
RSS-Feed abonnieren
DOI: 10.1055/s-0043-1777719
Radiographic Outcome in Supracondylar Humeral Fractures Gartland Type III
Artikel in mehreren Sprachen: español | English
Abstract
Objective This study evaluated Gartland Type 3 supracondylar humeral fracture features before and 3 months after surgical closed reduction.
Material and method Retrospective and observational medical records on 294 cases. We recorded age, gender, lesion mechanism, diagnosis, and classification according to the Gartland and Wilkins system. Radiological characteristics before and 3 months after surgery (Baumann angle, condyle-humeral angle, and rotation) were analyzed with t-Student and chi-square tests.
Results We identified 86 distal humerus fractures, including 75.8% supracondylar humeral fractures. The average age was 5.2 ± 2.8 years old (range, 1 to 14). Per the Garland classification, 45.3% of the fractures were type IIIB and 48.4% were type IIIA. According to Flynn's criteria, 98% had good or excellent outcomes. Postoperative complementary Baumann average angle was 12.8 ± 4.18° (t-Student: -1.94, p: 0.05), and the average condyle humeral angle was 46.9 ± 10.45 (t-Student: 10.68, p <0.001). Postoperative rotation persisted in six cases (chi-square <0.0001, p <0.001).
Discussion Our results are consistent with the international literature. We attributed the lower rate of neurologic lesions in comparison to other papers to lateral stabilization.
Conclusions Closed reduction and percutaneous pinning for treatment of supracondylar humeral fractures Gartland type III resulted in satisfactory outcomes.
Level of Evidence: IV
Introduction
Supracondylar humeral fractures are the second most common type of bone injury in children. The incidence of these fractures' ranges from 55% to 75% of all fractures in the elbow[1] and 3% of all pediatric fractures. The incidence by gender is similar due to the increased sports performance by girls. The peak incidence occurs from 5 to 6 years old. The annual incidence of these fractures is estimated at 177.3/100,000 children. These injuries have a seasonal distribution, with a higher frequency during the summer months. In addition, supracondylar humeral fractures are more common in the left elbow.[2]
Ninety-seven percent of humeral supracondylar fractures result from forces hyperextending the upper limb. In rare occasions, these injuries occur due to a strong direct impact on the posterior surface of the humerus with the elbow in flexion (3%).[3] In hyperextension-related injuries, the fracture line typically propagates through the center of the olecranon fossa, potentially displacing the distal fragment in a posterolateral or posteromedial direction.[4]
In extension fractures, the Gartland classification helps to describe injury severity and guides therapeutic management[5] [6] ([Table 1]).
|
I |
No displacement |
|
|
II |
Displacement > 2 mm with an intact posterior cortex |
|
|
III |
Displacement with no cortical contact |
|
|
III A |
Posteromedial displacement |
|
|
III B |
Posterolateral displacement |
|
|
IV |
Fractures with multidirectional instability, circumferential periosteal tear, and instability in flexion and extension. |
|
These injuries are potentially dangerous since the raw edge of the proximal fragment can damage vascular and nervous structures. Early complications include brachial artery injury (3.7% to 7%), nerve injuries (6% to 12%), and compartment syndrome. Late complications include valgus or varus axis deviations (6% to 16%) and elbow stiffness. Therefore, the ideal treatment for these lesions should occur within 12 hours, be exact, and be as least invasive as possible.[3]
Useful measurable angular relationships for humeral supracondylar fractures include the Baumann angle on the anteroposterior radiograph of the elbow and the anterior humeral line and condylar-humeral angle, among others, in lateral radiographs[2] [7] ([Fig. 1]).

Some treatment modalities for Gartland type III fractures ([Fig. 2]) include cast immobilization, traction, open reduction, and closed reduction with percutaneous pinning.[4] Different pin configurations have been described: two crossed pins, two lateral and one crossed pins, and pins on a single side (usually two or three).[2]

Vuillermin et al.[8] described the steps of closed reduction and percutaneous nailing. Abraham et al.[9] described the correction of varus or valgus alignment in their experimental report, and Ariño[10] reported fixation with two lateral pins. The reinforcement with a third wire described by Larsson[11] has been used in a standardized way by our study group per the following methodology.
Surgical Technique ([Fig. 3])

-
Patient placement in a supine position with the affected limb close to the fluoroscopic detector.
-
Reduction occurs as follows: a) Longitudinal traction with the elbow at 30° of flexion; b) Medial or lateral displacement correction through forced valgus or varus; c) Maintaining traction and with the elbow in flexion, pressure the olecranon (“ordering” maneuver) to correct the posterior displacement at the fracture site; d) Varus or valgus malalignment correction by forearm pronation or supination with the elbow at 90° of flexion according to the experimental study by Abraham et al.[9]
-
Reduction assessment using anteroposterior and lateral fluoroscopic views.[7]
-
Using the technique conceived by Ariño for fracture fixation[10] (lateral crossed wires), placement of two parallel Kirschner wires introduced through the lateral condyle, crossing the fracture, and anchored at the medial cortex. Occasionally, a third wire may increase stability, as described by Larson et al.[11]
-
Fixation stability checking by elbow mobilizing.
-
Wire cut and bending outside the skin; next, placement of a long splint with the elbow at 70° of flexion.[8]
-
Pin removal between the sixth and seventh postoperative week in our population (average observed union time), depending on the radiographic signs of consolidation, followed by elbow mobility.[8] ([Fig. 4])

Material and Methods
This study is a retrospective longitudinal analysis of medical records from patients with Gartland and Wilkins type III pediatric humeral supracondylar fractures from March 1, 2018, to June 30, 2018. We collected the following data: age, gender, mechanism of injury, diagnosis, classification, affected side, additional lesions, and pre- and postoperative (3 months) radiological features in the coronal and sagittal planes (fracture line, Baumann angle, condylar-humeral angle, displacement, rotation, and overriding). The study did not include open or pathological fractures.
The sampling technique was the convenience of consecutive cases.
Descriptive statistics included central tendency (mean, median, and mode for ungrouped quantitative variables), dispersion (standard deviation), and simple frequency measurements (percentages for qualitative variables).
For radiological variables in the coronal and sagittal planes before and 3 months after surgery (Baumann angle and condylar-humeral angle), the statistical analysis used the student's t-test and Pearson's chi-square (for rotation evaluation).
This study complies with the ethical standards regarding scientific research on human beings by the Nuremberg Declaration and its modifications. Similarly, it complies with the Regulations of the General Health Law on Health Research and institutional ethical standards. The study did not require an informed consent form since the information came from secondary sources.
The research team received no contributions from third parties or sponsorships.
Results
Between March 1, 2018, and June 30, 2018, 86 patients presented with distal humerus fractures, including 66 cases of humeral supracondylar fractures.
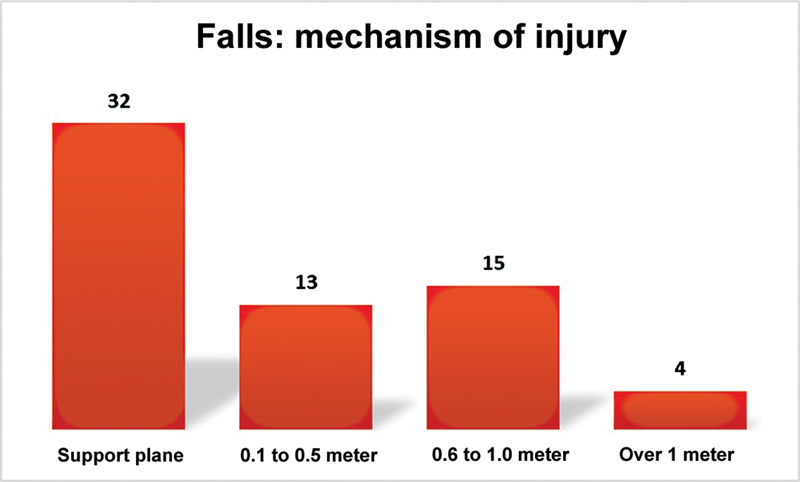
All injuries occurred after falls, including 50% (32 cases) from the patient's plane of support, 20.3% (13 cases) from a height ranging from 0.1 to 0.5 meter, 23.4% (15 cases) from a height ranging from 0.6 to 1 meter, and only 6.3% (four cases) from a height higher than 1 but lower than 2 meters ([Fig. 5]).
Supracondylar humeral fractures occurred in a male-to-female ratio of 2.8 to 1, with 73.4% males and 26.6% females. Fractures involved the right side in 26.6% of the cases and the left side in 73.4% ([Fig. 6]).

The mean age of the patients was 5.2 ± 2.8 years old, ranging from 1 to 14. Age distribution was as follows: 0 to 4 years old, 32.8%; 5 to 8 years old, 48.4%; 9 to 12 years old, 15.6%; and 13 years old or more, 3.1%. On average, males presented these injuries a year and a half later than females (5.7 years old for males versus 4 years old for females).
Per the Gartland and Wilkins classification, 45.3% of the cases had a posterolateral displacement (Group IIIB), 48.4% had a posteromedial displacement (Group IIIA), and four cases (6.3%) presented a pure posterior displacement ([Fig. 7]).

Regarding the clinical outcomes per the aesthetic Flynn scale, 78.1% had excellent results, and 2.9% presented good outcomes. In contrast, functionality was excellent in 65.6% of cases, good in 32.8%, and limited in a single case (with a 15° extension deficit).
As for radiographic characteristics according to the complementary Baumann angle, type III fractures presented a range of 5° to 18° (mean, 8.6° ± 6.75°) before surgery and a range of 5° to 15° (mean, 10° ± 5°) 3 months after surgery. The Student's t-test for the Baumann complementary angle revealed t = 0.70 and p = 0.5, potentially due to the limited number of cases. The preoperative humeral condylar angle ranged from 30° to 60° (mean, 48.2° ± 14.14°), and the postoperative humeral condylar angle ranged from 42° to 45° (mean, 45° ± 0°). The Student's t-test for the humeral condylar angle revealed t = 0.61 and p = 0.58. In contrast, there were no rotations before or 3 months after surgery.
The radiographic complementary Baumann angle in type IIIA fractures ranged from -20° to 60° (mean, 9.19° ± 17.52°) before surgery and 0° to 25° degrees (mean, 14.03° ± 4.3°) 3 months after surgery. The student's t-test for the Baumann complementary angle revealed t = 8.75 and p <0.0001. The humeral condylar angle ranged from 30° to 110° (mean, 77.75° ± 20.82°) before surgery and 40° to 80° (mean, 48° ± 9.8°) after surgery. The student's t-test for the humeral condylar angle revealed t = -1.47 and p = 0.15. On the other hand, 23 of 31 fractures presented preoperative rotations, of which only two persisted after the reduction (chi-square <0.0001, p <0.0001)
The radiographic complementary Baumann angle in type IIIB fractures ranged from 0° to 35° (mean, 12.07° ± 12.6°) before surgery and from 0° to 20° degrees (mean, 15° ± 3.4°) after surgery. The student's t-test for the Baumann complementary angle revealed t = 7.003 and p <0.0001. The humeral condylar angle ranged from 30° to 110° (mean, 74.5° ± 25°) before surgery and from 30° to 80° (mean, 47.75° ± 11.2°) after surgery. The student's t-test for the humeral condylar angle revealed t = -1.18 and p = 0.24. In contrast, 24 of 29 fractures presented preoperative rotations, of which four persisted after the reduction (chi-square <0.0001, p <0.0001).
All cases consolidated 6 weeks postoperatively.
There were no cases of intraoperatively conversion to open treatment.
Two patients presented a neuropraxia-type nerve injury (3%). One of them had an injury involving the median nerve, while the other one had a preoperative radial nerve injury and no further complications from the traumatic event. No complications occurred after surgical treatment.
Discussion
Closed reduction and percutaneous nailing, described by Swenson[12] and later popularized by Flynn et al., is a simple procedure with excellent outcomes[.13]
The Flynn criteria ([Tabla 2]) are probably the most frequently used tool to evaluate cosmetic and functional outcomes in patients with supracondylar humeral fractures. These criteria allow a clinical assessment to differentiate functional and cosmetic outcomes since some patients may have a large deformity and good function, and vice-versa.[13] Following Ducic et al., our group opts for closed reduction and percutaneous nailing as a treatment method due to the clinical outcomes obtained[.14] In addition, Kazimoglu et al. reported that closed reduction has similar clinical outcomes to open reduction[15] with no need for conversion to open surgical. These authors also reported good or excellent outcomes in more than 95% of the cases per the Flynn scale.
|
Outcome |
Cosmetic factor: Loss of carrying angle |
Functional factor: Loss of movement |
|---|---|---|
|
Excellent |
0°-5° |
0°-5° |
|
Good |
6°-10° |
6°-10° |
|
Regular |
11°-15° |
11°-15° |
|
Poor |
>15° |
>15° |
A meta-analysis from Guol et al. found that closed reduction and percutaneous fixation provide similar clinical outcomes to open treatment according to the Flynn criteria, with no statistically significant cosmetic and functional differences. Likewise, Guol et al. suggest that fixation with two lateral wires is an effective and reliable method to avoid iatrogenic ulnar nerve injury, warranting the selection of this fixation form by our department. The incidence of infection was 6.4% for closed reduction and percutaneous fixation and 7.1% for open reduction. However, there were no postoperative infections.[1]
Scaglione et al. evaluated 76 type III supracondylar fractures in patients aged 6 to 15, including 66 type IIIA and 10 type IIIB. Using the Flynn criteria for overall result evaluation, 101 patients (81%) did not have varus/valgus deformities. Valgus deformity occurred in seven subjects, and 17 patients presented varus deformities. Only two varus elbows presented a 15° deviation. No patients showed limitations in range of motion. The average Baumann angle was 16°. Considering these results, 80% were very good, 11% were good, 6% were borderline, and 3% were poor. There were no complications or conversions to open surgeries.[3]
Our functional outcomes are consistent with Kumar, who, in 1974, treated 192 Gartland grade II and 85 grade III fractures with closed reduction and percutaneous fixation with crossed pins. Kumar obtained 97.4% of good to excellent outcomes and 2.52% of poor or borderline outcomes. The poor and borderline outcomes were due to cosmetic factors, but the function was excellent. Six patients required a conversion to open surgery.[13] In our study, the only case with a borderline function was due to loss of extension at 15° degrees, which did not limit the functional life of the patient.
Barr reviewed 159 patients and found 97% of extension fractures, of which only 28 were Gartland type III. This author treated all cases with closed/open reduction and pin fixation. Six patients developed neurological injuries after the fracture compared to only two subjects in our study.[16]
In the Woratanarat meta-analysis, Sinikumpu et al. treated 16 fractures with closed reduction and percutaneous fixation with good or excellent outcomes according to the Flynn criteria.[17]
Farnsworth and Barr reported that up to 38% of fractures were due to falls from sports equipment such as handrails and trampolines and 16% from falls from furniture.[16] [18] This contrasts with our study, in which the most frequent mechanism was a fall from the patient's support plane, including 43.7% occurring from a height of up to one meter, i.e., the height of any domestic furniture. However, we did not record this data.
Conclusion
Closed reduction and percutaneous nailing provided satisfactory outcomes for treating Gartland type III pediatric supracondylar humeral fractures from a clinical, radiological, and aesthetic point of view within 3 months after surgery. The patients studied did not present immediate additional complications beyond those upon admission. Longer follow-up is required to evaluate long-term complications such as avascular necrosis, physeal damage, and angular deformity, among other factors.
Conflict of Interest
None.
-
Bibliografía
- 1 Lin-Guo, Xue-Ning Zhang, Jian-Ping Yang. , cols . A systematic review and meta-analysis of two different managements for supracondylar humeral fractures in children. J Orthop Surg Res 2018; 13 (141) 1-9 PubMed
- 2 Zorrilla S de Neira J, Prada-Cañizares A, Marti-Ciruelos R, Pretell-Mazzini J, Pretell-Mazzini J. Supracondylar humeral fractures in children: current concepts for management and prognosis. Int Orthop 2015; 39 (11) 2287-2296 (SICOT)
- 3 Scaglione M, Giovannelli D, Fabbri L, Dell'omo D, Goffi A, Guido G. Supracondylar humerus fractures in children treated with closed reduction and percutaneous pinning. Musculoskelet Surg 2012; 96 (02) 111-116
- 4 Edwardson SA, Murray O, Joseph J, Duncan R. Paediatric supracondylar fractures: an overview of current management and guide to open approaches. Orthop Trauma 2013; 27 (05) 303-311
- 5 Gartland JJ. Management of supracondylar fractures of the humerus in children. Surg Gynecol Obstet 1959; 109 (02) 145-154
- 6 Leitch KK, Kay RM, Femino JD, Tolo VT, Storer SK, Skaggs DL. Treatment of multidirectionally unstable supracondylar humeral fractures in children. A modified Gartland type-IV fracture. J Bone Joint Surg Am 2006; 88 (05) 980-985
- 7 Ladenhauf HN, Schaffert M, Bauer J. The displaced supracondylar humerus fracture: indications for surgery and surgical options: a 2014 update. Curr Opin Pediatr 2014; 26 (01) 64-69
- 8 Vuillermin C, May C, Kasser J. Closed Reduction and Percutaneous Pinning of Pediatric Supracondylar Humeral Fractures. Bone Joint Surg Am 2007; 89 (04) 706-712
- 9 Abraham E, Powers T, Witt P, Ray RD. Experimental hyperextension supracondylar fractures in monkeys. Clin Orthop Relat Res 1982; (171) 309-318
- 10 Ariño VL, Lluch EE, Ramirez AM, Ferrer J, Rodriguez L, Baixauli F. Percutaneous fixation of supracondylar fractures of the humerus in children. J Bone Joint Surg Am 1977; 59 (07) 914-916
- 11 Larson L, Firoozbakhsh K, Passarelli R, Bosch P. Biomechanical analysis of pinning techniques for pediatric supracondylar humerus fractures. J Pediatr Orthop 2006; 26 (05) 573-578
- 12 Swenson AL. The treatment of supracondylar fractures of the humerus by Kirschner-wire transfixion. J Bone Joint Surg Am 1948; 30A (04) 993-997
- 13 Flynn JC, Matthews JG, Benoit RL. Blind pinning of displaced supracondylar fractures of the humerus in children. Sixteen years' experience with long-term follow-up. J Bone Joint Surg Am 1974; 56 (02) 263-272
- 14 Ducić S, Bumbasirević M, Radlović V. et al. Displaced supracondylar humeral fractures in children: Comparison of three treatment approaches. Srp Arh Celok Lek 2016; 144 (1-2) 46-51
- 15 Kazimoglu C, Cetin M, Sener M, Aguş H, Kalanderer O. Operative management of type III extension supracondylar fractures in children. Int Orthop 2009; 33 (04) 1089-1094
- 16 Barr LV. Paediatric supracondylar humeral fractures: epidemiology, mechanisms and incidence during school holidays. J Child Orthop 2014; 8 (02) 167-170
- 17 Woratanarat P, Angsanuntsukh C, Rattanasiri S, Attia J, Woratanarat T, Thakkinstian A. Meta-analysis of pinning in supracondylar fracture of the humerus in children. J Orthop Trauma 2012; 26 (01) 48-53
- 18 Farnsworth CL, Silva PD, Mubarak SJ. Etiology of supracondylar humerus fractures. J Pediatr Orthop 1998; 18 (01) 38-42
Address for correspondence
Publikationsverlauf
Eingereicht: 25. August 2021
Angenommen: 27. November 2023
Artikel online veröffentlicht:
26. Dezember 2023
© 2023. Sociedad Chilena de Ortopedia y Traumatologia. This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/)
Thieme Revinter Publicações Ltda.
Rua do Matoso 170, Rio de Janeiro, RJ, CEP 20270-135, Brazil
-
Bibliografía
- 1 Lin-Guo, Xue-Ning Zhang, Jian-Ping Yang. , cols . A systematic review and meta-analysis of two different managements for supracondylar humeral fractures in children. J Orthop Surg Res 2018; 13 (141) 1-9 PubMed
- 2 Zorrilla S de Neira J, Prada-Cañizares A, Marti-Ciruelos R, Pretell-Mazzini J, Pretell-Mazzini J. Supracondylar humeral fractures in children: current concepts for management and prognosis. Int Orthop 2015; 39 (11) 2287-2296 (SICOT)
- 3 Scaglione M, Giovannelli D, Fabbri L, Dell'omo D, Goffi A, Guido G. Supracondylar humerus fractures in children treated with closed reduction and percutaneous pinning. Musculoskelet Surg 2012; 96 (02) 111-116
- 4 Edwardson SA, Murray O, Joseph J, Duncan R. Paediatric supracondylar fractures: an overview of current management and guide to open approaches. Orthop Trauma 2013; 27 (05) 303-311
- 5 Gartland JJ. Management of supracondylar fractures of the humerus in children. Surg Gynecol Obstet 1959; 109 (02) 145-154
- 6 Leitch KK, Kay RM, Femino JD, Tolo VT, Storer SK, Skaggs DL. Treatment of multidirectionally unstable supracondylar humeral fractures in children. A modified Gartland type-IV fracture. J Bone Joint Surg Am 2006; 88 (05) 980-985
- 7 Ladenhauf HN, Schaffert M, Bauer J. The displaced supracondylar humerus fracture: indications for surgery and surgical options: a 2014 update. Curr Opin Pediatr 2014; 26 (01) 64-69
- 8 Vuillermin C, May C, Kasser J. Closed Reduction and Percutaneous Pinning of Pediatric Supracondylar Humeral Fractures. Bone Joint Surg Am 2007; 89 (04) 706-712
- 9 Abraham E, Powers T, Witt P, Ray RD. Experimental hyperextension supracondylar fractures in monkeys. Clin Orthop Relat Res 1982; (171) 309-318
- 10 Ariño VL, Lluch EE, Ramirez AM, Ferrer J, Rodriguez L, Baixauli F. Percutaneous fixation of supracondylar fractures of the humerus in children. J Bone Joint Surg Am 1977; 59 (07) 914-916
- 11 Larson L, Firoozbakhsh K, Passarelli R, Bosch P. Biomechanical analysis of pinning techniques for pediatric supracondylar humerus fractures. J Pediatr Orthop 2006; 26 (05) 573-578
- 12 Swenson AL. The treatment of supracondylar fractures of the humerus by Kirschner-wire transfixion. J Bone Joint Surg Am 1948; 30A (04) 993-997
- 13 Flynn JC, Matthews JG, Benoit RL. Blind pinning of displaced supracondylar fractures of the humerus in children. Sixteen years' experience with long-term follow-up. J Bone Joint Surg Am 1974; 56 (02) 263-272
- 14 Ducić S, Bumbasirević M, Radlović V. et al. Displaced supracondylar humeral fractures in children: Comparison of three treatment approaches. Srp Arh Celok Lek 2016; 144 (1-2) 46-51
- 15 Kazimoglu C, Cetin M, Sener M, Aguş H, Kalanderer O. Operative management of type III extension supracondylar fractures in children. Int Orthop 2009; 33 (04) 1089-1094
- 16 Barr LV. Paediatric supracondylar humeral fractures: epidemiology, mechanisms and incidence during school holidays. J Child Orthop 2014; 8 (02) 167-170
- 17 Woratanarat P, Angsanuntsukh C, Rattanasiri S, Attia J, Woratanarat T, Thakkinstian A. Meta-analysis of pinning in supracondylar fracture of the humerus in children. J Orthop Trauma 2012; 26 (01) 48-53
- 18 Farnsworth CL, Silva PD, Mubarak SJ. Etiology of supracondylar humerus fractures. J Pediatr Orthop 1998; 18 (01) 38-42






