

Subscribe to RSS
DOI: 10.1055/s-0042-1755468
MRI Features of Synchronous Masses in Known Breast Cancer Patients in Predicting Benign Versus Malignant Lesions: A Case Based Review at Tertiary Care Cancer Hospital
Authors
Funding None.

Abstract

Objectives The purpose of this study was to determine the diagnostic accuracy of breast magnetic resonance imaging (MRI) in classifying incidental satellite masses in biopsy-proven breast cancer patients as benign or malignant masses and assessing its impact on surgical management of these patients. We also analyzed the incidence of MRI-detected lesions, which were thereafter assessed with second look ultrasound (US).
Materials and Methods A retrospective study was performed on breast cancer patients presenting from August 01, 2016 to July 31, 2019, with satellite masses seen on base line MRI. Satellite masses were classified as benign and malignant based on MRI features of shape, margin, T2-weighted imaging signals, internal enhancement pattern, enhancement kinetic curves, and diffusion restriction. This was compared with results of histopathological examination. The number of MRI-detected lesions, location of the satellite mass, and type of surgery were also documented.
Results Out of 400 breast cancer patients undergoing MRI breast, 115 patients had multiple masses. Histopathological diagnosis was available for 73 patients; and a total of 93 satellite masses were evaluated. There was evidence of additional masses on second look ultrasound in 21 patients. Of 72 masses classified as malignant on MRI, 58 showed malignant pathological outcome; while out of 21 masses characterized as benign on MRI, 18 turned out to be benign on histopathology. A statistically significant association was found between MRI features and pathological outcome of satellite masses (p = 0.001). The sensitivity, specificity, positive and negative predictive values, and accuracy were 95%, 56%, 80.56%, 85.7% and 81.7%, respectively. Based on these findings, modified radical mastectomy (MRM)/mastectomy was done for 42 patients, 5 patients underwent lumpectomy limited to a single tumor, extended resection done for 14 patients, 5 underwent bilateral breast conservation surgery (BCS), BCS for contralateral breast done for 4 patients undergoing ipsilateral MRM/mastectomy, and bilateral MRM/mastectomies were performed for 2 patients. One patient was lost to follow up.
Conclusion Breast MRI is the most sensitive modality for the assessment of breast cancer and plays an essential role in the detection of additional tumor foci. These findings can modify the surgical approach in these patients. However, considering the low specificity, biopsy of satellite masses is imperative to determine the most appropriate surgical plan.
Keywords
magnetic resonance imaging - breast cancer - synchronous masses - satellite masses - multifocal - multicentricIntroduction
Magnetic resonance imaging (MRI) of the breasts is a useful imaging modality for detection and characterization of breast lesions. Indications for breast MRI include screening of high-risk patients (e.g., patients with BRCA 1 gene), determination of extent of disease and presence of multifocality and multicentricity, assessment of neoadjuvant chemotherapy response, localization of occult primary tumor in patients presenting with histologically proven breast cancer metastasis and in evaluation of breast implant. MRI breast must be evaluated together with clinical history, physical examination, and conventional imaging including mammography and ultrasound.[1] [2]
Breast conservation surgery (BCS) requires precise assessment of extent of disease to avoid inadequate surgical management. MRI is more sensitive than combined sonomammography in the detection of multiple cancer foci especially in heterogeneous and extremely dense breasts and in patients with ductal carcinoma in situ (DCIS), invasive lobular carcinoma and Paget's disease.[3] [4] MRI can detect clinically and mammographically occult cancers with sensitivity ranging from 94 to 100% for invasive carcinoma and from 40 to 100% for DCIS.[5] However, limitations include low specificity, ranging from 40 to 80%, a large number of false-positive findings and difficulty in managing incidentally detected lesions.[6]
The aim of this study was to determine the diagnostic accuracy of MRI in classifying incidental breast masses in biopsy-proven breast cancer patients as benign or malignant masses and correlation with histopathological findings of ultrasound-guided biopsy/FNA and assessing the impact of these findings on surgical management of these patients, i.e., breast conservation therapy versus mastectomy/wider excision. We also wanted to find the incidence of additional satellite masses picked up during second-look ultrasound after MRI that were not documented on initial ultrasound.
Materials and Methods
Our hospital institutional review board approved the retrospective data collection for this study and granted waiver for informed consent for all patients (EX-05–08–19–01). The Hospital Information System (HIS) was reached for records of breast cancer patients undergoing breast MRI from August 01, 2016, to July 31, 2019. In our hospital, MRI breast is performed in conjunction to conventional sonomammography for patients with dense breast, invasive lobular carcinoma, suspected multifocal (MF)/multicentric (MC) disease, young age (less than 30 years) and Paget's disease. We included all patients with satellite masses seen on baseline MRI for which pathological diagnosis was available. Patients with no evidence of satellite lesions on MRI or for which pathological diagnosis was not available were excluded.
Dynamic contrast-enhanced MRI study of breasts was performed with MAGNETOM Vida 3 Tesla (Siemens) and Ingenia 1.5 Tesla (Philips) using a dedicated breast surface coil and the patient in prone position. Noncontrast axial T1, T2, short tau inversion recovery (STIR) and dynamic post-contrast axial and sagittal T1 fat saturation, and subtraction images were acquired after IV administration of contrast medium (0.1 mmol/kg gadovist). Images were reviewed by four radiologists, one had fellowship training in breast imaging followed by 2 years of experience in breast imaging. The other consultant radiologists had 7 to 15 years of experience in breast imaging.
The following data were obtained from HIS: age, sex, laterality, primary diagnosis, location of satellite masses and their distance from main mass, MRI features of satellite masses, histopathology/cytology of satellite masses, documentation of additional masses on second-look ultrasound, and type of surgery performed.
Satellite masses were evaluated for morphology and enhancement patterns according to American College of Radiology (ACR) BI-RADS Atlas fifth edition guidelines.[7] MRI features of shape (round, oval or irregular), margin (circumscribed, not circumscribed [spiculated or irregular]) and T2-weighted image (T2WI) signals (low, intermediate, and high) were documented. Internal enhancement patterns were also assessed (homogeneous, heterogeneous, rim enhancement, dark internal septations).[7] Qualitative assessment of lesion enhancement was done dynamically by plotting signal intensity values after contrast injection. This comprises an initial phase within the first 2 minutes (slow, medium, or fast) and delayed phase after 2 minutes (persistent, plateau, or washout). Type I curve is a pattern of progressive enhancement, type II curve has a rapid initial rise in the signal intensity followed by plateau pattern and type III involves an initial fast increase in enhancement followed by washout pattern.[7] [8] The presence of diffusion restriction (present or absent) was also noted. The satellite masses with at least one malignant feature were categorized as malignant, while masses with all benign features were classed as probably benign.
Typical benign features include smooth margins, lobulated shape with non-enhancing internal septa, and homogenous enhancement with type I kinetic curve. Criteria for malignant features include irregular mass with non-circumscribed margins (irregular or spiculated), T2WI hypointense signal, showing heterogenous or rim-like enhancement or enhancing septations and diffusion restriction. Both type II and III enhancement curves were considered suggestive of malignancy.[2] [8] This was compared with results of histopathological examination. The location of the satellite mass (same or different quadrant in same breast or in opposite breast) and type of surgery were also documented.
Results
From August 01, 2016, to July 31, 2019, MRI breast was performed for 400 patients. Out of these 400 patients, 115 patients had multiple masses on base-line MRI. Histopathological diagnosis was available for 73 patients, 42 patients had single-satellite lesion, 18 patients had two satellite masses, 5 patients had three, and more than three synchronous masses were noted in 8 patients. A total of 93 satellite masses were evaluated. Masses without histopathological correlation were excluded. All patients were females (mean age: 45.6 years; range: 22–81 years). Based on the distance from the main mass and clock location, 38 masses were noted in the same quadrant, 26 in the opposite quadrant, and 29 masses were seen in the opposite breast. There was evidence of additional masses on MRI in 21 patients, which were subsequently noted on second-look ultrasound.
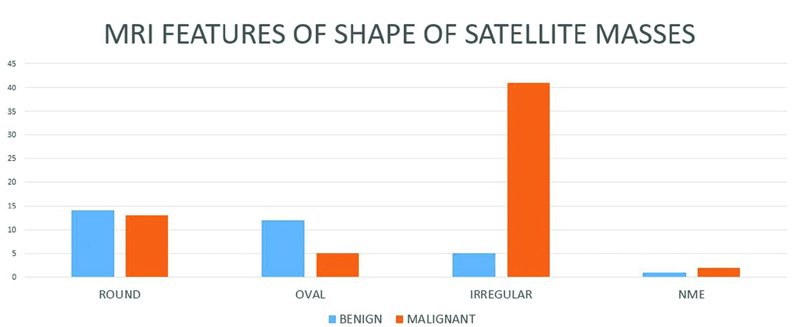
[Fig. 1] shows pathological outcome satellite masses according to the MRI feature of shape of the lesion. Most of the benign masses were round or oval in shape (14 masses; 43.75% and 12 masses; 37.5%, respectively), while 41 out of 61 malignant masses had an irregular shape (67.2%). [Fig. 2] shows that most of the benign masses had circumscribed margins (25 masses; 78.1%); while nearly two-thirds (62.3%) of malignant masses had non-circumscribed margins with spiculated margins noted in 20 masses, and irregular margins in 18 masses. Nonmass enhancement (NME) was observed in three lesions with malignant outcome (ILCa) of two areas of segmental heterogeneous enhancement in the same patient; while focal heterogeneous NME turned out benign (stromal fibrosis). Also, 78.1% of benign masses were bright on T2WI (25 masses). Of malignant masses, only 10 masses were hypointense on T2WI (16.39%), 11 were T2WI intermediate (18%), and 65.56% (40 masses) were hyperintense ([Fig. 3]). Three quarter of benign masses (24 masses) did not restrict diffusion, while diffusion restriction was appreciated in most of malignant masses (49 masses; 80.3%) ([Fig. 4]).



Most of benign masses showed homogenous internal enhancement pattern (21 masses; 65.63%), and showed type I enhancement curve (21 masses; 65.63%). Thirty-six malignant masses had heterogeneous internal enhancement pattern (59%) and 18 masses (29.5%) had homogenous enhancement pattern. Thirty-three masses showed type I enhancement curve (54.1%), 19 masses showed type II (31.15%), while type III curve was seen in only 9 masses (14.75%) ([Figs. 5] and [6]).


Out of 72 masses categorized as malignant on MRI, 58 showed malignant pathological outcome, while out of 21 masses characterized as benign on MRI, 18 turned out to be benign on histopathology. Pearson's chi-square test was used to find an association between MRI findings and final histopathology results. A statistically significant association was found between MRI features and pathological outcome of satellite masses (p = 0.001). The sensitivity, specificity, positive and negative predictive values, and accuracy were 95%, 56%, 80.56%, 85.7% and 81.7%, respectively.
[Fig. 7] shows different types for surgeries performed for patients. Most of patients underwent modified radical mastectomy (MRM)/mastectomy (42 patients). Fifteen patients had a single malignant satellite lesion in the same quadrant, 13 patients had a single satellite mass in a different quadrant, and 5 patients had two malignant satellite masses. This group also included nine patients with a benign satellite mass in the same or contralateral breast. BCS confined to a single presenting malignant mass was done for five patients. The satellite masses in these patients turned out benign on final histopathology/cytology. Extended resection with wire localization of malignant satellite lesion was done for 14 patients. The satellite lesions were located in the same quadrant of primary malignant mass in eight patients, while in different quadrant in six patients. Bilateral BCS was done for five patients due to malignant masses in the opposite breast. MRM/mastectomy with contralateral BCS was done for four patients. Two patients underwent bilateral MRM due to extensive DCIS in one patient, while the second patient had bilateral multicentric ILC. One patient was lost to follow-up.

Discussion
Breast cancer treatment has been revolutionized since the last few decades, with BCS being considered the preferred therapeutic option.[4] BCS requires accurate pre-surgical staging of breast cancer with precise detection of multifocal (MF)/multicentric (MC) and contralateral disease, assessment of patients' risk factors, and multidisciplinary team (MDT) discussion. Multiple tumors are defined by the presence of synchronous invasive tumors in the same breast and are further categorized as MF when there is more than one distinct tumor within the same quadrant of the breast and MC when multiple cancers develop in different quadrants of the breast.[9] MF/MC breast cancers have been reported with an incidence of 40 to 70% in serial sectioning of mastectomy specimens.[10] [11] The incidence of contralateral synchronous tumors ranges from 0.3 to 3%.[12]
Breast MRI is the most sensitive modality for the detection of additional satellite masses that are not detectable with conventional imaging techniques, particularly in scattered fibroglandular or heterogeneously and extremely dense breasts with sensitivity ranging from 94 to 100% for invasive carcinoma and from 40 to 100% for DCIS.[3] [5] It has been reported in earlier studies that MRI has increased sensitivity (81 to 89%) for correct detection of MF/MC cancer in comparison with mammography alone (48 to 72%) or combined sonomammography (26 to 63%).[3] An MRI-detected lesion is defined as an enhancing lesion that is not considered as normal breast parenchyma by breast radiologists and was not detected at conventional imaging or physical examination. An MRI-detected lesion has been documented in 11 to 29% of patients in earlier published studies. This variation is attributed to differences in patient population and definition criteria.[13] Our study showed similar incidence of MRI-detected lesion of 28.8%. The most important disadvantage of breast MRI is low specificity (ranging from 40 to 80%), which means that new MRI-detected lesions must always be biopsied before changing therapy.[6] MRI-guided biopsy and needle localization can be performed, but these methods are not widely available and are both costly and time consuming. Other limitations include contrast administration and difficult approach to posteriorly located lesions.[5] [14] Second-look ultrasound refers to ultrasound examination to locate additional lesions noted on MRI. US-guided biopsy is preferable to MRI-guided biopsy due to easy accessibility, less cost, real-time visualization of lesions, and less patient discomfort.[14]
The MRI features of margins of a mass are most important predictive features of malignant potential. Features suggestive of benign entity are circumscribed masses with smooth margins (NPV 95%). Masses with irregular or spiculated margins are highly suggestive of malignancy (84–91%).[8] [15] Our study showed similar results with most of the benign masses having a lobulated shape with circumscribed margins, while the malignant masses were irregular in shape with non-circumscribed margins. T2 signal hyperintensity in the enhancing part of the circumscribed mass is highly suggestive of benign etiology. A lobulated mass with little or no enhancement is likely benign (NPV 100%).[8] Breast cancers usually appear iso- to hypointense on T2WI (87%); however, T2WI hyperintense signal in irregular or spiculated masses should not be considered a reliable sign of benign histopathology.[2] [8] In contrast to this, most of malignant masses did not appear hypointense on T2WI in our study. Rim-like enhancement in an uncommon feature; however, when present it is highly suggestive of cancer (PPV 84%).[8] [15] Heterogenous internal enhancement pattern and enhancing internal septations are also suspicious for malignancy. Regional nonmass enhancement with a stippled pattern is noted in both benign and malignant conditions. Clumped, heterogenous, and homogenous nonmass enhancement is usually associated with an increased malignancy risk.[8] Type I enhancement curve is usually associated with benign findings with 9% risk of malignancy. The sensitivity and specificity for predicting benign nature were 52.2% and 71%, respectively. Type II curve has 42.6% sensitivity and 75% specificity for the detection of malignancy. Type III curve is usually not observed in benign masses (specificity of 90.4%) but has sensitivity of 20.5%. Both type II and III curves should be considered suspicious for malignancy. Nearly half of malignant masses showed type I enhancement curve in our study. As there is an overlap in enhancement characteristics of benign and malignant masses, reliance on kinetic curve alone should not be done, rather both morphological and kinetic features should be considered during MRI interpretation.[8]
Diffusion restriction was noted in a significant number of satellite masses in this study (sensitivity 85.96%). It has been shown in earlier reported studies that DWI is a useful additional tool for breast cancer diagnosis and ADC values are significantly lower in malignant masses as compared with benign masses or normal breast tissue.[16] The reported sensitivity and specificity in diagnosing malignant masses ranges from 62.5 to 92.8% and 45.8 to 96.7%, respectively.[17] Cai et al demonstrated a marked improvement in the diagnostic performance and specificity of breast MRI in characterization of breast lesions by combining DWI with Dynamic Contrast Enhanced (DCE) MRI.[18]
Sensitivity of MRI in the detection of additional tumor foci leading to a modification in treatment plan has been demonstrated in several studies.[19] Detection of additional tumor foci results in the change in the type of surgery, such as, extended resection, quadrantectomy, or mastectomy, or bilateral surgery due to synchronous MF/bilateral tumors.[20] [21] In our hospital too, the final treatment plan is discussed in MDT after the review of multimodality imaging findings, histopathological diagnosis, hormonal receptor status, axillary and distal metastatic work up results.
There are several limitations in our study. First, it was a retrospective single-center study. Second, we evaluated satellite masses in known breast cancer patients, so our results can be different from masses seen in the screening population. Third, we included only the masses with histopathological diagnosis and excluded a large number, for which the pathological diagnosis was not available. Nevertheless, this study explores different aspects of MRI breast and will surely lead to further prospective studies.
Conclusion
Breast MRI is the most sensitive imaging modality in the accurate assessment of disease extent and the presence of multiple tumor foci in breast cancer patients. However, the major disadvantage is its low specificity. Therefore, biopsy should be performed to ascertain the most appropriate treatment plan.
Conflict of Interest
None.
Acknowledgments
We would like to thank Muhammad Abu Bakar, the Biostatistician and Cancer Epidemiologist Cancer Registry and Clinical Data Management.
Note
This study was presented as an e-poster at the Shaukat Khanum Cancer Symposium in November 2021 and as poster at the Association of Breast Surgery Conference, Liverpool, in May 2022.
Authors' Contributions
Dr. SR contributed to conceptualization, data curation, statistical analysis, literature search, and writing original draft. Dr. BR contributed to data curation, statistical analysis, and editing. Dr. AR contributed to supervision, review, and editing. Dr. IUD contributed to supervision, review, and editing. Dr. AI contributed to supervision, review, and editing. Dr. AJ contributed to data curation and editing. Dr. MAP contributed to supervision, review, and editing.
Institutional Review Board (IRB) Approval
Our hospital's institutional review board approved this retrospective data collection and analysis and granted waiver of informed consent (EX-05–08–19–01).
-
References
- 1 American College of Radiology. ACR practice parameter for the performance of contrast-enhanced magnetic resonance imaging (MRI) of the breast. American College of Radiology; 2018
- 2 Malich A, Fischer DR, Wurdinger S. et al. Potential MRI interpretation model: differentiation of benign from malignant breast masses. Am J Roentgenol 2005; 185 (04) 964-970
- 3 Sardanelli F, Giuseppetti GM, Panizza P. et al; Italian Trial for Breast MR in Multifocal/Multicentric Cancer. Sensitivity of MRI versus mammography for detecting foci of multifocal, multicentric breast cancer in Fatty and dense breasts using the whole-breast pathologic examination as a gold standard. Am J Roentgenol 2004; 183 (04) 1149-1157
- 4 Sardanelli F. Overview of the role of pre-operative breast MRI in the absence of evidence on patient outcomes. Breast 2010; 19 (01) 3-6
- 5 Hong MJ, Cha JH, Kim HH. et al. Second-look ultrasonography for MRI-detected suspicious breast lesions in patients with breast cancer. Ultrasonography 2015; 34 (02) 125-132
- 6 Abe H, Schmidt RA, Shah RN. et al. MR-directed (“Second-Look”) ultrasound examination for breast lesions detected initially on MRI: MR and sonographic findings. Am J Roentgenol 2010; 194 (02) 370-377
- 7 American College of Radiology. . D'Orsi CJ. ACR BI-RADS atlas: breast imaging reporting and data system; mammography, ultrasound, magnetic resonance imaging, follow-up and outcome monitoring, data dictionary. ACR, American College of Radiology; 2013: 125-143
- 8 Macura KJ, Ouwerkerk R, Jacobs MA, Bluemke DA. Patterns of enhancement on breast MR images: interpretation and imaging pitfalls. Radiographics 2006; 26 (06) 1719-1734, quiz 1719
- 9 Middleton LP, Vlastos G, Mirza NQ, Eva S, Sahin AA. Multicentric mammary carcinoma: evidence of monoclonal proliferation. Cancer 2002; 94 (07) 1910-1916
- 10 Tot T. Axillary lymph node status in unifocal, multifocal, and diffuse breast carcinomas: differences are related to macrometastatic disease. Ann Surg Oncol 2012; 19 (11) 3395-3401
- 11 Neri A, Marrelli D, Megha T. et al. “Clinical significance of multifocal and multicentric breast cancers and choice of surgical treatment: a retrospective study on a series of 1158 cases”. BMC Surg 2015; 15 (01) 1
- 12 Rehman S, Niazi IK, Naveed MA, Javaid A, Rehman B. Sonographic evaluation of incidental synchronous masses in patients with breast cancer: clinical significance and diagnostic workup. Eur J Breast Health 2020; 17 (01) 28-35
- 13 Yamaguchi K, Schacht D, Sennett CA. et al. Decision making for breast lesions initially detected at contrast-enhanced breast MRI. Am J Roentgenol 2013; 201 (06) 1376-1385
- 14 Park VY, Kim MJ, Kim EK, Moon HJ. Second-look US: how to find breast lesions with a suspicious MR imaging appearance. Radiographics 2013; 33 (05) 1361-1375
- 15 Liberman L, Morris EA, Lee MJ. et al. Breast lesions detected on MR imaging: features and positive predictive value. Am J Roentgenol 2002; 179 (01) 171-178
- 16 Jiang X, Xie F, Liu L, Peng Y, Cai H, Li L. Discrimination of malignant and benign breast masses using automatic segmentation and features extracted from dynamic contrast-enhanced and diffusion-weighted MRI. Oncol Lett 2018; 16 (02) 1521-1528
- 17 Chen X, Li WL, Zhang YL, Wu Q, Guo YM, Bai ZL. Meta-analysis of quantitative diffusion-weighted MR imaging in the differential diagnosis of breast lesions. BMC Cancer 2010; 10: 693
- 18 Cai H, Liu L, Peng Y, Wu Y, Li L. Diagnostic assessment by dynamic contrast-enhanced and diffusion-weighted magnetic resonance in differentiation of breast lesions under different imaging protocols. BMC Cancer 2014; 14: 366
- 19 Lim HI, Choi JH, Yang JH. et al. Does pre-operative breast magnetic resonance imaging in addition to mammography and breast ultrasonography change the operative management of breast carcinoma?. Breast Cancer Res Treat 2010; 119 (01) 163-167
- 20 Fischer U, Baum F, Luftner-Nagel S. Preoperative MR imaging in patients with breast cancer: preoperative staging, effects on recurrence rates, and outcome analysis. Magn Reson Imaging Clin N Am 2006; 14 (03) 351-362, vi
- 21 Tillman GF, Orel SG, Schnall MD, Schultz DJ, Tan JE, Solin LJ. Effect of breast magnetic resonance imaging on the clinical management of women with early-stage breast carcinoma. J Clin Oncol 2002; 20 (16) 3413-3423
Address for correspondence
Publication History
Article published online:
22 August 2022
© 2022. MedIntel Services Pvt Ltd. This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/)
Thieme Medical and Scientific Publishers Pvt. Ltd.
A-12, 2nd Floor, Sector 2, Noida-201301 UP, India
-
References
- 1 American College of Radiology. ACR practice parameter for the performance of contrast-enhanced magnetic resonance imaging (MRI) of the breast. American College of Radiology; 2018
- 2 Malich A, Fischer DR, Wurdinger S. et al. Potential MRI interpretation model: differentiation of benign from malignant breast masses. Am J Roentgenol 2005; 185 (04) 964-970
- 3 Sardanelli F, Giuseppetti GM, Panizza P. et al; Italian Trial for Breast MR in Multifocal/Multicentric Cancer. Sensitivity of MRI versus mammography for detecting foci of multifocal, multicentric breast cancer in Fatty and dense breasts using the whole-breast pathologic examination as a gold standard. Am J Roentgenol 2004; 183 (04) 1149-1157
- 4 Sardanelli F. Overview of the role of pre-operative breast MRI in the absence of evidence on patient outcomes. Breast 2010; 19 (01) 3-6
- 5 Hong MJ, Cha JH, Kim HH. et al. Second-look ultrasonography for MRI-detected suspicious breast lesions in patients with breast cancer. Ultrasonography 2015; 34 (02) 125-132
- 6 Abe H, Schmidt RA, Shah RN. et al. MR-directed (“Second-Look”) ultrasound examination for breast lesions detected initially on MRI: MR and sonographic findings. Am J Roentgenol 2010; 194 (02) 370-377
- 7 American College of Radiology. . D'Orsi CJ. ACR BI-RADS atlas: breast imaging reporting and data system; mammography, ultrasound, magnetic resonance imaging, follow-up and outcome monitoring, data dictionary. ACR, American College of Radiology; 2013: 125-143
- 8 Macura KJ, Ouwerkerk R, Jacobs MA, Bluemke DA. Patterns of enhancement on breast MR images: interpretation and imaging pitfalls. Radiographics 2006; 26 (06) 1719-1734, quiz 1719
- 9 Middleton LP, Vlastos G, Mirza NQ, Eva S, Sahin AA. Multicentric mammary carcinoma: evidence of monoclonal proliferation. Cancer 2002; 94 (07) 1910-1916
- 10 Tot T. Axillary lymph node status in unifocal, multifocal, and diffuse breast carcinomas: differences are related to macrometastatic disease. Ann Surg Oncol 2012; 19 (11) 3395-3401
- 11 Neri A, Marrelli D, Megha T. et al. “Clinical significance of multifocal and multicentric breast cancers and choice of surgical treatment: a retrospective study on a series of 1158 cases”. BMC Surg 2015; 15 (01) 1
- 12 Rehman S, Niazi IK, Naveed MA, Javaid A, Rehman B. Sonographic evaluation of incidental synchronous masses in patients with breast cancer: clinical significance and diagnostic workup. Eur J Breast Health 2020; 17 (01) 28-35
- 13 Yamaguchi K, Schacht D, Sennett CA. et al. Decision making for breast lesions initially detected at contrast-enhanced breast MRI. Am J Roentgenol 2013; 201 (06) 1376-1385
- 14 Park VY, Kim MJ, Kim EK, Moon HJ. Second-look US: how to find breast lesions with a suspicious MR imaging appearance. Radiographics 2013; 33 (05) 1361-1375
- 15 Liberman L, Morris EA, Lee MJ. et al. Breast lesions detected on MR imaging: features and positive predictive value. Am J Roentgenol 2002; 179 (01) 171-178
- 16 Jiang X, Xie F, Liu L, Peng Y, Cai H, Li L. Discrimination of malignant and benign breast masses using automatic segmentation and features extracted from dynamic contrast-enhanced and diffusion-weighted MRI. Oncol Lett 2018; 16 (02) 1521-1528
- 17 Chen X, Li WL, Zhang YL, Wu Q, Guo YM, Bai ZL. Meta-analysis of quantitative diffusion-weighted MR imaging in the differential diagnosis of breast lesions. BMC Cancer 2010; 10: 693
- 18 Cai H, Liu L, Peng Y, Wu Y, Li L. Diagnostic assessment by dynamic contrast-enhanced and diffusion-weighted magnetic resonance in differentiation of breast lesions under different imaging protocols. BMC Cancer 2014; 14: 366
- 19 Lim HI, Choi JH, Yang JH. et al. Does pre-operative breast magnetic resonance imaging in addition to mammography and breast ultrasonography change the operative management of breast carcinoma?. Breast Cancer Res Treat 2010; 119 (01) 163-167
- 20 Fischer U, Baum F, Luftner-Nagel S. Preoperative MR imaging in patients with breast cancer: preoperative staging, effects on recurrence rates, and outcome analysis. Magn Reson Imaging Clin N Am 2006; 14 (03) 351-362, vi
- 21 Tillman GF, Orel SG, Schnall MD, Schultz DJ, Tan JE, Solin LJ. Effect of breast magnetic resonance imaging on the clinical management of women with early-stage breast carcinoma. J Clin Oncol 2002; 20 (16) 3413-3423