

RSS-Feed abonnieren
DOI: 10.1055/s-0044-1782614
A Glimpse into the Prognostic Factors of Outcomes for Isolated, Operated Severe Traumatic Head Injury Patients in a Resource Constrained Trauma Center Setup
Autoren


Abstract
Background
Severe traumatic brain injury (STBI) continues to burden health care in developing countries. This study focuses on STBI patients undergoing surgical intervention to understand the factors affecting their outcomes in a constrained trauma center setup.
Aim
This aims to study the epidemiological and clinical factors to understand the long-term morbidity, mortality risks, and triaging among STBI patients requiring surgery.
Materials and Methods
A prospective observational study was conducted on 227 isolated STBI patients with Glasgow Coma Scale (GCS) ≤ 8 who underwent surgical evacuation of intracranial lesions. Patients were classified based on their neurological status and lesions on computed tomography head. Postoperative data on complications were collected. At 6-month follow-up, patients with Glasgow (Extended) scores of 7 to 8 were deemed good outcomes, and scores of 1 to 6 were deemed poor. Cox regression analysis was used to identify independent influencing factors, with p < 0.05 as statistically significant.
Results
The clinicoradiological factors including age (p = 0.02), asymmetric pupillary reaction (p = 0.002), low presenting pulse rate (p = 0.041), and low systolic and diastolic blood pressure (p = 0.016 and p < 0.0001, respectively), low GCS (p = 0.011), midline shift > 5 mm (p < 0.0001), and obliterated basal cisterns were significantly associated with poor outcome. Tracheostomy, respiratory tract infection, bedsore, meningitis, deep vein thrombosis, cerebrospinal fluid leak, and bone flap site infection were significantly associated with survival of the patients (p = 0.036). The most common cause of mortality during home care included respiratory tract infection and was associated with the care of the tracheostomized. GCS (p < 0.0001), age (p = 0.005), and alcohol use (p = 0.034) were independent predictors for the outcome of patients.
Conclusion
This study helps clinicians predict prognosis, postoperative recovery, manage challenges, counsel caregivers, and predict long-term patient outcomes.
Keywords
severe traumatic brain injury - Glasgow Coma Scale (GCS) - midline shift - tracheostomy - respiratory tract infection and prognosisIntroduction
Traumatic brain injuries (TBIs) are a significant global health concern, with 27 million new cases reported annually.[1] Of these, 4% require neurosurgical intervention.[2] Timely and adequate emergency surgery for TBI can dramatically improve outcomes. However, most injuries occur in developing nations with limited access to neurosurgical care.[3]
Emergency surgical interventions for neurotrauma, such as the evacuation of traumatic intracranial hematomas and the elevation of depressed skull fractures, are recognized as essential worldwide.[4] Trauma presents with various injuries and problems that require rapid assessment, discussion, and intervention to prevent mortality and avoid permanent disability.[5] Hypovolemic shock and brain injuries are the two major causes of early mortality from trauma.[6] Severe TBI (STBI) is a leading cause of morbidity and mortality among young adults in the developing world, causing an immense socioeconomic burden.[7]
Computed tomography (CT) provides an early and reliable method of identifying an intracranial lesion; therefore, CT findings significantly predict the outcome. It may be necessary to repeat the scan when required, correlating it with the patient's clinical condition, as hematomas may evolve with increasing mass effects and the appearance of new lesions is not uncommon.[8]
The leading cause of TBIs worldwide is road traffic accidents (RTAs), followed by falls from height and violence. In developing countries like India, nonuse of helmets is a significant risk factor for TBIs.[9] [10] Outcome prediction models derived from studies in developed countries may not fit well in developing countries like India. As a resource-constrained country, India requires predictive models focusing on its needs and facilities.[11] A review of 55 studies found that helmet use reduced the risk of TBIs by 53%.[12] Additionally, approximately 15 to 20% of TBI patients are found to be under the influence of alcohol at the time of injury, posing a significant health burden.[11]
India, along with other developing countries, faces key challenges in trauma prevention, transportation from the site of injury to the hospital, prehospital care, and rehabilitation.[13] [14] These challenges need to be addressed to reduce the impact of TBIs on their population. The text focuses on the prognostic factors in STBIs.
This study aimed to investigate the predictors of mortality/morbidity in operated cases of isolated STBI based on their clinical presentation, management based on surgical indications, and the procedure followed. Moreover, surgical complications during the hospital stay and outcomes of patients at various intervals, up to 6 months, using the Glasgow Outcome Scale (Extended) (GOS-E) were examined.
Materials and Methods
Patient Population
This prospective observational study was conducted on 351 patients with severe head injuries admitted to the Department of Neurosurgery from July 2021 to June 2022. Of these, 227 patients underwent surgical intervention and 132 were managed medically. The above 227 patients were included in the study and followed for the course of their illness. Thirty-two patients acquired leave against medical advice (LAMA) following surgical intervention owing to the loss of hope of improvement or lack of monetary funds for further treatment. In the present study, patients with STBI (Glasgow Coma Scale [GCS] ≤ 8) who underwent surgical evacuation of the lesion were admitted and followed up for a minimum of 6 months. Patients' attendants who were unwilling to participate in the study, patients with other significant torso injuries (chest injury, abdominal trauma, spine injury, pelvic injury), and patients with GCS-E1V1M1 and absent brainstem reflexes were excluded from the study.
Clinical Assessments
History was obtained and a detailed neurological examination was done. Radiologically, a noncontrast CT head was done to look for the type of intracranial injury. Surgical management was done according to type and indications. During the postoperative period, the requirements of intensive care unit, or ventilatory support, were tabulated, and complications such as surgical site infection, wound dehiscence, cerebral spinal fluid leakage, urinary tract infection, respiratory tract infection, deep vein thrombosis, and reexploration were noted.
Outcomes Measure
The severity of TBI was defined according to the GCS of patients at admission and after resuscitation; a score of 13 to 15 was considered mild TBI, 9 to 12 as moderate TBI, and ≤ 8 as STBI. The outcome of patients was based on the GOS-E. The GOS-E scale included the following: 8 = upper good recovery, 7 = low good recovery, 6 = upper moderate disability, 5 = low, moderate disability, 4 = upper severe disability, 3 = low severe disability, 2 = persistent vegetative status, and 1 = death. Further, patients with GOS-E 7 to 8 had been classified as having good outcomes and GOS-E- 1 to 6 as poor outcomes.
Statistical Analysis
Statistical analysis was performed using the SPSS software (SPSS Inc., Chicago, Illinois, United States) for Windows program (21.0 version). The dichotomous variables were presented in number/frequency. The chi-square test and Student's t-test were used to calculate the clinical outcomes. The Cox regression (univariate and multivariate) analysis was used to find the influencing factors. A p-value of < 0.05 was considered statistically significant.
Results
Demographic and Clinicoradiological Characteristics: Predicting Outcomes in Operated STBI Patients
The study involved 227 patients with STBI who underwent surgery. The mean age of patients in the good outcome group was slightly lower than the poor outcome group (37.89 ± 16.98 vs. 41.98 ± 15.23 years, p = 0.057). Most patients were male (83.70%).
The most common cause of injury was RTAs (79.3%), but the mode of injury did not impact the outcome (p = 0.684). Most patients belonged to the lower and lower middle socioeconomic status (SES), with a significant association between low SES and poor outcomes (p = 0.0007). A significant correlation was found between alcohol intake and final outcome of patients (p < 0.0001).
Patients with a low presenting GCS were significantly associated with poor outcomes (p = 0.011). Abnormal pupillary reaction was significantly associated with poor outcomes (p = 0.002). Lower pulse rate, systolic blood pressure (SBP), and diastolic blood pressure (DBP) were also significantly associated with poor outcomes (p = 0.041, p = 0.016, and p < 0.0001, respectively). Comorbidities were not associated with outcome (p = 0.99). Midline shift (MLS) was significantly associated with outcome (p = 0.01). The type of injury on CT head had no significant statistical correlation with the outcome (p = 0.331).
Operative Procedures and Their Impact on Outcomes in STBI Patients
These patients underwent the following operative procedures: decompressive craniectomy (DECRA), craniotomy, and debridement craniectomy. Among these 227 patients, 126 (55.50%) underwent a DECRA, 81 (35.68%) patients underwent a craniotomy with evacuation of extradural hematoma (EDH)/subdural hematoma (SDH)/parenchymal hematoma, and 20 (8.82%) patients underwent a debridement craniectomy ([Table 2]). The patients undergoing a debridement craniectomy included those with a compound skull fracture with underlying intradural pathology requiring evacuation. In these patients, debridement of the scalp wound and small pieces of infected bone was done. The survival of the patients was significantly associated with the operative procedure, with proportional mortality of 63.7% among the DECRA group, 28.9% among the craniotomy group, and 7.4% among the debridement craniectomy group (p = 0.012).
|
Demographical variables |
All patients (N = 227) N (%) |
Clinical outcome |
p-Value |
|
|---|---|---|---|---|
|
Good outcome (n = 79), N (%) |
Poor outcome (n = 148), N (%) |
|||
|
Mean age (y), mean ± SD |
36.17 ± 17.43 |
37.89 ± 16.98 |
41.98 ± 15.23 |
0.057 |
|
Gender |
0.671 |
|||
|
Male |
190 (83.7) |
65 (82.3) |
125 (84.4) |
|
|
Female |
37 (16.3) |
14 (17.7) |
23 (15.5) |
|
|
Mode of injury |
0.670 |
|||
|
Road accident |
180 (79.3) |
64 (81.0) |
116 (78.4) |
|
|
Machinery injury |
2 (0.9) |
1 (1.3) |
1 (0.7) |
|
|
Fall |
32 (14.1) |
8 (10.1) |
24 (16.2) |
|
|
Assault |
11 (4.8) |
5 (6.3) |
6 (4.0) |
|
|
Slip |
2 (0.9) |
1 (1.3) |
1 (0.7) |
|
|
SES |
0.001[a] |
|||
|
Lower |
58 (25.5) |
10 (12.7) |
48 (32.4) |
|
|
Upper lower |
29 (12.8) |
8 (10.1) |
21 (14.2) |
|
|
Lower middle |
103 (45.4) |
37 (46.8) |
66 (44.6) |
|
|
Upper middle |
35 (15.4) |
23 (29.1) |
12 (8.1) |
|
|
Upper |
2 (0.9) |
1 (1.3) |
1 (0.7) |
|
|
Residence |
0.227 |
|||
|
Rural |
158 (69.6) |
51 (64.6) |
107 (72.3) |
|
|
Urban |
69 (30.4) |
28 (35.4) |
41 (27.7) |
|
|
Alcohol |
< 0.0001[a] |
|||
|
Yes |
101 (44.5) |
10 (12.7) |
91 (61.5) |
|
|
No |
126 (55.5) |
69 (87.3) |
57 (38.5) |
|
|
Clinicoradiological parameters |
||||
|
GCS score |
0.011[a] |
|||
|
3–4 |
61 (26.8) |
8 (10.1) |
53 (35.8) |
|
|
5 |
48 (21.1) |
13 (16.4) |
35 (23.6) |
|
|
6 |
42 (18.5) |
14 (17.7) |
28 (18.9) |
|
|
7 |
26 (11.5) |
9 (11.4) |
17 (11.6) |
|
|
8 |
50 (22.0) |
35 (44.3) |
15 (10.1) |
|
|
Pupillary reaction |
0.002[a] |
|||
|
Both fixed |
67 (29.5) |
14 (17.70) |
53 (35.8) |
|
|
One reacting |
45 (19.8) |
13 (16.4) |
32 (21.6) |
|
|
Both reacting |
115 (50.6) |
52 (65.8) |
63 (42.6) |
|
|
Vitals (mean ± SD) |
0.041[a] 0.016[a] < 0.0001[a] 0.078 |
|||
|
Pulse rate (beats/min) |
92.0 ± 20.4 |
90.0 ± 19.0 |
88.0 ± 17.8 |
|
|
SBP (mm Hg) |
122.4 ± 21.6 |
118.4 ± 20.2 |
112.6 ± 15.8 |
|
|
DBP (mm Hg) |
74.25 ± 11.4 |
70.9 ± 10.2 |
62.8 ± 9.2 |
|
|
Respiratory rate (/min) |
22.9 ± 5.1 |
20.2 ± 4.5 |
19.3 ± 3.1 |
|
|
Comorbidities |
0.995 |
|||
|
DM |
13 (5.7) |
5 (6.3) |
8 (5.4) |
|
|
Hypertension |
17 (7.5) |
6 (7.6) |
11 (7.4) |
|
|
DM + HTN |
8 (3.5) |
3 (3.8) |
5 (3.4) |
|
|
Seizure disorder |
2 (0.9) |
1 (1.3) |
1 (0.7) |
|
|
CKD |
3 (1.3) |
1 (1.3) |
2 (1.4) |
|
|
MLS (mm) |
0.010[a] |
|||
|
0–5 |
70 (30.8) |
29 (36.7) |
41 (27.7) |
|
|
5–10 |
78 (34.4) |
16 (20.2) |
62 (42.0) |
|
|
10–15 |
60 (26.4) |
27 (34.2) |
33 (22.3) |
|
|
15–20 |
19 (8.4) |
7 (8.9) |
12 (8.1) |
|
|
Cistern obliteration |
0.087 |
|||
|
Absent |
89 (39.2) |
34 (43.1) |
55 (37.2) |
|
|
Compromised |
124 (54.6) |
37 (46.8) |
87 (58.8) |
|
|
Normal |
14 (6.2) |
8 (10.1) |
6 (4.0) |
|
|
CT findings |
0.331 |
|||
|
Contusion |
69 (30.4) |
27 (34.1) |
42 (28.4) |
|
|
EDH |
47 (20.7) |
20 (25.3) |
27 (18.2) |
|
|
SDH |
29 (12.7) |
10 (12.6) |
19 (12.8) |
|
|
Mixed lesion (SDH + contusion) |
80 (35.2) |
21 (26.6) |
59 (39.9) |
|
|
Comminuted skull fracture with brain matter leak |
2 (0.8) |
1 (1.3) |
1 (0.7) |
|
Abbreviations: CKD, chronic kidney disease; CT, computed tomography; DBP, diastolic blood pressure; DM, diabetes mellitus; HTN, hypertension; EDH, extradural hematoma; GCS, Glasgow Coma Scale; MLS, midline shift; SBP, systolic blood pressure; SD, standard deviation; SDH, subdural hematoma; SES, socioeconomic status; TBI, traumatic brain injury.
Note: Patients with Glasgow Outcome Scale (Extended) (GOS-E)- 7 to 8 were classified as having good outcomes and GOS- 1 to 6 as poor outcomes. The chi-square test and Student's t-test were used to calculate the p-value between the clinical outcomes.
a p-Value < 0.05 was considered statistically significant.
Abbreviation: TBI, traumatic brain injury.
a pa < 0.05 is considered as significant.
One of the common intraoperative complications was severe brain bulge leading to a mass closure in 18 patients, out of which 14 (77.8%) patients expired. The common radiological features among the patients undergoing a mass closure due to malignant bulge had mixed lesions, a MLS of more than 10 mm, and an obliterated basal cistern on CT head. Sinus bleed was encountered in 7 patients, of which 6 (85.7%) patients expired. These patients were found to have a skull bone fracture with a superior sagittal sinus or a transverse sinus bleed intraoperatively and were associated with EDH in 2 patients and mixed lesions in 3 patients. Two of these patients had a depressed bone fracture over the sagittal sinus. A difficult dural closure was encountered in 15 patients due to the shattering of dura owing to the skull base fracture and was managed with pericranial patch/tensor fascia lata patch and glue, among which 5 (33.3%) patients expired. This suggested that intraoperative mass closure and sinus bleeding had a significantly poor impact on the final outcome (p = 0.011) of patients with STBI undergoing surgical intervention. Lobectomy (frontal/temporal) was performed in burst lobe, causing a significant mass effect in 42 patients. It was statistically compared with 91 other patients with lobar contusions not undergoing lobectomy. We observed that lobectomy did not have a significant impact on the outcome of patients ([Table 2]).
Postoperative Incidence of In-Hospital Issues during Hospital Stay Associated with Survival of Patients
This study comprises 227 patients of STBI undergoing surgical intervention. Among these patients, 103 (45.37%) had an in-hospital mortality and 92 (40.53%) were discharged alive and stable. Thirty-two (14.1%) patients took LAMA. The 32 patients who went LAMA expired either on the same day or the next day after leaving the hospital. The cumulative mortality in this study, including the LAMA patients, was 135 (59.47%).
Among the in-hospital expiry group, an expiry within 7 days was attributed to cranial cause, and any mortality after that was considered due to extracranial pathology. In this study, of the 135 expired patients, 100 (74.04%) patients expired within 7 days and 35 (25.9%) patients expired after 7 days of surgery, possibly expiring due to noncranial causes like ventilator-associated pneumonia.
Most patients developed respiratory tract infections during their hospital stay, with Acinetobacter baumannii being the most common pathological organism identified in culture specimens. Tracheostomy, respiratory tract infection, bedsore, meningitis, deep vein thrombosis, cerebrospinal fluid leak, and bone flap site infection (p = 0.034) during hospital stay were significantly associated with poor outcomes of patients ([Table 3]).
Abbreviations: CSF, cerebrospinal fluid; CT, computed tomography; DBP, diastolic blood pressure; DVT, deep vein thrombosis; MCA, middle cerebral artery; PCA, posterior cerebral artery; RTI, respiratory tract infection; SBP, systolic blood pressure.
The 92 discharged patients were followed up telephonically and in the outpatient department and we noted further that 17 patients expired after discharge from the hospital and 10 patients were lost to follow-up due to wrong contact details provided.
Four (23.5%) patients were readmitted within 1 month of discharge with severe pneumonia and succumbed to respiratory failure. The mortality of patients during home care was followed telephonically and the possible causes were studied. We found that tracheostomy-related complications, including difficulty reinserting the tracheostomy tube during routine care, were the most common cause of mortality, as stated by the attendants of 5 (29.41%) patients. Other causes included respiratory tract infection in 2 (15.40%), status epilepticus among 2 (15.40%), bone flap site infection leading to sepsis in 1 (7.70%), and 3 (23.10%) patients expired due to unidentified cause of death. All these patients who expired during home care belonged to the lower SES and care of the comatose was a limiting factor in the outcome.
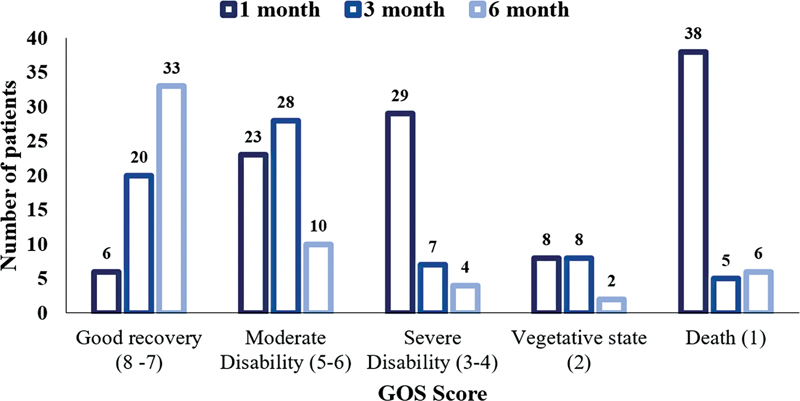
In a study of 227 patients, the GOS-E scale scores were tracked over 6 months. Initially, most patients had moderate to severe disability or had passed away. Only 0.46% showed good recovery. Good recovery increased to 32.46% by the third month, and moderate disability to 49.35%. Severe disability and death decreased to 5.19 and 7.79%, respectively. By the sixth month, 63.38% had good recovery, with few remaining in severe disability, vegetative state, or death categories ([Fig. 1]). The percentages may not total 100% due to category shifts during the study, emphasizing the need for continuous monitoring and reassessment ([Table 4]).
Abbreviation: TBI, traumatic brain injury.
Note: The table presents data from a study using the Glasgow Outcome Scale Extended (GOS-E) score, ranging from 1 to 8. The number and percentage of patients in each category (good recovery, moderate disability, severe disability, vegetative state, and death) are tracked over three time periods: 1, 3, and 6 months. Percentages may not total 100% due to patients shifting categories during the study, underscoring the importance of continuous monitoring and reassessment.
|
Variables |
Univariate Chi-square (95% CI) |
Univariate p-Value |
Multivariate Chi-square (CI) (95% CI) |
Multivariate p-Value |
|---|---|---|---|---|
|
Age (y) |
9.35 (1.01–1.03) |
0.002[a] |
9.12 (1.01–1.02) |
0.005[a] |
|
Gender |
0.598 (0.44–1.42) |
0.439 |
− |
− |
|
Residency |
1.44 (0.85–1.95) |
0.230 |
− |
− |
|
SES |
1.36 (0.84–1.91) |
0.242 |
− |
− |
|
MOI |
1.06 (0.95–1.18) |
0.303 |
− |
− |
|
Alcohol use |
12.37 (1.87–108.29) |
0.006[a] |
11.23 (1.18–71.68) |
0.034[a] |
|
GCS score |
28.60 (0.60–0.79) |
< 0.0001[a] |
26.69 (0.59–0.80) |
< 0.0001[a] |
Abbreviations: CI, confidence interval; GCS, Glasgow Coma Scale; SES, socioeconomic status; MOI, Mode of injury.
Note: Cox regression analysis was used to calculate the univariate and multivariate analysis.
a p-Value < 0.05 was considered as statistically significant.
Independent Factors Influencing Outcomes in STBI Patients Undergoing Surgical Intervention
Three independent factors significantly influence outcomes in patients with STBI undergoing surgical intervention. First, increasing patient age positively correlates with worse outcomes, with a statistically significant odds ratio (OR) of 9.12 (95% confidence interval [CI]: 1.01–1.02, p = 0.005). Second, trauma following alcohol use was associated with poorer outcomes, as indicated by an OR of 11.2 (95% CI: 1.18–71.68, p = 0.034). Third, a lower GCS score, indicative of more severe injury, is significantly associated with poor outcomes (OR: 26.69, 95% CI: 0.59–0.80, p < 0.0001). These factors are considered independent in their effect on patient outcomes ([Table 5]).
Discussion
A developing country still faces challenges in providing primary resources at the site of injury, during transport, and even during hospital admissions, such as intensivists, ventilator support, and a multidisciplinary team for managing patients with STBI. In this context, obtaining specific data to establish the most effective methods for delivering surgical care and predicting outcomes for traumatic neurological injuries is crucial. Describing the epidemiological and clinical factors associated with outcomes in different settings is crucial in managing patients with TBI in neurosurgical care.
Our data demonstrated that most patients sustained a RTA followed by fall from height and assault. The most common mode of injury demonstrated in various studies conducted worldwide has been RTA, owing to the rapid urbanization and motorization of human transport. Still, among the pediatric age group, fall from height remains the predominant mode of injury, as observed in our study.[15] [16] Most head injuries occurred due to not wearing helmets, driving under the influence of alcohol, overspeeding, and overtaking, and were considered the major behavioral factors responsible for high rates of RTA in our country. The high proportion of patients with a history of alcohol intake before trauma suggests the impact of alcohol on the state of mind and sluggishness of reflexes while driving on the road, significantly increasing the risk factor for sustaining trauma and associated with poor outcomes.[17] [18]
The patients in the study were grouped based on the Kuppuswamy scale for their SES.[19] The present finding demonstrated that our center had significantly higher admission rates for low and middle-class patients than the upper class. This disparity is attributed to the high proportion of rural, illiterate, and poor patients presenting to our hospital. Hence, a poorer outcome is observed in this group of patients owing to multifactorial reasons like delay in hospitalization and lack of basic neurosurgical facilities at the primary caregiving hospitals. Moreover, we found that the mortality at-home care was higher among the lower socioeconomic class, demonstrating a lack of proper home care for comatose in these families.
The GCS score on admission is the most important factor that independently predicts the outcome of patients with severe head injuries. A proper evaluation of the GCS score is of utmost importance and can be confounded by factors leading to unconsciousness like hypotension, hypoglycemia, and being under the influence of alcohol. Moreover, GCS on presentation combined with CT head findings clears the mist around the prediction of the outcome of STBI patients.[20] Our data revealed that GCS at admission was the most important independent factor that can predict the outcome of patients.
Ritter et al[21] found a bilateral pupillary dilation associated with decreased cerebral blood flow and ischemia rather than mechanical compression of the third cranial nerve. This may indicate mid-brain ischemia and poor outcome at 12 months. The above study found that bilaterally nonreacting pupils had poor outcomes, with 63.07% mortality rates and 51.1% mortality in single-reacting pupils. A similar finding was observed in our study, that an abnormal pupillary reaction was significantly associated with poorer outcomes.
The initial recorded low pulse rate, low SBP, and low DBP on presentation were significantly associated with poor outcome of the STBI patients. Although there is no doubt that early resuscitation of hypotension alters the outcome, it is well established that there are better factors for predicting poor outcomes and mortality in trauma patients in the emergency room.
Preoperative factors found inextricably linked to poor outcome in our prospective study of severe head injury patients undergoing surgical intervention include low SES, low GCS (3–5) on presentation, abnormal pupillary reaction, persisting bradycardia and hypotension postresuscitation, and MLS > 15 mm on CT head. Although obliterated basal cisterns and mixed lesions (SDH + contusion) on CT head were associated with higher mortality rates, their statistical significance was not found.[22] A study on 216 head injury cases by Chiewvit et al in 2010 compared MLS on CT with the outcome and concluded a poor clinical outcome with MLS greater than 10 mm.[23] In a study published in All India Institute of Medical Sciences in 1991–92 on 18 severe head injury patients, patients with single lesions on CT had better outcomes (60.6% survival) than those with multiple lesions (42.2% survival).[24] Our findings are similar to the above findings. Intraoperative factors associated with poor outcomes in this study included mass closure and sinus bleeding. Patients undergoing a DECRA overall had an unfavorable outcome as compared with patients undergoing a craniotomy, although it can be related to the fact that patients undergoing DECRA had a lower preoperative GCS besides more mass effect and severe injury to the brain; our finding is consistent with Coplin et al[25] and Chen et al, demonstrating a poorer outcome among the patients undergoing DECRA.[26]
The common factors responsible for a poor outcome of patients in the postoperative period include respiratory tract infections and deep vein thrombosis. Although lack of ventilatory support availability in the immediate postoperative period was found to be a limiting factor in the appropriate goal-oriented management of severe head injury patients, these lacunae were not a significant factor in impacting the final outcome of these patients in this study. These patients were managed on Bain's circuit ventilation until ventilator support could be arranged. Since these patients require aggressive intensive care, the lack of such facilities can alter the outcome and need detailed evaluation.
Our findings advocate that age, alcohol use, and GCS are independent predictors of survival of patients with STBI. Hukkelhoven et al found that patients younger than 35 years had a 21% mortality rate and 39% adverse outcome, while those over 55 had a 52% mortality rate and 74% unfavorable outcome.[27] Advanced age is linked to a deteriorating outcome in severe head injuries.[28] Tien et al found that high blood alcohol concentration was associated with a higher mortality rate.[19] A similar study conducted by Ogunlade et al on severe head injury patients undergoing surgical intervention demonstrated a highly significant correlation between the presenting GCS and the outcome of patients representing a poor outcome among patients of low GCS (3–5). The most impactful factor as a predictor of mortality was found to be preoperative GCS.[29] The most important single factor that can be used for prognostication of the attendants in TBI would be the presenting GCS, and the patients with a GCS of 3 or 4 can be considered to have a grave prognosis.
In this study, we observed that the patients with a good recovery escalated from 0.46% at the 1-month follow-up to an astounding improvement of 63.38% on the 6-month follow-up. A similar finding was observed by Wilkins et al where 46% of the survivors had a favorable outcome and 74% of surviving adults with a documented GOS-E at 2 years after injury had a favorable outcome, demonstrating a significant improvement of mean GOS-E from 3 months to 2-year follow-up.[30]
The rehabilitation process involves the disabled person and their family, where they must go beyond the confines of physical disease and deal with the psychological consequences of physical disability. The recovery curve is steepest in the first 3 months after injury and it is important to capitalize as much as possible on this phase of rapid improvement. The rehabilitation process faces a major setback in a center with most patients of lower socioeconomic backgrounds. Upfront education on physiotherapy and care of the bedridden psychological motivation on improving such patients brings about a behavioral change among the attendants and improves outcomes.
This study has some limitations. First, excluding polytrauma cases may limit the applicability of the findings to other STBI patients with multiple injuries. Second, relying on the GCS and GOS-E might not fully capture the range of neurological impairments and functional outcomes in STBI patients. Third, conducting the study in a single center with limited resources could affect the quality of care and availability of interventions for STBI patients. Lastly, the relatively small sample size and short follow-up period might reduce the statistical power and its ability to detect the long-term effects of STBI. These limitations should be taken into account for future study.
Conclusion
TBIs are a leading cause of morbidity, mortality, disability, and socioeconomic losses in India. Awareness, education, and stringent road safety laws need to be implemented to reduce the incidence of TBI. GCS score should be considered the primary tool for triaging the patients for early investigation and management. Moreover, GCS on presentation combined with CT head findings clears the mist around the prediction of the outcome of patients. This helps considerably for appropriate counseling of the attendants. Preoperative factors found inextricably linked to poor outcome in our prospective study of severe head injury patients undergoing surgical intervention includes advancing age, low GCS (3–5) on presentation, obliterated basal cisterns, MLS > 15 mm, and mixed lesions (SDH + contusion) on CT head. Hence, this study provides a baseline for the clinician to predict the prognosis on admission, anticipate the postoperative course of recovery, tackle the management challenges, counsel the caregivers regarding the pitfalls and pearls of home care, and prophesize these patients' long-term outcomes.
Conflict of Interest
None declared.
Ethical Approval
The institutional ethical committee approved this study (Ref. code: VII-PGTSC-IIA/P7). It adhered to the principles of the Declaration of Helsinki. Before enrolment, all participants provided written informed consent. A structured form was used to gather each participant's medical, personal, and historical information.
Authors' Contributions
A.C. was responsible for conceptualization, methodology, and supervision. B.K.O. contributed to validation and formal analysis. C.S. managed resources and data curation, while S.J. provided resources and handled software. A.S. was involved in investigation, data curation, writing – review and editing, and visualization.
-
References
- 1 James SL, Theadom A, Ellenbogen RG. et al; GBD 2016 Traumatic Brain Injury and Spinal Cord Injury Collaborators. Global, regional, and national burden of traumatic brain injury and spinal cord injury, 1990-2016: a systematic analysis for the Global Burden of Disease Study 2016. Lancet Neurol 2019; 18 (01) 56-87
- 2 Esposito TJ, Reed II RL, Gamelli RL, Luchette FA. Neurosurgical coverage: essential, desired, or irrelevant for good patient care and trauma center status. Ann Surg 2005; 242 (03) 364-370 , discussion 370–374
- 3 Botman M, Meester RJ, Voorhoeve R. et al. The Amsterdam declaration on essential surgical care. World J Surg 2015; 39 (06) 1335-1340
- 4 Mock CN, Donkor P, Gawande A, Jamison DT, Kruk ME, Debas HT. DCP3 Essential Surgery Author Group. Essential surgery: key messages from Disease Control Priorities, 3rd edition. Lancet 2015; 385 (9983): 2209-2219
- 5 MacKenzie EJ. Epidemiology of injuries: current trends and future challenges. Epidemiol Rev 2000; 22 (01) 112-119
- 6 Sobrino J, Shafi S. Timing and causes of death after injuries. Proc Bayl Univ Med Cent 2013; 26 (02) 120-123
- 7 Langlois JA, Rutland-Brown W, Wald MM. The epidemiology and impact of traumatic brain injury: a brief overview. J Head Trauma Rehabil 2006; 21 (05) 375-378
- 8 Marshall LF. Head injury: recent past, present, and future. Neurosurgery 2000; 47 (03) 546-561
- 9 Murray CJ, Lopez AD. Global mortality, disability, and the contribution of risk factors: Global Burden of Disease Study. Lancet 1997; 349 (9063): 1436-1442
- 10 Dhandapani S, Mukherjee KK. Outcome prediction in traumatic brain injury: is it a “Holy Grail?”. Neurol India 2017; 65 (01) 87-88
- 11 Høye A. Bicycle helmets - To wear or not to wear? A meta-analyses of the effects of bicycle helmets on injuries. Accid Anal Prev 2018; 117: 85-97
- 12 Gururaj G. Epidemiology of traumatic brain injuries: Indian scenario. Neurol Res 2002; 24 (01) 24-28
- 13 Marehbian J, Muehlschlegel S, Edlow BL, Hinson HE, Hwang DY. Medical management of the severe traumatic brain injury patient. Neurocrit Care 2017; 27 (03) 430-446
- 14 Fong R, Konakondla S, Schirmer CM, Lacroix M. Surgical interventions for severe traumatic brain injury. J Emerg Crit Care Med 2017; 1 (10) 28
- 15 Powell J, Heslin J, Greenwood R. Community based rehabilitation after severe traumatic brain injury: a randomised controlled trial. J Neurol Neurosurg Psychiatry 2002; 72 (02) 193-202
- 16 Ravi D, Sinha A, Sinha A. Analysis of prognostic factors and post operative outcome of decompressive craniectomy for traumatic brain injury: study at a government hospital. Int J 2021; 4 (05) 641
- 17 Araki T, Yokota H, Morita A. Pediatric traumatic brain injury: characteristic features, diagnosis, and management. Neurol Med Chir (Tokyo) 2017; 57 (02) 82-93
- 18 Salim A, Teixeira P, Ley EJ, DuBose J, Inaba K, Margulies DR. Serum ethanol levels: predictor of survival after severe traumatic brain injury. J Trauma 2009; 67 (04) 697-703
- 19 Tien HC, Tremblay LN, Rizoli SB. et al. Association between alcohol and mortality in patients with severe traumatic head injury. Arch Surg 2006; 141 (12) 1185-1191 , discussion 1192
- 20 Wani RT. Socioeconomic status scales-modified Kuppuswamy and Udai Pareekh's scale updated for 2019. J Family Med Prim Care 2019; 8 (06) 1846-1849
- 21 Ritter AM, Muizelaar JP, Barnes T. et al. Brain stem blood flow, pupillary response, and outcome in patients with severe head injuries. Neurosurgery 1999; 44 (05) 941-948
- 22 Ono J, Yamaura A, Kubota M, Okimura Y, Isobe K. Outcome prediction in severe head injury: analyses of clinical prognostic factors. J Clin Neurosci 2001; 8 (02) 120-123
- 23 Chiewvit P, Tritakarn SO, Nanta-aree S, Suthipongchai S. Degree of midline shift from CT scan predicted outcome in patients with head injuries. J Med Assoc Thai 2010; 93 (01) 99-107
- 24 Mahapatra AK, Kamal R, Kumar R. Textbook of Traumatic Brain Injury. JP Medical Ltd, 83 Victoria St.London SW1H. ISBN 978–93–80704–76–0. Chapter 22. pg 145, 146
- 25 Coplin WM, Cullen NK, Policherla PN. et al. Safety and feasibility of craniectomy with duraplasty as the initial surgical intervention for severe traumatic brain injury. J Trauma 2001; 50 (06) 1050-1059
- 26 Chen SH, Chen Y, Fang WK, Huang DW, Huang KC, Tseng SH. Comparison of craniotomy and decompressive craniectomy in severely head-injured patients with acute subdural hematoma. J Trauma 2011; 71 (06) 1632-1636
- 27 Hukkelhoven CW, Steyerberg EW, Rampen AJ. et al. Patient age and outcome following severe traumatic brain injury: an analysis of 5600 patients. J Neurosurg 2003; 99 (04) 666-673
- 28 Luerssen TG, Klauber MR, Marshall LF. Outcome from head injury related to patient's age. A longitudinal prospective study of adult and pediatric head injury. J Neurosurg 1988; 68 (03) 409-416
- 29 Ogunlade J, Elia C, Duong J. et al. Severe traumatic brain injury requiring surgical decompression in the young adult: factors influencing morbidity and mortality - a retrospective analysis. Cureus 2018; 10 (07) e3042
- 30 Wilkins TE, Beers SR, Borrasso AJ. et al. Favorable functional recovery in severe traumatic brain injury survivors beyond six months. J Neurotrauma 2019; 36 (22) 3158-3163
Address for correspondence
Publikationsverlauf
Artikel online veröffentlicht:
04. Juni 2024
© 2024. The Author(s). This is an open access article published by Thieme under the terms of the Creative Commons Attribution License, permitting unrestricted use, distribution, and reproduction so long as the original work is properly cited. (https://creativecommons.org/licenses/by/4.0/)
Thieme Medical and Scientific Publishers Pvt. Ltd.
A-12, 2nd Floor, Sector 2, Noida-201301 UP, India
-
References
- 1 James SL, Theadom A, Ellenbogen RG. et al; GBD 2016 Traumatic Brain Injury and Spinal Cord Injury Collaborators. Global, regional, and national burden of traumatic brain injury and spinal cord injury, 1990-2016: a systematic analysis for the Global Burden of Disease Study 2016. Lancet Neurol 2019; 18 (01) 56-87
- 2 Esposito TJ, Reed II RL, Gamelli RL, Luchette FA. Neurosurgical coverage: essential, desired, or irrelevant for good patient care and trauma center status. Ann Surg 2005; 242 (03) 364-370 , discussion 370–374
- 3 Botman M, Meester RJ, Voorhoeve R. et al. The Amsterdam declaration on essential surgical care. World J Surg 2015; 39 (06) 1335-1340
- 4 Mock CN, Donkor P, Gawande A, Jamison DT, Kruk ME, Debas HT. DCP3 Essential Surgery Author Group. Essential surgery: key messages from Disease Control Priorities, 3rd edition. Lancet 2015; 385 (9983): 2209-2219
- 5 MacKenzie EJ. Epidemiology of injuries: current trends and future challenges. Epidemiol Rev 2000; 22 (01) 112-119
- 6 Sobrino J, Shafi S. Timing and causes of death after injuries. Proc Bayl Univ Med Cent 2013; 26 (02) 120-123
- 7 Langlois JA, Rutland-Brown W, Wald MM. The epidemiology and impact of traumatic brain injury: a brief overview. J Head Trauma Rehabil 2006; 21 (05) 375-378
- 8 Marshall LF. Head injury: recent past, present, and future. Neurosurgery 2000; 47 (03) 546-561
- 9 Murray CJ, Lopez AD. Global mortality, disability, and the contribution of risk factors: Global Burden of Disease Study. Lancet 1997; 349 (9063): 1436-1442
- 10 Dhandapani S, Mukherjee KK. Outcome prediction in traumatic brain injury: is it a “Holy Grail?”. Neurol India 2017; 65 (01) 87-88
- 11 Høye A. Bicycle helmets - To wear or not to wear? A meta-analyses of the effects of bicycle helmets on injuries. Accid Anal Prev 2018; 117: 85-97
- 12 Gururaj G. Epidemiology of traumatic brain injuries: Indian scenario. Neurol Res 2002; 24 (01) 24-28
- 13 Marehbian J, Muehlschlegel S, Edlow BL, Hinson HE, Hwang DY. Medical management of the severe traumatic brain injury patient. Neurocrit Care 2017; 27 (03) 430-446
- 14 Fong R, Konakondla S, Schirmer CM, Lacroix M. Surgical interventions for severe traumatic brain injury. J Emerg Crit Care Med 2017; 1 (10) 28
- 15 Powell J, Heslin J, Greenwood R. Community based rehabilitation after severe traumatic brain injury: a randomised controlled trial. J Neurol Neurosurg Psychiatry 2002; 72 (02) 193-202
- 16 Ravi D, Sinha A, Sinha A. Analysis of prognostic factors and post operative outcome of decompressive craniectomy for traumatic brain injury: study at a government hospital. Int J 2021; 4 (05) 641
- 17 Araki T, Yokota H, Morita A. Pediatric traumatic brain injury: characteristic features, diagnosis, and management. Neurol Med Chir (Tokyo) 2017; 57 (02) 82-93
- 18 Salim A, Teixeira P, Ley EJ, DuBose J, Inaba K, Margulies DR. Serum ethanol levels: predictor of survival after severe traumatic brain injury. J Trauma 2009; 67 (04) 697-703
- 19 Tien HC, Tremblay LN, Rizoli SB. et al. Association between alcohol and mortality in patients with severe traumatic head injury. Arch Surg 2006; 141 (12) 1185-1191 , discussion 1192
- 20 Wani RT. Socioeconomic status scales-modified Kuppuswamy and Udai Pareekh's scale updated for 2019. J Family Med Prim Care 2019; 8 (06) 1846-1849
- 21 Ritter AM, Muizelaar JP, Barnes T. et al. Brain stem blood flow, pupillary response, and outcome in patients with severe head injuries. Neurosurgery 1999; 44 (05) 941-948
- 22 Ono J, Yamaura A, Kubota M, Okimura Y, Isobe K. Outcome prediction in severe head injury: analyses of clinical prognostic factors. J Clin Neurosci 2001; 8 (02) 120-123
- 23 Chiewvit P, Tritakarn SO, Nanta-aree S, Suthipongchai S. Degree of midline shift from CT scan predicted outcome in patients with head injuries. J Med Assoc Thai 2010; 93 (01) 99-107
- 24 Mahapatra AK, Kamal R, Kumar R. Textbook of Traumatic Brain Injury. JP Medical Ltd, 83 Victoria St.London SW1H. ISBN 978–93–80704–76–0. Chapter 22. pg 145, 146
- 25 Coplin WM, Cullen NK, Policherla PN. et al. Safety and feasibility of craniectomy with duraplasty as the initial surgical intervention for severe traumatic brain injury. J Trauma 2001; 50 (06) 1050-1059
- 26 Chen SH, Chen Y, Fang WK, Huang DW, Huang KC, Tseng SH. Comparison of craniotomy and decompressive craniectomy in severely head-injured patients with acute subdural hematoma. J Trauma 2011; 71 (06) 1632-1636
- 27 Hukkelhoven CW, Steyerberg EW, Rampen AJ. et al. Patient age and outcome following severe traumatic brain injury: an analysis of 5600 patients. J Neurosurg 2003; 99 (04) 666-673
- 28 Luerssen TG, Klauber MR, Marshall LF. Outcome from head injury related to patient's age. A longitudinal prospective study of adult and pediatric head injury. J Neurosurg 1988; 68 (03) 409-416
- 29 Ogunlade J, Elia C, Duong J. et al. Severe traumatic brain injury requiring surgical decompression in the young adult: factors influencing morbidity and mortality - a retrospective analysis. Cureus 2018; 10 (07) e3042
- 30 Wilkins TE, Beers SR, Borrasso AJ. et al. Favorable functional recovery in severe traumatic brain injury survivors beyond six months. J Neurotrauma 2019; 36 (22) 3158-3163