

Subscribe to RSS
DOI: 10.1055/s-0043-1771196
When Friend Becomes Foe: Complications of Fibroadenoma Imaging Spectrum
Authors

Abstract
Fibroadenoma are the most common benign breast lesions. Complications in fibroadenoma although rare in occurrence, are reported. It is important to be aware of the possible complications, both benign and malignant which may require surgical management. Commonly encountered benign complications in a fibroadenoma are infarction, rapid increase in size, and lactational changes. A common differential of a giant fibroadenoma is phyllodes tumor which has subtle imaging differences. Malignant transformation of a fibroadenoma is very rare although cases are reported (0.02%). Breast is a dynamic organ and is influenced by the hormone surges occurring typically during pregnancy and lactation, it causes changes in morphology of prior existing fibroadenoma which may mimic like a malignancy and hence knowledge of these benign complications in a fibroadenoma is also important. To identify the subtle radiologic imaging features which may suggest complication developing in a known fibroadenoma, prompting for a histopathological examination correlation. In this article, we discuss the imaging features of complications in a fibroadenoma—benign and malignant. Sinister etiology secondarily engulfing a fibroadenoma and sinister focus developing in a fibroadenoma will be discussed. Also, the benign complications in a fibroadenoma like lactational changes, spontaneous infarction within a fibroadenoma, and excessive increase in the size of fibroadenoma with degenerative changes due to the estrogen and progesterone effect which can mimic like a malignancy will be illustrated. A careful history, meticulous scanning, close monitoring, and histopathological correlation is invaluable to identify these complications in a known fibroadenoma and thus guide in the appropriate management of these lesions.
Introduction
Fibroadenoma is the most common benign breast lump. These are benign fibroepithelial neoplasms with proliferation of stromal and epithelial cells. Most of the patients are asymptomatic and these can be picked up on routine screening mammograms or incidentally diagnosed on breast ultrasound performed for other reasons. Another common presentation is of a woman complaining of a palpable long-standing painless mobile lump.
Fibroadenomas' general mammographic imaging features are circumscribed discrete oval mass hypo- or isodense to the breast glandular tissue, to a mass with macrolobulation or partially obscured margin. On ultrasound they are typically seen as a circumscribed, round to ovoid, or macrolobulated mass with generally uniform hypoechogenicity. Intralesional sonographically detectable calcification may be seen in approximately 10% of cases.[1] A close mimicker of a fibroadenoma is phyllodes tumor, subtle imaging features which point to a suspicion of phyllodes are a rapidly growing mass with macrolobulated margins, internal cleft-like cystic spaces, posterior acoustic enhancement, and presence of prominent internal vascularity. These features when present should be classified as Breast Imaging Reporting and Data System (BI-RADS) 4A lesion and a histopathological correlation should be performed.[2]
Typical fibroadenoma on imaging are classified as BI-RADS 3 lesions having a 0 to 2% risk of malignancy and are to be followed up on routine imaging. Involuting calcified/partly calcified fibroadenoma are classified as BI-RADS 2 lesions with essentially 0% risk of malignancy. Although these are benign breast lesions, complications in fibroadenoma can occur, though rare.[3] The usual presentation in a fibroadenoma undergoing complication is of a woman complaining of a long-standing lump which may or may not have been a histopathologically confirmed fibroadenoma now presenting with increasing size of the lump/pain in the lump. Another presentation is an asymptomatic woman, undergoing a follow-up for fibroadenoma, developing suspicious features on subsequent scan like heterogeneous echotexture with or without internal cystic/necrotic areas, irregular margins, interval appearance of vascularity or pleomorphic microcalcifications as compared with the previous imaging, and histopathology confirmed fibroadenoma. These require biopsies to confirm if there is malignant transformation or if it is due to benign complications like degenerative changes in a fibroadenoma, lactational changes in a fibroadenoma, or infarcted fibroadenoma. Interval development of malignancy adjacent to fibroadenoma engulfing it could also be responsible for similar patient presentation.
As for general population, fibroadenomas are also the most common benign neoplasms seen during pregnancy and lactation, these are thought to be present prior to pregnancy and not known to the patient as they were nonpalpable and routine screening is not performed in the said age group. Fibroadenomas being hormone-sensitive tumors undergo morphologic changes in response to the gravidic hormone surge which could lead to increase in the size of fibroadenoma which now may become palpable to the woman with associated ultrasonographically detected changes like increased tumoral vascularity. A lactating woman might present with a sudden-onset acute pain in the prior known fibroadenoma, which might suggest an infarction in a fibroadenoma which although rare is seen in the third trimester or during lactation.[4]
Another known entity is lactational change in a fibroadenoma which occurs due to hormonal effect on the epithelial cells in fibroadenoma.
Due to the varied morphologic changes in fibroadenomas during pregnancy and lactation, these should be meticulously scanned with a good knowledge of the commonly seen pregnancy-associated changes and if a sinister etiology is thought of, a core needle biopsy should be performed in order not to misdiagnose an underlying pregnancy-associated breast cancer.[5]
In this article, we aim to discuss and illustrate the radiologic features which help us identify a complicated fibroadenoma and also help us in the identification of any newly developed sinister morphologic feature in a previously known fibroadenoma which would now need a core needle biopsy and a histopathological diagnosis.
The commonly seen complications in fibroadenoma in our clinical practice are fibromyxoid changes in fibroadenoma, lactational changes in fibroadenoma, spontaneous infarction in a fibroadenoma, carcinoma engulfing an involuted fibroadenoma, and carcinoma arising in a fibroadenoma. These will be discussed further in this article.
Case 1
A 27-year-old female with 5 months of pregnancy presented with a history of right breast lump, which on ultrasound ([Fig. 1A] and [B]) and on histopathology ([Fig. 1C]) was confirmed to be a fibroadenoma.
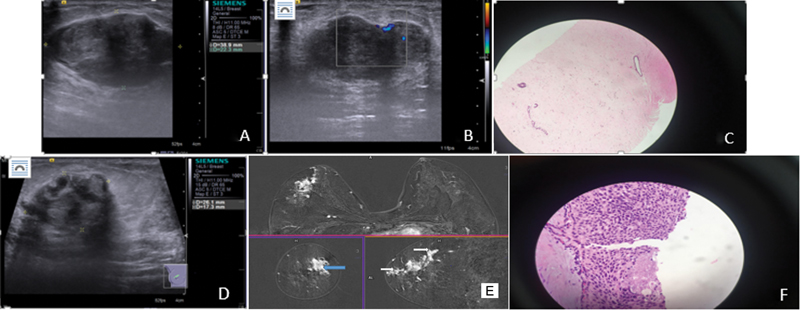
Patient presented again after 4 years as the lump felt different in consistency. On follow-up ultrasound, although the size of the mass was same, it now had heterogeneous echotexture with internal vascularity and subtle irregularity of the margins ([Fig. 1D]). In addition, there was interval appearance of few prominent ducts with mild ductal wall thickening and nodularity extending from the mass to the nipple.
Magnetic resonance imaging (MRI) breast was performed, which revealed heterogeneously enhancing ill-defined mass lesion in the upper outer quadrant of the right breast. There were thickened nodular enhancing ducts seen anterior and posterior to the lesion in a segmental distribution reaching up till the nipple ([Fig. 1E]). As the findings on the current scan were not typical of benign etiology, a repeat biopsy of the same lesion was performed and it revealed low-grade ductal carcinoma in situ (DCIS) on a background of fibroadenoma ([Fig. 1F]). On final histopathological examination (HPE) it was confirmed to be invasive ductal carcinoma; grade 2 with extensive DCIS.
Case 2
A 37-year-old female presented with a long-standing lump in left breast which had increased in size over some time. External core biopsy was reported as benign. Patient underwent a mammogram with spot compression view of the mass in left breast which revealed an oval circumscribed mass seen in the upper outer quadrant of the left breast associated with fine pleomorphic microcalcification along its lateral margin ([Fig. 2A] - left MLO [mediolateral oblique], 2B - left CC [craniocaudal], and 2C - spot compression view of the mass in CC view). Ultrasonogram ([Fig. 2D]) revealed a circumscribed, parallel hypoechoic mass with multiple calcific specks along its lateral margin, in the area of mammographic concern. The mass revealed peripheral vascularity and had an appearance of a fibroadenoma except that it had subtle indistinct margin along its lateral aspect and microcalcification were concentrated along this margin rather than uniformly distributed. The part of the lump which showed calcification was more hypoechoic than the rest of the area. As the initial biopsy results were discordant, patient had contrast-enhanced (CE) breast MRI ([Fig. 2E]) which revealed an oval circumscribed mass with subtle irregular margin showing enhancement along its lateral aspect. In view of majority of the mass not showing any significant enhancement and relatively circumscribed with history of long duration of mass, a possibility of fibroadenoma with malignant transformation was given on MRI. A core needle biopsy targeting the lateral aspect of the mass was done and microcalcifications were confirmed on the specimen radiograph. Histopathology confirmed invasive ductal carcinoma (IDC) arising de novo in a fibroadenoma. On final histopathology, IDC grade II with high-grade DCIS arising in a background of fibroadenoma was confirmed.

Case 3
A 44-year-old female came to the breast clinic with complaint of multiple bilateral breast lumps. Mammogram ([Fig. 3A] and [B]) was extremely dense, with multiple high-density oval/round masses, few of them showing obscured margins. On ultrasound ([Fig. 3C]) numerous low echogenic nodules were seen nearly completely occupying both breasts. A diagnosis of multiple fibroadenomas in bilateral breast was made, BI-RADS 2.

Although 1-year follow-up was unremarkable, her second follow-up was after another 10 months as she complained of right breast swelling, skin thickening, and right nipple retraction.
Ultrasound again confirmed multiple fibroadenomas in both breasts; however, the fibroadenoma in the right retroareolar region revealed internal specks of calcification ([Fig. 3D]) and marked internal vascularity ([Fig. 3E]). Skin thickening was also seen on the right side.
CE-MRI breast ([Fig. 3F]) revealed multiple enhancing mass lesions of varying sizes scattered in both breasts as before with interval appearance of skin thickening and nipple retraction on the right side. Ultrasound-guided biopsy from the suspicious lesion with internal calcification on the right side was performed along with random biopsies from the right breast.
Histopathology of both samples revealed neoplasm comprising of compressed and few dilated ducts embedded in a fibromyxoid stroma suggestive of fibroadenomas. In addition, few tumor emboli were seen. The tumor cells possessed moderate eosinophilic cytoplasm and moderately pleomorphic nuclei. Few mitotic figures were discernible.
The final diagnosis was of fibroadenomas with malignant lymphovascular invasion and tumor emboli in the fibroadenoma as well as in the adjoining parenchyma in the right breast.
Case 4
A 33-year-old female with a past history of adenocarcinoma of gallbladder presented with a hard palpable lump in the left breast. A mammogram was done which showed a partly obscured dense mass in the upper central left breast ([Fig. 4A] and [B]).

On ultrasonogram, in the area of the palpable abnormality a relatively circumscribed mass with heterogeneous echotexture and no internal vascularity was seen. There were thick-walled nodular ducts extending from the mass toward the nipple ([Fig. 4C] and [D]). BI-RADS 4B was given and a core needle biopsy was performed. On biopsy IDC grade II was diagnosed.
CE-MRI breast was done to know the exact extent of disease ([Fig. 4E–H]). There was an area of non-mass enhancement seen in the upper inner quadrant of the left breast which was seen partially encasing a nonenhancing circumscribed mass suggesting a malignant lesion adjoining a benign fibroadenoma which was abutting the malignant mass. This was further confirmed on positron emission tomography-computed tomography which showed a fluorodeoxyglucose (FDG) avid area of segmental enhancement abutting a non-FDG avid circumscribed fibroadenoma ([Fig. 4I]). Differentiating a cancer developing de novo within a fibroadenoma and cancer adjoining to the fibroadenoma partially/completely encasing the fibroadenoma can be difficult on imaging and histopathology may be decisive.
The patient was started on neoadjuvant chemotherapy followed by surgery. On HPE, findings were confirmed.
Case 5
A 45-year-old female presented with a complaint of right breast lump. A diagnostic mammogram ([Fig. 5A]) was done which showed circumscribed rounded high-density mass with macrolobulated margins in the right breast nearly occupying whole of the breast. This was an interval development compared with a previous screening mammogram done 4 years back.

On ultrasound ([Fig. 5B]) there was a large heterogeneous oval parallel mass with macrolobulated mildly hyperechoic mass occupying nearly the whole of the right breast. Marked internal vascularity was noted. BI-RADS 4A was assigned and a possibility of a giant fibroadenoma/phyllodes was considered.
A core needle biopsy was done. The biopsy confirmed a cellular fibroadenoma. Patient was advised excision in view of large size, however, the patient refused. A close follow-up was advised.
Patient returned after 6 months with history of increase in the size of right breast lump. On ultrasound there was a large complex cystic lesion in the retroareolar region with no significant/minimal internal vascularity ([Fig. 5C]). A CE-MRI confirmed a large lobulated cystic lesion occupying the whole of the central right breast, with internal hemorrhagic contents and enhancing septae ([Fig. 5D]). The solid peripheral component revealed type II curves with minimal low apparent diffusion coefficient values. Possibility of a malignant phyllodes and infarcted fibroadenoma were raised.
On histopathology an infarcted fibroadenoma was confirmed.
Case 6
A 23-year-old lactating female came to the breast clinic with a large palpable painless soft lump in the right breast. Her ultrasound ([Fig. 6A]) revealed a large complex solid cystic lesion with circumscribed margins in the central right breast ([Fig. 6B]). Mobile hyperechoic nodules were seen floating in the nondependent part. The solid component revealed marked internal vascularity. BI-RADS 4 was assigned and biopsy was done.

Fibroadenoma with florid lactational changes within was confirmed on histopathology. In view of suspicious imaging findings, the mass was excised. Histopathology revealed a neoplasm composed of compressed ducts, tubules, and occasional dilated ducts embedded in a fibrous stroma. Lactational changes were noted.
The final diagnosis was again of a fibroadenoma with florid lactational changes.
Discussion
Fibroadenomas are benign fibroepithelial neoplasms. Although there is no increased risk of occurrence of carcinoma in patients with fibroadenomas, rare cases of development of in situ/invasive carcinoma in long-standing fibroadenomas are reported. It is therefore prudent to view these benign lesions with caution and a HPE should be performed in cases with atypical imaging features such as an increase in size, irregularity of margins, altered echotexture, marked internal vascularity, etc.[3]
A close mimicker of fibroadenoma is phyllodes tumor, subtle imaging differences like large lesions with lobulated margins, internal cystic clefts, prominent internal vascularity, and posterior acoustic enhancement should raise a suspicion of phyllodes tumor and a tissue diagnosis should be done.[4] [6] [7] These require wide local excision, because of the potential of local recurrence and possibility of malignant transformation.
Pregnancy-related changes in breast are caused due to elevated estrogen levels which causes morphological alterations in preexisting benign breast lesions like fibroadenomas such as infarction and florid lactational changes.[3] [8] However, a low threshold of suspicion should be kept for performing HPE to avoid delay in diagnosis of a pregnancy-associated breast cancers due to their varied imaging features.
Conflict of Interest
None declared.
-
References
- 1 Fornage BD, Lorigan JG, Andry E. Fibroadenoma of the breast: sonographic appearance. ERadiology 1989; 172 (03) 671-675
- 2 Plaza MJ, Swintelski C, Yaziji H, Torres-Salichs M, Esserman LE. Phyllodes tumor: review of key imaging characteristics. Breast Dis 2015; 35 (02) 79-86
- 3 El-Essawy MAL, Haidary A, Khan AL. Ductal carcinoma in situ (DCIS) in breast fibroadenoma. Egypt J Radiol Nucl Med 2020; 51: 1-7
- 4 Lee SE, Bae YK. Breast lesions during pregnancy and lactation: a pictorial essay. Ultrasonography 2020; 39 (03) 298-310
- 5 Maia AF, Solinho M, Vicente Costa R, Alves O, Nogueira M. The importance of carefully evaluating breast masses during pregnancy. Acta Med Port 2023; 36 (02) 143-144
- 6 Tan PH. Fibroepithelial lesions revisited: implications for diagnosis and management. Mod Pathol 2021; 34 (Suppl. 01) 15-37
- 7 Sharma BB, Bhardwaj N, Dewan S, Aziz MR. Adolescent fibroadenoma (Breast” Mouse”)–role of Radiology in assisting diagnosis: a case report. European Journal of Medical Case Reports. 2017; 1: 5-9
- 8 Cha Y, Kim HW, Kim HS, Won TW. Spontaneous infarction of phyllodes tumor of the breast in a postpartum woman: a case report. J Korean Soc Radiol 2017; 77 (05) 327-332
Address for correspondence
Publication History
Article published online:
05 October 2023
© 2023. Indographics. This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/)
Thieme Medical and Scientific Publishers Pvt. Ltd.
A-12, 2nd Floor, Sector 2, Noida-201301 UP, India
-
References
- 1 Fornage BD, Lorigan JG, Andry E. Fibroadenoma of the breast: sonographic appearance. ERadiology 1989; 172 (03) 671-675
- 2 Plaza MJ, Swintelski C, Yaziji H, Torres-Salichs M, Esserman LE. Phyllodes tumor: review of key imaging characteristics. Breast Dis 2015; 35 (02) 79-86
- 3 El-Essawy MAL, Haidary A, Khan AL. Ductal carcinoma in situ (DCIS) in breast fibroadenoma. Egypt J Radiol Nucl Med 2020; 51: 1-7
- 4 Lee SE, Bae YK. Breast lesions during pregnancy and lactation: a pictorial essay. Ultrasonography 2020; 39 (03) 298-310
- 5 Maia AF, Solinho M, Vicente Costa R, Alves O, Nogueira M. The importance of carefully evaluating breast masses during pregnancy. Acta Med Port 2023; 36 (02) 143-144
- 6 Tan PH. Fibroepithelial lesions revisited: implications for diagnosis and management. Mod Pathol 2021; 34 (Suppl. 01) 15-37
- 7 Sharma BB, Bhardwaj N, Dewan S, Aziz MR. Adolescent fibroadenoma (Breast” Mouse”)–role of Radiology in assisting diagnosis: a case report. European Journal of Medical Case Reports. 2017; 1: 5-9
- 8 Cha Y, Kim HW, Kim HS, Won TW. Spontaneous infarction of phyllodes tumor of the breast in a postpartum woman: a case report. J Korean Soc Radiol 2017; 77 (05) 327-332