

Subscribe to RSS
DOI: 10.1055/s-0043-1762580
Comparison of Estrogen Receptor Status and Ki-67 Index in Core Needle Biopsy and Resected Specimen of Breast Carcinoma
Authors
Funding None.

Abstract
Background and Objectives The status of estrogen receptor (ER), progesterone receptor (PR), human epidermal growth factor receptor 2 (HER2), and Ki-67 expression in core needle biopsy and excision specimens has concurrent results, but many show discordance. However, only a few studies on the subject are available in India. Therefore, this study aims to compare the ER and Ki-67 expression status in core needle biopsy and excision specimens of breast carcinoma.
Materials and Methods In this cross-sectional analytical study, 50 breast carcinoma cases were histopathologically examined for ER and Ki-67 expression in both core needle biopsy and excision specimen. The interpreter was blinded for the evaluation of ER and Ki-67 expression index and the data obtained were analyzed using SPSS version 27.
Results The average age of the participants was 50 years and breast lump was the most common presenting complaint in all the cases. The concordance rate of histological typing between core needle biopsy and excision specimens was 96%, and the majority were invasive ductal carcinoma (60%) and not otherwise specified (48%) having Nottingham histologic grade 3 (46%). The concordance rate between core needle biopsy and excision specimen for ER and Ki-67 expression was 86% (n = 43) and 54% (n = 27), respectively. Most of the cases were found to be luminal A type (38%). Additionally, the sensitivity, specificity, positive predictive value, and negative predictive value of ER between core needle biopsy and excision specimen were 78.79, 100, 100, and 70.83%, respectively; however, these were 44, 64, 55, and 53.33%, respectively, for Ki-67.
Conclusion Although the concordance of the ER status between core needle biopsy and excision specimen was substantial, the discordance rate of Ki-67 was found to be high. Hence, relying solely on core needle biopsy for critical decision-making is inadvisable; however, core needle biopsy can be used as an initial procedure to examine histology and receptor status, Therefore, it is better to reconsider performing immunohistochemistry for the excision specimen, more importantly in ER-negative cases, to benefit the patient with targeted therapy.
Keywords
breast carcinoma - core needle biopsy - estrogen receptor - excision specimen - immunohistochemistry - Ki-67Introduction
Breast cancer (BC) is one of the most commonly diagnosed cancers, causing significant morbidity and mortality in women. BC is a molecularly heterogeneous disease and has high metastatic capacity; however, recent data show that the death rates due to BC have decreased due to early recognition and successful treatment.[1] The expression of estrogen receptor (ER) and progesterone receptor (PR) and, more recently, human epidermal growth factor receptor 2 (HER2)/neu have increasing importance in the management of breast malignancy.[2] In addition to these molecular markers, Ki-67 also aids in assessing the disease prognosis and determining the management plan accordingly. Many studies show that patients with ER + BC have prolonged disease-free survival after the primary treatment. Various studies also suggest that ER concordance rate is significantly higher than PR concordance rate because status assessment of PR requires a higher preparation quality than ER. The heterogeneous distribution of PR compared with ER detection within the tumor is also notable.[3]
Ki-67 is a nuclear protein and a biological tumor marker associated with cellular proliferation. It is considered the most representative tumor marker to predict proliferation. It is expressed during the S, G1, G2, and M phase of cell cycle but not in the resting phase (G0). Studies suggest that high index of Ki-67 indicates an aggressive tumor and predicts a poor prognosis.[4] Preoperative diagnosis of BC is one of the main goals of modern BC patient care. Core needle biopsy (CNB) of the breast has become a vital diagnostic tool for the diagnosis of both palpable and nonpalpable breast lesions. CNB plays a significant role in the preoperative triple assessment. Studies have revealed that CNB has a high sensitivity (91–99%), specificity (96–100%), positive predictive value (PPV; 100%), and negative predictive value (NPV; 100%).[5] Grading and typing of the tumor are also possible on CNB, thereby increasing the diagnostic information available when considering treatment options. Many studies imply that relying solely on CNB samples is not advisable because of the false-negative results that occur due to the heterogeneity of the tumor. Many western studies documented reasonable concordance rate of ER, PR, HER2/neu status, and Ki-67 expression between CNB and excision specimens and few with discordance. However, only a few Indian studies are available on this subject; hence, this study aims to evaluate and compare the ER status and Ki-67 expression between CNB and excision specimens in patients with breast carcinoma, which would provide both prognostic and therapeutic implications.
Materials and Methods
Study Population and Data Collection
This single-center cross-sectional study consists of conveniently sampled 50 female subjects having clinically presenting a lump in the breast, which is confirmed to be malignant by histopathological examination (HPE). They all had undergone both CNB and excision biopsy. However, the subjects with BC who have received neoadjuvant chemotherapy and were of non-neoplastic lesions of the breast were excluded from this study. Each subject was clinically evaluated by a surgeon for the presence of lump in the breast and the CNB and excision specimen were examined separately by a pathologist for gross and microscopic findings. The demographic and clinical data regarding clinical history, examination, investigations, clinical diagnosis, and operative findings were retrieved from the patient's data sheet and the data were anonymized. The study data were compiled in accordance with the declaration of Helsinki and the study was approved by the institutional ethics committee (# INST.EC/EC/091/2018–19 dt. 11.10.2018).
Immunohistochemistry
The whole CNB was embedded; however, a representative area from the excision specimen was taken for the preparation of paraffin-embedded block. A 5-µm section placed on positively charged slide was incubated at 60°C overnight and then subjected to antigen retrieval with trisodium citrate dihydrate (pH 8 to 9) in microwave oven at 95°C for 20 minutes with a 2-minute cooling interval followed by incubation at 50°C for 10 minutes. After peroxide blocking for 20 minutes, the sections were incubated with ER (# R06042RA) and Ki-67 (# R06096UA) primary antibodies purchased from PathnSitu for 90 minutes and the subsequent steps were performed according to the kit protocols. The evaluation of ER and Ki-67 status was blinded for data collection by the interpreter.
Statistical Analysis
The data collected were tabulated in MS Excel and analyzed using the IBM-SPSS software version 27.0. A correlation analysis was performed for the Ki-67 and ER statuses of CNBs and excision specimens, and a Student's t-test was also performed.
Results
Demographics and Clinicopathologic Characteristics
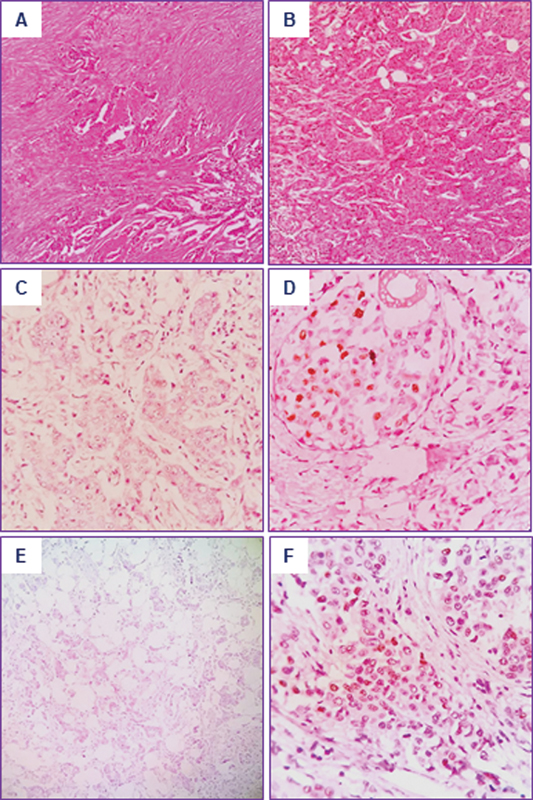
The basic demographic and clinicopathologic characteristics of the 50 patients in this cross-sectional study are summarized in [Table 1]. The mean age of the subjects was 50 years, with the most common age of presentation ranging from 41 to 60 years, which accounted for 62% of the cases. The laterality of the tumor in the study subjects did not differ significantly from left-sided (48%) to right-sided (52%) tumors; however, one of the cases was bilateral. All the subjects (100%) were presented with a palpable breast lump and the other associated symptoms in the decreasing frequency were breast pain (14%), skin ulceration (10%), puckering of the skin (8%), nipple retraction (4%), and nipple discharge (4%). According to the College of American Pathologists (CAP) protocol and WHO 2012, HPE was reported and it was found that the majority of the subjects had invasive ductal carcinoma (CNB in 60% and excision in 48%) and invasive lobular carcinoma (CNB in 30% and excision in 20%). A few subjects had pleomorphic lobular carcinoma, invasive carcinoma with medullary features and apocrine features, and metaplastic and mucinous carcinoma ([Figs. 1A, B]). Nottingham histologic grading of CNB and excision specimen showed that the majority were grade 3 (CNB in 59% and excision in 46%), followed by grade 2 (CNB in 29% and excision in 42%) and grade 1 (CNB in 12% and excision in 12%). The molecular phenotyping of BC found that the majority of the subjects (n = 19 [38%]) were of luminal A type, followed by triple negative (n = 11 [22%]), luminal B (HER2-negative, n = 7 [14%]), luminal B (HER2-positive, n = 7 [14%]), and HER2-positive (nonluminal, n = 6 [12%]) phenotype.
Abbreviations: CAP, College of American Pathologists; CNB, core needle biopsy; ER, estrogen receptor.
ER Status and Ki-67 Index in Breast Carcinoma
The immunohistochemical (IHC) analysis of the ER was positive in 26 (52%) and 33 (66%) subjects' CNB and excision specimen, respectively. Meanwhile, negative IHC staining for the ER was observed in 24 (48%) and 17 (34%) subjects' CNB and excision specimen, respectively ([Fig. 1C–F]; [Table 2]). There was a discrepancy in the ER status in seven subjects, and the majority of them (n = 4) were found to be invasive ductal carcinoma not otherwise specified (NOS; [Table S1]). In addition, low expression of Ki-67 was observed in 30 (60%) and 25 (50%) subjects' CNB and excision specimen, respectively. High expression of Ki-67 was seen in 20 (40%) and 25 (50%) subjects' CNB and excision specimen, respectively ([Table 2]). Twenty-three subjects showed a discrepancy for the Ki-67 index, and the majority of them (n = 14) were found to be invasive ductal carcinoma NOS ([Table S2]; [Fig. 2A–F]). Further, the cutoff values of ≤20 as low and >20 as high were used to categorize luminal A and luminal B molecular types. The concordance analysis of the receptor status, including positive and negative agreement, was calculated statistically using the kappa test and it was found that there was an extremely statistically significant (κ > 0.6, p < 0.0001) association between the ER status of CNB and excision specimen, while no significant difference was found for the Ki-67 index ([Table 2]).[6] [7] Further, sensitivity, specificity, PPV, and NPV of the ER and Ki-67 between the CNB and excision specimen are given in [Table 3]. It was found that the ER has better values, when compared with the Ki-67 index.
Abbreviations: CNB, core needle biopsy; ER, estrogen receptor.
Abbreviations: CI, confidence interval; CNB, core needle biopsy; ER, estrogen receptor.

Discussion
BC is currently the most common cancer among women and has seen a rise in the number of cases in recent years. Breast conservation surgery is becoming popular among women with BC. In recent years, interest in prognostic factors has been stimulated by the success of systemic adjuvant therapy for an early stage of cancer of the breast.[8] Fine needle aspiration cytology (FNAC) of the breast is being replaced by CNB and it is accepted as a choice for tissue sampling and as a part of the triple assessment for BC.[9] FNAC does not differentiate in situ and invasive breast carcinoma, but it can be examined in CNB. Therefore, it is considered superior.[8] Biomarker testing is most commonly performed on the CNB tissue, which has advantages such as rapid tissue fixation and the ability to utilize the results for systemic therapy planning, including administration of neoadjuvant systemic therapy and to observe the response to treatment.[10] An excision breast biopsy is indicated in the management of benign breast lesions like fibroadenoma and phyllodes tumor.[11] Few lesions are underestimated in CNB and in such cases excision of the tumor is advised.
IHC analysis of an invasive breast carcinoma is required for better categorization and intervention. IHC for the ER, PR, HER2/neu, and Ki-67, a proliferation marker, is more often performed in cases of BC as these biomarkers help in molecular classification and guide in treatment using targeted therapies.[12] The ER level is a powerful predictive factor for response to endocrine treatment and long-term outcome.[9] The American Society of Clinical Oncology (ASCO)/CAP guideline recommended 1% as the cutoff value for ER or PR positivity, leading to more patients receiving adjuvant endocrine therapy.[13] The Ki-67 antigen has been used to evaluate the proliferative activity of BC for several decades, and a meta-analysis has shown that high Ki-67 expression confers a higher risk of relapse and worse survival. In patients with advanced BC, higher Ki-67 levels have been significantly associated with decreased time to aromatase inhibitor treatment failure.[14] In this study, we performed IHC of only the ER and Ki-67 because an ER-positive BC has a targeted neoadjuvant therapy and Ki-67 aids in differentiating luminal A and luminal B like molecular types. However, the PR is an independent prognostic factor in molecular typing of BC, and in equivocal cases of HER2/neu, additionally, fluorescence in situ hybridization (FISH) has to be done to determine the molecular subtype. Moreover, the PR is infrequently expressed in ER tumors and is usually considered less important than the ER.[15]
The fifth decade of life is the most common age group in this study subjects. Similar observations were made by Pervin et al and Vaibhaw et al[23] wherein the peak incidence of BC is in the fifth decade of life.[16] [17] Further, the epidemiological studies at regional and global levels suggest that BC more frequently occurs at the premenopausal age in Indian and Asian women compared with the western women who get it a decade later.[17] In addition, the present study found that the most common presenting complaint was palpable lump, which was present in all the cases, and other associated complaints such as pain, nipple discharge, puckering of the skin, nipple retraction and skin ulceration were also observed. The studies by Pervin et al,[16] Al-amri et al[18] and Newton et al[19] observed similar complaints along with pain symptoms, more frequently, in 80% of cases because the patients were unaware of the lump in the early stages of breast carcinoma. Invasive ductal carcinoma NOS was the most common histological type in the CNB and excision specimens. This observation was supported by studies by Chen et al[14] (87.2%), You et al[6] (85.8%), and Robertson et al[20] (68.4%). Other rare histologic subtypes described in the present study are metaplastic carcinoma, pleomorphic lobular carcinoma, invasive carcinoma with medullary features, invasive carcinoma with apocrine features, mucinous carcinoma, invasive carcinoma with metaplastic features, invasive carcinoma with ductal and lobular features, and invasive carcinoma with neuroendocrine features. A positive correlation was noted between the CNB and excision specimens (96%) in this study and the study done by O'Leary et al.[21] Tumor type correlation between CNB and excision specimens was seen in 65.41% of cases.
We have observed a good concordance of the ER status between CNB and excision specimens, and our results are well supported by the findings in Ough et al,[22] Meattini et al,[23] and You et al,[6] suggesting that ER determination in CNB is reliable. The heterogeneity of the ER expression in tumor cell populations may have implications for analytic cell selection and for prognosis in patients with ER-positive carcinomas. Previous studies have reported that if core biopsy specimens are ER negative, surgical specimens should be analyzed.[24] However, a poor concordance was observed for Ki-67 between the CNB and excision specimens. Of the 23 discordant cases of Ki-67, 14 cases showed high index in the excision specimen. The possible explanation for this difference may be related to sampling error and tumor heterogeneity, as CNB might not reflect the real status of the entire tumor.[23] Additionally, edge artifacts can also yield discordant result.[15] Further, the high levels of Ki-67 have been associated with an increased risk of BC relapse and death, but there is no established cutoff for the classification of Ki-67 as high or low. Although some studies showed a higher Ki-67 index in core biopsy specimens, other studies showed a higher Ki-67 index in surgical specimens. However, the discordance rates of the Ki-67 index were higher than those of the ER, PR, and HER2 as there is an absence of guidelines for this marker. This may also be a contributing factor to its low concordance.[10]
Therefore, we suggest that Ki-67 should be detected both on CNB and excision samples, especially in hormonal-positive HER2-negative tumors, to avoid misclassifying tumor subtypes and possible omission of effective systemic therapy. The sensitivity and specificity with PPV and NPV of the ER and Ki-67 of the CNB and excision specimens was optimal and poor, respectively. Meattini et al[23] observed a higher sensitivity, specificity, NPV, and PPV. Overall, various studies suggest that the concordance rate between the CNB and excision specimens is higher for the ER than for the PR. A further large-scale study with long-term follow-up is advised to come up with an established guideline for Ki-67 measurement.[25]
Conclusion
Overall, this study found a substantially good concordance of the ER status and a higher discordance for the Ki-67 index between the CNB and excision specimens. However, it was difficult to categorize the ER-positive and HER2-negative tumors into luminal A and luminal B type tumor in discordant cases of Ki-67. Therefore, CNB is considered a valuable tool to classify breast carcinoma into surrogate molecular subtypes in patients without preoperative treatment. But relying solely on CNB for critical decision with regard to the treatment modalities is not recommended. Instead, it can be used as an initial procedure to examine the histology and the receptor status. Further, it is better to reconsider repeating IHC in the excision specimen, more importantly in ER-negative cases to benefit the patient with targeted therapy.
Conflict of Interest
None declared.
-
References
- 1 Feng Y, Spezia M, Huang S, Yuan C, Zeng Z, Zhang L. et al. Breast cancer development and progression: Risk factors, cancer stem cells, signaling pathways, genomics, and molecular pathogenesis. Genes Dis 2018; 5 (02) 77-106
- 2 Dabbs DJ. ed. Diagnostic Immunohistochemistry: Theranostic and Genomic Applications. 4th ed. Philadelphia, PA: Elsevier Saunders; 2014: 1-38
- 3 Dai X, Xiang L, Li T, Bai Z. Cancer Hallmarks, Biomarkers and Breast Cancer Molecular Subtypes. J Cancer 2016; 7 (10) 1281-1294
- 4 Miller I, Min M, Yang C, Tian C, Gookin S, Carter D. et al. Ki67 is a Graded Rather than a Binary Marker of Proliferation versus Quiescence. Cell Rep 2018; 24 (05) 1105-1112.e5
- 5 Saha A. FNAC Versus Core Needle Biopsy: A Comparative Study in Evaluation of Palpable Breast Lump. J Clin Diagn Res 2016; 342-353
- 6 You K, Park S, Ryu JM, Kim I, Lee SK, Yu J. et al. Comparison of Core Needle Biopsy and Surgical Specimens in Determining Intrinsic Biological Subtypes of Breast Cancer with Immunohistochemistry. J Breast Cancer 2017; 20 (03) 297
- 7 Chen X, Sun L, Mao Y, Zhu S, Wu J, Huang O. et al. Preoperative core needle biopsy is accurate in determining molecular subtypes in invasive breast cancer. BMC Cancer 31:185
- 8 Gupta MK, Gupta B, Kumar K. Comparative study of core needle biopsy with excisional biopsy: To determine diagnostic accuracy & concordance with er/pr/her-2/neu status. Indian J Pathol Oncol 2016; 3 (04) 576
- 9 Asogan A, Hong G, Arni PrabhakaranS. Concordance between core needle biopsy and surgical specimen for oestrogen receptor, progesterone receptor and human epidermal growth factor receptor 2 status in breast cancer. Singapore Med J 2017; 58 (03) 145-149
- 10 Greer LT, Rosman M, Mylander WC, Hooke J, Kovatich A, Sawyer K. et al. Does Breast Tumor Heterogeneity Necessitate Further Immunohistochemical Staining on Surgical Specimens?. J Am Coll Surg 2013; 216 (02) 239-251
- 11 Isikhuemen ME, Eliboh MO, Eni EU, Ekwedigwe KC, Sunday-Adeoye I. Outcome of open excisional breast biopsies in Abakaliki, South-East Nigeria. Pan Afr Med J [Internet] 2018;31:185
- 12 Clark BZ, Onisko A, Assylbekova B, Li X, Bhargava R, Dabbs DJ. Breast cancer global tumor biomarkers: a quality assurance study of intratumoral heterogeneity. Mod Pathol 2019; Mar; 32 (03) 354-366
- 13 Zhu S, Wu J, Huang O, He J, Zhu L, Li Y. et al. Clinicopathological Features and Disease Outcome in Breast Cancer Patients with Hormonal Receptor Discordance between Core Needle Biopsy and Following Surgical Sample. Ann Surg Oncol 2019; 26 (09) 2779-2786
- 14 Chen X, Sun L, Mao Y, Zhu S, Wu J, Huang O. et al. Preoperative core needle biopsy is accurate in determining molecular subtypes in invasive breast cancer. BMC Cancer 2013 13. 390
- 15 Arnedos M, Nerurkar A, Osin P, A'Hern R, Smith IE, Dowsett M. Discordance between core needle biopsy (CNB) and excisional biopsy (EB) for estrogen receptor (ER), progesterone receptor (PgR) and HER2 status in early breast cancer (EBC). Ann Oncol 2009; 20 (12) 1948-1952
- 16 Pervin M, Nath H, Bahar M, Alam A, Bhowmik J. Study on Clinical Presentation of Breast Carcinoma of 50 Cases. Chattagram Maa-O-Shishu Hosp Med Coll J 2014; 13 (02)
- 17 Vaibhaw K, Rathi S. Assessment of Incidence of Various Types of Breast Cancer According to Age. Int J Med Res Prof 2018; 4 (02) 140-143
- 18 Al-Amri A. Clinical presentation and causes of the delayed diagnosis of breast cancer in patients with pregnancy associated breast cancer. J Fam Community Med 2015; 22 (02) 96
- 19 Newton P. The presentation and management of female breast symptoms in general practice in Sheffield. Fam Pract 1999; 16 (04) 360-365
- 20 Robertson S, Rönnlund C, de Boniface J, Hartman J. Re-testing of predictive biomarkers on surgical breast cancer specimens is clinically relevant. Breast Cancer Res Treat 2019; 174 (03) 795-805
- 21 O'Leary R. Agreement between preoperative core needle biopsy and postoperative invasive breast cancer histopathology is not dependent on the amount of clinical material obtained. J Clin Pathol 2004; 57 (02) 193-195
- 22 Ough M, Velasco J, Hieken TJ. A comparative analysis of core needle biopsy and final excision for breast cancer: histology and marker expression. Am J Surg 2011; 201 (05) 692-694
- 23 Meattini I, Bicchierai G, Saieva C, De Benedetto D, Desideri I, Becherini C. et al. Impact of molecular subtypes classification concordance between preoperative core needle biopsy and surgical specimen on early breast cancer management: Single-institution experience and review of published literature. Eur J Surg Oncol 2017; 43 (04) 642-648
- 24 Ricci MD, Calvano FilhoCMC, Oliveira FilhoHR, de, Filassi JR, Pinotti JA, Baracat EC. Analysis of the concordance rates between core needle biopsy and surgical excision in patients with breast cancer. Rev Assoc Medica Bras 1992 2012; 58 (05) 532-536
- 25 Ahn S, Lee J, Cho M-S, Park S, Sung SH. Evaluation of Ki-67 Index in Core Needle Biopsies and Matched Breast Cancer Surgical Specimens. Arch Pathol Lab Med 2018; 142 (03) 364-368
Address for correspondence
Publication History
Article published online:
14 April 2023
© 2023. The Author(s). This is an open access article published by Thieme under the terms of the Creative Commons Attribution License, permitting unrestricted use, distribution, and reproduction so long as the original work is properly cited. (https://creativecommons.org/licenses/by/4.0/)
Thieme Medical and Scientific Publishers Pvt. Ltd.
A-12, 2nd Floor, Sector 2, Noida-201301 UP, India
-
References
- 1 Feng Y, Spezia M, Huang S, Yuan C, Zeng Z, Zhang L. et al. Breast cancer development and progression: Risk factors, cancer stem cells, signaling pathways, genomics, and molecular pathogenesis. Genes Dis 2018; 5 (02) 77-106
- 2 Dabbs DJ. ed. Diagnostic Immunohistochemistry: Theranostic and Genomic Applications. 4th ed. Philadelphia, PA: Elsevier Saunders; 2014: 1-38
- 3 Dai X, Xiang L, Li T, Bai Z. Cancer Hallmarks, Biomarkers and Breast Cancer Molecular Subtypes. J Cancer 2016; 7 (10) 1281-1294
- 4 Miller I, Min M, Yang C, Tian C, Gookin S, Carter D. et al. Ki67 is a Graded Rather than a Binary Marker of Proliferation versus Quiescence. Cell Rep 2018; 24 (05) 1105-1112.e5
- 5 Saha A. FNAC Versus Core Needle Biopsy: A Comparative Study in Evaluation of Palpable Breast Lump. J Clin Diagn Res 2016; 342-353
- 6 You K, Park S, Ryu JM, Kim I, Lee SK, Yu J. et al. Comparison of Core Needle Biopsy and Surgical Specimens in Determining Intrinsic Biological Subtypes of Breast Cancer with Immunohistochemistry. J Breast Cancer 2017; 20 (03) 297
- 7 Chen X, Sun L, Mao Y, Zhu S, Wu J, Huang O. et al. Preoperative core needle biopsy is accurate in determining molecular subtypes in invasive breast cancer. BMC Cancer 31:185
- 8 Gupta MK, Gupta B, Kumar K. Comparative study of core needle biopsy with excisional biopsy: To determine diagnostic accuracy & concordance with er/pr/her-2/neu status. Indian J Pathol Oncol 2016; 3 (04) 576
- 9 Asogan A, Hong G, Arni PrabhakaranS. Concordance between core needle biopsy and surgical specimen for oestrogen receptor, progesterone receptor and human epidermal growth factor receptor 2 status in breast cancer. Singapore Med J 2017; 58 (03) 145-149
- 10 Greer LT, Rosman M, Mylander WC, Hooke J, Kovatich A, Sawyer K. et al. Does Breast Tumor Heterogeneity Necessitate Further Immunohistochemical Staining on Surgical Specimens?. J Am Coll Surg 2013; 216 (02) 239-251
- 11 Isikhuemen ME, Eliboh MO, Eni EU, Ekwedigwe KC, Sunday-Adeoye I. Outcome of open excisional breast biopsies in Abakaliki, South-East Nigeria. Pan Afr Med J [Internet] 2018;31:185
- 12 Clark BZ, Onisko A, Assylbekova B, Li X, Bhargava R, Dabbs DJ. Breast cancer global tumor biomarkers: a quality assurance study of intratumoral heterogeneity. Mod Pathol 2019; Mar; 32 (03) 354-366
- 13 Zhu S, Wu J, Huang O, He J, Zhu L, Li Y. et al. Clinicopathological Features and Disease Outcome in Breast Cancer Patients with Hormonal Receptor Discordance between Core Needle Biopsy and Following Surgical Sample. Ann Surg Oncol 2019; 26 (09) 2779-2786
- 14 Chen X, Sun L, Mao Y, Zhu S, Wu J, Huang O. et al. Preoperative core needle biopsy is accurate in determining molecular subtypes in invasive breast cancer. BMC Cancer 2013 13. 390
- 15 Arnedos M, Nerurkar A, Osin P, A'Hern R, Smith IE, Dowsett M. Discordance between core needle biopsy (CNB) and excisional biopsy (EB) for estrogen receptor (ER), progesterone receptor (PgR) and HER2 status in early breast cancer (EBC). Ann Oncol 2009; 20 (12) 1948-1952
- 16 Pervin M, Nath H, Bahar M, Alam A, Bhowmik J. Study on Clinical Presentation of Breast Carcinoma of 50 Cases. Chattagram Maa-O-Shishu Hosp Med Coll J 2014; 13 (02)
- 17 Vaibhaw K, Rathi S. Assessment of Incidence of Various Types of Breast Cancer According to Age. Int J Med Res Prof 2018; 4 (02) 140-143
- 18 Al-Amri A. Clinical presentation and causes of the delayed diagnosis of breast cancer in patients with pregnancy associated breast cancer. J Fam Community Med 2015; 22 (02) 96
- 19 Newton P. The presentation and management of female breast symptoms in general practice in Sheffield. Fam Pract 1999; 16 (04) 360-365
- 20 Robertson S, Rönnlund C, de Boniface J, Hartman J. Re-testing of predictive biomarkers on surgical breast cancer specimens is clinically relevant. Breast Cancer Res Treat 2019; 174 (03) 795-805
- 21 O'Leary R. Agreement between preoperative core needle biopsy and postoperative invasive breast cancer histopathology is not dependent on the amount of clinical material obtained. J Clin Pathol 2004; 57 (02) 193-195
- 22 Ough M, Velasco J, Hieken TJ. A comparative analysis of core needle biopsy and final excision for breast cancer: histology and marker expression. Am J Surg 2011; 201 (05) 692-694
- 23 Meattini I, Bicchierai G, Saieva C, De Benedetto D, Desideri I, Becherini C. et al. Impact of molecular subtypes classification concordance between preoperative core needle biopsy and surgical specimen on early breast cancer management: Single-institution experience and review of published literature. Eur J Surg Oncol 2017; 43 (04) 642-648
- 24 Ricci MD, Calvano FilhoCMC, Oliveira FilhoHR, de, Filassi JR, Pinotti JA, Baracat EC. Analysis of the concordance rates between core needle biopsy and surgical excision in patients with breast cancer. Rev Assoc Medica Bras 1992 2012; 58 (05) 532-536
- 25 Ahn S, Lee J, Cho M-S, Park S, Sung SH. Evaluation of Ki-67 Index in Core Needle Biopsies and Matched Breast Cancer Surgical Specimens. Arch Pathol Lab Med 2018; 142 (03) 364-368