-hormonal therapies. Aims, limitations and benefits of the follow-up should be discussed comprehensively with the patients at the very beginning of the follow-up to enable the patient to make an informed decision.
The strength of the present study lies in the population of more than 900 non-selected breast cancer patients who were followed-up in quite different facilities. The coupling of objective treatment data and subjective estimations of the patients not only opens up a further perspective but also makes a non-responder analysis possible. The high response rate of 61 % and the results of the non-responder analysis back up the validity and representativeness of the collected data even when the responders were on average somewhat younger than the non-responders. Against the background of a 99 % participation rate in follow-up options, however, it must be critically questioned if the study population is really representative for all breast cancer patients. It is possible that primarily women who actively use the follow-up options considered themselves to be directly addressed by the survey.
Since only few studies have been concerned with the opinions of physicians on the topic follow-up [5], the evaluations of more than 100 treating physicians represent a special feature of the project. However, the low response rate of 12 % provides grounds for criticism. Comparable rates of between 9 and 57 % can be found in the literature [14], [24], [36], [37], [38], [39], however, these surveys were often initiated by professional organisations such as, for example, ASCO. Selection effects in the sense that first and foremost those physicians participated for whom the follow-up of breast cancer patients represents an important and practically relevant topic can thus not be discounted.
Conclusions
The great majority of patients take advantage of follow-up options. From the patientʼs perspective the importance of the follow-up lies above all in contact with the physician and the comforting reassurance that the breast cancer disease has not recurred. Deficits are seen in psychosocial care and the appreciation and treatment of physical complaints. Not recommended examinations are employed by a significant proportion of the physicians.
Acknowledgements
This project was financially supported by “medac, Gesellschaft für klinische Spezialpräparate mbH”.
Conflict of Interest
The authors declare that they have no conflicts of interest.
-
References
- 1 Stanton AL. What happens now? Psychosocial care for cancer survivors after medical treatment completion. J Clin Oncol 2012; 30: 1215-1220
- 2 Kwast AB, Drossaert CH, Siesling S. follow-up working group. Breast cancer follow-up: from the perspective of health professionals and patients. Eur J Cancer Care (Engl) 2013; 22: 754-764
- 3 Hayes DF. Clinical practice. Follow-up of patients with early breast cancer. N Engl J Med 2007; 356: 2505-2513
- 4 Mandelblatt JS, Lawrence WF, Cullen J et al. Patterns of care in early-stage breast cancer survivors in the first year after cessation of active treatment. J Clin Oncol 2006; 24: 77-84
- 5 van Hezewijk M, Hille ET, Scholten AN et al. Professionalsʼ opinion on follow-up in breast cancer patients; perceived purpose and influence of patientsʼ risk factors. Eur J Surg Oncol 2011; 37: 217-224
- 6 Bördlein I. Ärzte Zeitung: Medizin.. Online: http://www.aerztezeitung.de/medizin/krankheiten/krebs/mamma-karzinom/article/337165/brustkrebsnachsorge-noch-zeitgemaess-aerzte-betroffene-wollen-verbessertes-screening-metastasen.html?sh=25&h=502751114 last access: 19.12.2014
- 7 mamazone. Umfragen/Ergebnisse unserer Umfragen/Nachsorge-Umfrage.. Online: http://www.mamazone.de/fileadmin/downloads/Umfragen/Nachsorgeumfrage_Ergebnisse_2009.pdf last access: 19.07.2015
- 8 Bessen T, Chen G, Street J et al. What sort of follow-up services would Australian breast cancer survivors prefer if we could no longer offer long-term specialist-based care? A discrete choice experiment. Br J Cancer 2014; 110: 859-867
- 9 Ochsner A, Zuber M, Viehl CT. Tumornachsorge nach potentiell kurativer Resektion eines Karzinoms. Ther Umsch 2012; 69: 49-55
- 10 Zuber M, Viehl CT, Güller U et al. Nachsorge-Empfehlungen für Patientinnen mit kurativ therapiertem, invasivem Mammakarzinom. Ther Umsch 2008; 65: 319-321
- 11 Khatcheressian JL, Hurley P, Bantug E et al. American Society of Clinical Oncology: Breast cancer follow-up and management after primary treatment: American Society of Clinical Oncology clinical practice guideline update. J Clin Oncol 2013; 31: 961-965
- 12 Deutsche Gesellschaft für Senologie. Publikationen/Leitlinien.. Online: http://www.senologie.org/fileadmin/downloads/S3-Brustkrebs-v2012-OL-Kurzversion.pdf last access: 19.12.2014
- 13 de Bock GH, Bonnema J, van der Hage J et al. Effectiveness of routine visits and routine tests in detecting isolated locoregional recurrences after treatment for early-stage invasive breast cancer: a meta-analysis and systematic review. J Clin Oncol 2004; 22: 4010-4018
- 14 Donnelly P, Hiller L, Bathers S et al. Questioning specialistsʼ attitudes to breast cancer follow-up in primary care. Ann Oncol 2007; 18: 1467-1476
- 15 Henry NL, Hayes DF, Ramsey SD et al. Promoting quality and evidence-based care in early-stage breast cancer follow-up. J Natl Cancer Inst 2014; 106: dju034
- 16 Earle CC, Ganz PA. Cancer survivorship care: donʼt let the perfect be the enemy of the good. J Clin Oncol 2012; 30: 3764-3768
- 17 Kukar M, Watroba N, Miller A et al. Fostering coordinated survivorship care in breast cancer: who is lost to follow-up?. J Cancer Surviv 2014; 8: 199-204
- 18 Lu W, Jansen L, Schaapveld M et al. Underuse of long-term routine hospital follow-up care in patients with a history of breast cancer?. BMC Cancer 2011; 11: 279
- 19 Feiten S, Dünnebacke J, Heymanns J et al. Breast cancer morbidity: questionnaire survey of patients on the long term effects of disease and adjuvant therapy. Dtsch Arztebl Int 2014; 111: 537-544
- 20 Mehnert A, Lehmann C, Koch U. Distress Thermometer. In: Herschbach P, Weis J, Hrsg. Screeningverfahren in der Psychoonkologie. Testinstrumente zur Identifikation betreuungsbedürftiger Krebspatienten. Eine Empfehlung der PSO für die psychoonkologische Behandlungspraxis. 2. Aufl. Berlin: DKG; 2010: 14-18
- 21 Chopra I, Chopra A. Follow-up care for breast cancer survivors: improving patient outcomes. Patient Relat Outcome Meas 2014; 5: 71-85
- 22 Montgomery DA, Krupa K, Wilson C et al. Patientsʼ expectations for follow-up in breast cancer—a preliminary, questionnaire-based study. Breast 2008; 17: 347-352
- 23 Kimman ML, Dellaert BG, Boersma LJ et al. Follow-up after treatment for breast cancer: one strategy fits all? An investigation of patient preferences using a discrete choice experiment. Acta Oncol 2010; 49: 328-337
- 24 Margenthaler JA, Allam E, Chen L et al. Surveillance of patients with breast cancer after curative-intent primary treatment: current practice patterns. J Oncol Pract 2012; 8: 79-83
- 25 Hahn EE, Hays RD, Kahn KL et al. Use of imaging and biomarker tests for posttreatment care of early-stage breast cancer survivors. Cancer 2013; 119: 4316-4324
- 26 Grandjean I, Kwast AB, de Vries H et al. Evaluation of the adherence to follow-up care guidelines for women with breast cancer. Eur J Oncol Nurs 2012; 16: 281-285
- 27 Schapira MM, McAuliffe TL, Nattinger AB. Underutilization of mammography in older breast cancer survivors. Med Care 2000; 38: 281-289
- 28 Grunfeld E, Hodgson DC, Del Giudice ME et al. Population-based longitudinal study of follow-up care for breast cancer survivors. J Oncol Pract 2010; 6: 174-181
- 29 Schmidt S. Aktuelle Nachsorge beim Mammakarzinom: Ergebnisse einer Umfrage im Großraum München. [Dissertation]. München: LMU; 2013
- 30 Impact of follow-up testing on survival and health-related quality of life in breast cancer patients. A multicenter randomized controlled trial. The GIVIO Investigators. JAMA 1994; 271: 1587-1592
- 31 Rosselli Del Turco M, Palli D, Cariddi A et al. Intensive diagnostic follow-up after treatment of primary breast cancer. A randomized trial. National Research Council Project on Breast Cancer follow-up. JAMA 1994; 271: 1593-1597
- 32 Bornhak S, Heidemann E, Meisner C et al. Symptom-oriented follow-up of early breast cancer compared to intensive surveillance. Results of a prospective multicentre study: update and 10-year overall survival. Dtsch Med Wochenschr 2012; 137: 2142-2148
- 33 de Bock GH, Bonnema J, Zwaan RE et al. Patientʼs needs and preferences in routine follow-up after treatment for breast cancer. Br J Cancer 2004; 90: 1144-1150
- 34 mamazone. Umfragen/Ergebnisse unserer Umfragen.. Online: http://www.mamazone.de/fileadmin/downloads/Umfragen/2012/Report_UmfrageMitUndNachBrustkrebs.pdf last access: 19.12.2014
- 35 Bördlein I. Patienten nach Krebstherapie: Ziel ist, mehr Rezidive zu verhindern. Dtsch Arztebl 2014; 111: A-1942/B-1658/C-1590
- 36 Paradiso A, Nitti P, Frezza P et al. A survey in Puglia: the attitudes and opinions of specialists, general physicians and patients on follow-up practice. G.S.Bio.Ca.M. Ann Oncol 1995; 6 (Suppl. 02) 53-56
- 37 Tomiak EM, Diverty B, Verma S et al. Follow-up practices for patients with early stage breast cancer: a survey of Canadian oncologists. Cancer Prev Control 1998; 2: 63-71
- 38 Aitken C, Power R, Dwyer R. A very low response rate in an on-line survey of medical practitioners. Aust N Z J Public Health 2008; 32: 288-289
- 39 Stark ME, Crowe jr. JP. Breast cancer evaluation and follow-up: a survey of The Ohio Chapter of The American College of Surgeons. Am Surg 1996; 62: 458-460
Correspondence
-
References
- 1 Stanton AL. What happens now? Psychosocial care for cancer survivors after medical treatment completion. J Clin Oncol 2012; 30: 1215-1220
- 2 Kwast AB, Drossaert CH, Siesling S. follow-up working group. Breast cancer follow-up: from the perspective of health professionals and patients. Eur J Cancer Care (Engl) 2013; 22: 754-764
- 3 Hayes DF. Clinical practice. Follow-up of patients with early breast cancer. N Engl J Med 2007; 356: 2505-2513
- 4 Mandelblatt JS, Lawrence WF, Cullen J et al. Patterns of care in early-stage breast cancer survivors in the first year after cessation of active treatment. J Clin Oncol 2006; 24: 77-84
- 5 van Hezewijk M, Hille ET, Scholten AN et al. Professionalsʼ opinion on follow-up in breast cancer patients; perceived purpose and influence of patientsʼ risk factors. Eur J Surg Oncol 2011; 37: 217-224
- 6 Bördlein I. Ärzte Zeitung: Medizin.. Online: http://www.aerztezeitung.de/medizin/krankheiten/krebs/mamma-karzinom/article/337165/brustkrebsnachsorge-noch-zeitgemaess-aerzte-betroffene-wollen-verbessertes-screening-metastasen.html?sh=25&h=502751114 last access: 19.12.2014
- 7 mamazone. Umfragen/Ergebnisse unserer Umfragen/Nachsorge-Umfrage.. Online: http://www.mamazone.de/fileadmin/downloads/Umfragen/Nachsorgeumfrage_Ergebnisse_2009.pdf last access: 19.07.2015
- 8 Bessen T, Chen G, Street J et al. What sort of follow-up services would Australian breast cancer survivors prefer if we could no longer offer long-term specialist-based care? A discrete choice experiment. Br J Cancer 2014; 110: 859-867
- 9 Ochsner A, Zuber M, Viehl CT. Tumornachsorge nach potentiell kurativer Resektion eines Karzinoms. Ther Umsch 2012; 69: 49-55
- 10 Zuber M, Viehl CT, Güller U et al. Nachsorge-Empfehlungen für Patientinnen mit kurativ therapiertem, invasivem Mammakarzinom. Ther Umsch 2008; 65: 319-321
- 11 Khatcheressian JL, Hurley P, Bantug E et al. American Society of Clinical Oncology: Breast cancer follow-up and management after primary treatment: American Society of Clinical Oncology clinical practice guideline update. J Clin Oncol 2013; 31: 961-965
- 12 Deutsche Gesellschaft für Senologie. Publikationen/Leitlinien.. Online: http://www.senologie.org/fileadmin/downloads/S3-Brustkrebs-v2012-OL-Kurzversion.pdf last access: 19.12.2014
- 13 de Bock GH, Bonnema J, van der Hage J et al. Effectiveness of routine visits and routine tests in detecting isolated locoregional recurrences after treatment for early-stage invasive breast cancer: a meta-analysis and systematic review. J Clin Oncol 2004; 22: 4010-4018
- 14 Donnelly P, Hiller L, Bathers S et al. Questioning specialistsʼ attitudes to breast cancer follow-up in primary care. Ann Oncol 2007; 18: 1467-1476
- 15 Henry NL, Hayes DF, Ramsey SD et al. Promoting quality and evidence-based care in early-stage breast cancer follow-up. J Natl Cancer Inst 2014; 106: dju034
- 16 Earle CC, Ganz PA. Cancer survivorship care: donʼt let the perfect be the enemy of the good. J Clin Oncol 2012; 30: 3764-3768
- 17 Kukar M, Watroba N, Miller A et al. Fostering coordinated survivorship care in breast cancer: who is lost to follow-up?. J Cancer Surviv 2014; 8: 199-204
- 18 Lu W, Jansen L, Schaapveld M et al. Underuse of long-term routine hospital follow-up care in patients with a history of breast cancer?. BMC Cancer 2011; 11: 279
- 19 Feiten S, Dünnebacke J, Heymanns J et al. Breast cancer morbidity: questionnaire survey of patients on the long term effects of disease and adjuvant therapy. Dtsch Arztebl Int 2014; 111: 537-544
- 20 Mehnert A, Lehmann C, Koch U. Distress Thermometer. In: Herschbach P, Weis J, Hrsg. Screeningverfahren in der Psychoonkologie. Testinstrumente zur Identifikation betreuungsbedürftiger Krebspatienten. Eine Empfehlung der PSO für die psychoonkologische Behandlungspraxis. 2. Aufl. Berlin: DKG; 2010: 14-18
- 21 Chopra I, Chopra A. Follow-up care for breast cancer survivors: improving patient outcomes. Patient Relat Outcome Meas 2014; 5: 71-85
- 22 Montgomery DA, Krupa K, Wilson C et al. Patientsʼ expectations for follow-up in breast cancer—a preliminary, questionnaire-based study. Breast 2008; 17: 347-352
- 23 Kimman ML, Dellaert BG, Boersma LJ et al. Follow-up after treatment for breast cancer: one strategy fits all? An investigation of patient preferences using a discrete choice experiment. Acta Oncol 2010; 49: 328-337
- 24 Margenthaler JA, Allam E, Chen L et al. Surveillance of patients with breast cancer after curative-intent primary treatment: current practice patterns. J Oncol Pract 2012; 8: 79-83
- 25 Hahn EE, Hays RD, Kahn KL et al. Use of imaging and biomarker tests for posttreatment care of early-stage breast cancer survivors. Cancer 2013; 119: 4316-4324
- 26 Grandjean I, Kwast AB, de Vries H et al. Evaluation of the adherence to follow-up care guidelines for women with breast cancer. Eur J Oncol Nurs 2012; 16: 281-285
- 27 Schapira MM, McAuliffe TL, Nattinger AB. Underutilization of mammography in older breast cancer survivors. Med Care 2000; 38: 281-289
- 28 Grunfeld E, Hodgson DC, Del Giudice ME et al. Population-based longitudinal study of follow-up care for breast cancer survivors. J Oncol Pract 2010; 6: 174-181
- 29 Schmidt S. Aktuelle Nachsorge beim Mammakarzinom: Ergebnisse einer Umfrage im Großraum München. [Dissertation]. München: LMU; 2013
- 30 Impact of follow-up testing on survival and health-related quality of life in breast cancer patients. A multicenter randomized controlled trial. The GIVIO Investigators. JAMA 1994; 271: 1587-1592
- 31 Rosselli Del Turco M, Palli D, Cariddi A et al. Intensive diagnostic follow-up after treatment of primary breast cancer. A randomized trial. National Research Council Project on Breast Cancer follow-up. JAMA 1994; 271: 1593-1597
- 32 Bornhak S, Heidemann E, Meisner C et al. Symptom-oriented follow-up of early breast cancer compared to intensive surveillance. Results of a prospective multicentre study: update and 10-year overall survival. Dtsch Med Wochenschr 2012; 137: 2142-2148
- 33 de Bock GH, Bonnema J, Zwaan RE et al. Patientʼs needs and preferences in routine follow-up after treatment for breast cancer. Br J Cancer 2004; 90: 1144-1150
- 34 mamazone. Umfragen/Ergebnisse unserer Umfragen.. Online: http://www.mamazone.de/fileadmin/downloads/Umfragen/2012/Report_UmfrageMitUndNachBrustkrebs.pdf last access: 19.12.2014
- 35 Bördlein I. Patienten nach Krebstherapie: Ziel ist, mehr Rezidive zu verhindern. Dtsch Arztebl 2014; 111: A-1942/B-1658/C-1590
- 36 Paradiso A, Nitti P, Frezza P et al. A survey in Puglia: the attitudes and opinions of specialists, general physicians and patients on follow-up practice. G.S.Bio.Ca.M. Ann Oncol 1995; 6 (Suppl. 02) 53-56
- 37 Tomiak EM, Diverty B, Verma S et al. Follow-up practices for patients with early stage breast cancer: a survey of Canadian oncologists. Cancer Prev Control 1998; 2: 63-71
- 38 Aitken C, Power R, Dwyer R. A very low response rate in an on-line survey of medical practitioners. Aust N Z J Public Health 2008; 32: 288-289
- 39 Stark ME, Crowe jr. JP. Breast cancer evaluation and follow-up: a survey of The Ohio Chapter of The American College of Surgeons. Am Surg 1996; 62: 458-460