
RSS-Feed abonnieren
DOI: 10.1055/s-0043-57228
Cardiac Surgery 2022 Reviewed
Funding None.
- Abstract
- Introduction
- Methods
- Surgical Treatment of Coronary Artery Disease
- Surgical Treatment of Valve Disease
- Glimpse into Surgery of the Aorta and for Terminal Heart Failure
- References
Abstract
PubMed displayed almost 37,000 hits for the search term “cardiac surgery AND 2022.” As before, we used the PRISMA approach and selected relevant publications for a results-oriented summary. We focused on coronary and conventional valve surgery, their overlap with interventional alternatives, and briefly assessed surgery for aorta or terminal heart failure. In the field of coronary artery disease (CAD), key manuscripts addressed prognostic implications of invasive treatment options, classically compared modern interventions (percutaneous coronary intervention [PCI]) with surgery (coronary artery bypass grafting [CABG]), and addressed technical aspects of CABG. The general direction in 2022 confirms the superiority of CABG over PCI in patients with anatomically complex chronic CAD and supports an infarct-preventative effect as underlying mechanism. In addition, the relevance of proper surgical technique to achieve durable graft patency and the need for optimal medical treatment in CABG patients was impressively illustrated. In structural heart disease, the comparisons of interventional and surgical techniques have been characterized by prognostic and mechanistic investigations underscoring the need for durable treatment effects and reductions of valve-related complications. Early surgery for most valve pathologies appears to provide significant survival advantages, and two publications on the Ross operation prototypically illustrate an inverse association between long-term survival and valve-related complications. For surgical treatment of heart failure, the first xenotransplantation was certainly dominant, and in the aortic surgery field, innovations in arch surgery prevailed. This article summarizes publications perceived as important by us. It cannot be complete nor free of individual interpretation, but provides up-to-date information for decision-making and patient information.
Introduction
For almost a decade, we have prepared these reviews of the surgical literature. As with every repeating process, changes in content and style occur. While we believe that the mere summary of selected publications that we presented in the beginnings may be outdated, we began to apply a mechanistic perspective wherever possible, asking how individual data may fit into a common and plausible concept. Such an activity has generated the concept of surgical collateralization, for instance, which solved many contradictions in publications on coronary artery disease (CAD) treatment. We have subsequently tried to apply this principle also to the other areas of this review. We hope the reader appreciates our efforts, which are strictly adherent to the common principle that everyone is entitled to his or her own opinion, but not to his or her own facts. In other words, readers may not agree with our interpretation of the data, but they can rest assured that the quoted data and associations are accurate.
Methods
We used the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) approach for a systematic literature review. The MEDLINE database was searched using the following search terms combined with the publication date being between January 1 and December 28, 2022, for the different chapters of this manuscript: Coronary Artery Bypass Grafting; Aortic Valve; TAVI; Aortic Valve Disease; Mitral Valve Surgery; MitraClip; TEER; Tricuspid Valve; Aortic Aneurysm; Aortic dissection; LVAD; Mechanical Circulatory Support and Heart Transplantation; Clinical Trial. [Supplementary Fig. S1] (available in the online version only) shows the PRISMA diagram for the literature review. We selected publications based on their value for indications, decision-making, and patient information. Manuscripts with focus on individual technical details without relevant information for the above-described goals were omitted.
Surgical Treatment of Coronary Artery Disease
The ISCHEMIA trial (showing no survival impact of an invasive diagnostic and treatment approach for symptomatic patients with inducible ischemia on medical therapy) and the recent REVIVED trial (showing no survival impact for percutaneous coronary intervention [PCI] compared with medical therapy in patients with ischemic heart failure and inducible ischemia) brought up concern about the prognostic impact of invasive CAD treatment for chronic coronary syndrome. Since a small fraction of patients in the invasive arm of ISCHEMIA were treated with coronary artery bypass grafting (CABG), this concern (that primarily affects PCI) is currently also applied to CABG.[1] Summarizing PCI and CABG under the term “revascularization” is not helpful in this context. We have specifically addressed this issue in 2021[2] and 2022[3] and concluded that the term revascularization is scientifically inappropriate and for patients misleading ([Fig. 1A]). The literature in 2022 impressively underscores the individual ability of CABG (but not PCI) to prolong life in patients with appropriate indications (i.e., with anatomically complex CAD).

An important publication in this context is the meta-analysis of Gaudino et al,[4] who demonstrate a significant survival advantage of CABG over medical therapy assessing all randomized controlled trials (total of 2,523 patients) where CABG and PCI was compared, and patients received at least aspirin, statins, and β-blockers ([Fig. 1B]). The previous demonstration of this effect was from the 1990s and was heavily criticized because of the outdated medical therapy in the more than 30-year-old trials. Gaudino et al now repeat the findings with patients from trials using contemporary medical therapy. It is interesting that medical and surgical therapy have been complementary throughout the years, which is also visible in 2022. Heer et al, for instance, demonstrated in patients from the “Ticagrelor in CABG” trial that optimal medical therapy after CABG reduces mortality and adverse events significantly.[5] Furthermore, an individual patient data meta-analysis of four trials shows the addition of ticagrelor to the medication of post-CABG patients improves patency rates of bypass grafts (although at the cost of more bleeding events[6]). These findings are all consistent with the infarct-preventative effect of both CABG (by surgical collateralization) and medical therapy (primarily by inhibiting thrombus formation and slowing CAD progression[3]).
These mechanistic considerations may also explain all presumably conflicting publications in 2022. Senior et al[7] assessed the Ischemia trial population for the ability to detect left main disease. They found that stress testing was not well suited to detect the presence of significant left main CAD and that anatomic imaging is required. Ono et al[8] reported no influence of the presence of a proximal left anterior descending artery lesion for the selection of PCI or CABG in the SYNTAXES patient population, and Ninomiya et al[9] showed that CABG is better than PCI if bifurcation lesions are present. These and other data may appear contradictory. However, seen through the mechanistic lenses of surgical collateralization and infarct prevention ([Fig. 1A]), it is not the individual lesion that causes CABG and PCI to differ in their effect, but the general risk of coronary events. If high, CABG is superior, and if low, PCI is noninferior.[10] However, it is important to underscore that this suggested mechanism is a hypothesis that has not been and cannot be fully proven, but the available evidence is in impressive support of its value.
Both the individual patient data meta-analysis of all CABG versus PCI trials in chronic coronary syndrome[11] and the newer FAME 3 trial (reviewed in detail last year)[12] speak for CABG in more complex CAD. Since randomized trials reflect the average treatment effects for an often-selected patient population, we reasoned that risk-adjusted registry data are likely to reflect the actual treatment effect for most patients in a specific region. We therefore systematically searched the literature for registry studies comparing CABG and PCI in chronic CAD in which the region can be identified.[13] We found 22 studies, of which 19 were propensity risk–adjusted, from around the world. The great majority of these studies (74%) demonstrated a significant advantage in long-term mortality and major adverse cardiovascular event for CABG over PCI. There was a weighted actual mortality difference of almost 6% in the CABG group in the long-term follow-up. We also found a piece of information that appears very relevant for patient counseling. Mortality after 30 days in those all-comers registry analyses was not different after CABG or PCI (1.68 vs 1.54%). Values were somewhat higher than in previous publications from randomized trials, but the general finding was identical to the randomized trials.[14] A real-world examination of invasive treatment strategies in patients from Ontario, Canada, with left main disease treated with PCI or CABG between 2008 and 2020 supports this finding in 1,128 propensity-matched pairs. In-hospital mortality was 3.7% in PCI and 3.8% in CABG patients (p = 0.91) and survival at 7 years was significantly better with CABG ([Fig. 1C]).[15] Thus, based on the currently available evidence, one may state that CABG is certainly more invasive than PCI, but for the treatment of chronic coronary syndromes it appears not to be more dangerous with respect to mortality.
The comparative investigations of CABG and PCI in 2022 presented again some studies suggesting equal outcomes between PCI and CABG, specifically with non-ST elevation myocardial infarction.[16] Our global review and the most recently appearing publications, however, broadly support superiority of CABG over PCI in properly selected patients. For instance, an Israeli analysis comparing CABG and PCI in patients with acute coronary syndrome demonstrated in 2022 survival advantages for CABG in diabetic patients[17] ([Fig. 1C]). A Canadian analysis of all patients undergoing CABG or PCI for multivessel disease in Ontario shows a survival advantage for CABG, if multiple grafts were placed[18] ([Fig. 1C]). Tasoudis et al performed a meta-analysis of CABG versus PCI studies in dialysis patients and also demonstrated a long-term-survival advantage for CABG, although this advantage was associated with higher periprocedural mortality.[19] Finally, a single-center retrospective analysis on patients with complete total occlusions receiving CABG or PCI also demonstrated better survival with CABG.[20]
Since this repeated superiority of CABG is mostly visible in registry-type data, significant biases are likely. However, the overwhelming number of publications pro-CABG and the lack of data demonstrating superiority of PCI make the need for shared decision-making on a broad scale very important for optimal patient counseling. The study by El-Andari et al[21] provides impressive support for this statement. The authors analyzed nearly 28,000 patients from two centers (A and B) in the same jurisdiction in Canada who underwent coronary catheterization for suspected CAD in 2017 and 2018. Only center B applied a full heart team review in all patients. There were more than three times the number of PCIs (47 vs 12.8%, p < 0.01) and only two-thirds of CABG procedures (8.5 vs 13.3%, p > 0.001) in center A. At the same time, 1-year mortality was significantly higher compared with center B (4.6 vs 3.9%, p = 0.004). Thus, proper patient-selection currently appears to be the greatest treatment effect modifier, with a complete heart team approach scoring best.
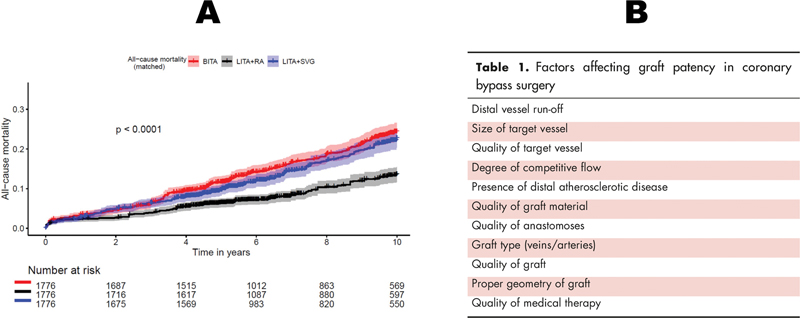
To exploit the optimal CABG treatment effect, grafts must stay patent. In 2022, a new controversy arose among surgeons because the value of the highly appraised but rarely performed bilateral internal thoracic artery grafting was scrutinized with unexpectedly poor outcome data. Alboom et al[22] showed very poor rates of long-term patency for the left internal thoracic artery (RITA) in patients enrolled in the COMPASS trial, with occlusion rates of up to 27% versus around 10% for saphenous vein graft and radial artery at 1 year. Other publications demonstrated excellent long-term patency for the radial artery as second graft in a single-center retrospective analysis[23] and again others showed less intimal hyperplasia in grafted veins, if they were supported by an external stent.[24] A pooled data meta-analysis (PDMA) of four randomized trials finally suggested a survival advantage of using the radial artery over vein or RITA as second grafts[25] ([Fig. 2A]). To complete this confusion, Urso et al[26] presented the best long-term outcomes with bilateral internal thoracic artery grafting compared with left internal thoracic artery plus radial artery, but the differences only appeared after 10 years. We reviewed various factors influencing patency of grafts[27] and suggested that surgical precision and experience taking all factors into account may influence patency rates more than only one factor (such as graft type, degree of competitive flow, or target vessel quality; [Fig. 2B]). It is conceivable that this suggestion explains the apparent discrepancies in the data. Finally, Bianco et al[28] demonstrated the immense power of fully arterial bypass grafting in a propensity-matched comparison of selected patients to PCI. Although the study appears heavily biased (because only those having received fully arterial bypass surgery were compared with patients selected from all PCI patients of that hospital), the 50% mortality reduction may serve as prototypical illustration of the possible dimension of an individual treatment effect ([Fig. 1C]).
In conclusion:
-
The evidence supporting CABG as gold standard for the treatment of CAD, specifically in multivessel disease and/or high anatomic complexity, continues to increase.
-
In patients selected for CABG around the world, long-term survival appears to be superior to that from patients with PCI, independent of the geographic location. Importantly, there appears to be no difference in 30-day mortality between CABG and PCI in risk-adjusted patients.
-
Graft patency is key for a CABG treatment effect. In 2022, evidence for the radial artery as best second graft grew and long-term patency of the RITA was questioned.
-
Patient selection for and surgical precision during CABG appear to be the greatest surgical effect modifiers in current times.
Surgical Treatment of Valve Disease
Aortic Valve
After publication of the new valve guidelines in 2021 and the ramifications of the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) pandemic, the quantitative care of patients with aortic valve stenosis has made another shift toward transcatheter aortic valve implantation (TAVI). In Germany, 80% of all invasively treated aortic stenosis patients received a TAVI.[29] The initial competition of surgical aortic valve replacement (SAVR) and TAVI has calmed down in 2022, and publications now mainly addressed prognostic and technical surgical aspects as well as investigations into the impact and management of valve-related complications. Myers et al published a position statement of the joint surgical societies addressing strengths and weaknesses of the definition of outcome measures for valve research (VARC 3 criteria),[30] the lecture of which can only be recommended.
The only new randomized TAVI versus SAVR comparison was the UK TAVI trial, in which treatments of patients with moderate risk above 70 years were compared. The primary end point (1-year mortality) was not different, adding to the plethora of information that finds similar or slightly better short-term outcomes with TAVI. Chung et al[31] illustrate these better short-term outcomes by demonstrating more days at home with TAVI than with SAVR in the first year after treatment based on assessment of the U.S. CoreValve High Risk trial patients. TAVI patients spent on average ∼4 weeks more at home in the first year than SAVR patients. There was no difference any more in the 4 years to come.
The current status here can be summarized as follows: SAVR patients have slightly higher postprocedural gradients and more postprocedural atrial fibrillation (AF), while TAVI patients require more pacemakers, have more thrombus formation on the valve (hypoattenuating leaflet thickening [HALT]), more paravalvular leaks, and possibly worse survival at longer follow-up.[32] The latter finding is supported also in 2022 from a Polish registry analysis ([Fig. 3A])[33] that repeats registry outcomes from Germany, Italy, and France, demonstrating better survival with SAVR after 5 years, while short-term outcomes are either the same or better with TAVI. These findings cannot be explained by early TAVI degeneration (structural valve degeneration [SVD]), which was long considered the Achilles heel of TAVI. O'Hair et al[34] demonstrate in a post hoc analysis of patients from three intermediate to high-risk trials (U.S. CoreValve High Risk Pivotal, SURTAVI, and CoreValve Extreme Risk Pivotal) that at 5 years SVD appears even higher in SAVR than in TAVI using CoreValve. The potential difference in survival may therefore arise from a combination of events and not directly from one factor. Since the guidelines give a strict age cutoff (primary recommendation for TAVI above 75 years and for SAVR below 75 years in low-risk patients), the plausible conclusion from these data (i.e., to individually decide based on residual life expectancy and fitness to undergo SAVR) is left to the local heart team.

Similarities between TAVI and SAVR up to 5 years were also reported by the U.S. CoreValve investigators[35] and from the GARY registries for patients with mild-moderate chronic kidney disease.[36] Efforts to reduce stroke rates in TAVI (which have thus far been similar in most TAVI/SAVR comparisons) by utilizing embolic protection devices (CEPs) in the PROTECTED TAVR trial have failed to show any measurable effect. The study showed in 3,000 patients who received a TAVI with or without CEP, 2.3 or 2.9% (p = 0.30) suffered from a stroke within 72 hours. This dimension is practically not different to SAVR. A common pattern begins to emerge, in which long-term outcomes appear to be related to a combination of hemodynamic valve performance and their valve-related complications (or their absence), rather than one factor being the main culprit. In any case, it may be prudent to wait the required time for TAVI data to be “old enough” so that long-term effects can properly be assessed. Based on the current practice, one can only hope for all the current TAVI patients that they live up to their expectations.
Another common principle in this context, which has been accepted for decades, is a life-prolonging impact of relieving a pressure-loaded heart from a stenosis in symptomatic patients. In 2022, the AVATAR trial illustrated a significant survival advantage in 157 asymptomatic patients with regular indications for surgery (i.e., mean gradient > 40 mm Hg, flow velocity > 4.9 m/s; [Fig. 3B]).[37] In addition to this proof-of-principle trial, a state-of-the-art review addressing the optimal treatment of aortic stenosis makes a convincing argument that the quality of hemodynamic performance after replacement of a stenotic valve correlates with mortality.[38] The authors describe the current status of prosthesis–patient mismatch and illustrate an algorithm for dealing with high postprocedural gradients
Other investigations have aimed at identifying underlying mechanisms for the occurrence of adverse events. Fukui et al[39] demonstrate that deformations of implanted TAVI contribute to the generation of HALT, which is plausible because proper flow must be disturbed across a valve if the intended shape is not established, and valve thrombosis can be expected as consequence. Squiers et al[40] addressed durability of three pericardial bioprostheses after SAVR using a network meta-analysis. The authors found the best long-term durability with the Magna Ease valve compared with the Mitroflow or the Trifecta. This finding has been a bit surprising, since the Trifecta is the newest valve of the three and has been praised not only for its novel design but also for its superior hemodynamic performance. Possible arguments explaining the differences may be the rather demanding implantation process of the Trifecta, which may result in early damage of the valve and limitation of long-term durability. In any case, the analysis shows that it is not the general type of the prosthesis (e.g., bovine or porcine) that explains the difference, but the long-term performance of each individual valve. This principle is supported by a publication from Sweden, where long-term durability of frequently used surgical bioprostheses was evaluated in almost 17,000 patients (operated between 2003 and 2017) from the SWEDEHEART registry. The authors present again the best results with the Perimount valve (predecessor of Magna Ease), which was in survival only paralleled by the Epic porcine valve ([Fig. 4A]).[41] Finally, a comparison of mechanical versus surgical bioprostheses was also published in 2022. Sotade et al[42] compared almost 4,000 propensity-matched patients having received mechanical or biological aortic valves between age 55 and 64 years. The authors found that mortality was equal up to 10 years and then an advantage for mechanical valves appeared, possibly related to increased rates of reoperations for biological prostheses ([Fig. 4B]).

An alternative to the replacement of the aortic valve with a manufactured artificial valve prostheses is the transfer of the patient's own pulmonary valve into the aortic position and implanting a homograft into the pulmonary position (Ross procedure), a procedure considered valuable specifically in younger patients. Two manuscripts addressed the Ross procedure in 2022 (average patients' age in their 40s). El-Hamamsy et al[43] compared long-term outcomes after the Ross procedure with biological and mechanical aortic valve replacement (AVR) in adults undergoing aortic valve surgery. In propensity-matched cohorts, they found that the Ross procedure was associated with better long-term survival and freedom from valve-related complications compared with prosthetic AVR. At 15 years, the actuarial survival after the Ross procedure was similar to that of the age-, sex-, and race-matched U.S. general population ([Fig. 4C]). Mazine et al[44] reported a propensity-matched single-center comparison of the long-term outcomes of patients after Ross with those receiving bioprosthetic AVR. Again, the Ross procedure was associated with better long-term survival and greater freedom from valve-related events.
These findings are encouraging and demonstrate the advances in cardiac surgery in recent years, because a few decades ago, the Ross procedure was considered a treatment option with a considerable perioperative risk. Similar advances have been demonstrated by Mahboubi et al for patients undergoing redo SAVR.[45] While 10 years ago, there was still a significantly higher mortality risk for redo aortic valve surgery, the risk has now come down to the same level as the primary operation (3.4% in 1985 to 1.3% in 2011). This information is also important for the heart team because the so-called “lifetime management of patients”[38] has moved center stage and heart team members are therefore required to know the outcomes of the different treatment options available now and in the future.
Mitral Valve
Like the aortic valve, direct comparisons of interventional with surgical treatments have become rare. Nappi et al performed a meta-analysis of all trials assessing the impact of invasive treatment of functional mitral regurgitation (FMR). They selected a mix of studies comparing either MitraClip with medical therapy, surgical mitral repair to no mitral procedure in CABG patients with severe FMR, or the impact of repair versus replacement. Based on this potpourri of studies, the authors suggest that FMR is a complex condition, in which invasive treatment reduces the incidence of adverse events (e.g., reoperation, readmission) with the best freedom from adverse events with surgical repair utilizing a subvalvular technique in addition to annuloplasty.[46]
While this meta-analysis evaluated neither the degree of mitral regurgitation (MR) reduction with treatment nor the durability of the repairs, the results and other data give rise to assuming a correlation between the degree of MR and mortality and/or adverse events. This assumption was supported in 2022 by Sannino et al[47] assessing 158 patients with severe FMR who either received MitraClip (60%) or medical therapy alone (40%) as treatment. They measured the change in MR degree in response to the treatment. While they found no significant difference between the MitraClip and the conservative group, there was significantly better survival in those patients that had an elimination of severe MR compared with those where MR remained severe ([Fig. 5]). Similar findings were reported by the COAPT group a year earlier,[48] where postrandomization survival was a function of valve competence in both the interventional and the conservative arm. These data suggest that a durable elimination of MR (irrespective of the underlying pathology or treatment modality) should have the greatest potential to prolong life. However, one would expect that replacement should then be associated with a long-term survival, which could not yet be demonstrated. Three publications addressed this question in 2022[49] [50] [51] and even found superiority of repair in two cases.[49] [51] Thus, while repairs seem to generate the best long-term outcome if the repair is durable, the jury is still out on the exact value of mitral valve replacement.

In general, the advances in mitral valve surgery have been tremendous. Selected patients can now routinely go home 3 days after surgery, a resource that may be exploited more broadly as suggested by Sabatino et al.[52] Current surgical techniques, with[53] or without using PTFE (polytetrafluoroethylene) neochords[54] provide durable repairs for more than 10 years in structural MR. A growing majority of patients is operated upon without sternotomy, although even using robotic assistance does not reduce the pain perceived by the patients.[55] Concomitant procedures can be performed routinely in practically all patients if indicated (e.g., cryoablation for AF[56]) and continuous CO2 flooding of the operative field in minimal-access cases reduces postoperative duration of intubation and the incidence of delirium.[57]
Tricuspid Valve
The main publication addressing the tricuspid valve in 2022 was the CTSN tricuspid trial. Gammie et al present the outcomes of 401 patients with indication for mitral valve surgery and concomitant mild to moderate tricuspid regurgitation (TR) with evidence of tricuspid annular dilatation. Patients were randomized to receive either concomitant tricuspid valve annuloplasty or mitral valve surgery alone. The study demonstrated a greater freedom from TR progression in the tricuspid repair arm at the cost of a significantly higher rate of pacemaker implantations (2.5 vs 14.1%).[58]
Treatment of isolated TR has also received more attention lately. We presented a large series of patients having undergone isolated tricuspid surgery, which we split into three groups separated by the Model of End-Stage Liver Disease (MELD) score. While in patients with MELD scores below 20 the classic EuroSCORE II and STS scores overestimated mortality slightly, patients with MELD scores above 20 had dramatically elevated mortality, making risk prediction with the classic scores practically impossible ([Fig. 6A]).[59] Also, in 2022, Dreyfus et al[60] proposed the TriScore for essentially the same reason. Their score was evaluated in 466 patients and contains components as age, New York Heart Association (NYHA) classification, right-sided heart failure signs, dose of furosemide, glomerular filtration rate, elevation of total bilirubin, left ventricular ejection fraction, and right ventricular dysfunction.[60] Finally, Russo et al presented data from a multicenter registry of 406 patients undergoing isolated tricuspid surgery, suggesting that performing the procedure on the beating heart is associated with the best long-term survival[61] ([Fig. 6B]).

The main findings in 2022 for classic valve surgery are as follows:
-
Evidence in 2022 for the treatment of aortic stenosis supports the notion of similar or slightly better short-term outcome for TAVI but less long-term complications and possibly better survival after 5 years with SAVR. For younger patients, a Ross operation may provide superior long-term results compared with prosthetic valve replacement, which is associated with less valve-related complications.
-
In the field of mitral valve surgery, evidence culminated in 2022 supporting the concept that the best long-term treatment effects, including life prolongation, are associated with the quality (degree of MR reduction) and the durability of the repair.
-
The treatment of TR, if performed concomitantly, may lead to more pacemaker implantations. If performed as isolated procedure, perioperative risk is dominated by liver dysfunction and may be significantly mitigated if performed on the beating heart.
Glimpse into Surgery of the Aorta and for Terminal Heart Failure
Surgery for aortic disease, specifically for type A dissections, is moving toward hybrid operations that utilize frozen stent technology addressing the aortic arch without physically replacing it. The stented arm of the prosthesis is placed into the descending aorta and arch with the proximal connection made at the level of zone 1 or 2 of the aortic arch and debranching of the head vessels. The result is a significant shortening of the arrest, clamp, and operation room times with the potential for less neurological and other complications.[62] Besides the publications in 2022 that supported the concept that arch replacement potentially including elephant trunks may be an option in experienced hands with improved long-term survival,[63] other publications addressed the elevated risk of octogenarians with type A dissections[64] and the need for individual patient selection.[65] An impressive study was published from Paris and Bologna. In patients with extreme risk, the surgeons performed an off-pump wrapping of the aorta with a Teflon sheet and presented favorable outcomes in 35 patients.[66] The video linked to the article is certainly worth watching. Importantly, for patients with acceptable risk for classic surgery, wrapping may not be optimal, as adverse events may still occur in the long run.[67] Finally, a meta-analysis assessed the impact of reperfusion efforts for mesenteric malperfusion in type A dissections. The analysis summarized five manuscripts and concluded that waiting and re-establishing blood flow before surgery for type A dissection is associated with improved outcomes.[68]
In the treatment of terminal heart failure, the field was dominated by the first human xenotransplantation.[69] A 57-year-old patient with nonischemic cardiomyopathy received a heart from a genetically modified pig as compassionate use. Despite a challenging intra- and perioperative course, the patient survived surgery with adequate cardiac function. Subsequently, however, the xenograft began to fail, requiring mechanical circulatory support. With no recovery of pump function, the patient died after 60 days. Investigations on the role of a pig cytomegalovirus virus infection and other issues are still ongoing.
In the left ventricular assist device (LVAD) field, the MOMENTUM3 investigators provided a survival score that may assist heart failure physicians in decision-making, which patient may benefit most from LVAD therapy.[70]
Conflicts of Interest
None declared.
Acknowledgment
We would like to thank for expert technical assistance in the preparation of the manuscript.
-
References
- 1 De Caterina R, Liga R, Boden WE. Myocardial revascularization in ischaemic cardiomyopathy: routine practice vs. scientific evidence. Eur Heart J 2022; 43 (05) 387-390
- 2 Doenst T, Bonow RO, Bhatt DL, Falk V, Gaudino M. Improving terminology to describe coronary artery procedures: JACC review topic of the week. J Am Coll Cardiol 2021; 78 (02) 180-188
- 3 Doenst T, Thiele H, Haasenritter J, Wahlers T, Massberg S, Haverich A. The treatment of coronary artery disease. Dtsch Arztebl Int 2022; 119 (42) 716-723
- 4 Gaudino M, Audisio K, Hueb WA. et al. Coronary artery bypass grafting versus medical therapy in patients with stable coronary artery disease: an individual patient data pooled meta-analysis of randomized trials. J Thorac Cardiovasc Surg 2022 (e-pub ahead of print). Doi: 10.1016/j.jtcvs.2022.06.003
- 5 Heer T, von Scheidt M, Boening A. et al. Prognostic impact of secondary prevention after coronary artery bypass grafting-insights from the TiCAB trial. Eur J Cardiothorac Surg 2022; 62 (03) 62
- 6 Sandner S, Redfors B, Angiolillo DJ. et al. Association of dual antiplatelet therapy with ticagrelor with vein graft failure after coronary artery bypass graft surgery: a systematic review and meta-analysis. JAMA 2022; 328 (06) 554-562
- 7 Senior R, Reynolds HR, Min JK. et al; ISCHEMIA Research Group. Predictors of left main coronary artery disease in the ISCHEMIA trial. J Am Coll Cardiol 2022; 79 (07) 651-661
- 8 Ono M, Hara H, Gao C. et al; SYNTAX Extended Survival Investigators. Mortality after multivessel revascularisation involving the proximal left anterior descending artery. Heart 2022; 108 (22) 1784-1791
- 9 Ninomiya K, Serruys PW, Garg S. et al; SYNTAX Extended Survival Investigators. Predicted and observed mortality at 10 years in patients with bifurcation lesions in the SYNTAX trial. JACC Cardiovasc Interv 2022; 15 (12) 1231-1242
- 10 Gaudino M, Di Franco A, Spadaccio C. et al. Difference in spontaneous myocardial infarction and mortality in percutaneous versus surgical revascularization trials: a systematic review and meta-analysis. J Thorac Cardiovasc Surg 2023; 165 (02) 662-669.e14
- 11 Head SJ, Milojevic M, Daemen J. et al. Mortality after coronary artery bypass grafting versus percutaneous coronary intervention with stenting for coronary artery disease: a pooled analysis of individual patient data. Lancet 2018; 391 (10124): 939-948
- 12 Fearon WF, Zimmermann FM, De Bruyne B. et al; FAME 3 Investigators. Fractional flow reserve-guided PCI as compared with coronary bypass surgery. N Engl J Med 2022; 386 (02) 128-137
- 13 Caldonazo T, Kirov H, Riedel LL, Gaudino M, Doenst T. Comparing CABG and PCI across the globe based on current regional registry evidence. Sci Rep 2022; 12 (01) 22164
- 14 Doenst T, Falk V, Gaudino M. The issues with risk and benefit evaluation for invasive treatment of cardiac disease. Ann Thorac Surg 2021; 112 (06) 1733-1735
- 15 Tam DY, Fang J, Rocha RV. et al. Real-world examination of revascularization strategies for left main coronary disease in Ontario, Canada. JACC Cardiovasc Interv 2023; 16 (03) 277-288
- 16 Kirov H, Caldonazo T, Rahouma M. et al. A systematic review and meta-analysis of percutaneous coronary intervention compared to coronary artery bypass grafting in non-ST-elevation acute coronary syndrome. Sci Rep 2022; 12 (01) 5138
- 17 Ram E, Fisman EZ, Tenenbaum A. et al. Revascularization outcomes in diabetic patients presenting with acute coronary syndrome with non-ST elevation. Cardiovasc Diabetol 2022; 21 (01) 175
- 18 Rocha RV, Fang J, Tam DY. et al. Multiple arterial coronary bypass grafting is associated with better survival compared with second-generation drug-eluting stents in patients with stable multivessel coronary artery disease. J Thorac Cardiovasc Surg 2021 (e-pub ahead of printy). Doi: 10.1016/j.jtcvs.2021.12.026
- 19 Tasoudis PT, Varvoglis DN, Tzoumas A. et al. Percutaneous coronary intervention versus coronary artery bypass graft surgery in dialysis-dependent patients: a pooled meta-analysis of reconstructed time-to-event data. J Card Surg 2022; 37 (10) 3365-3373
- 20 Lin S, Guan C, Wu F. et al. Coronary artery bypass grafting and percutaneous coronary intervention in patients with chronic total occlusion and multivessel disease. Circ Cardiovasc Interv 2022; 15 (02) e011312
- 21 El-Andari R, Nagendran J, Hong Y, Ali I, Nagendran J. Percutaneous coronary intervention versus coronary artery bypass grafting for patients with three vessel coronary artery disease: a comparison of centers in the same jurisdiction with differing multidisciplinary heart team approaches. Ann Surg 2022; 278 (01) e190-e195
- 22 Alboom M, Browne A, Sheth T. et al. Conduit selection and early graft failure in coronary artery bypass surgery: A post hoc analysis of the Cardiovascular Outcomes for People Using Anticoagulation Strategies (COMPASS) coronary artery bypass grafting study. J Thorac Cardiovasc Surg 2022; (e-pub ahead of print)
- 23 Ren J, Royse C, Siderakis C, Srivastav N, Royse A. Long-term observational angiographic patency and perfect patency of radial artery compared with saphenous vein or internal mammary artery in coronary bypass surgery. J Thorac Cardiovasc Surg 2022 (e-pub ahead of print). Doi: 10.1016/j.jtcvs.2022.08.047
- 24 Sandner SE, Donovan TJ, Edelstein S. et al. Effects of the harvesting technique and external stenting on progression of vein graft disease 2 years after coronary artery bypass. Eur J Cardiothorac Surg 2022; 62 (01) 62
- 25 Gaudino M, Audisio K, Di Franco A. et al. Radial artery versus saphenous vein versus right internal thoracic artery for coronary artery bypass grafting. Eur J Cardiothorac Surg 2022; 62 (01) 62
- 26 Urso S, Sadaba R, González Martín JM, Nogales E, Tena MÁ, Portela F. Bilateral internal thoracic artery versus single internal thoracic artery plus radial artery: a double meta-analytic approach. J Thorac Cardiovasc Surg 2022 (e-pub ahead of print). Doi: 10.1016/j.jtcvs.2022.03.010
- 27 Doenst T, Sousa-Uva M. How to deal with nonsevere stenoses in coronary artery bypass grafting - a critical perspective on competitive flow and surgical precision. Curr Opin Cardiol 2022; 37 (06) 468-473
- 28 Bianco V, Mulukutla S, Aranda-Michel E. et al. Coronary artery bypass with multiarterial grafting vs percutaneous coronary intervention. Ann Thorac Surg 2023; 115 (02) 404-410
- 29 Gaede L, Blumenstein J, Eckel C. et al. Transcatheter-based aortic valve replacement vs. isolated surgical aortic valve replacement in 2020. Clin Res Cardiol 2022; 111 (08) 924-933
- 30 Myers PO, Beyersdorf F, Sadaba R, Milojevic M. European Association for Cardio-Thoracic Surgery Statement regarding the 2021 American Heart Association/American College of Cardiology/Society for Cardiovascular Angiography and Interventions Coronary Artery Revascularization guidelines. Eur J Cardiothorac Surg 2022; 62 (01) 62
- 31 Chung M, Butala NM, Faridi KF. et al. Days at home after transcatheter or surgical aortic valve replacement in high-risk patients. Am Heart J 2023; 255: 125-136
- 32 Doenst T, Schneider U, Can T. et al. Cardiac surgery 2021 reviewed. Thorac Cardiovasc Surg 2022; 70 (04) 278-288
- 33 Kowalówka AR, Kowalewski M, Wańha W. et al. Surgical and transcatheter aortic valve replacement for severe aortic stenosis in low-risk elective patients: analysis of the Aortic Valve Replacement in Elective Patients From the Aortic Valve Multicenter Registry. J Thorac Cardiovasc Surg 2022 (e-pub ahead of print). Doi: 10.1016/j.jtcvs.2022.10.026
- 34 O'Hair D, Yakubov SJ, Grubb KJ. et al. Structural valve deterioration after self-expanding transcatheter or surgical aortic valve implantation in patients at intermediate or high risk. JAMA Cardiol 2023; 8 (02) 111-119
- 35 Van Mieghem NM, Deeb GM, Søndergaard L. et al; SURTAVI Trial Investigators. Self-expanding transcatheter vs surgical aortic valve replacement in intermediate-risk patients: 5-year outcomes of the SURTAVI randomized clinical trial. JAMA Cardiol 2022; 7 (10) 1000-1008
- 36 Mas-Peiro S, Faerber G, Bon D. et al; GARY-Executive Board. Propensity matched comparison of TAVI and SAVR in intermediate-risk patients with severe aortic stenosis and moderate-to-severe chronic kidney disease: a subgroup analysis from the German Aortic Valve Registry. Clin Res Cardiol 2022; 111 (12) 1387-1395
- 37 Banovic M, Putnik S, Penicka M. et al; AVATAR Trial Investigators. Aortic valve replacement versus conservative treatment in asymptomatic severe aortic stenosis: the AVATAR trial. Circulation 2022; 145 (09) 648-658
- 38 Pibarot P, Herrmann HC, Wu C. et al; Heart Valve Collaboratory. Standardized definitions for bioprosthetic valve dysfunction following aortic or mitral valve replacement: JACC state-of-the-art review. J Am Coll Cardiol 2022; 80 (05) 545-561
- 39 Fukui M, Bapat VN, Garcia S. et al. Deformation of transcatheter aortic valve prostheses: implications for hypoattenuating leaflet thickening and clinical outcomes. Circulation 2022; 146 (06) 480-493
- 40 Squiers JJ, Robinson NB, Audisio K. et al. Structural valve degeneration of bioprosthetic aortic valves: a network meta-analysis. J Thorac Cardiovasc Surg 2023; 166 (01) 52-59
- 41 Persson M, Glaser N, Nilsson J, Friberg Ö, Franco-Cereceda A, Sartipy U. Comparison of long-term performance of bioprosthetic aortic valves in Sweden from 2003 to 2018. JAMA Netw Open 2022; 5 (03) e220962
- 42 Sotade OT, Falster MO, Pearson SA, Jorm LR, Sedrakyan A. Comparison of long-term outcomes of bioprosthetic and mechanical aortic valve replacement in patients younger than 65 years. J Thorac Cardiovasc Surg 2022; (e-pub ahead of print).
- 43 El-Hamamsy I, Toyoda N, Itagaki S. et al. Propensity-matched comparison of the Ross procedure and prosthetic aortic valve replacement in adults. J Am Coll Cardiol 2022; 79 (08) 805-815
- 44 Mazine A, David TE, Stoklosa K, Chung J, Lafreniere-Roula M, Ouzounian M. Improved outcomes following the Ross procedure compared with bioprosthetic aortic valve replacement. J Am Coll Cardiol 2022; 79 (10) 993-1005
- 45 Mahboubi R, Kakavand M, Soltesz EG. et al. The decreasing risk of reoperative aortic valve replacement: implications for valve choice and transcatheter therapy. J Thorac Cardiovasc Surg 2022 (e-pub ahead of print). Doi: 10.1016/j.jtcvs.2022.02.052
- 46 Nappi F, Antoniou GA, Nenna A. et al. Treatment options for ischemic mitral regurgitation: A meta-analysis. J Thorac Cardiovasc Surg 2022; 163 (02) 607-622.e14
- 47 Sannino A, Banwait JK, Sudhakaran S. et al. Impact of improving severity of secondary mitral regurgitation on survival. ESC Heart Fail 2023; 10 (01) 742-745
- 48 Kar S, Mack MJ, Lindenfeld J. et al. Relationship between residual mitral regurgitation and clinical and quality-of-life outcomes after transcatheter and medical treatments in heart failure: COAPT trial. Circulation 2021; 144 (06) 426-437
- 49 Brescia AA, Watt TMF, Murray SL. et al; Michigan Mitral Research Group. Rheumatic mitral valve repair or replacement in the valve-in-valve era. J Thorac Cardiovasc Surg 2022; 163 (02) 591-602.e1
- 50 Chen SW, Chen CY, Chien-Chia Wu V. et al. Mitral valve repair versus replacement in patients with rheumatic heart disease. J Thorac Cardiovasc Surg 2022; 164 (01) 57-67.e11
- 51 Muncan B, Amabile A, Kalogeropoulos AP, Geirsson A, Krane M. Midterm outcomes of mitral valve repair versus replacement in elderly patients: a propensity score-matched analysis. J Card Surg 2022; 37 (12) 4391-4396
- 52 Sabatino ME, Okoh AK, Chao JC. et al. Early discharge after minimally invasive aortic and mitral valve surgery. Ann Thorac Surg 2022; 114 (01) 91-97
- 53 Lang M, Vitanova K, Voss B. et al. Beyond the 10-year horizon: mitral valve repair solely with chordal replacement and annuloplasty. Ann Thorac Surg 2023; 115 (01) 96-103
- 54 Folino G, Salica A, Scaffa R. et al. Mitral repair of myxomatous valves with simple annuloplasty: a follow-up up to 12 years. Eur J Cardiothorac Surg 2022; 63 (01) 63
- 55 Jahanian S, Arghami A, Wittwer ED. et al. Does minimally invasive mitral valve repair mean less postoperative pain?. Ann Thorac Surg 2023; 115 (05) 1172-1178
- 56 McCarthy PM, Cox JL, Kruse J, Elenbaas C, Andrei AC. One hundred percent utilization of a modified CryoMaze III procedure for atrial fibrillation with mitral surgery. J Thorac Cardiovasc Surg 2022 (e-pub ahead of print). Doi: 10.1016/j.jtcvs.2022.08.028
- 57 Nasso G, Condello I, Santarpino G. et al. Continuous field flooding versus final one-shot CO2 insufflation in minimally invasive mitral valve repair. J Cardiothorac Surg 2022; 17 (01) 279
- 58 Gammie JS, Chu MWA, Falk V. et al; CTSN Investigators. Concomitant tricuspid repair in patients with degenerative mitral regurgitation. N Engl J Med 2022; 386 (04) 327-339
- 59 Färber G, Marx J, Scherag A. et al. Risk stratification for isolated tricuspid valve surgery assisted using the Model for End-Stage Liver Disease score. J Thorac Cardiovasc Surg 2022 (e-pub ahead of print). Doi: 10.1016/j.jtcvs.2021.11.102
- 60 Dreyfus J, Audureau E, Bohbot Y. et al. TRI-SCORE: a new risk score for in-hospital mortality prediction after isolated tricuspid valve surgery. Eur Heart J 2022; 43 (07) 654-662
- 61 Russo M, Di Mauro M, Saitto G. et al. Beating versus arrested heart isolated tricuspid valve surgery: long-term outcomes. Ann Thorac Surg 2022; 113 (02) 585-592
- 62 Huang F, Li X, Zhang Z, Li C, Ren F. Comparison of two surgical approaches for acute type A aortic dissection: hybrid debranching versus total arch replacement. J Cardiothorac Surg 2022; 17 (01) 166
- 63 Sá MP, Jacquemyn X, Tasoudis PT. et al. Long-term outcomes of total arch replacement versus proximal aortic replacement in acute type A aortic dissection: meta-analysis of Kaplan-Meier-derived individual patient data. J Card Surg 2022; 37 (12) 4256-4266
- 64 Eranki A, Merakis M, Williams ML. et al. Outcomes of surgery for acute type A dissection in octogenarians versus non-octogenarians: a systematic review and meta analysis. J Cardiothorac Surg 2022; 17 (01) 222
- 65 Hemli JM, Pupovac SS, Gleason TG. et al; IRAD Investigators. Management of acute type A aortic dissection in the elderly: an analysis from IRAD. Eur J Cardiothorac Surg 2022; 61 (04) 838-846
- 66 Vento V, Multon S, Ramadan R. et al. Outcomes of urgent aortic wrapping for acute type A aortic dissection. J Thorac Cardiovasc Surg 2022; 164 (05) 1412-1420
- 67 Ehrlich T, Federspiel JM, Bohle RM, Schäfers HJ. Severe aortic wall degeneration after aortic wrapping. Eur J Cardiothorac Surg 2021; 60 (02) 425-427
- 68 Xu X, Wu Y, Wu Z. Revascularization-first strategy versus central repair-first strategy for acute type A aortic dissection complicated with mesenteric malperfusion syndrome: A meta-analysis. J Card Surg 2022; 37 (12) 4427-4433
- 69 Griffith BP, Goerlich CE, Singh AK. et al. Genetically modified porcine-to-human cardiac xenotransplantation. N Engl J Med 2022; 387 (01) 35-44
- 70 Mehra MR, Nayak A, Morris AA. et al. Prediction of survival after implantation of a fully magnetically levitated left ventricular assist device. JACC Heart Fail 2022; 10 (12) 948-959
Address for correspondence
Publikationsverlauf
Eingereicht: 17. Februar 2023
Angenommen: 23. März 2023
Artikel online veröffentlicht:
17. Mai 2023
© 2023. Thieme. All rights reserved.
Georg Thieme Verlag KG
Rüdigerstraße 14, 70469 Stuttgart, Germany
-
References
- 1 De Caterina R, Liga R, Boden WE. Myocardial revascularization in ischaemic cardiomyopathy: routine practice vs. scientific evidence. Eur Heart J 2022; 43 (05) 387-390
- 2 Doenst T, Bonow RO, Bhatt DL, Falk V, Gaudino M. Improving terminology to describe coronary artery procedures: JACC review topic of the week. J Am Coll Cardiol 2021; 78 (02) 180-188
- 3 Doenst T, Thiele H, Haasenritter J, Wahlers T, Massberg S, Haverich A. The treatment of coronary artery disease. Dtsch Arztebl Int 2022; 119 (42) 716-723
- 4 Gaudino M, Audisio K, Hueb WA. et al. Coronary artery bypass grafting versus medical therapy in patients with stable coronary artery disease: an individual patient data pooled meta-analysis of randomized trials. J Thorac Cardiovasc Surg 2022 (e-pub ahead of print). Doi: 10.1016/j.jtcvs.2022.06.003
- 5 Heer T, von Scheidt M, Boening A. et al. Prognostic impact of secondary prevention after coronary artery bypass grafting-insights from the TiCAB trial. Eur J Cardiothorac Surg 2022; 62 (03) 62
- 6 Sandner S, Redfors B, Angiolillo DJ. et al. Association of dual antiplatelet therapy with ticagrelor with vein graft failure after coronary artery bypass graft surgery: a systematic review and meta-analysis. JAMA 2022; 328 (06) 554-562
- 7 Senior R, Reynolds HR, Min JK. et al; ISCHEMIA Research Group. Predictors of left main coronary artery disease in the ISCHEMIA trial. J Am Coll Cardiol 2022; 79 (07) 651-661
- 8 Ono M, Hara H, Gao C. et al; SYNTAX Extended Survival Investigators. Mortality after multivessel revascularisation involving the proximal left anterior descending artery. Heart 2022; 108 (22) 1784-1791
- 9 Ninomiya K, Serruys PW, Garg S. et al; SYNTAX Extended Survival Investigators. Predicted and observed mortality at 10 years in patients with bifurcation lesions in the SYNTAX trial. JACC Cardiovasc Interv 2022; 15 (12) 1231-1242
- 10 Gaudino M, Di Franco A, Spadaccio C. et al. Difference in spontaneous myocardial infarction and mortality in percutaneous versus surgical revascularization trials: a systematic review and meta-analysis. J Thorac Cardiovasc Surg 2023; 165 (02) 662-669.e14
- 11 Head SJ, Milojevic M, Daemen J. et al. Mortality after coronary artery bypass grafting versus percutaneous coronary intervention with stenting for coronary artery disease: a pooled analysis of individual patient data. Lancet 2018; 391 (10124): 939-948
- 12 Fearon WF, Zimmermann FM, De Bruyne B. et al; FAME 3 Investigators. Fractional flow reserve-guided PCI as compared with coronary bypass surgery. N Engl J Med 2022; 386 (02) 128-137
- 13 Caldonazo T, Kirov H, Riedel LL, Gaudino M, Doenst T. Comparing CABG and PCI across the globe based on current regional registry evidence. Sci Rep 2022; 12 (01) 22164
- 14 Doenst T, Falk V, Gaudino M. The issues with risk and benefit evaluation for invasive treatment of cardiac disease. Ann Thorac Surg 2021; 112 (06) 1733-1735
- 15 Tam DY, Fang J, Rocha RV. et al. Real-world examination of revascularization strategies for left main coronary disease in Ontario, Canada. JACC Cardiovasc Interv 2023; 16 (03) 277-288
- 16 Kirov H, Caldonazo T, Rahouma M. et al. A systematic review and meta-analysis of percutaneous coronary intervention compared to coronary artery bypass grafting in non-ST-elevation acute coronary syndrome. Sci Rep 2022; 12 (01) 5138
- 17 Ram E, Fisman EZ, Tenenbaum A. et al. Revascularization outcomes in diabetic patients presenting with acute coronary syndrome with non-ST elevation. Cardiovasc Diabetol 2022; 21 (01) 175
- 18 Rocha RV, Fang J, Tam DY. et al. Multiple arterial coronary bypass grafting is associated with better survival compared with second-generation drug-eluting stents in patients with stable multivessel coronary artery disease. J Thorac Cardiovasc Surg 2021 (e-pub ahead of printy). Doi: 10.1016/j.jtcvs.2021.12.026
- 19 Tasoudis PT, Varvoglis DN, Tzoumas A. et al. Percutaneous coronary intervention versus coronary artery bypass graft surgery in dialysis-dependent patients: a pooled meta-analysis of reconstructed time-to-event data. J Card Surg 2022; 37 (10) 3365-3373
- 20 Lin S, Guan C, Wu F. et al. Coronary artery bypass grafting and percutaneous coronary intervention in patients with chronic total occlusion and multivessel disease. Circ Cardiovasc Interv 2022; 15 (02) e011312
- 21 El-Andari R, Nagendran J, Hong Y, Ali I, Nagendran J. Percutaneous coronary intervention versus coronary artery bypass grafting for patients with three vessel coronary artery disease: a comparison of centers in the same jurisdiction with differing multidisciplinary heart team approaches. Ann Surg 2022; 278 (01) e190-e195
- 22 Alboom M, Browne A, Sheth T. et al. Conduit selection and early graft failure in coronary artery bypass surgery: A post hoc analysis of the Cardiovascular Outcomes for People Using Anticoagulation Strategies (COMPASS) coronary artery bypass grafting study. J Thorac Cardiovasc Surg 2022; (e-pub ahead of print)
- 23 Ren J, Royse C, Siderakis C, Srivastav N, Royse A. Long-term observational angiographic patency and perfect patency of radial artery compared with saphenous vein or internal mammary artery in coronary bypass surgery. J Thorac Cardiovasc Surg 2022 (e-pub ahead of print). Doi: 10.1016/j.jtcvs.2022.08.047
- 24 Sandner SE, Donovan TJ, Edelstein S. et al. Effects of the harvesting technique and external stenting on progression of vein graft disease 2 years after coronary artery bypass. Eur J Cardiothorac Surg 2022; 62 (01) 62
- 25 Gaudino M, Audisio K, Di Franco A. et al. Radial artery versus saphenous vein versus right internal thoracic artery for coronary artery bypass grafting. Eur J Cardiothorac Surg 2022; 62 (01) 62
- 26 Urso S, Sadaba R, González Martín JM, Nogales E, Tena MÁ, Portela F. Bilateral internal thoracic artery versus single internal thoracic artery plus radial artery: a double meta-analytic approach. J Thorac Cardiovasc Surg 2022 (e-pub ahead of print). Doi: 10.1016/j.jtcvs.2022.03.010
- 27 Doenst T, Sousa-Uva M. How to deal with nonsevere stenoses in coronary artery bypass grafting - a critical perspective on competitive flow and surgical precision. Curr Opin Cardiol 2022; 37 (06) 468-473
- 28 Bianco V, Mulukutla S, Aranda-Michel E. et al. Coronary artery bypass with multiarterial grafting vs percutaneous coronary intervention. Ann Thorac Surg 2023; 115 (02) 404-410
- 29 Gaede L, Blumenstein J, Eckel C. et al. Transcatheter-based aortic valve replacement vs. isolated surgical aortic valve replacement in 2020. Clin Res Cardiol 2022; 111 (08) 924-933
- 30 Myers PO, Beyersdorf F, Sadaba R, Milojevic M. European Association for Cardio-Thoracic Surgery Statement regarding the 2021 American Heart Association/American College of Cardiology/Society for Cardiovascular Angiography and Interventions Coronary Artery Revascularization guidelines. Eur J Cardiothorac Surg 2022; 62 (01) 62
- 31 Chung M, Butala NM, Faridi KF. et al. Days at home after transcatheter or surgical aortic valve replacement in high-risk patients. Am Heart J 2023; 255: 125-136
- 32 Doenst T, Schneider U, Can T. et al. Cardiac surgery 2021 reviewed. Thorac Cardiovasc Surg 2022; 70 (04) 278-288
- 33 Kowalówka AR, Kowalewski M, Wańha W. et al. Surgical and transcatheter aortic valve replacement for severe aortic stenosis in low-risk elective patients: analysis of the Aortic Valve Replacement in Elective Patients From the Aortic Valve Multicenter Registry. J Thorac Cardiovasc Surg 2022 (e-pub ahead of print). Doi: 10.1016/j.jtcvs.2022.10.026
- 34 O'Hair D, Yakubov SJ, Grubb KJ. et al. Structural valve deterioration after self-expanding transcatheter or surgical aortic valve implantation in patients at intermediate or high risk. JAMA Cardiol 2023; 8 (02) 111-119
- 35 Van Mieghem NM, Deeb GM, Søndergaard L. et al; SURTAVI Trial Investigators. Self-expanding transcatheter vs surgical aortic valve replacement in intermediate-risk patients: 5-year outcomes of the SURTAVI randomized clinical trial. JAMA Cardiol 2022; 7 (10) 1000-1008
- 36 Mas-Peiro S, Faerber G, Bon D. et al; GARY-Executive Board. Propensity matched comparison of TAVI and SAVR in intermediate-risk patients with severe aortic stenosis and moderate-to-severe chronic kidney disease: a subgroup analysis from the German Aortic Valve Registry. Clin Res Cardiol 2022; 111 (12) 1387-1395
- 37 Banovic M, Putnik S, Penicka M. et al; AVATAR Trial Investigators. Aortic valve replacement versus conservative treatment in asymptomatic severe aortic stenosis: the AVATAR trial. Circulation 2022; 145 (09) 648-658
- 38 Pibarot P, Herrmann HC, Wu C. et al; Heart Valve Collaboratory. Standardized definitions for bioprosthetic valve dysfunction following aortic or mitral valve replacement: JACC state-of-the-art review. J Am Coll Cardiol 2022; 80 (05) 545-561
- 39 Fukui M, Bapat VN, Garcia S. et al. Deformation of transcatheter aortic valve prostheses: implications for hypoattenuating leaflet thickening and clinical outcomes. Circulation 2022; 146 (06) 480-493
- 40 Squiers JJ, Robinson NB, Audisio K. et al. Structural valve degeneration of bioprosthetic aortic valves: a network meta-analysis. J Thorac Cardiovasc Surg 2023; 166 (01) 52-59
- 41 Persson M, Glaser N, Nilsson J, Friberg Ö, Franco-Cereceda A, Sartipy U. Comparison of long-term performance of bioprosthetic aortic valves in Sweden from 2003 to 2018. JAMA Netw Open 2022; 5 (03) e220962
- 42 Sotade OT, Falster MO, Pearson SA, Jorm LR, Sedrakyan A. Comparison of long-term outcomes of bioprosthetic and mechanical aortic valve replacement in patients younger than 65 years. J Thorac Cardiovasc Surg 2022; (e-pub ahead of print).
- 43 El-Hamamsy I, Toyoda N, Itagaki S. et al. Propensity-matched comparison of the Ross procedure and prosthetic aortic valve replacement in adults. J Am Coll Cardiol 2022; 79 (08) 805-815
- 44 Mazine A, David TE, Stoklosa K, Chung J, Lafreniere-Roula M, Ouzounian M. Improved outcomes following the Ross procedure compared with bioprosthetic aortic valve replacement. J Am Coll Cardiol 2022; 79 (10) 993-1005
- 45 Mahboubi R, Kakavand M, Soltesz EG. et al. The decreasing risk of reoperative aortic valve replacement: implications for valve choice and transcatheter therapy. J Thorac Cardiovasc Surg 2022 (e-pub ahead of print). Doi: 10.1016/j.jtcvs.2022.02.052
- 46 Nappi F, Antoniou GA, Nenna A. et al. Treatment options for ischemic mitral regurgitation: A meta-analysis. J Thorac Cardiovasc Surg 2022; 163 (02) 607-622.e14
- 47 Sannino A, Banwait JK, Sudhakaran S. et al. Impact of improving severity of secondary mitral regurgitation on survival. ESC Heart Fail 2023; 10 (01) 742-745
- 48 Kar S, Mack MJ, Lindenfeld J. et al. Relationship between residual mitral regurgitation and clinical and quality-of-life outcomes after transcatheter and medical treatments in heart failure: COAPT trial. Circulation 2021; 144 (06) 426-437
- 49 Brescia AA, Watt TMF, Murray SL. et al; Michigan Mitral Research Group. Rheumatic mitral valve repair or replacement in the valve-in-valve era. J Thorac Cardiovasc Surg 2022; 163 (02) 591-602.e1
- 50 Chen SW, Chen CY, Chien-Chia Wu V. et al. Mitral valve repair versus replacement in patients with rheumatic heart disease. J Thorac Cardiovasc Surg 2022; 164 (01) 57-67.e11
- 51 Muncan B, Amabile A, Kalogeropoulos AP, Geirsson A, Krane M. Midterm outcomes of mitral valve repair versus replacement in elderly patients: a propensity score-matched analysis. J Card Surg 2022; 37 (12) 4391-4396
- 52 Sabatino ME, Okoh AK, Chao JC. et al. Early discharge after minimally invasive aortic and mitral valve surgery. Ann Thorac Surg 2022; 114 (01) 91-97
- 53 Lang M, Vitanova K, Voss B. et al. Beyond the 10-year horizon: mitral valve repair solely with chordal replacement and annuloplasty. Ann Thorac Surg 2023; 115 (01) 96-103
- 54 Folino G, Salica A, Scaffa R. et al. Mitral repair of myxomatous valves with simple annuloplasty: a follow-up up to 12 years. Eur J Cardiothorac Surg 2022; 63 (01) 63
- 55 Jahanian S, Arghami A, Wittwer ED. et al. Does minimally invasive mitral valve repair mean less postoperative pain?. Ann Thorac Surg 2023; 115 (05) 1172-1178
- 56 McCarthy PM, Cox JL, Kruse J, Elenbaas C, Andrei AC. One hundred percent utilization of a modified CryoMaze III procedure for atrial fibrillation with mitral surgery. J Thorac Cardiovasc Surg 2022 (e-pub ahead of print). Doi: 10.1016/j.jtcvs.2022.08.028
- 57 Nasso G, Condello I, Santarpino G. et al. Continuous field flooding versus final one-shot CO2 insufflation in minimally invasive mitral valve repair. J Cardiothorac Surg 2022; 17 (01) 279
- 58 Gammie JS, Chu MWA, Falk V. et al; CTSN Investigators. Concomitant tricuspid repair in patients with degenerative mitral regurgitation. N Engl J Med 2022; 386 (04) 327-339
- 59 Färber G, Marx J, Scherag A. et al. Risk stratification for isolated tricuspid valve surgery assisted using the Model for End-Stage Liver Disease score. J Thorac Cardiovasc Surg 2022 (e-pub ahead of print). Doi: 10.1016/j.jtcvs.2021.11.102
- 60 Dreyfus J, Audureau E, Bohbot Y. et al. TRI-SCORE: a new risk score for in-hospital mortality prediction after isolated tricuspid valve surgery. Eur Heart J 2022; 43 (07) 654-662
- 61 Russo M, Di Mauro M, Saitto G. et al. Beating versus arrested heart isolated tricuspid valve surgery: long-term outcomes. Ann Thorac Surg 2022; 113 (02) 585-592
- 62 Huang F, Li X, Zhang Z, Li C, Ren F. Comparison of two surgical approaches for acute type A aortic dissection: hybrid debranching versus total arch replacement. J Cardiothorac Surg 2022; 17 (01) 166
- 63 Sá MP, Jacquemyn X, Tasoudis PT. et al. Long-term outcomes of total arch replacement versus proximal aortic replacement in acute type A aortic dissection: meta-analysis of Kaplan-Meier-derived individual patient data. J Card Surg 2022; 37 (12) 4256-4266
- 64 Eranki A, Merakis M, Williams ML. et al. Outcomes of surgery for acute type A dissection in octogenarians versus non-octogenarians: a systematic review and meta analysis. J Cardiothorac Surg 2022; 17 (01) 222
- 65 Hemli JM, Pupovac SS, Gleason TG. et al; IRAD Investigators. Management of acute type A aortic dissection in the elderly: an analysis from IRAD. Eur J Cardiothorac Surg 2022; 61 (04) 838-846
- 66 Vento V, Multon S, Ramadan R. et al. Outcomes of urgent aortic wrapping for acute type A aortic dissection. J Thorac Cardiovasc Surg 2022; 164 (05) 1412-1420
- 67 Ehrlich T, Federspiel JM, Bohle RM, Schäfers HJ. Severe aortic wall degeneration after aortic wrapping. Eur J Cardiothorac Surg 2021; 60 (02) 425-427
- 68 Xu X, Wu Y, Wu Z. Revascularization-first strategy versus central repair-first strategy for acute type A aortic dissection complicated with mesenteric malperfusion syndrome: A meta-analysis. J Card Surg 2022; 37 (12) 4427-4433
- 69 Griffith BP, Goerlich CE, Singh AK. et al. Genetically modified porcine-to-human cardiac xenotransplantation. N Engl J Med 2022; 387 (01) 35-44
- 70 Mehra MR, Nayak A, Morris AA. et al. Prediction of survival after implantation of a fully magnetically levitated left ventricular assist device. JACC Heart Fail 2022; 10 (12) 948-959