

Subscribe to RSS
DOI: 10.1055/s-0043-1761192
Adipose Mesenchymal Stem Cell Metabolites Oral Gel Enhance Pro-Angiogenic Factors Expression, Angiogenesis, and Clinical Outcome of Oral Ulcer Rat Model
Authors
Funding This study was supported by Hibah Penelitian Tesis Magister (PTM) 2022 from Kementrian Riset dan Teknologi Republik Indonesia with Decree Number 1004/UN3/2022 and Agreement/Contract Number 085/E5/PG.02.00.PT/2022 and 845/UN3.15/PT/2022.

Abstract
Objective Enhancing wound healing capacity is one of the main principles in oral ulcer management. Efficient oral ulcer management will accelerate clinical symptom amelioration and prevent complications. Adipose mesenchymal stem cell metabolites (AdMSCM), a novel biological product, contains a plethora of bioactive mediators that can induce a series of processes in wound healing. This study will analyze the clinical outcome, angiogenesis, and expression of FGF-2 and VEGFA in the oral ulcer rat model after AdMSCM oral gel application.
Materials and Methods Twenty healthy male Wistar rats (Rattus novergicus) were used to create oral ulcer animal models. AdMSCM oral gel treatment was performed three times daily for 3 and 7 days. Clinical outcome was assessed by measuring the major diameter of the ulcer; the angiogenesis was evaluated through histological assessment; the expression of VEGFA and FGF-2 was assessed using the immunohistochemistry method.
Statistical Analysis This study uses parametric comparative analysis using one-way analysis of variance (ANOVA) and post-hoc Tukey's HSD test
Results The application of AdMSCM oral gel in an oral ulcer rat model significantly enhanced the clinical outcome (p < 0.05). In addition, similar results were shown in the histologic assessment of angiogenesis and supported by the significant increase of VEGFA and FGF-2 expression.
Conclusions AdMSCM oral gel accelerates oral ulcer healing processes, proven by the enhancement of angiogenesis, pro-angiogenic factors expression, and clinical outcomes.
Introduction
Accelerating the oral ulcer healing process is pivotal in managing pain and discomfort and preventing complications.[1] The healing process of oral ulcers is a complex mechanism that involves various cellular and molecular components. The ulcer healing mechanism consists of four overlapping spatiotemporal phases: hemostasis, inflammation, proliferation, and remodeling.[2] Under normal conditions, the healing period for oral mucosal ulcers is between 7 and 14 days. Still, several local (e.g., local irritants, infection) and systemic factors (e.g., diabetes mellitus, aging, vascular insufficiencies, medication) may impede the healing process.[2] [3] One of the essential aspects of the healing process is angiogenesis. Angiogenesis is the mechanism of capillaries formation from pre-existing blood vessels. This biological event is pivotal in wound healing because it facilitates adequate blood and nutrient supply and transports many cells and molecular factors to the wound site. The previous study has also reported that insufficient angiogenesis may lead to chronic, non-healing wound formation. The initiation of angiogenesis requires the stimulation of several pro-angiogenic factors, such as vascular endothelial growth factor (VEGF) and fibroblast growth factor-2 (FGF-2).[2] [3] [4]
The current pharmacological approaches for oral ulcers (i.e., topical steroid, non-steroid, and herbal medication therapies) still have several clinical limitations in their use, especially when it comes to managing chronic or extensive oral ulcer cases. For instance, inappropriate timing and dosage of topical corticosteroid drugs can inhibit wound healing due to their anti-inflammatory and anti-mitotic effects.[5] [6] Karavana-Hizarcioğlu et al also identified that the healing rate of oral ulcers treated with benzydamine hydrochloride only differed by 33% compared with the placebo group.[7]
Constant scientific developments, especially in regenerative medicine, have induced the discovery of several therapeutic biological products. Mesenchymal stem cells (MSCs) are one of the most notorious technologies in regenerative medicine that have been widely explored.[8] The recent development of MSCs is utilizing their culture medium, previously regarded as waste, as a highly clinically promising biological product due to its content of various bioactive factors. The collection of these factors is often referred to as mesenchymal stem cell metabolites (MSCM).[9] The proteomic analysis of MSCM has reported that it contains a variety of growth factors, cytokines, chemokines, and interventional RNA (iRNA). Bioactive molecules contained in MSCM have been postulated to interfere with multiple biological activities positively, especially wound healing and tissue regeneration.[9] [10] [11] [12] During the wound healing process, the factors in MSCM can interact with host tissue via the paracrine mechanism, activating several pro-regenerative pathways.[10] Another study reported that metabolites of mesenchymal stem cells (MSCM) are material with good biocompatibility and can induce the proliferation of human gingival somatic cells in in vitro studies.[13] These findings initiate the development of adipose mesenchymal stem cell metabolites (AdMSCM) oral gel as the mean of MSCM application in the oral mucosa. This study will confirm whether the application of AdMSCM oral gel can enhance the expression of VEGFA and FGF-2, angiogenesis, and clinical outcome in oral ulcer rat models.
Materials and Methods
Study Design and Setting
Faculty of Dental Medicine, Universitas Airlangga, Surabaya, Indonesia assigned this study protocol ethical approval for animal laboratories with number 209/HRECC.FODM/IV/2022. This work is a true experimental laboratory study using an analytical post-test control group design. Lemeshow's formula determines the minimum sample; the total sample needed is 20, with five samples for each group. Male Wistar rats (Rattus norvegicus) weighing 250–300 g and 1 to 2 months old made up the sample. The experimental animals were free of any oral and systemic pathologies.
AdMSCM Oral Gel Preparation
The AdMSCM oral gel was acquired from a patent owned by Research Center for Vaccine Technology and Development, Institute of Tropical Disease, Universitas Airlangga, Surabaya, Indonesia. The AdMSCM Gel preparation begins with the collection of plain culture medium after the fourth passage of AdMSC culture. Then, the AdMSC culture medium was purified using the dialysis method to remove the remnants of metabolic products, resulting in the isolated soluble bioactive factors released by AdMSC during culture. The purified culture media was combined with 5% hydroxypropyl-methylcellulose (HPMC) with a 1:3 volume ratio to create AdMSCM oral gel with 30 mg/mL concentration.
Oral Ulcer (OU) Animal Model
An oral ulcer was created using an 8 g/3 mm punch biopsy tool (Premier, Plymouth, USA) on the mucosa of the inferior incisive labial fornix. Then, the base of the tissue was cut using a no. 15 surgical blade.[14] The lesion was then clinically observed 24 hours after punch-biopsy to assess the formation of OU (clinically characterized by a white-colored lesion surrounded by an erythematous arc). While making traumatic ulcers, experimental animals were under general anesthesia using sodium pentobarbital which was injected intramuscularly into the gluteal region.
The oral ulcer treatment in animals was divided into four groups, and they were treated with 5% HPMC (control) and AdMSCM oral gel. The treatment was performed three times daily, using disposable micro applicators (Cotisen, China), for 3 and 7 days. The termination of experimental animals was performed using the cervical dislocation technique. Before termination, the animals were anaesthetized using a single intraperitoneal injection of pentobarbital 50 mg/kg (pentobarbital solution, no. cat: P-010, Sigma Aldrich) systemically (20–40 mL).
Clinical Evaluation of Ulcer's Diameter
The major ulcer diameters of each sample were measured using a fine precision ruler (Fisherbrand, Pittsburg, USA) with a 1 mm increment. The measurement was conducted while the animals were under general anesthesia.
Tissue Preparation
An excisional biopsy of the inferior fornix labial mucosa was conducted for tissue harvesting. The tissues were then fixated in a 10% neutral buffer formalin (NBF) solution (Sigma Aldrich, California, USA) for three days. After that, the tissues were washed three more times with PBS (OneMed, Sidoarjo, Indonesia) for 5 to 10 minutes each. Then, the tissues were embedded in paraffin and sectioned with a rotary microtome to obtain HPA slides.
Histological Evaluation of Angiogenesis
The histopathology slides were processed and stained with hematoxylin–eosin (HE). Then, the angiogenesis of each slide was observed using a light microscope with 100 × , 400 × , and 1000× magnification (Nikon, H600L, Japan) at the Dental Research Center, Faculty of Dental Medicine, Universitas Airlangga. The calculations of the angiogenesis number were performed in five different fields of view by two observers.
Immunohistochemistry
The immunohistochemistry staining was used to evaluate VEGFA and FGF-2 positive expressions in the tissues. The histopathology slides were processed immunohistochemically using horse radish-labeled monoclonal antibodies (anti-VEGFA #SC-7269 (Santa Cruz Biotechnology Inc., California, USA), FGF-2 #SC-74412 (Santa Cruz Biotechnology Inc., California, USA)), and 3–3′ diaminobenzidine (DAB) (Abcam, USA). Then, the positive expression of the protein marked by brown precipitate on the cells of the oral ulcer site was observed using an inverted light microscope with 100 × , 400 × , and 1000× magnification in five different fields of view by two observers.
Statistical Analysis
Statistical analysis was performed using GraphPad Prism 8.0 (for MacBook, v9.4.1, San Diego, USA). The normality test was performed using the Shapiro–Wilk test and the homogeneity test using Levene's test. If the data obtained met the requirements for parametric tests, a one-way analysis of variance (ANOVA) test (p < 0.05) is going to be conducted to find the differences between all groups. If the data did not meet the requirements for a parametric test, a nonparametric test was performed using the Kruskal–Wallis test (p < 0.05). Then, the multiple comparison post-hoc test using Tukey's HSD was performed to uncover specific differences between groups.
Results
In this investigation, it was discovered that the data on the ulcer diameter, angiogenesis, and the expression of VEGFA and FGF-2 was homogeneous and fitted with Gaussian distribution (p > 0.05); thus, comparative parametric analysis using one-way ANOVA was performed with statistical significance is assumed at the p < 0.05.
Clinical Outcome
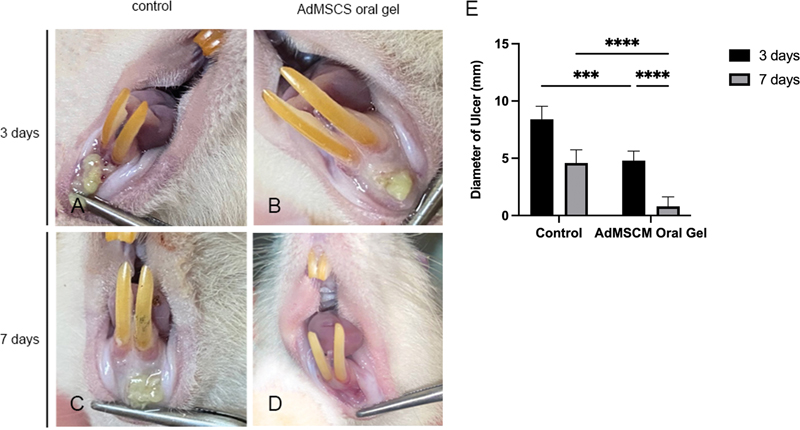
Clinical images showing the oral ulcers after treatment for 3 and 7 days can be seen in [Fig. 1A-1D]. The AdMSCM oral gel treatment groups reveals substantial evidence of a significant reduction in ulcer diameter found after treatment for three (p = 0.0002) and seven days (p < 0.0001) ([Fig. 1E]; [Table 1]).
|
Treatment Duration |
Group |
Ulcer Diameter |
Angiogenesis |
VEGFA |
FGF-2 |
|---|---|---|---|---|---|
|
Mean ± SD |
|||||
|
Three days |
control |
8.4 ± 1.140 |
4.8 ± 1.304 |
2.2 ± 0.837 |
2.2 ± 0.837 |
|
AdMSCM oral gel |
4.6 ± 1.140 |
4.2 ± 1.304 |
4.0 ± 1.000 |
4.8 ± 1.304 |
|
|
Seven days |
control |
4.8 ± 0.837 |
5.2 ± 0.837 |
7.0 ± 1.581 |
7.0 ± 1.581 |
|
AdMSCM oral gel |
0.8 ± 0.837 |
9.0 ± 1.581 |
10.0 ± 1.581 |
11.40 ± 1.140 |
|
|
p-Value |
0.0001* |
0.0001* |
0.0001* |
0.0001[*] |
|
Abbreviations: AdMSCM, adipose mesenchymal stem cell metabolite; FGF-2, fibroblast growth factor-2; OU, oral ulcer; SD, standard deviation. VEGFA, vascular endothelial growth factor A.
* Significant difference of one-way ANOVA represented by p < 0.05.
Angiogenesis
The histologic assessment of angiogenesis in the oral ulcer site is represented in [Fig. 2A-2D]. The AdMSCM oral gel treatment on oral ulcers for three days did not significantly increase the angiogenesis (p = 0.9597). However, significantly higher angiogenesis was found seven days after AdMSCM oral gel treatment (p = 0.0001; [Fig. 2E]; [Table 1]).

FGF-2 Expression
The histopathology view of the FGF-2 expression pattern in the oral ulcer site can be seen in [Fig. 3A-3D]. Brown precipitates in the epithelial layer and connective tissue of the ulcer site mark FGF-2 expression. According to the results of the one-way ANOVA, there were statistically significant differences between all groups (p = 0.0001; [Table 1]). The AdMSCS oral gel demonstrates a significantly higher FGF-2 expression after three (p < 0.0001) and seven days (p < 0.0001) compared with the control ([Fig. 3E]).

VEGFA Expression
The VEGFA expression pattern is marked by brown precipitates in the epithelial layer and connective tissue of the ulcer site, as seen in Figure 4A-4D. The VEGFA expression after AdMSCM oral gel treatment for 3 and 7 days was higher than the control (p = 0.0001 and p < 0.0001, respectively; [Fig. 4E]).

Discussion
AdMSCM oral gel contains a collection of bioactive molecules, such as growth factors, cytokines, chemokines, and noncoding RNAs (e.g., micro RNA [miRNA]) produced by MSCs during culture. The study by Park et al reported that AdMSCM contains more than 40 types of growth factors, mainly EGF, FGF-2, IGF-1, and HGF, which are reported to be able to accelerate the wound healing process via a paracrine mechanism.[9] [10] The same study also reported that the administration of AdMSCM was able to increase the activity of the PI3K/Akt or FAK/ERK1/2 pathways that play a role in regulating the proliferation and migration activity of various skin and oral mucosal cells, such as fibroblasts, keratinocytes, and vascular endothelial cells that will induce the process of wound contraction.[10] In addition, another study by Nugraha et al reported that MSCM is biocompatible, nontoxic, and able to increase the proliferation of human somatic cell culture 12 hours after application.[13] These studies supported the finding of this study that reported the excellent clinical outcome of the AdMSCM oral gel treatment groups.
Limiting inflammatory activity in wound healing is essential for creating an optimal healing process.[15] [16] Previous studies reported that a prolonged inflammatory phase of wound healing would cause the proliferative phase not to be achieved, which may lead to the formation of chronic wounds.[2] [5] In addition to proregenerative effects, AdMSCM oral gel can exert immunomodulatory effects produced by various anti-inflammatory components.[11] AdMSCM contained various soluble anti-inflammatory cytokines (such as TGF-β, IL-10, and PGE-2), extracellular proteins that act as a resolution-associated molecular pattern (RAMPs) (e.g., IDO, HSP10, HSP70), and interference RNAs (e.g., the miR-family).[17] [18] [19] According to research by Zriek et al, the immunomodulatory components of MSCM can interact with immune cells to activate anti-inflammatory regulatory phenotypes.[20]
Macrophages with the M1 phenotype are one of the primary mediators of inflammation in wound healing. Various anti-inflammatory cytokines (e.g., TGF-β and IL-10) present in the AdMSCM oral gel can interact with their respective receptors on macrophages and trigger the polarization of pro-inflammatory macrophages (M1) to anti-inflammatory macrophages (M2). In addition, anti-inflammatory cytokines can also induce the activation of M0 macrophages through the alternative pathways. This theory is proven by Holthauss et al where it was reported that the administration of preconditioned AdMSCM to M0 cells was able to increase the expression of Arg1 and MerTK genes, which are genes that are highly expressed in the activation of the alternative pathway of macrophages (M0 to M2 polarization).[18] The role of RAMPs in the resolution of inflammation was also demonstrated in the study by Borges et al, where HSP70 can produce an anti-inflammatory effect through the activation of the TLR-2 pathway, which will trigger the activation of downstream ERK proteins to induce the production of IL-10.[21] Recent studies have also demonstrated the critical role of miRNAs in the resolution of inflammation in physiological wound healing.[22] [23] The immunomodulatory effect of miRNA is evidenced by the reported role of miR-let7b in triggering M1 to M2 polarization.[24] Accelerated resolution of inflammation in the wound healing process can accelerate the transition to the proliferative phase so that it will indirectly accelerate wound closure, as illustrated in the results of this study.[23] In addition, miRNAs have also been reported to regulate the proliferative phase of wound healing, specifically at the stages of re-epithelialization, angiogenesis, and granulation tissue formation.[22]
This study also reported that the level of angiogenesis that occurred in the treatment group was significantly higher than in the control group (p < 0.05). Angiogenesis is the growth of new capillaries from existing blood vessels.[4] This event occurs in the proliferative phase of the wound-healing process.[2] This process is crucial to creating an effective and optimal wound-healing process.[4] The process of angiogenesis is initiated by an injury that causes microvascular endothelial cells (MEC) that line the tunica intima of blood vessels to be activated by hypoxia and pro-angiogenic factors such as VEGF and FGF-2.[25] Angiogenesis primary function in wound healing is to facilitate oxygen and nutrient supply and transport cells and molecules. The content of pro-angiogenic factors (e.g., VEGF and FGF-2) in the AdMSCM oral gel is thought to have contributed to the findings in this study. Previous study reported similar results, where the application of AdMSCM could significantly increase the expression of CD-31 (platelet endothelial cluster adhesion molecule-1/PECAM1), a specific marker molecule of vascular endothelial cells.[10] Angiogenesis can also be induced by miRNAs contained in MSCM.[19] Previous studies reported that MSCM contains several pro-angiogenic miRNAs, such as miRNA-23a.[19] miRNA-23a can inhibit the prolyl hydroxylase ½ (PHD ½) gene, leading to the accumulation of HIF-1α in vascular endothelial cells, thereby inducing angiogenesis.[26] In addition, miRNA-23a can increase vascular permeability and cell migration which is crucial in angiogenesis.[22]
As the primary pro-angiogenic factor, observing VEGFA expression may indicate the potency of AdMSCM oral gel in enhancing angiogenesis.[4] This study also found that the expression of VEGFA in the AdMSCM oral gel treatment group on the third and seventh days was significantly higher than in the control group (p < 0.05). A similar result was also reported by Sunarto et al, where the administration of MSCM can increase VEGF levels in skin wound model.[27] In addition, similar results were also found in the observation of FGF-2 expression, where the mean FGF-2 expression in the AdMSCM oral gel treatment group on the third and seventh days was significantly higher than the control group (p < 0.05). The importance of FGF-2 in wound healing is not only limited to their function to induce angiogenesis, but also the proliferation of fibroblast in granulation tissue formation phase. FGF-2 able to induce proliferation of human dermal fibroblast via the activation of ERK ½ and JNK pathways.[28] [29] The findings that the expression of these two growth factors in the treatment group was significantly higher than in the control group can be explained by the significant role of M2 macrophages in producing various growth factors that can induce wound healing.[2] [30] Larjava et al reported that M2 macrophages could produce various growth factors relevant to the wound healing process, such as VEGFA, IGF-1, FGF-2, and HGF.[2] [31] As previously mentioned, the immunomodulatory content of the AdMSCM oral gel was able to induce pro-reparative M1 to M2 polarization of macrophages.[30] [32]
Conclusion
This investigation reveals that the topical application of AdMSCM oral gel is able to enhance the clinical outcome, angiogenesis, and expression of VEGFA and FGF-2 in the oral ulcer animal model (R. novergicus). Further exploration through other approaches is still required to evaluate AdMSCM oral gel potency in inducing oral ulcer healing.
Conflict of Interest
None declared.
Acknowledgments
The authors appreciate the support and resources provided by the Research Center for Vaccine Technology and Development, Institute of Tropical Disease, Universitas Airlangga; Dental Research Center, Faculty of Dental Medicine, Universitas Airlangga; Department of Medical Biochemistry; and Animal Research Laboratory, Faculty of Medicine, Universitas Airlangga.
-
References
- 1 Glick M. ed. Burket's Oral Medicine. 12th ed.. People's Medical Publishing House USA; 2015
- 2 Larjava H. ed. Oral Wound Healing: Cell Biology and Clinical Management. Wiley-Blackwell; 2012
- 3 Farah CS. Contemporary Oral Medicine: A Comprehensive Approach to Clinical Practice. Springer Berlin Heidelberg; 2019
- 4 Johnson KE, Wilgus TA. Vascular endothelial growth factor and angiogenesis in the regulation of cutaneous wound repair. Adv Wound Care (New Rochelle) 2014; 3 (10) 647-661
- 5 Landén NX, Li D, Ståhle M. Transition from inflammation to proliferation: a critical step during wound healing. Cell Mol Life Sci 2016; 73 (20) 3861-3885
- 6 Bosanquet DC, Rangaraj A, Richards AJ, Riddell A, Saravolac VM, Harding KG. Topical steroids for chronic wounds displaying abnormal inflammation. Ann R Coll Surg Engl 2013; 95 (04) 291-296 . Doi: 10.1308/003588413 × 13629960045634
- 7 Karavana Hizarcioğlu SY, Sezer B, Güneri P. et al. Efficacy of topical benzydamine hydrochloride gel on oral mucosal ulcers: an in vivo animal study. Int J Oral Maxillofac Surg 2011; 40 (09) 973-978
- 8 Bunnell BA. Adipose tissue-derived mesenchymal stem cells. Cells 2021; 10 (12) 3433
- 9 Ahangar P, Mills SJ, Cowin AJ. Mesenchymal stem cell secretome as an emerging cell-free alternative for improving wound repair. Int J Mol Sci 2020; 21 (19) 7038
- 10 Park SR, Kim JW, Jun HS, Roh JY, Lee HY, Hong IS. Stem cell secretome and its effect on cellular mechanisms relevant to wound healing. Mol Ther 2018; 26 (02) 606-617
- 11 Ajit A, Ambika GopalankuttyI. Adipose-derived stem cell secretome as a cell-free product for cutaneous wound healing. Biotech 2021; 11 (09) 413
- 12 Ferreira JR, Teixeira GQ, Santos SG, Barbosa MA, Almeida-Porada G, Gonçalves RM. Mesenchymal stromal cell secretome: influencing therapeutic potential by cellular pre-conditioning. Front Immunol 2018; 9: 2837
- 13 Nugraha AP, Susilowati H, Hendrianto E. et al; Purwati. Medicinal signaling cells metabolite oral based as a potential biocompatible biomaterial accelerating oral ulcer healing (in vitro study). Eur J Dent 2019; 13 (03) 432-436
- 14 Silva PGB, de Codes ÉBB, Freitas MO, Martins JOL, Alves APNN, Sousa FB. Experimental model of oral ulcer in mice: comparing wound healing in three immunologically distinct animal lines. J Oral Maxillofac Pathol 2018; 22 (03) 444
- 15 Gonzalez Ade O, Costa TF, Andrade Zde A, Medrado ARAP. Wound healing - A literature review. An Bras Dermatol. 2016; 91 (05) 614-620
- 16 Politis C, Schoenaers J, Jacobs R, Agbaje JO. Wound healing problems in the mouth. Front Physiol 2016; 7: 507
- 17 Shields AM, Panayi GS, Corrigall VM. Resolution-associated molecular patterns (RAMP): RAMParts defending immunological homeostasis?. Clin Exp Immunol 2011; 165 (03) 292-300
- 18 Holthaus M, Santhakumar N, Wahlers T, Paunel-Görgülü A. The secretome of preconditioned mesenchymal stem cells drives polarization and reprogramming of M2a macrophages toward an IL-10-producing phenotype. Int J Mol Sci 2022; 23 (08) 4104
- 19 Mitchell R, Mellows B, Sheard J. et al. Secretome of adipose-derived mesenchymal stem cells promotes skeletal muscle regeneration through synergistic action of extracellular vesicle cargo and soluble proteins. Stem Cell Res Ther 2019; 10 (01) 116
- 20 Zriek F, Di Battista JA, Alaaeddine N. Mesenchymal stromal cell secretome: immunomodulation, tissue repair and effects on neurodegenerative conditions. Curr Stem Cell Res Ther 2021; 16 (06) 656-669
- 21 Borges TJ, Wieten L, van Herwijnen MJC. et al. The anti-inflammatory mechanisms of Hsp70. Front Immunol 2012; 3: 95
- 22 Soliman AM, Das S, Abd Ghafar N, Teoh SL. Role of microRNA in proliferation phase of wound healing. Front Genet 2018; 9: 38
- 23 Jiang Y, Xu X, Xiao L, Wang L, Qiang S. The role of microRNA in the inflammatory response of wound healing. Front Immunol 2022; 13: 852419
- 24 Jiang CM, Liu J, Zhao JY. et al. Effects of hypoxia on the immunomodulatory properties of human gingiva-derived mesenchymal stem cells. J Dent Res 2015; 94 (01) 69-77
- 25 Demidova-Rice TN, Durham JT, Herman IM. Wound healing angiogenesis: innovations and challenges in acute and chronic wound healing. Adv Wound Care (New Rochelle) 2012; 1 (01) 17-22
- 26 Zimna A, Kurpisz M. Hypoxia-inducible factor-1 in physiological and pathophysiological angiogenesis: applications and therapies. BioMed Res Int 2015; 2015: 549412
- 27 Sunarto H, Trisnadi S, Putra A, Sa'dyah N, Tjipta A. The role of hypoxic mesenchymal stem cells conditioned medium in increasing vascular endothelial growth factors (VEGF) levels and collagen synthesis to accelerate wound healing. Indones J Cancer Chemoprevent 2020; 11 (03) 134-143
- 28 Farooq M, Khan AW, Kim MS, Choi S. The role of fibroblast growth factor (FGF) signaling in tissue repair and regeneration. Cells 2021; 10 (11) 3242
- 29 Makino T, Jinnin M, Muchemwa FC. et al. Basic fibroblast growth factor stimulates the proliferation of human dermal fibroblasts via the ERK1/2 and JNK pathways. Br J Dermatol 2010; 162 (04) 717-723
- 30 Viola A, Munari F, Sánchez-Rodríguez R, Scolaro T, Castegna A. The metabolic signature of macrophage responses. Front Immunol 2019; 10: 1462
- 31 Arundina I, Diyatri I, Kusumaningsih T, Surboyo MDC, Monica E, Afanda NM. The role of rice hull liquid smoke in the traumatic ulcer healing. Eur J Dent 2021; 15 (01) 33-38
- 32 Kim SY, Nair MG. Macrophages in wound healing: activation and plasticity. Immunol Cell Biol 2019; 97 (03) 258-267
Address for correspondence
Publication History
Article published online:
24 March 2023
© 2023. The Author(s). This is an open access article published by Thieme under the terms of the Creative Commons Attribution License, permitting unrestricted use, distribution, and reproduction so long as the original work is properly cited. (https://creativecommons.org/licenses/by/4.0/)
Thieme Medical and Scientific Publishers Pvt. Ltd.
A-12, 2nd Floor, Sector 2, Noida-201301 UP, India
-
References
- 1 Glick M. ed. Burket's Oral Medicine. 12th ed.. People's Medical Publishing House USA; 2015
- 2 Larjava H. ed. Oral Wound Healing: Cell Biology and Clinical Management. Wiley-Blackwell; 2012
- 3 Farah CS. Contemporary Oral Medicine: A Comprehensive Approach to Clinical Practice. Springer Berlin Heidelberg; 2019
- 4 Johnson KE, Wilgus TA. Vascular endothelial growth factor and angiogenesis in the regulation of cutaneous wound repair. Adv Wound Care (New Rochelle) 2014; 3 (10) 647-661
- 5 Landén NX, Li D, Ståhle M. Transition from inflammation to proliferation: a critical step during wound healing. Cell Mol Life Sci 2016; 73 (20) 3861-3885
- 6 Bosanquet DC, Rangaraj A, Richards AJ, Riddell A, Saravolac VM, Harding KG. Topical steroids for chronic wounds displaying abnormal inflammation. Ann R Coll Surg Engl 2013; 95 (04) 291-296 . Doi: 10.1308/003588413 × 13629960045634
- 7 Karavana Hizarcioğlu SY, Sezer B, Güneri P. et al. Efficacy of topical benzydamine hydrochloride gel on oral mucosal ulcers: an in vivo animal study. Int J Oral Maxillofac Surg 2011; 40 (09) 973-978
- 8 Bunnell BA. Adipose tissue-derived mesenchymal stem cells. Cells 2021; 10 (12) 3433
- 9 Ahangar P, Mills SJ, Cowin AJ. Mesenchymal stem cell secretome as an emerging cell-free alternative for improving wound repair. Int J Mol Sci 2020; 21 (19) 7038
- 10 Park SR, Kim JW, Jun HS, Roh JY, Lee HY, Hong IS. Stem cell secretome and its effect on cellular mechanisms relevant to wound healing. Mol Ther 2018; 26 (02) 606-617
- 11 Ajit A, Ambika GopalankuttyI. Adipose-derived stem cell secretome as a cell-free product for cutaneous wound healing. Biotech 2021; 11 (09) 413
- 12 Ferreira JR, Teixeira GQ, Santos SG, Barbosa MA, Almeida-Porada G, Gonçalves RM. Mesenchymal stromal cell secretome: influencing therapeutic potential by cellular pre-conditioning. Front Immunol 2018; 9: 2837
- 13 Nugraha AP, Susilowati H, Hendrianto E. et al; Purwati. Medicinal signaling cells metabolite oral based as a potential biocompatible biomaterial accelerating oral ulcer healing (in vitro study). Eur J Dent 2019; 13 (03) 432-436
- 14 Silva PGB, de Codes ÉBB, Freitas MO, Martins JOL, Alves APNN, Sousa FB. Experimental model of oral ulcer in mice: comparing wound healing in three immunologically distinct animal lines. J Oral Maxillofac Pathol 2018; 22 (03) 444
- 15 Gonzalez Ade O, Costa TF, Andrade Zde A, Medrado ARAP. Wound healing - A literature review. An Bras Dermatol. 2016; 91 (05) 614-620
- 16 Politis C, Schoenaers J, Jacobs R, Agbaje JO. Wound healing problems in the mouth. Front Physiol 2016; 7: 507
- 17 Shields AM, Panayi GS, Corrigall VM. Resolution-associated molecular patterns (RAMP): RAMParts defending immunological homeostasis?. Clin Exp Immunol 2011; 165 (03) 292-300
- 18 Holthaus M, Santhakumar N, Wahlers T, Paunel-Görgülü A. The secretome of preconditioned mesenchymal stem cells drives polarization and reprogramming of M2a macrophages toward an IL-10-producing phenotype. Int J Mol Sci 2022; 23 (08) 4104
- 19 Mitchell R, Mellows B, Sheard J. et al. Secretome of adipose-derived mesenchymal stem cells promotes skeletal muscle regeneration through synergistic action of extracellular vesicle cargo and soluble proteins. Stem Cell Res Ther 2019; 10 (01) 116
- 20 Zriek F, Di Battista JA, Alaaeddine N. Mesenchymal stromal cell secretome: immunomodulation, tissue repair and effects on neurodegenerative conditions. Curr Stem Cell Res Ther 2021; 16 (06) 656-669
- 21 Borges TJ, Wieten L, van Herwijnen MJC. et al. The anti-inflammatory mechanisms of Hsp70. Front Immunol 2012; 3: 95
- 22 Soliman AM, Das S, Abd Ghafar N, Teoh SL. Role of microRNA in proliferation phase of wound healing. Front Genet 2018; 9: 38
- 23 Jiang Y, Xu X, Xiao L, Wang L, Qiang S. The role of microRNA in the inflammatory response of wound healing. Front Immunol 2022; 13: 852419
- 24 Jiang CM, Liu J, Zhao JY. et al. Effects of hypoxia on the immunomodulatory properties of human gingiva-derived mesenchymal stem cells. J Dent Res 2015; 94 (01) 69-77
- 25 Demidova-Rice TN, Durham JT, Herman IM. Wound healing angiogenesis: innovations and challenges in acute and chronic wound healing. Adv Wound Care (New Rochelle) 2012; 1 (01) 17-22
- 26 Zimna A, Kurpisz M. Hypoxia-inducible factor-1 in physiological and pathophysiological angiogenesis: applications and therapies. BioMed Res Int 2015; 2015: 549412
- 27 Sunarto H, Trisnadi S, Putra A, Sa'dyah N, Tjipta A. The role of hypoxic mesenchymal stem cells conditioned medium in increasing vascular endothelial growth factors (VEGF) levels and collagen synthesis to accelerate wound healing. Indones J Cancer Chemoprevent 2020; 11 (03) 134-143
- 28 Farooq M, Khan AW, Kim MS, Choi S. The role of fibroblast growth factor (FGF) signaling in tissue repair and regeneration. Cells 2021; 10 (11) 3242
- 29 Makino T, Jinnin M, Muchemwa FC. et al. Basic fibroblast growth factor stimulates the proliferation of human dermal fibroblasts via the ERK1/2 and JNK pathways. Br J Dermatol 2010; 162 (04) 717-723
- 30 Viola A, Munari F, Sánchez-Rodríguez R, Scolaro T, Castegna A. The metabolic signature of macrophage responses. Front Immunol 2019; 10: 1462
- 31 Arundina I, Diyatri I, Kusumaningsih T, Surboyo MDC, Monica E, Afanda NM. The role of rice hull liquid smoke in the traumatic ulcer healing. Eur J Dent 2021; 15 (01) 33-38
- 32 Kim SY, Nair MG. Macrophages in wound healing: activation and plasticity. Immunol Cell Biol 2019; 97 (03) 258-267