

Subscribe to RSS
DOI: 10.1055/s-0043-1761928
In-vitro Activity of Isepamicin against Gram-negative Bacteria in Comparison to Other Aminoglycosides Routinely used at a Teaching Hospital in Northern India
Authors
Funding None.

Abstract
Background Isepamicin is a 1-N-S-a-hydroxy-b-aminopropionyl derivative of gentamicin B and the spectrum of pathogenic microorganisms covered by it and its effectiveness is similar to that of amikacin except the action of aminoglycoside inhibitor enzymes is ineffectual on it.
Material and Methods We performed a prospective study in the Bacteriology section of the Department of Microbiology at a 1,600-bedded hospital in Northern India from Jan 2022 to March 2022. Isepamicin was tested for susceptibility against gram-negative bacteria, identified by routine biochemicals and matrix-assisted-desorption/ionization –time of flight-mass spectrometry (MALDI-TOF-MS) assay. The antibiotic susceptibility testing for each of the isolates was performed by Kirby Bauer's disc diffusion method, according to the CLSI 2019 guidelines.
Results The majority of isolates were obtained from blood samples (50, 39.1%). Among the non-inducible Enterobacteriaceae, Escherichia coli was least susceptible to amikacin (8/27, 29.63%) and most susceptible to isepamicin (18/27, 66.67%). Klebsiella pneumoniae followed the same pattern of susceptibility as E. coli and was least susceptible to Amikacin (20/46, 43.48%) and most susceptible to isepamicin (24/46, 52.17%). Enterobacter cloacae (6/7, 85.71%) was most susceptible to both amikacin and isepamicin, followed by 71.43% (5/7, 71.43%) susceptibility to gentamicin and tobramycin each. Enterobacter aerogenes was equally 53.33% (8/15) susceptible to all antibiotics. Pseudomonas aeruginosa was the most susceptible isolate to all antibiotics (18/21, 85.71%).
Conclusion Isepamicin is a potential antimicrobial agent for treating an array of gram-negative bacteria-associated infections and shows better in vitro activity than older aminoglycoside agents.
Introduction
Aminoglycosides serves as the fundamental drug for treating a spectrum of life-threatening ailments caused by gram-negative bacteria. Its rampant and imprudent use in hospitals has encouraged the emergence of resistance to these antibiotics among the isolates obtained from clinical samples.[1] The emergence of this resistance is attributed to the acquisition of plasmids that program the microorganisms to secrete aminoglycoside inactivating enzymes.[2]
Earlier the most widely used aminoglycosides used were gentamicin, netilmicin, and tobramycin. Amikacin was discovered to thwart the microorganisms that developed resistance to the above-mentioned drugs. Although amikacin has had a successful outcome in combating most multidrug-resistant infections over time resistance of 30% to 40% was observed among the isolates due to the emergence of amikacin resistant microorganisms producing a specific 6-N' aminoglycoside transferase [AAC(6')- I].[3] [4] [5] [6]
Isepamicin is a 1-N-S-a-hydroxy-b-aminopropionyl derivative of gentamicin B.[7] The spectrum of pathogenic microorganisms covered by it and its effectiveness is similar to that of Amikacin except the action of aminoglycoside inhibitor enzymes is ineffectual on it.[8] [9] [10] [11] [12] It has been made available in countries such as Belgium, China, Italy, Japan, and South Korea.[13] It is also manufactured in India but not used commonly at our center due to a lack of data on better in vitro activity in comparison to other aminoglycosides, especially amikacin.
Gram-negative bacteria have been the flag-bearers of emerging multidrug resistance. It is the need of the hour to produce newer antimicrobial agents to combat this drug resistance. It is due to this reason that the old and forgotten antibiotics such as fosfomycin and colistin that have not been used for a considerable amount of time are being brought into use again. Similarly, isepamicin could be one of those forgotten agents that can be effective against gram-negative bacteria.[14] [15]
Our study aimed to demonstrate and compare the in vitro activity of isepamicin to other aminoglycosides used against the gram-negative bacteria obtained from the clinical samples included in the study.
Materials and Methods
Study Design
A prospective observational study was conducted in the Bacteriology section of the Department of Microbiology at university hospital in Northern India from January 2022 to March 2022. We intended to demonstrate the in vitro activity of isepamicin against the gram-negative bacteria isolated from the clinical samples included in this study over 3 months and to compare its activity to three other aminoglycoside antibiotics which include amikacin, gentamicin, and tobramycin that are regularly used in the wards and critical care units of our hospital. We did not test its activity against all non-lactose fermenting bacteria except Pseudomonas aeruginosa as there are no cut-off guidelines.
The identification of each isolate was done using conventional biochemical tests and/or matrix-assisted laser desorption/ionization–time of flight-mass spectrometry (MALDI-TOF-MS) assay. The sample from which the isolate was obtained and the outcome of the patient was included and recorded. We did not make any endeavor to identify the pathogenic or colonizing nature of the microorganism, nor was the ability of the infection to influence the outcome of the patients.
Selection of the Isolates
We included non-repeat samples in the study so that no similar gram-negative isolate was included in the study twice. Samples that were inappropriate or delayed in transport were excluded. All gram-positive isolates along with bacterial isolates belonging to Neisseria, Haemophilus, and Moraxella species were discarded. Bacterial isolates against which isepamicin was tested mainly include gram-negative bacteria isolates from the blood samples and respiratory samples which include sputum, tracheal aspirates, and endotracheal aspirates. Samples from only patients admitted to our hospital were included in the study and samples from the outpatient department (OPD) were excluded.
Antimicrobial Susceptibility Testing
The antibiotic susceptibility for each of the bacterial isolates was conducted by using Kirby Bauer disc diffusion method, according to the CLSI 2019 guidelines.[16] Antibiotic discs containing amikacin (30 µg), gentamicin (10 µg), tobramycin (10 µg), and isepamicin (30 µg) were obtained from HiMedia diagnostics (Mumbai, India). Standard inocula for each bacterial isolate were prepared and set to 0.5 McFarland and a lawn culture was applied on cation-adjusted Muller–Hinton agar plates. The above-mentioned antibiotic discs were manually placed on the lawn cultured plates and incubated overnight at 37°C. The measurement of zones of inhibition for each antibiotic against each isolate was measured and classified as sensitive, intermediate, and resistant according to the tables and guidelines by CLSI 2019.[16] The zone diameter interpretation for amikacin was applied to that of isepamicin: ≥ 17 mm zone diameter is susceptible; 15–16 mm diameter is intermediate; and a zone diameter ≤ 14 mm is resistant. Escherichia coli American Type Culture Collection (ATCC; Rockville, MD, USA) 25922 and Pseudomonas aeruginosa ATCC27853 were used for daily quality control testing recommended by the CLSI.
Results
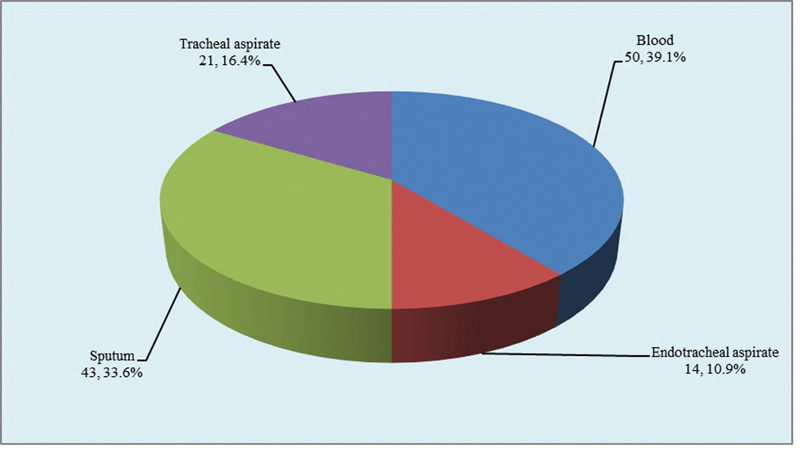
A total of 128 non-repeat gram-negative isolates were obtained from the clinical samples obtained from adult patients admitted to the inpatient department of our hospital. [Figure 1] shows the distribution of samples from which the isolated microorganisms were tested for susceptibility to isepamicin. The majority of isolates were obtained from blood samples (50, 39.1%), followed by sputum samples (43, 33.6%). The other samples included in our study were tracheal aspirates (21, 16.4%) and endotracheal aspirates (14, 10.9%).
Overall, the most frequent microorganism tested for susceptibility to this drug was K. pneumoniae (46, 35.9%), followed by E. coli (27, 21.1%) and P. aeruginosa (21, 16.4%) as seen in [Table 1]. As far as the groups of microorganisms go, the antibiotic was more predominantly tested for its susceptibility against the non-inducible Enterobacteriaceae group (which includes E. coli and K. pneumoniae) in comparison to the inducible Enterobacteriaceae group (which includes Enterobacter aerogenes, Enterobacter cloacae, and Serratia marcescens), which is 57.03% (n = 73) versus 17.96% (n = 23) respectively. Isepamicin was also tested for susceptibility against non- fermenters groups in 25.0% (n = 32) isolates identified in our study. Being a single-center study, no comparison in the prevalence of the isolates being tested could be made among other centers and this limits our study from representing the susceptibility to isepamicin among the isolates identified from the whole region of Northern India.
[Table 2] represents the susceptibility of the isolates included in the study to amikacin, gentamicin, tobramycin, and isepamicin. Pseudomonas aeruginosa was the most susceptible isolate to all the antibiotics and was 85.71% (18/21, 85.71%) susceptible to all four antibiotics. Klebsiella pneumoniae and Enterobacter aerogenes were most resistant to all four antibiotics. Klebsiella pneumoniae was most resistant to amikacin (26, 56.52%) followed by gentamicin (24, 52.17%) and tobramycin (23, 50.0%), and was marginally more susceptible to isepamicin (24, 52.17%). Enterobacter aerogenes was equally resistant to all four antibiotics by 46.67% (7/15). The overall susceptibility to all antibiotics in descending order was isepamicin (81/128, 63.28%), tobramycin (76/128, 59.38%), gentamicin (75/128, 58.59%), and amikacin (66/128, 51.56%). Pseudomonas aeruginosa was the most susceptible isolate to all the antibiotics (18/21, 85.71%).
Among the non-inducible Enterobacteriaceae, E. coli was the least susceptible to amikacin (8/27, 29.63%) and most susceptible to isepamicin (18/27, 66.67%). Klebsiella pneumoniae followed the same pattern of susceptibility as E. coli and was least susceptible to amikacin (20/46, 43.48%) and most susceptible to isepamicin (24/46, 52.17%).
Among the inducible Enterobacteriaceae, E. cloacae was the most susceptible to all four antibiotics. Enterobacter cloacae (6/7, 85.71%) was most susceptible to both amikacin and isepamicin, followed by 71.43% (5/7, 71.43%) susceptibility to gentamicin and tobramycin each. Enterobacter aerogenes was equally 53.33% (8/15) susceptible to all antibiotics, which records the equivocal rate of resistance of the isolates to all the aminoglycosides included in the study.
On overall analysis, the activity of amikacin and isepamicin was almost comparable among the inducible Enterobacteriaceae and non-fermenter isolates included in our study. But the activity of isepamicin was better in comparison to amikacin in the case of non-inducible Enterobacteriaceae which includes E. coli and K. pneumoniae. Further comparative activity of isepamicin and amikacin against the three most common isolates against which sensitivity of the above-mentioned aminoglycoside was tested has been discussed in [Table 3].
The three most common microorganisms isolated from the samples included in our study were K. pneumoniae (n = 46), E. coli (n = 27), and P. aeruginosa (n = 21). The isolates were sensitive to both amikacin and isepamicin in 43.48% (20/46) K. pneumoniae, 33.33% (9/27) E. coli and 85.71% (18/21) P. aeruginosa. The isolates were resistant to both amikacin and isepamicin in 47.83% (22/46) K. pneumoniae, 33.33% (9/27) E. coli and 14.28% (3/21) P. aeruginosa. The isolates were sensitive to isepamicin and resistant to amikacin in 8.69% (4/46) K. pneumoniae, 33.33% (9/27) E. coli, and 0% (0/21) P. aeruginosa isolates. None of the above-mentioned microorganisms were resistant to isepamicin and sensitive to amikacin.
Among the 128 isolates, 54.68% (70/128) isolates were found to be multidrug resistant organisms (MDROs). Among these isolates, K. pneumoniae was found to be 69.57% (32/46), E. coli was found to be 66.67% (18/27), and P. aeruginosa was found to be 61.90% (13/21) resistant to one drug in three or more categories of antimicrobials. While isolates were found most resistant to fluoroquinolones (∼90%), followed by third-generation cephalosporins (∼80%), K. pneumoniae was found to be 96.88% (31/32), E. coli was found to be 100% (18/18), and P. aeruginosa was found to be 92.31% (12/13) sensitive to the drug of last resort, colistin. While we report one isolate each of K. pneumoniae and P. aeruginosa to be extremely drug resistant.
Isepamicin had better activity in comparison to other aminoglycosides against the isolates from the samples included in our study. Whereas the isolates were least susceptible to amikacin and the susceptibility to tobramycin and gentamicin was almost similar to each other while was low in comparison to isepamicin.
Discussion
The most common pathogens accountable for increased morbidity and mortality in hospitalized patients are gram-negative bacteria.[17] Administration of appropriate antibiotic treatment early in case of gram-negative bacterial infection can avoid the chances of complications leading to increased morbidity and mortality.[18] The identification of bacterial isolates and their antibiotic susceptibility can help decide the appropriate treatment and the best antibiotic agents for the particular isolate.[19] Newer antibiotic agents are the need of the hour to combat the alarming increase in multidrug resistance among infection-causing gram-negative bacteria. A new agent among aminoglycosides is isepamicin, but it is not routinely used in India. Therefore, our study aimed to demonstrate the susceptibility of isepamicin against gram-negative isolates from clinical samples included in this study.
Aminoglycosides are either used alone or in combination with other drugs to treat many serious gram-negative bacterial infections.[20] The aminoglycosides exert their function by uptake of the antibiotic by an energy-dependent mechanism that binds to the 30S ribosomal subunit and blocks the protein synthesis leading to cell death by loss of cell membrane function.[21] The chemical formula of isepamicin is 1-N-S-α-hydroxy-β-aminoproprionyl. It is derived from gentamicin B and acts as an active agent against many bacteria including non-inducible and inducible Enterobacteriaceae microorganisms and non-fermenters not susceptible to other aminoglycoside agents.[22] [23] [24]
Among the isolates recovered in our study K. pneumoniae, E. coli, and P. aeruginosa were identified as the most common microorganisms against which isepamicin was tested for its susceptibility along with other aminoglycosides used routinely in our clinical setting. A similar predominance of E. coli and P. aeruginosa was observed in studies conducted by Verbist et al,[25] Glupczynski et al,[26] Vincent et al,[27] Spencer et al,[28] Jarlier et al,[29] and Belgian Isepamicin Multicenter Study Group.[1]
As observed in [Table 2], almost all four aminoglycoside drugs were active against the gram-negative bacilli. The resistance rate ranged from 36.72% to 48.44% among all aminoglycosides tested against the isolates, which is fairly higher in comparison to a study conducted by the Belgian Isepamicin Multicenter Study Group[1] where the resistance range averaged around 10% among all the isolates. In a study by Tsai et al,[19] susceptibility of 247 gram-negative bacilli was tested to isepamicin and found to be 95%, which is in contrast to the susceptibility of 63.3% of isolates in our study. The reason for this difference in susceptibility can be attributed to the fact that patients received inappropriate or incomplete treatment from various government and private medical centers before getting referred to our hospital which promotes the inheritance of multidrug resistance.
A study conducted by the Belgian Isepamicin Multicenter Study Group also suggested that isepamicin was rendered most sensitive to all gram-negative bacteria isolated from clinical samples obtained from intensive care unit (ICU) patients,[1] which corroborates with the isolates from our study. Another study conducted in Turkey by Küçükates et al tested the susceptibility of isepamicin to be compared with carbapenems and found it to be more effective against the Enterobacteriaceae group of gram-negative bacteria, which correlates with the findings in our study.[30]
As isepamicin is less affected by aminoglycosides modifying enzymes, this could be the reason for its good in vitro activity against the bacterial isolates. Older studies suggest that the aac (6)-I subfamily of enzymes were inactive against isepamicin.[2] [11] This study suggests that although isepamicin was not used in gram-negative bacterial infections at our hospital; nevertheless, 36.72% resistance was observed in the isolates in agreement to a study where soon after initiation of isepamicin against gram-negative bacteria, emerging antimicrobial resistance was encountered.[2] The presence to a combination of more than one aminoglycoside-modifying enzymes or efflux mechanisms or decreased influx of the antibiotic molecules associated with such an enzyme in the gram negative bacteria, rendering it resistant to the actions of tsepamicin.[11]
The total death of 62 (62/128, 48.44%) patients was recorded in our study. Out of 62 patients, isolates from clinical samples of 38 (38/62, 61.29%) patients were sensitive to isepamicin except as it is not commonly used in the wards, its in vivo activity could not be interpreted. Thus, the use of aminoglycoside such as isepamicin holds a chance to improve the outcome of the patients admitted to the ward or intensive care unit.
Conclusion
Our study defines a good in vitro activity of isepamicin against non-inducible, inducible, and non-fermenters in comparison to other aminoglycosides used routinely in the wards and intensive care units. It is a potential antimicrobial agent for treating an array of gram-negative bacteria-associated infections and it improves the outcome of patients suffering mainly from bacteremia and respiratory tract infections in comparison to other aminoglycoside agents.
Conflict of Interest
None declared.
Acknowledgment
The author thanks the contribution of all other laboratory staff for providing technical and logistic support.
Authors' Contributions
Protocol development: T.S., A.D., C.S.
Data collection: A.D., T.S. Data analysis: C.S., S.S.P. Supervision: C.S., S.S.P.
Writing - original draft: M.K., A.D. Writing – review & editing: M.K., A.D., T.S., C.S., S.S.P.
All authors read and approved the final version of the manuscript.
Consent for Publication
All individuals have given consent to participate in the study.
Ethical Statement
The study protocol was approved by the institutional Ethics Committee of Sanjay Gandhi Postgraduate Institute of Medical Sciences (Reference number 2020–100-EMP-EXP-16)
-
References
- 1 Belgian Isepamicin Multicenter Study Group. Comparative in vitro activity of isepamicin and other antibiotics against gram-negative bacilli from intensive care units (ICU) in Belgium. Acta Clin Belg 2001; 56 (05) 307-315
- 2 Mingeot-Leclercq MP, Glupczynski Y, Tulkens PM. Aminoglycosides: activity and resistance. Antimicrob Agents Chemother 1999; 43 (04) 727-737
- 3 Miller GH, Sabatelli FJ, Naples L, Hare RS, Shaw KJ. The Aminoglycoside Resistance Study Groups. The most frequently occurring aminoglycoside resistance mechanisms–combined results of surveys in eight regions of the world. J Chemother 1995; 7 (Suppl. 02) 17-30
- 4 Miller GH, Sabatelli FJ, Naples L, Hare RS, Shaw KJ. The Aminoglycoside Resistance Study Groups. The changing nature of aminoglycoside resistance mechanisms and the role of isepamicin–a new broad-spectrum aminoglycoside. J Chemother 1995; 7 (Suppl. 02) 31-44
- 5 Miller GH, Sabatelli FJ, Hare RS. et al. The most frequent aminoglycoside resistance mechanisms–changes with time and geographic area: a reflection of aminoglycoside usage patterns? Aminoglycoside Resistance Study Groups. Clin Infect Dis 1997; 24 (Suppl. 01) S46-S62
- 6 Vanhoof R, Nyssen HJ, Van Bossuyt E, Hannecart-Pokorni E. Aminoglycoside Resistance Study Group. Aminoglycoside resistance in gram-negative blood isolates from various hospitals in Belgium and the Grand Duchy of Luxembourg. J Antimicrob Chemother 1999; 44 (04) 483-488
- 7 Goering RV, Sanders CC, Sanders WE. In vivo analysis of structure-activity relationships among four aminoglycosides: gentamicin, netilmicin, 1-N HAPA gentamicin B, and amikacin. Curr Ther Res Clin Exp 1979; 26: 329-341
- 8 Nagabhushan TL, Cooper AB, Tsai H, Daniels PJ, Miller GH. The syntheses and biological properties of 1-N-(S-4-amino-2-hydroxybutyryl)-gentamicin B and 1-N-(S-3-amino-2-hydroxypropionyl)-gentamicin B. J Antibiot (Tokyo) 1978; 31 (07) 681-687
- 9 Oshitani H, Kawai S, Kobayashi H. Experimental and clinical studies of HAPA-B. Chemother 1985; 33: 201-205
- 10 Takumida M, Nishida I, Nikaido M, Hirakawa K, Harada Y, Bagger-Sjöbäck D. Effect of dosing schedule on aminoglycoside ototoxicity: comparative cochlear ototoxicity of amikacin and isepamicin. ORL J Otorhinolaryngol Relat Spec 1990; 52 (06) 341-349
- 11 Over U, Gür D, Unal S, Miller GH. Aminoglycoside Resistance Study Group. The changing nature of aminoglycoside resistance mechanisms and prevalence of newly recognized resistance mechanisms in Turkey. Clin Microbiol Infect 2001; 7 (09) 470-478
- 12 Cheng NC, Hsueh PR, Liu YC. et al. In vitro activities of tigecycline, ertapenem, isepamicin, and other antimicrobial agents against clinically isolated organisms in Taiwan. Microb Drug Resist 2005; 11 (04) 330-341
- 13 Maraki S, Samonis G, Karageorgopoulos DE, Mavros MN, Kofteridis D, Falagas ME. In vitro antimicrobial susceptibility to isepamicin of 6,296 Enterobacteriaceae clinical isolates collected at a tertiary care university hospital in Greece. Antimicrob Agents Chemother 2012; 56 (06) 3067-3073
- 14 Falagas ME, Kasiakou SK. Colistin: the revival of polymyxins for the management of multidrug-resistant gram-negative bacterial infections. Clin Infect Dis 2005; 40 (09) 1333-1341
- 15 Falagas ME, Kastoris AC, Kapaskelis AM, Karageorgopoulos DE. Fosfomycin for the treatment of multidrug-resistant, including extended-spectrum beta-lactamase producing, Enterobacteriaceae infections: a systematic review. Lancet Infect Dis 2010; 10 (01) 43-50
- 16 Wayne PA. Clinical and Laboratory Standards Institute. Performance standards for antimicrobial susceptibility testing: Twenty-third informational supplement. Clinical and Laboratory Standards Institute. CLSI document M100–S29; USA; 2019
- 17 Martin MA. Epidemiology and clinical impact of gram-negative sepsis. Infect Dis Clin North Am 1991; 5 (04) 739-752
- 18 Bryan CS, Reynolds KL, Brenner ER. Analysis of 1,186 episodes of gram-negative bacteremia in non-university hospitals: the effects of antimicrobial therapy. Rev Infect Dis 1983; 5 (04) 629-638
- 19 Tsai TY, Chang SC, Hsueh PR, Feng NH, Wang JT. In vitro activity of isepamicin and other aminoglycosides against clinical isolates of Gram-negative bacteria causing nosocomial bloodstream infections. J Microbiol Immunol Infect 2007; 40 (06) 481-486
- 20 Craig WA. Once-daily versus multiple-daily dosing of aminoglycosides. J Chemother 1995; 7 (Suppl. 02) 47-52
- 21 Siu LK. Antibiotics: action and resistance in gram-negative bacteria. J Microbiol Immunol Infect 2002; 35 (01) 1-11
- 22 Fauvelle F, Coulaud JM, Lecointre K, Tardy D, Poussel JF, Trape G. Comparison of two methods to obtain a desired first isepamicin peak in intensive care patients. Fundam Clin Pharmacol 2001; 15 (02) 151-156
- 23 Jones RN. Isepamicin (SCH 21420, 1-N-HAPA gentamicin B): microbiological characteristics including antimicrobial potency of spectrum of activity. J Chemother 1995; 7 (Suppl. 02) 7-16
- 24 Miller GH, Chiu PJ, Waitz JA. Biological activity of SCH 21420, the 1-N-S-alpha-hydroxy-beta-aminopropionyl derivative of gentamicin B. J Antibiot (Tokyo) 1978; 31 (07) 688-696
- 25 Verbist L. Incidence of multi-resistance in gram-negative bacterial isolates from intensive care units in Belgium: a surveillance study. Scand J Infect Dis Suppl 1991; 78 (Suppl. 78) 45-53
- 26 Glupczynski Y, Delmée M, Goossens H, Struelens M. on behalf of a Belgian Multicenter study group. A multicenter survey of antimicrobial resistance in gram-negative isolates from Belgian intensive care units in 1994–1995. Acta Clin Belg 1998; 53 (01) 35-45
- 27 Vincent JL, Bihari DJ, Suter PM. et al; EPIC International Advisory Committee. The prevalence of nosocomial infection in intensive care units in Europe. Results of the European Prevalence of Infection in Intensive Care (EPIC) Study. JAMA 1995; 274 (08) 639-644
- 28 Spencer RC. Predominant pathogens found in the European Prevalence of Infection in Intensive Care Study. Eur J Clin Microbiol Infect Dis 1996; 15 (04) 281-285
- 29 Jarlier V, Fosse T, Philippon A. Antibiotic susceptibility in aerobic gram-negative bacilli isolated in intensive care units in 39 French teaching hospitals (ICU study). Intensive Care Med 1996; 22 (10) 1057-1065
- 30 Küçükates¸ E, Kansız E, Gültekin N. Resistance to isepamicin, amikacin and gentamicin in gram-negative bacteria. Infeks Derg 2007; 21: 21-25
Address for correspondence
Publication History
Article published online:
22 March 2023
© 2023. The Indian Association of Laboratory Physicians. This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/)
Thieme Medical and Scientific Publishers Pvt. Ltd.
A-12, 2nd Floor, Sector 2, Noida-201301 UP, India
-
References
- 1 Belgian Isepamicin Multicenter Study Group. Comparative in vitro activity of isepamicin and other antibiotics against gram-negative bacilli from intensive care units (ICU) in Belgium. Acta Clin Belg 2001; 56 (05) 307-315
- 2 Mingeot-Leclercq MP, Glupczynski Y, Tulkens PM. Aminoglycosides: activity and resistance. Antimicrob Agents Chemother 1999; 43 (04) 727-737
- 3 Miller GH, Sabatelli FJ, Naples L, Hare RS, Shaw KJ. The Aminoglycoside Resistance Study Groups. The most frequently occurring aminoglycoside resistance mechanisms–combined results of surveys in eight regions of the world. J Chemother 1995; 7 (Suppl. 02) 17-30
- 4 Miller GH, Sabatelli FJ, Naples L, Hare RS, Shaw KJ. The Aminoglycoside Resistance Study Groups. The changing nature of aminoglycoside resistance mechanisms and the role of isepamicin–a new broad-spectrum aminoglycoside. J Chemother 1995; 7 (Suppl. 02) 31-44
- 5 Miller GH, Sabatelli FJ, Hare RS. et al. The most frequent aminoglycoside resistance mechanisms–changes with time and geographic area: a reflection of aminoglycoside usage patterns? Aminoglycoside Resistance Study Groups. Clin Infect Dis 1997; 24 (Suppl. 01) S46-S62
- 6 Vanhoof R, Nyssen HJ, Van Bossuyt E, Hannecart-Pokorni E. Aminoglycoside Resistance Study Group. Aminoglycoside resistance in gram-negative blood isolates from various hospitals in Belgium and the Grand Duchy of Luxembourg. J Antimicrob Chemother 1999; 44 (04) 483-488
- 7 Goering RV, Sanders CC, Sanders WE. In vivo analysis of structure-activity relationships among four aminoglycosides: gentamicin, netilmicin, 1-N HAPA gentamicin B, and amikacin. Curr Ther Res Clin Exp 1979; 26: 329-341
- 8 Nagabhushan TL, Cooper AB, Tsai H, Daniels PJ, Miller GH. The syntheses and biological properties of 1-N-(S-4-amino-2-hydroxybutyryl)-gentamicin B and 1-N-(S-3-amino-2-hydroxypropionyl)-gentamicin B. J Antibiot (Tokyo) 1978; 31 (07) 681-687
- 9 Oshitani H, Kawai S, Kobayashi H. Experimental and clinical studies of HAPA-B. Chemother 1985; 33: 201-205
- 10 Takumida M, Nishida I, Nikaido M, Hirakawa K, Harada Y, Bagger-Sjöbäck D. Effect of dosing schedule on aminoglycoside ototoxicity: comparative cochlear ototoxicity of amikacin and isepamicin. ORL J Otorhinolaryngol Relat Spec 1990; 52 (06) 341-349
- 11 Over U, Gür D, Unal S, Miller GH. Aminoglycoside Resistance Study Group. The changing nature of aminoglycoside resistance mechanisms and prevalence of newly recognized resistance mechanisms in Turkey. Clin Microbiol Infect 2001; 7 (09) 470-478
- 12 Cheng NC, Hsueh PR, Liu YC. et al. In vitro activities of tigecycline, ertapenem, isepamicin, and other antimicrobial agents against clinically isolated organisms in Taiwan. Microb Drug Resist 2005; 11 (04) 330-341
- 13 Maraki S, Samonis G, Karageorgopoulos DE, Mavros MN, Kofteridis D, Falagas ME. In vitro antimicrobial susceptibility to isepamicin of 6,296 Enterobacteriaceae clinical isolates collected at a tertiary care university hospital in Greece. Antimicrob Agents Chemother 2012; 56 (06) 3067-3073
- 14 Falagas ME, Kasiakou SK. Colistin: the revival of polymyxins for the management of multidrug-resistant gram-negative bacterial infections. Clin Infect Dis 2005; 40 (09) 1333-1341
- 15 Falagas ME, Kastoris AC, Kapaskelis AM, Karageorgopoulos DE. Fosfomycin for the treatment of multidrug-resistant, including extended-spectrum beta-lactamase producing, Enterobacteriaceae infections: a systematic review. Lancet Infect Dis 2010; 10 (01) 43-50
- 16 Wayne PA. Clinical and Laboratory Standards Institute. Performance standards for antimicrobial susceptibility testing: Twenty-third informational supplement. Clinical and Laboratory Standards Institute. CLSI document M100–S29; USA; 2019
- 17 Martin MA. Epidemiology and clinical impact of gram-negative sepsis. Infect Dis Clin North Am 1991; 5 (04) 739-752
- 18 Bryan CS, Reynolds KL, Brenner ER. Analysis of 1,186 episodes of gram-negative bacteremia in non-university hospitals: the effects of antimicrobial therapy. Rev Infect Dis 1983; 5 (04) 629-638
- 19 Tsai TY, Chang SC, Hsueh PR, Feng NH, Wang JT. In vitro activity of isepamicin and other aminoglycosides against clinical isolates of Gram-negative bacteria causing nosocomial bloodstream infections. J Microbiol Immunol Infect 2007; 40 (06) 481-486
- 20 Craig WA. Once-daily versus multiple-daily dosing of aminoglycosides. J Chemother 1995; 7 (Suppl. 02) 47-52
- 21 Siu LK. Antibiotics: action and resistance in gram-negative bacteria. J Microbiol Immunol Infect 2002; 35 (01) 1-11
- 22 Fauvelle F, Coulaud JM, Lecointre K, Tardy D, Poussel JF, Trape G. Comparison of two methods to obtain a desired first isepamicin peak in intensive care patients. Fundam Clin Pharmacol 2001; 15 (02) 151-156
- 23 Jones RN. Isepamicin (SCH 21420, 1-N-HAPA gentamicin B): microbiological characteristics including antimicrobial potency of spectrum of activity. J Chemother 1995; 7 (Suppl. 02) 7-16
- 24 Miller GH, Chiu PJ, Waitz JA. Biological activity of SCH 21420, the 1-N-S-alpha-hydroxy-beta-aminopropionyl derivative of gentamicin B. J Antibiot (Tokyo) 1978; 31 (07) 688-696
- 25 Verbist L. Incidence of multi-resistance in gram-negative bacterial isolates from intensive care units in Belgium: a surveillance study. Scand J Infect Dis Suppl 1991; 78 (Suppl. 78) 45-53
- 26 Glupczynski Y, Delmée M, Goossens H, Struelens M. on behalf of a Belgian Multicenter study group. A multicenter survey of antimicrobial resistance in gram-negative isolates from Belgian intensive care units in 1994–1995. Acta Clin Belg 1998; 53 (01) 35-45
- 27 Vincent JL, Bihari DJ, Suter PM. et al; EPIC International Advisory Committee. The prevalence of nosocomial infection in intensive care units in Europe. Results of the European Prevalence of Infection in Intensive Care (EPIC) Study. JAMA 1995; 274 (08) 639-644
- 28 Spencer RC. Predominant pathogens found in the European Prevalence of Infection in Intensive Care Study. Eur J Clin Microbiol Infect Dis 1996; 15 (04) 281-285
- 29 Jarlier V, Fosse T, Philippon A. Antibiotic susceptibility in aerobic gram-negative bacilli isolated in intensive care units in 39 French teaching hospitals (ICU study). Intensive Care Med 1996; 22 (10) 1057-1065
- 30 Küçükates¸ E, Kansız E, Gültekin N. Resistance to isepamicin, amikacin and gentamicin in gram-negative bacteria. Infeks Derg 2007; 21: 21-25