
Subscribe to RSS
DOI: 10.1055/s-0042-1743513
Treatment of Sagittal Plane Instability of the Proximal Interphalangeal Joint through Volar Plate Repair
Article in several languages: English | español
Abstract
Incompetence of the volar plate of the proximal interphalangeal (PIP) joint can cause instability in the sagittal plane, repetitive dorsal dislocations, pain, and functional disability. The authors herein present five cases of repeated dorsal dislocations of the PIP joint secondary to rupture and incompetence of the volar plate. The patients were aged between 17 and 45 years, and the time elapsed from injury to intervention ranged from 16 weeks to 14 years. Volar plate repair was possible in all cases, resulting in joint stabilization. The mean postoperative follow-up period was of 18 months. Of the five cases, the outcomes were excellent in three, good in one, and fair in one, according to the Catalano et al.[2] criteria. Direct volar plate repair is a reliable technique to treat volar plate incompetence resulting in repeated dorsal dislocation of the PIP joint, regardless of the time from injury to intervention.
Keywords
proximal interphalangeal joint - volar plate - hyperextension deformity - swan neck deformity - late volar plate repairIntroduction
Dorsal dislocation of the proximal interphalangeal (PIP) joint is a relatively common injury, especially in sports-related accidents. It can result from an isolated rupture of the volar plate (VP) or, more frequently, from collateral ligament ruptures or fractures at the anterior lip of the base of the middle phalanx.[1] Acute traumatic rupture due to VP hyperextension usually occurs in its distal insertion, at the level of the base of the middle phalanx; less frequently, it happens in the middle zone of the VP or at a proximal location, such as the attachment of the proximal phalanx.[1] Correct treatment with splint and rehabilitation leads to healing in most patients. Incorrect diagnosis or treatment can result in VP incompetence and repeated episodes of dorsal dislocation due to hyperextensions, potentially leading to pain, clicks, functional impotence, deformity, and stiffness in the medium and long terms. According to some authors,[2] [3] VP rupture at the level of its attachment at the base of the middle phalanx can cause chronic deformity due to PIP joint hyperextension, the so-called swan-neck deformity, and a rupture at the level of its attachment in the proximal phalanx causes a pseudo-boutonnière deformity.
Mild incompetence, clinically manifested as minimal hyperextension, is well tolerated; more severe incompetence can cause pain and functional impotence, as the lateral bands of the extensor digitorum muscle slide over the head of the proximal phalanx for PIP joint mobilization.[2] In the long term, this instability can result in joint degeneration, pain, and stiffness.[3] [4]
Treatment aims at restoring VP competence and joint stability. In cases of minimal instability and no clinical repercussions, the initial management is conservative. Failure of the conservative measures, increased instability, or symptoms of pain and functional impotence indicate the need for surgical treatment. This treatment depends on the degree of joint degeneration (direct VP repair, arthroplasty, arthrodesis, corrective osteotomy etc.) and the patient's requirements.
The authors herein present their experience treating chronic dorsal dislocations of the PIP joint by VP repair.
Clinical Cases
The present is a retrospective review of five cases of VP incompetence clinically manifested by repeated dorsal dislocations of the PIP joint. The patients had a mean age of 35.8 years (range: 17 to 45 years), and the time elapsed from trauma to treatment was o 5.26 years (range: 4 months to 14 years) ([Table 1]). The fifth finger was affected in four out of five cases; in the fifth case, the second finger was affected. As for the cause, three patients reported sports-related accidents, and two patients reported work accidents. One patient had a swan-neck deformity with functional impotence for active flexion ([Figure 1]), while the remaining four patients presented hyperextension of the PIP joint with preserved flexion ([Figure 2]). All patients reported several episodes of dorsal dislocations caused by efforts or falls followed by self-reduction.


|
Age (years) |
Finger |
Time |
Preoperative ROM |
Postopoperative ROM |
Follow-up |
Preoperative strength |
Postoperative strength |
Catalano et al.[2] classification |
|
|---|---|---|---|---|---|---|---|---|---|
|
1 |
42 |
5th |
4 months |
-20°– + 5° |
+30°– + 85° |
7 months |
33/48 (68.75%) |
40/55 (72.72%) |
Fair |
|
2 |
34 |
5th |
14 years |
-52°– + 86° |
+15°– + 91° |
13 months |
28/58 (48.27%) |
52/55 (94.54%) |
Good |
|
3 |
41 |
5th |
8 years |
-60°– + 95° |
+5°– + 85° |
15 months |
36/54 (66.66%) |
50/56 (89.28%) |
Excellent |
|
4 |
45 |
2nd |
29 months |
-15°– + 85 ° |
0°– + 90° |
18 months |
50/62 (80.64%) |
58/60 (96.66%) |
Excellent |
|
5 |
17 |
5th |
19 months |
-65°– + 100° |
+5°– + 90° |
27 months |
24/42 (57.14%) |
40/42 (94.23%) |
Excellent |
The patients in the present series had a history of dorsal dislocation of the PIP joint, anteroposterior instability, functional impotence, pain, and absence of lateral instability. In all cases, plain radiographs (on posteroanterior and lateral views) were performed preoperatively to rule out acute fractures, malunions, or degenerative changes; in addition, a magnetic resonance imaging (MRI) scan was requested to assess VP injury.
A functional evaluation performed before and after the intervention measured the range of motion (ROM) and grip strength of the joint with a Jamar (JLW Instruments, Chicago, IL, US) dynamometer. The clinical outcomes were classified as excellent, good, acceptable, and fair according to the Catalano et al.[2] criteria ([Table 2]), which are specific to assess hyperextension lesions at the PIP joint.
|
Catalano et al.[2] classification |
Hyperextension correction |
Flexion contracture |
Pain |
Stability |
|---|---|---|---|---|
|
Excellent |
Complete |
0° to 5° |
No |
Stable |
|
Good |
Complete |
5 to 15° |
No |
Stable |
|
Fair |
Complete |
> 15° |
Yes |
Partially unstable |
|
Poor |
No |
− |
Yes |
Completely unstable |
Surgical Technique
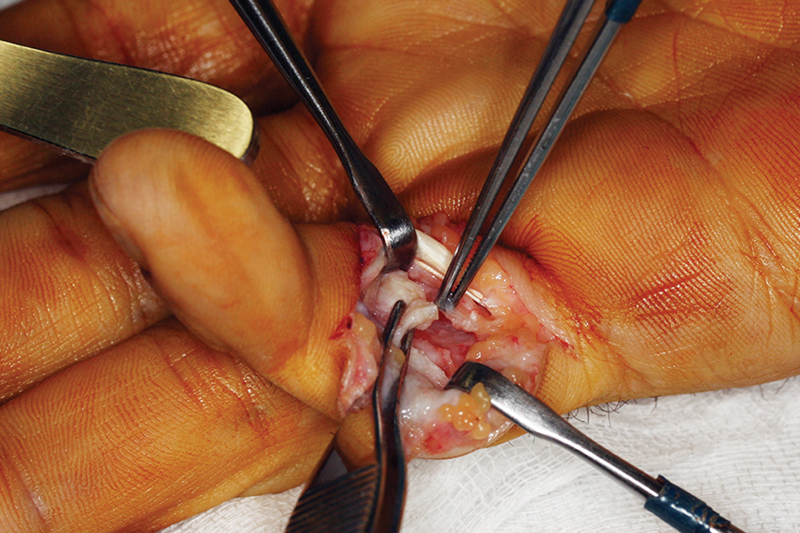
The surgical technique used was VP repair. The VP was exposed using a Bruner-type volar approach and reconstructed after minimal debridement of the affected ends. Central tears deemed repairable were treated directly with a 3/0 absorbable monofilament polydioxanone (PDS, Johnson & Johnson, New Brunswick, NJ, US) suture ([Figure 3]). Distal attachment avulsions ([Figure 4]) were treated with a transosseous reattachment through tunnels at the base of the middle phalanx. In both cases, the tension provided must not exceed 5° of joint flexion[3] [4] to avoid a residual flexion contracture.

Mobilization began at the first postoperative visit, 3 to 4 days after surgery, aided by dorsal splints that limited extension and enabled flexion ([Figure 5]). Initially, the extension was limited to -15°, and the patient was advised to seek full active flexion. The extension limit was reduced progressively every week until full extension, around the third or fourth weeks, when the splints were removed. At this stage, the patients were capable of performing full flexion, so our attention focused on avoiding a potential extension deficit due to flexion contracture with the overnight use of static splints or digital dynamic extension splints to correct it.

Results
The intraoperative findings showed central VP tear in two cases ([Figure 3]), and distal avulsion in three cases ([Figure 4]). The VP could be repaired or reattached in all cases, with correction of the hyperextension and swan-neck deformity, and no recurrences during the follow-up. There were no major complications during the postoperative and rehabilitation periods.
[Table 1] summarizes the clinical outcomes. The mean follow-up period for the 5 patients was of 18 months (range: 7 to 27 months). In the preoperative clinical examination, the mean passive hyperextension was of 42° (range: 15° to 65°). The mean correction of hyperextension was of 39°. Hyperextension was corrected in all patients, and none showed recurrence of the initial deformity. According to the Catalano et al.[2] criteria, which evaluate functional outcomes regarding the PIP joint, three outcomes were excellent, one was good, and one was fair. Of the three excellent cases, two patients eventually presented mean extension deficits of 5°, while the other patient had no deficit. The patient with a good outcome presented a 15° deficit, and the one with a fair outcome had a 30° deficit after surgery.
Grip strength improved 25.4% on average (range: 3.97% to 46.27%).
The patient with a fair outcome (case 1; [Figure 1]) presented to the clinic four months after surgery due to hyperextension resulting in dorsal dislocation. After reduction and immobilization, the patient presented hyperextension with stiffness and inability to perform flexion. An open reduction showed that the cartilage was in good condition and VP reattachment was feasible; later, however, the patient presented stiffness and a contracture at 30° of flexion. Three months after surgery, due to failure of the conservative measures, an arthrolysis was suggested to correct the extension deficit, but the patient refused it. The authors believe that this fair outcome does not result from a lack of rehabilitation or patient collaboration, but from a probable injury to the extensor apparatus.
The radiological examinations showed no signs of joint degeneration during the follow-up until the last visit.
Except for the case with the fair outcome, the rate of patient satisfaction was very high. All patients returned to work.
Discussion
Dorsal dislocation of the PIP joint is a relatively common injury, and, in most cases, patients respond well to conservative treatment, with good functional outcomes. Hyperextension of the PIP joint can produce different degrees of injury, both at the level of the VP and of the collateral ligaments. Most VP injuries heal with no major repercussions. Occasionally, the lack of diagnosis or inadequate treatment can result in chronic instability in the sagittal plane with PIP hyperextension or swan-neck deformity. Some patients may experience pain, functional impotence, instability manifested as repeated dislocation episodes from forced passive hyperextensions, and even osteoarthritis in the long term.[1],[2],[3],[4],[5],[6] These clinical manifestations indicate the need for surgical treatment to provide stability and preserve joint function.
Some authors[5] [6] [7] [8] [9] postulate that the longer the time between injury and treatment, the lower the probability of repair due to theoretical VP scarring, fibrosis, and retraction; they describe different techniques for reconstruction, including flexor digitorum superficialis (FDS) tenodesis and reconstruction with the use of tendon grafts, strips of the lateral band of the extensor digitorum muscle, or collateral ligaments.
In contrast, other authors[2] [3] [4] [5] [6] have described VP repairs with advancement and reattachment 8 to 12 years after the injury, with good functional outcomes. In our opinion, this second approach is more logical because the VP, due to its cartilaginous histological features (meniscus-like structure)[1],[10], suffers no retraction and keeps its structure regardless of the time since the injury,[1] [6] enabling a late repair. The intraoperative macroscopic appearance of the operated VPs (chronic cases) from our series confirmed this fact, since there were no differences compared to acute lesions; as such, their repair was possible, regardless of the time since the injury. The histological features of the VP can account for this finding.[1] [4] [10] Some authors[1] [2] [4] also believe that its vascularization pattern plays a role because the distal portion of the VP is vascularized from the proximal portion by branches of the transverse artery of the proximal digital arch, which connects the two digital arteries at the level of the head of the first phalanx.
Repair of the VP, either by an end-to-end suture for central ruptures or reattachment for avulsions, restores joint stability, correcting the deformity. Polydioxanone, a monofilament suture with a reabsorption time ranging from 180 to 210 days, is used to maintain the tension of the long-term repair. In addition, thanks to its reabsorption by hydrolysis, the PDS disappears, which avoids issues related to the persistence of foreign material at the joint.
Other techniques with higher morbidity, such as FDS tenodesis or reconstruction with tendon grafts, are technically more complex and present a higher risk of flexion contracture. In the Adams[5] series of VP reconstructions using a palmar minor tendon graft, 1 of 3 cases developed a flexion contracture of 25°. Littler[7] described the FDS tenodesis technique in 1959, and Catalano et al.[2] made it popular in 2003. Catalano et al.[2] presented 12 patients, with a mean ROM ranging from 12° to 100° after surgery, and 2 cases of flexion contractures of 60° and 90° respectively.[2] On the other hand, FDS tenodesis can alter the flexor mechanism and increase the risk of tendon adhesions.[5] Swanstrom et al.[6] describe an extra-articular modification of the classic FDS tenodesis using an intraosseous anchor to fix the ulnar hemitendon of the FDS. This technique was performed in 5 patients with a mean follow-up time of 5.5 years, resulting in a ROM ranging from -1 to 96°, with no reports of flexion contracture; in contrast, other tenodesis techniques with an articular approach resulted in flexion contracture ranging from 5° to 90°.[2] [5]
Foucher et al.[8] and Zancolli and Zancolli[9] described extra-articular techniques for the correction of hyperextension deformity. These techniques involved the transfer of strips from the lateral bands of the extensor digitorum muscle and had variable outcomes, with extension deficits ranging from 10° to 30° depending on the method.
The VP can be reattached to the middle phalanx using transosseous sutures,[4] pull-out techniques,[3] or any bone-anchoring system; no method was proven to be clearly superior to the others.[4] Kaneshiro et al.[3] presented 7 cases of VP reattachment using a transosseous pull-out suture with a mean time from injury to surgery of 21 months, and a postoperative follow-up time of 28 months. The average ROM was of 80.5°, with a mean flexion contracture of 9°.[3] Melone et al.[4] presented 25 cases of VP reattachment using a transosseous absorbable (PDS) suture with a mean time from injury to surgery of 8.2 years, and a postoperative follow-up time of 8 years; the mean ROM ranged from 6° to 92°, with flexion contracture ranging from 5° to 15°.
Consistent with other authors,[1] [3] [4] [5] we believe that, despite a long time between injury and repair, late reattachment of the VP is possible and enables a more anatomical reconstruction. It avoids the morbidity of sacrificing healthy structures, such as tendons or ligaments, and its complications, such as loss of strength, instability, adhesions, and/or stiffness, including flexion contractures.[3] [4]
In cases of compensatory swan-neck deformity due to VP incompetence, the treatment plan must include VP reattachment with the technique herein described, which corrected the swan-neck deformity in all treated patients. Had this not been enough, we would have considered personalized splints, Littler-type tenodesis, or reconstruction of the spiral oblique retinaculum ligament as required by each case.[4] [7] [9]
Tenodesis with the FDS may be a good alternative in patients with an irreparable VP.[2] [3] [4] If the radiological study reveals degenerative changes, the therapeutic options include arthroplasty with prosthesis, arthrodesis, or transfer of a vascularized PIP joint from a toe.
Conclusion
Repair is a reliable technique to treat VP incompetency and repeated dorsal dislocations of the PIP joint. It enables the restoration of joint stability and deformity correction with minimal morbidity. Thus, it should be considered an excellent option to treat PIP instability, regardless of the time elapsed since the injury.
Conflict of Interests
The authors have no conflict of interests to declare.
-
References
- 1 Bowers WH. The proximal interphalangeal joint volar plate. II: a clinical study of hyperextension injury. J Hand Surg Am 1981; 6 (01) 77-81
- 2 Catalano III LW, Skarparis AC, Glickel SZ. et al. Treatment of chronic, traumatic hyperextension deformities of the proximal interphalangeal joint with flexor digitorum superficialis tenodesis. J Hand Surg Am 2003; 28 (03) 448-452
- 3 Kaneshiro Y, Hidaka N, Fukuda M, Ota M, Akashi K. Late volar plate repair for chronic, post-traumatic hyperextension deformity of the proximal interphalangeal joint of the little finger. J Plast Surg Hand Surg 2015; 49 (04) 238-241
- 4 Melone Jr CP, Polatsch DB, Beldner S, Khorsandi M. Volar plate repair for posttraumatic hyperextension deformity of the proximal interphalangeal joint. Am J Orthop 2010; 39 (04) 190-194
- 5 Adams JP. Correction of chronic dorsal subluxation of the proximal interphalangeal joint by means of a criss-cross volar graft. J Bone Joint Surg Am 1959; 41-A (01) 111-115
- 6 Swanstrom MM, Henn CM, Hearns KA, Carlson MG. Modified Sublimis Tenodesis: Surgical Technique for Treating Chronic Traumatic Proximal Interphalangeal Joint Hyperextension Instability. Tech Hand Up Extrem Surg 2016; 20 (01) 48-51
- 7 Littler JW. The finger extensor mechanism. Surg Clin North Am 1967; 47 (02) 415-432
- 8 Foucher G, Tilquin B, Lenoble E. [Treatment of post-traumatic swan-neck deformities of the fingers. Apropos of a series of 43 patients]. Rev Chir Orthop Repar Appar Mot 1992; 78 (08) 505-511
- 9 Zancolli EA, Zancolli EJ. Surgical rehabilitation of the spastic upper limb in cerebral palsy. In: Lamb DW. editor. The Paralyzed Hand. London: Churchill Livingstone; 1987: 153-67
- 10 Bowers WH. The proximal interphalangeal joint volar plate. l: An anatomical and biomechanical study. J Hand Surg Am 1981; 6A: 77-81
Address for correspondence
Publication History
Received: 17 June 2020
Accepted: 25 October 2021
Article published online:
23 June 2022
© 2022. SECMA Foundation. This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commecial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/)
Thieme Revinter Publicações Ltda.
Rua do Matoso 170, Rio de Janeiro, RJ, CEP 20270-135, Brazil
-
References
- 1 Bowers WH. The proximal interphalangeal joint volar plate. II: a clinical study of hyperextension injury. J Hand Surg Am 1981; 6 (01) 77-81
- 2 Catalano III LW, Skarparis AC, Glickel SZ. et al. Treatment of chronic, traumatic hyperextension deformities of the proximal interphalangeal joint with flexor digitorum superficialis tenodesis. J Hand Surg Am 2003; 28 (03) 448-452
- 3 Kaneshiro Y, Hidaka N, Fukuda M, Ota M, Akashi K. Late volar plate repair for chronic, post-traumatic hyperextension deformity of the proximal interphalangeal joint of the little finger. J Plast Surg Hand Surg 2015; 49 (04) 238-241
- 4 Melone Jr CP, Polatsch DB, Beldner S, Khorsandi M. Volar plate repair for posttraumatic hyperextension deformity of the proximal interphalangeal joint. Am J Orthop 2010; 39 (04) 190-194
- 5 Adams JP. Correction of chronic dorsal subluxation of the proximal interphalangeal joint by means of a criss-cross volar graft. J Bone Joint Surg Am 1959; 41-A (01) 111-115
- 6 Swanstrom MM, Henn CM, Hearns KA, Carlson MG. Modified Sublimis Tenodesis: Surgical Technique for Treating Chronic Traumatic Proximal Interphalangeal Joint Hyperextension Instability. Tech Hand Up Extrem Surg 2016; 20 (01) 48-51
- 7 Littler JW. The finger extensor mechanism. Surg Clin North Am 1967; 47 (02) 415-432
- 8 Foucher G, Tilquin B, Lenoble E. [Treatment of post-traumatic swan-neck deformities of the fingers. Apropos of a series of 43 patients]. Rev Chir Orthop Repar Appar Mot 1992; 78 (08) 505-511
- 9 Zancolli EA, Zancolli EJ. Surgical rehabilitation of the spastic upper limb in cerebral palsy. In: Lamb DW. editor. The Paralyzed Hand. London: Churchill Livingstone; 1987: 153-67
- 10 Bowers WH. The proximal interphalangeal joint volar plate. l: An anatomical and biomechanical study. J Hand Surg Am 1981; 6A: 77-81




