

Subscribe to RSS
DOI: 10.1055/s-0043-1777322
Central Nonenhancement Sign in Carotid Body Tumor on CT Angiography
Authors


Abstract
Carotid body tumors are rare benign tumors that arise in the carotid space of neck typically presenting as soft to firm, painless swelling in the neck. While specific imaging characteristics have been previously described for carotid body tumors, we report a new imaging sign in three cases of carotid body tumors on computed tomography angiography.
Introduction
Carotid body is one of the sites of a group of paraganglia and receives its blood supply mostly from the carotid bifurcation and the external carotid artery (ECA).[1]
Carotid body tumor (CBT), the most common paraganglioma of the neck, is a rare benign tumor arising from the carotid body.[2] [3] [4] Radiological evaluation of CBTs ranges from ultrasonography, computed tomography (CT) scan, magnetic resonance imaging, to mildly invasive evaluations like diagnostic angiography.
On CT scans, these present as soft tissue lesions at the carotid bifurcation in the carotid space, causing the internal (ICA) and ECAs to splay apart with intense and homogenous enhancement on postcontrast scans.[3] While most studies have reported their findings based on the parenchymal phase, none of the studies have commented on its enhancement pattern on CT angiography.
We present a case series of three cases of CBT who underwent CT angiography showing a newly described enhancement pattern on CT angiography that might help in diagnosis of CBTs.
Cases
Case 1
A 44-year-old female patient presented with complaints of painless swelling on the left side of the neck for 1 year. On examination, the swelling was firm in consistency with thrill on palpation.
Ultrasonography showed a well-defined lesion adjacent to the carotid artery with significantly increased vascularity on color Doppler.
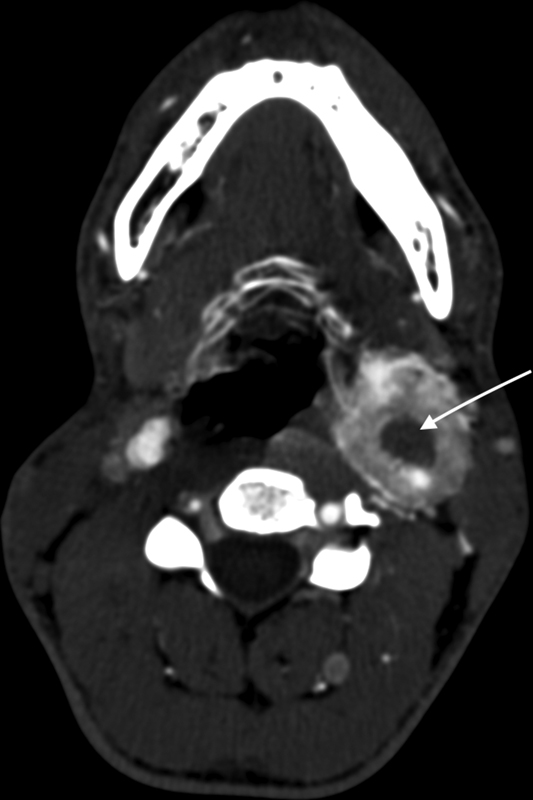
The patient was subjected to CT angiography. The angiogram phase was taken as soon as the tracker region of interest, placed at the arch reached 120 Hounsfield Unit threshold. Delayed phase was taken after 1 minute of the angiogram phase. CT showed a well-defined hypodense soft tissue lesion in left carotid space ([Fig. 1]). The lesion showed peripheral thick rind of enhancement with central area encasing the ICA showing no significant enhancement giving a central nonenhancement sign. The patient was taken up for surgery and tumor was removed with graft replacement of the involved ICA. Histopathology of the tumor showed features of CBT.

Case 2
A 21-year-old male patient presented with a painless swelling on the left side of his neck, below the angle of mandible, which had been present for past 8 months. On examination, a firm, pulsatile, and nontender swelling was detected just below the angle of mandible on the left side.
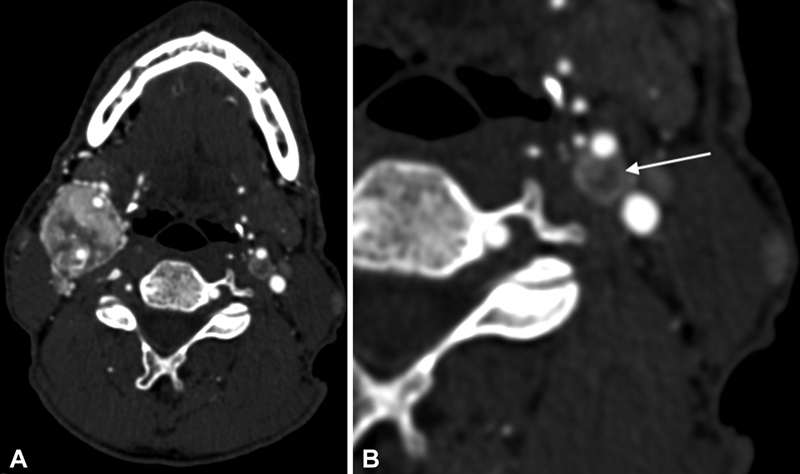
CT angiography revealed a well-defined enhancing lesion located at the left carotid bifurcation characterized by central nonenhancement and peripheral rind of enhancement ([Fig. 2]) The ICA was encased by the lesion with ECA at the periphery of the tumor. The tumor was surgically removed and subsequently diagnosed as CBT on histopathology.
Case 3
A 65-year-old male patient presented with complaints of swelling on the right side of the neck. CT angiography ([Fig. 3]) showed bilateral enhancing tumors at the carotid bifurcation. The larger CBT on the right side encased the right ICA and ECA and exhibited a more heterogenous enhancement pattern. The smaller tumor on the left side showed peripheral enhancement with central nonenhancing area on CT angiography.
Discussion
Typically described findings for CBTs on postcontrast scans include a well-defined lesion at carotid bifurcation, leading to the splaying of the carotid arteries and showing intense, homogenous enhancement. However, enhancement pattern of CBTs on CT angiography does not usually exhibit the intense, homogenous pattern, as seen in our case series. We describe a new enhancement pattern of CBTs on CT angiography that features a central area of nonenhancement. Possible explanation for this unique enhancement pattern of CBTs can be as follows:
-
The predominant blood supply to the carotid body, and consequently the tumor, originates from the carotid bifurcation and ECA. However, as the ICA is often the one that is completely encased, the branches of ECA supplying the highly vascular tumor may enter from the periphery, resulting in peripheral enhancement ([Fig. 1]).
-
Furthermore, with the advancement of CT machines, newer and faster scanner can scan the lesion more rapidly, allowing less time for the entire tumor to enhance. As a result, the peripheral part receives the initial bulk of the contrast, displaying enhancement and creating a central nonenhancement sign.
These reasons can be further strengthened by the fact that when delayed images (acquired 1 minute after the angiography phase) of the cases mentioned above were analyzed, the lesion showed uniform enhancement, thus ruling out the possibility of nonenhancing necrotic areas ([Fig. 4]).

Shamblin[5] in 1971 came up with a classification system that divides tumor based on their relationship with the surrounding vessels, correlating this with surgical difficulty encountered during tumor resection. While they did mention the encasement of the carotid arteries by the tumor, they did not comment on the involvement of ECA in comparison to the ICA.
To our knowledge, no study to date has reported the incidence of the involvement of the ECA compared to the ICA in CBTs. It is conceivable that tumors encasing the distal ICA with arterial supply from ECA may predominantly show this characteristic sign. However, a more extensive study with a larger cohort of CBT patients is necessary to analyze the incidence of involvement of each vessel. Furthermore, it is important to examine the presence of this sign in patients with different combinations of carotid artery involvement (i.e., other than the predominant encasement of ICA as compared to ECA observed in the reported cases). A larger series of CBT cases should be investigated to assess the diagnostic capabilities of the “central nonenhancement” sign on CT angiography for identifying the CBTs and differentiating them from other lesions in the carotid space.
Conclusion
CT angiography in three cases of CBTs shows this newly described sign of central nonenhancement that may be useful in identifying CBTs.
Conflict of Interest
None declared.
-
References
- 1 Muthoka JM, Hassanali J, Mandela P, Ogeng'o JA, Malek AA. Position and blood supply of the carotid body in a Kenyan population. Int J Morphol 2011; 29 (01) 65-69
- 2 Lin EP, Chin BB, Fishbein L. et al. Head and neck paragangliomas: an update on the molecular classification, state-of-the-art imaging, and management recommendations. Radiol Imaging Cancer 2022; 4 (03) e210088
- 3 Gad A, Sayed A, Elwan H. et al. Carotid body tumors: a review of 25 years experience in diagnosis and management of 56 tumors. Ann Vasc Dis 2014; 7 (03) 292-299
- 4 Hoang VT, Trinh CT, Lai TAK, Doan DT, Tran TTT. Carotid body tumor: a case report and literature review. J Radiol Case Rep 2019; 13 (08) 19-30
- 5 Shamblin WR, ReMine WH, Sheps SG, Harrison EG. Carotid body tumor (chemodectoma). Am J Surg 1971; 122 (06) 732-739
Address for correspondence
Publication History
Article published online:
15 December 2023
© 2023. Indian Radiological Association. This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/)
Thieme Medical and Scientific Publishers Pvt. Ltd.
A-12, 2nd Floor, Sector 2, Noida-201301 UP, India
-
References
- 1 Muthoka JM, Hassanali J, Mandela P, Ogeng'o JA, Malek AA. Position and blood supply of the carotid body in a Kenyan population. Int J Morphol 2011; 29 (01) 65-69
- 2 Lin EP, Chin BB, Fishbein L. et al. Head and neck paragangliomas: an update on the molecular classification, state-of-the-art imaging, and management recommendations. Radiol Imaging Cancer 2022; 4 (03) e210088
- 3 Gad A, Sayed A, Elwan H. et al. Carotid body tumors: a review of 25 years experience in diagnosis and management of 56 tumors. Ann Vasc Dis 2014; 7 (03) 292-299
- 4 Hoang VT, Trinh CT, Lai TAK, Doan DT, Tran TTT. Carotid body tumor: a case report and literature review. J Radiol Case Rep 2019; 13 (08) 19-30
- 5 Shamblin WR, ReMine WH, Sheps SG, Harrison EG. Carotid body tumor (chemodectoma). Am J Surg 1971; 122 (06) 732-739