
Subscribe to RSS
DOI: 10.1055/s-0043-1777824
Tibial Fracture Secondary to Anterior Tibial Tubercle Osteotomy: Report of Three Cases and Literature Review
Article in several languages: español | English
Abstract
There are multiple treatment options for the broad spectrum of patellofemoral conditions. The most common conditions are patellofemoral instability and osteoarthritis. Several treatment modalities have been described for these conditions, and distal realignment procedures are especially relevant. Although these techniques are effective in most cases, they are not free of problems, reported in up to one-third of cases.
This article presents three cases undergoing an anterior tibial tubercle osteotomy as a therapeutic tool for two distinct conditions. All cases had a tibial fracture in the osteotomy site, an uncommon complication with potential severe prognostic consequences.
#
Introduction
First described in 1938, osteotomy (OTT) of the anterior tibial tubercle (ATT) is a surgical technique realigning the tibial tubercle to redistribute the force vectors acting on the extensor apparatus.[1]
In most cases, it is the technique of choice for patients with patellofemoral instability due to an excessive lateral position of the ATT to the force vector coming from the quadriceps (tibial tubercle-trochlear groove [TT-TG] distance >20 mm),[2] mainly by medializing the tubercle. The second scenario, also quite common, occurs in patients with chondral lesions or patellofemoral osteoarthritis, in which ATT osteotomy is considered in the presence of pain, effusion, and/or mechanical symptoms after attempting appropriate conservative treatment. It is also important to mention the role of patellar height in the management algorithm of these conditions, often indicating a tubercle decrease when the patella is high, mainly in the instabilities. Tibial osteotomies can transfer the tubercle medially, distally, and/or anteriorly according to the patient's symptoms and bony anatomy.[2]
The most used techniques include anteromedialization (Fulkerson) for medial and anterior translation of the force vector of the extensor apparatus. Pure anteriorization (Maquet) involves the anterior translation of the tubercle to reduce pressure on the patellofemoral joint. Distalization procedures are usually combined with anteromedialization and pure anteriorization. In pure medialization (Elmslie Trillat), the medialization of the force vector of the extensor apparatus is carried out medially.
Complications of TTOs can be major or minor. Major complications reported in the literature include deep vein thrombosis (DVT), tibial fractures, nonunions, common peroneal nerve neuropraxia, deep infection, arthrofibrosis, and recurrent patellar instability. Minor complications include superficial infection, hypertrophic scar, surgical site pain, osteosynthesis material-related discomfort, and hematomas.[3] [4]
The recent literature reported complication rates ranging from 0% to 12%. However, cohort sizes limited these studies since the largest number of patients was 116 knees.[5] A systematic review from 2017 analyzed 21 studies (1,055 knees) and assessed outcomes from tibial osteotomies. This review found an overall complication rate of 8%. In addition, 21% of the patients required a second surgery for symptomatic osteosynthesis.[6] A recent publication from Dr. Arendt evaluating 150 patients undergoing ATT osteotomy reported major complications in 21.5% of cases and minor complications in 8%.[7] It is worth mentioning that these percentages are highly variable in the literature because of the lack of a clear objective definition of complications in ATT OTTs.
Tibial fracture at the osteotomy level is a rare complication with devastating consequences. For this reason, we present four fractures in three different patients with this complication, including three resolved with reduction plus fracture osteosynthesis and one conservatively treated fracture, all progressing satisfactorily.
#
Case Report
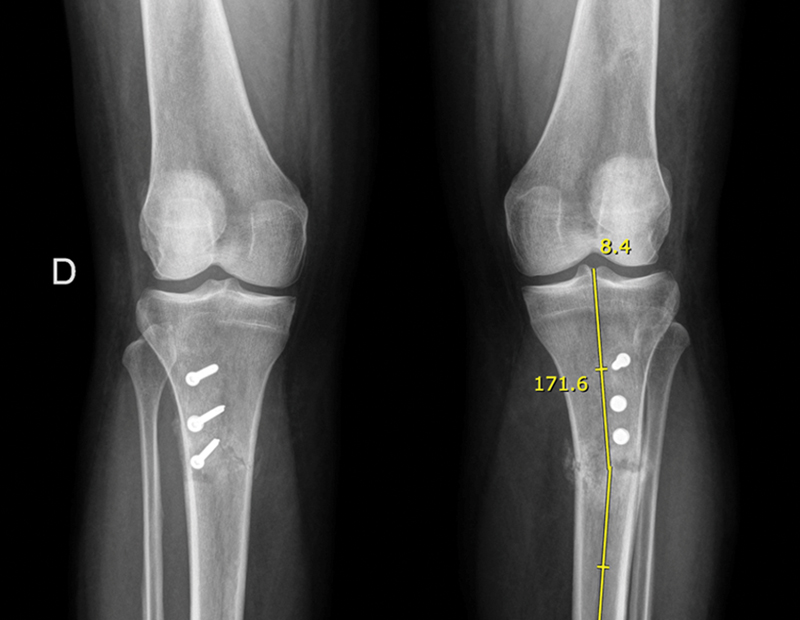
The first case was a 41-year-old female patient with a history of depression and anxiety attacks whose main complaint was disabling bilateral back pain, worse when going up and down stairs, which recently had limited her daily activities. Studies included bilateral magnetic resonance imaging (MRI) revealing grade II and III chondral lesions in the lateral facets of both patellae, with TT-TG of 20 mm on the right knee and 23 mm on the left knee. Initially, management was conservative, with kinetic therapy and analgesics. Since it was unsuccessful, we decided on an ATT medialization osteotomy (Elmslie Trillat), technically planning a tubercle bone block 5 cm long by 1 cm wide. This block underwent careful, progressive osteotomy with chisels in a latero-medial direction. The weakening of the distal hinge of the block used a 2.5-mm drill bit with multiple perforations in an anteroposterior direction. Fixation used three 3.5-mm diameter screws (two cortical and one cancellous screw) in an anteroposterior direction. In addition, we performed an arthroscopic chondroplasty of the chondral lesions ([Fig. 1]). Initially, the patient progressed favorably. However, she came back six weeks after surgery due to acute pain in both knees associated with sudden involuntary lifting movements while she was moving around her home. At that time, radiographs showed a bilateral tibial fracture at the osteotomy site ([Fig. 2]). At first, the fracture management was conservative, with unloading and immobilization for six weeks. This treatment was successful for the right lower extremity but not the left leg, with a progressive varus deviation requiring active surgical management through reduction and osteosynthesis with a lateral locking plate of the proximal tibia added to biological support. The retrospective analysis of the case revealed hypovitaminosis D before surgery (15.9 ng/mL; the normal value is > 20 ng/mL).

Subsequently, the patient achieved adequate recovery and consolidation of both fractures, returning to her normal activities of daily living without residual symptoms ([Fig. 3]).

The second case is a healthy 18-year-old patient with recurrent bilateral patellar instability. Initially, instability management was conservative, but it progressed with the persistence of symptoms. The most striking clinical elements included marked apprehension, patellofemoral pain, and frank hypermobility with a positive “J” sign. An imaging study revealed a TT-TG distance of 25 mm on the right knee and 23 mm on the left knee, leading to the decision to perform a medial patellofemoral ligament reconstruction surgery with allograft plus a bilateral Elmslie Trillat osteotomy. Each knee underwent a 10-mm medialization, with a tubercle bone block approximately 5 cm long and 1 cm wide. The block was progressively prepared with chisels in a latero-medial direction after flexing the distal hinge and multiple perforations in an anteroposterior direction with a 2.5-mm diameter drill bit. Osteotomy fixation used three screws of 3.5 mm in diameter, of which the two most distal were fully threaded cortical screws, and the most proximal was a cancellous screw ([Fig. 4]). The patient's progression was satisfactory until the 8th month when he had trauma and torsion at the right knee while playing soccer. The radiograph showed a tibial fracture at the osteotomy site ([Fig. 5]) requiring surgical management with fracture reduction and osteosynthesis with a 4.5-mm lateral proximal tibial locked plate, with good progression ([Fig. 6]).



The third case was a 14-year-old female patient with a history of genu valgus, medial femoral hemiepiphysiodesis surgery at 12 years old, and recurrent bilateral patella dislocation. She presented with persistent patellar instability and new episodes of dislocations in the right knee. Magnetic resonance imaging, radiographs, and computed tomography scans highlighted a high patella with a Caton Deschamps index of 1.44, a high-grade trochlear dysplasia (B according to Dejour), and a TT-TG distance of 22 mm ([Fig. 7]). In this context and considering the skeletal maturity, we decided to perform an ATT descent and medialization, with a complete osteotomy of approximately 5 cm and a net section at the distal level added to bone subtraction to achieve a 1-cm distalization and a 10-mm medialization. The same surgery reconstructed the medial patellofemoral ligament with a gracilis autograft. The patient progressed satisfactorily until the fourth week, with a full range of motion and no pain. She independently decided not to use the canes, and, in a sudden movement when standing up from a chair, she experienced intense pain and proximal tibial deformity. She went to the emergency department, and the examination revealed a tibial fracture at the osteotomy site ([Fig. 8]). Next, the patient underwent surgery for fracture reduction and osteosynthesis with a 4.5-mm lateral proximal tibia plate. The procedure was successful, with advanced consolidation in the third postoperative month ([Fig. 9]).



#
Discussion and Literature Review
Anterior tibial tubercle osteotomy is a common surgical procedure in orthopedic practice to treat several patellofemoral joint conditions. The consolidation process at the osteotomy site is a crucial factor for the success of this procedure. This consolidation can be affected by patient factors (age, comorbidities, smoking) and surgical issues (osteotomy depth, fixation method, and osteotomy type). The first case had hypovitaminosis D (15.9 ng/mL versus >20 ng/mL as a normal value) and an undertreated psychological condition that hindered the patient's compliance with postoperative treatment. These factors are potentially relevant when considering a surgical approach, especially bilateral.
Tibial fractures at the osteotomy site are part of the major complications of this technique. Stetson et al. conducted an exhaustive study reporting an incidence of tibial fracture of 2.6% (6/234 knees), all in the first 13 weeks post-surgery.[8] It is worth noting that all fractures occurred after a phase transition from partial to full support. Five of the six fractures consolidated with conservative management in a good axis, as occurred in one of the fractures in the first reported case. Of the six tibial fractures, two fractures began near the screw fixation site, two at the proximal osteotomy site, and two at the distal osteotomy site.[8] Payne et al. described eight postoperative tibial fractures in 787 patients (1%). Six of these patients underwent conservative treatment, while the remaining two underwent successful open reduction and internal fixation.[9] We can deduce that most cases consist of non-displaced fractures, which tend to consolidate well with conservative treatment. In contrast, given the need to consider a surgical approach, since most of our cases were successful, reduction and fixation with a robust lateral plate seem to be the best therapeutic alternative.
The distal osteotomy section appears to be a key factor in tibial fractures. Bellemans et al. reported four proximal tibia fractures in 53 Fulkerson osteotomies (7.5%), all of which occurred from the fourth to seventh week after surgery.[10] The risk of complications is higher when the osteotomy involves complete separation of the tibial tubercle (10.7%), in contrast to attempts to spare the distal cortical hinge, as in the Elmslie-Trillat (3.3%) and Fulkerson (3.7%) osteotomies.[9] We usually try to preserve the distal cortex of the osteotomy, only performing multiple perforations with a 2.5-mm drill bit to make it more flexible ([Fig. 10]), This increases the elasticity, facilitating the medialization of the bone fragment. This gesture is not feasible in cases like our last patient, which required a tibial tubercle distalization to achieve an adequate patellar height, increasing the risk of major complications such as nonunions or tibial fractures.

The surgical technique should aim to create an osteotomy involving cancellous bone to avoid the creation of a completely cortical bone fragment, optimizing bone consolidation, and minimizing the possibility of tibial tubercle fragment fracture. Avoid creating an osteotomized fragment too thin (less than 8 mm) due to the increased risk of nonunion and delayed union.[11]
Theoretically, 3.5-mm screws could produce less anterior soft tissue irritation due to their lower profile compared to 4.5-mm screws. Previous studies reporting screw sizes and the percentage of cases requiring osteosynthesis material removal support this point. These studies suggest that removal of 3.5-mm screws occurs in 16% of cases, 4.0-mm screws in 30% of cases, and 4.5-mm screws in 52% of cases.[1] The removal of 6.5-mm screws is usually planned from the beginning given its larger size.[12] Regarding the configuration and direction of the screws, Aykanat et al. carried out interesting biomechanical studies and concluded that the most stable configuration was with two screws, with the most proximal perpendicular to the osteotomy plane and the most distal perpendicular to the posterior tibial cortex.[13] It has been recommended that osteotomy fixation screws be at least 2 mm longer than the measured bicortical distance to ensure adequate fixation.[11] In our cases, we always used three 3.5-mm screws from different types, including cortical, cancellous, or partially threaded screws. This configuration offers adequate stability and fewer symptoms because the screws present a low profile.
As mentioned above, most fractures associated with these procedures are non-displaced fractures, which evolve satisfactorily with good conservative treatment (including load limitation for at least 8 weeks and serial careful rehabilitation). For surgical treatment, the suggestion is to use traumatology criteria influenced by factors like displacement, axis, rotation, and progression over time of each case.
Postoperative rehabilitation is crucial to ensure successful consolidation and minimize the risk of complications. This field has different protocols, often performed at the surgeon's discretion. It has been suggested that patients work in their passive range of motion with the limb unloaded during the first 6 to 8 weeks after surgery.[14] However, other authors allow progressive simulated partial loading. High-impact activities should be avoided for an average of 6 months, while return to competitive sports should wait from 9 months to 1 year after surgery.[14] From our cases, the first had complications during the first weeks due to involuntary limb loading of the limb, similar to the third case. On the other hand, our male patient prematurely resumed participating in impact sports activities without medical authorization. Specifically, he returned to playing soccer, a contact sport with a high risk of injury, especially during the first year after anterior tibial tubercle osteotomy.
#
Conclusions
Tibial tubercle osteotomy is a valuable surgical technique to address patellofemoral joint conditions. Surgical planning requires proper consideration of several factors to ensure optimal results. Elements such as patient characteristics, surgical technique, and postoperative care significantly influence union and the risk of potential complications, including postoperative fractures. Traumatologists must carefully evaluate these factors and tailor their approach to each patient to achieve successful outcomes while minimizing potential complications. A multidisciplinary approach and a good doctor-patient relationship are key to delivering information in a specific way, thereby avoiding potentially risky behaviors by our patients.
The three reported cases are unusual presentations of knee surgery complications. It is critical to consider how to prevent and manage these types of complications since they can have devastating consequences on the quality of life of our patients.
#
#
Conflict of Interest
None.
-
Bibliografía
- 1 Johnson AA, Cosgarea AJ, Wolfe EL. Complications of tibial tuberosity osteotomy. Sports Med Arthrosc Rev 2017; 25 (02) 85-91
- 2 Middleton KK, Gruber S, Shubin Stein BE. Why and where to move the tibial tubercle: indications and techniques for tibial tubercle osteotomy. Sports Med Arthrosc Rev 2019; 27 (04) 154-160
- 3 Longo UG, Rizzello G, Ciuffreda M. et al. Elmslie- Trillat, Maquet, Fulkerson, Roux Goldthwait, and other distal realignment procedures for the management of patellar dislocation: systematic review and quantitative synthesis of the literature. Arthroscopy 2016; 32 (05) 929-943
- 4 Dantas P, Nunes C, Moreira J, Amaral LB. Antero-medialisation of the tibial tubercle for patellar instability. Int Orthop 2005; 29 (06) 390-391
- 5 Johnson AA, Wolfe EL, Mintz DN, Demehri S, Shubin Stein BE, Cosgarea AJ. Complications after tibial tuberosity osteotomy: association with screw size and concomitant distalization. Orthop J Sports Med 2018; 6 (10) 2325967118803614
- 6 Saltzman BM, Rao A, Erickson BJ. et al. A Systematic review of 21 tibial tubercle osteotomy studies and more than 1000 knees: indications, clinical outcomes, complications, and reoperations. Am J Orthop 2017; 46 (06) E396-E407
- 7 Lundeen A, Macalena J, Agel J, Arendt E. High incidence of complication following tibial tubercle surgery. J ISAKOS 2023; 8 (02) 81-85
- 8 Stetson WB, Friedman MJ, Fulkerson JP, Cheng M, Buuck D. Fracture of the proximal tibia with immediate weightbearing after a Fulkerson osteotomy. Am J Sports Med 1997; 25 (04) 570-574
- 9 Payne J, Rimmke N, Schmitt LC, Flanigan DC, Magnussen RA. The incidence of complications of tibial tubercle osteotomy: A systematic review. Arthroscopy 2015; 31 (09) 1819-1825
- 10 Bellemans J, Cauwenberghs F, Brys P, Victor J, Fabry G. Fracture of the proximal tibia after Fulkerson anteromedial tibial tubercle transfer. A report of four cases. Am J Sports Med 1998; 26 (02) 300-302
- 11 Servien E, Archbold P. Episodic patellar dislocation. In: Neyret P, Demey G. eds. Surgery of the knee. London: Springer; 2014: 305-326
- 12 Endres S, Wilke A. A 10 year follow-up study after Roux-Elmslie-Trillat treatment for cases of patellar instability. BMC Musculoskelet Disord 2011; 12: 48
- 13 Aykanat F, Kose O, Guneri B. et al. Comparison of four different screw configurations for the fixation of Fulkerson osteotomy: a finite element analysis. J Orthop Traumatol 2023; 24 (01) 30
- 14 Harrison RK, Magnussen RA, Flanigan DC. Avoiding complications in patellofemoral surgery. Sports Med Arthrosc Rev 2013; 21 (02) 121-128
Address for correspondence
Publication History
Received: 27 September 2023
Accepted: 30 November 2023
Article published online:
26 December 2023
© 2023. Sociedad Chilena de Ortopedia y Traumatologia. This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/)
Thieme Revinter Publicações Ltda.
Rua do Matoso 170, Rio de Janeiro, RJ, CEP 20270-135, Brazil
-
Bibliografía
- 1 Johnson AA, Cosgarea AJ, Wolfe EL. Complications of tibial tuberosity osteotomy. Sports Med Arthrosc Rev 2017; 25 (02) 85-91
- 2 Middleton KK, Gruber S, Shubin Stein BE. Why and where to move the tibial tubercle: indications and techniques for tibial tubercle osteotomy. Sports Med Arthrosc Rev 2019; 27 (04) 154-160
- 3 Longo UG, Rizzello G, Ciuffreda M. et al. Elmslie- Trillat, Maquet, Fulkerson, Roux Goldthwait, and other distal realignment procedures for the management of patellar dislocation: systematic review and quantitative synthesis of the literature. Arthroscopy 2016; 32 (05) 929-943
- 4 Dantas P, Nunes C, Moreira J, Amaral LB. Antero-medialisation of the tibial tubercle for patellar instability. Int Orthop 2005; 29 (06) 390-391
- 5 Johnson AA, Wolfe EL, Mintz DN, Demehri S, Shubin Stein BE, Cosgarea AJ. Complications after tibial tuberosity osteotomy: association with screw size and concomitant distalization. Orthop J Sports Med 2018; 6 (10) 2325967118803614
- 6 Saltzman BM, Rao A, Erickson BJ. et al. A Systematic review of 21 tibial tubercle osteotomy studies and more than 1000 knees: indications, clinical outcomes, complications, and reoperations. Am J Orthop 2017; 46 (06) E396-E407
- 7 Lundeen A, Macalena J, Agel J, Arendt E. High incidence of complication following tibial tubercle surgery. J ISAKOS 2023; 8 (02) 81-85
- 8 Stetson WB, Friedman MJ, Fulkerson JP, Cheng M, Buuck D. Fracture of the proximal tibia with immediate weightbearing after a Fulkerson osteotomy. Am J Sports Med 1997; 25 (04) 570-574
- 9 Payne J, Rimmke N, Schmitt LC, Flanigan DC, Magnussen RA. The incidence of complications of tibial tubercle osteotomy: A systematic review. Arthroscopy 2015; 31 (09) 1819-1825
- 10 Bellemans J, Cauwenberghs F, Brys P, Victor J, Fabry G. Fracture of the proximal tibia after Fulkerson anteromedial tibial tubercle transfer. A report of four cases. Am J Sports Med 1998; 26 (02) 300-302
- 11 Servien E, Archbold P. Episodic patellar dislocation. In: Neyret P, Demey G. eds. Surgery of the knee. London: Springer; 2014: 305-326
- 12 Endres S, Wilke A. A 10 year follow-up study after Roux-Elmslie-Trillat treatment for cases of patellar instability. BMC Musculoskelet Disord 2011; 12: 48
- 13 Aykanat F, Kose O, Guneri B. et al. Comparison of four different screw configurations for the fixation of Fulkerson osteotomy: a finite element analysis. J Orthop Traumatol 2023; 24 (01) 30
- 14 Harrison RK, Magnussen RA, Flanigan DC. Avoiding complications in patellofemoral surgery. Sports Med Arthrosc Rev 2013; 21 (02) 121-128









