

Subscribe to RSS
DOI: 10.1055/s-0044-1792173
Usefulness of Nerve Transposition in Tetraplegic Patients: A Clinical Case
Article in several languages: español | EnglishAuthors

Abstract
Spinal cord injury has an incidence of 40 new cases per million inhabitants, the most affected regions being the cervical and lumbar spine. In cervical injuries, the function most challenging to recover is control of the hand. Still, when the injury is above C5, the tendon surgical options are minimal, so nerve transfer is the remaining surgical option. Determining which transfer is going to be useful and when to do it is the point of discussion. More and more progress is being made in this line, as well as in the combination of tendon and nervous treatment.
Introduction
The incidence of spinal cord injury is 40 new cases per million inhabitants, 50% of which are due to traffic accidents and 25% to falls, and the most affected regions are the cervical and lumbar spine. Injury at the C5-C8 level often presents strong shoulder muscles, but it has no or weak control at the level of the elbow, wrist, forearm, and hand, depending on the level of injury.[1] Cervical spinal cord injury produces severe disability, and although it represents a small part of total patient care, it is very important.
The function of the hand is of utmost importance to obtain maximum independence in daily life. Therefore, restoration of arm and hand function is the highest priority.[2] The surgical reconstruction of the upper limb began in the 1950s but was popularized by Moberg in the 1970s through tendon transfers. To perform tendon transfers aimed at restoring hand function, active wrist extension is required, which means that the injury is below C5. This allows for the availability of several active muscles for transposition.
Building on experience with nerve transfers in peripheral nerve and brachial plexus surgery, the use of these techniques was proposed for the treatment of the tetraplegic hand. One critical factor is the preservation of the second motor neuron below the spinal cord injury. When the second motor neuron is preserved, nerve reconstruction is not constrained by the time elapsed since the injury, as it is in peripheral nerve injuries, where the second motor neuron segment is affected. In such cases, irreversible muscle atrophy develops around 12 to 18 months after denervation, making nerve transfers time sensitive. However, in spinal cord injuries, time may not be as critical for the reasons mentioned above. In nerve transfers for spinal injuries, the upper motor neuron connects to the intact lower motor neuron, meaning the procedure is not limited by time. We present the clinical case of a male patient who underwent nerve transfers to restore hand functionality.
Clinical Case
A 32-year-old man on June 26, 2021, presented trauma with an ASIA (American Spinal Injury Association) spinal cord injury at level C4. From a motor point of view, there is only the presence of brachioradialis with strength 5 on the right side and 4 on the left side (Medical Research Council, MRC Scale).
Within the international classification for quadriplegic hand surgery (International Classification for Surgery of the Hand in Tetraplegia, ICSHT), it would be type 1 ([Fig. 1]). From a surgical perspective, tendon transposition options would not be viable, except for a tendon transfer that provides elbow extension (posterior deltoid to triceps).

Performing nerve transfer surgery on the right upper limb is proposed together with the patient.
Before surgery, an electromyogram was performed which indicated the presence of motor units in the brachioradialis and the presence of mild denervation in the supinator, but with motor units.
A triple nerve transfer is planned to provide elbow extension, wrist and finger extension, and finger flexion dependent on the anterior interosseous nerve.
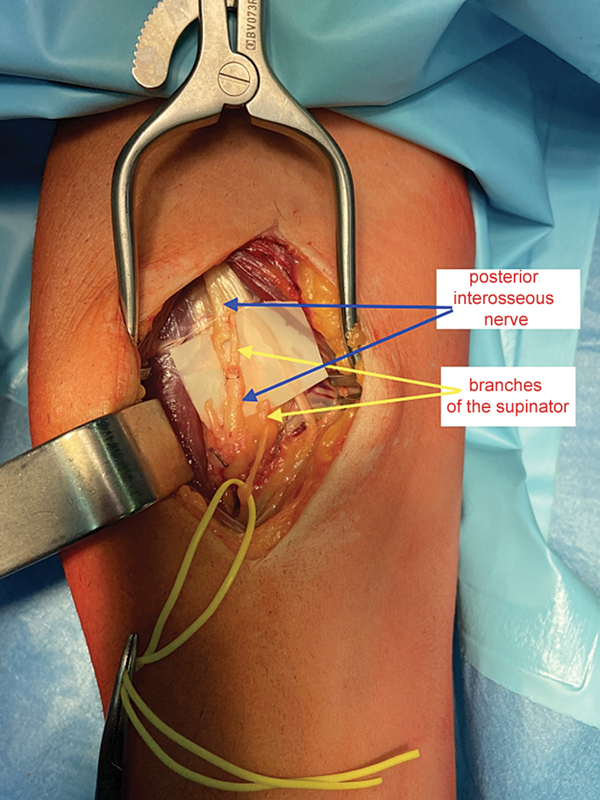
On March 2, 2022, this triple transfer was performed. A branch of the axillary nerve to teres minor is transferred to the triceps; branches of the musculocutaneous nerve to the brachialis are transferred to the fascicles of the anterior interosseous nerve of the median; and branches of the supinator are transferred to the posterior interosseous nerve. [Figs. 2] and [3]

After 15 days, the stitches and immobilizations are removed, and 4 weeks after the intervention, weight-bearing and the start of the rehabilitation protocol are authorized. Maintenance of articular arches and nervous stimulation of the muscles receiving nerve transfers. Stimulation of the triceps muscles, finger and thumb extensors, and finger flexors.
Results
3 months post-intervention, active wrist extension is evident, suggesting that the transfer from the supinator to the posterior interosseous nerve is functioning. However, no active function is observed in the triceps or hand flexors, likely due to the longer distance to the target nerves.
At 7 months, follow-up with electromyography (EMG) shows spontaneous activity in the triceps and extensor digitorum communis muscles. Motor unit potentials (MUPs) are recorded with increased amplitude in the extensor digitorum communis, but no MUPs are detected in the triceps.
At 9 months, wrist extensors score 4 on the MRC scale, and the extensor pollicis longus score 2. However, no activity is observed in the wrist or hand flexors, and triceps function remains questionable.
At 11 months, finger flexion begins to emerge, the thumb extension improves to 3, and finger extension reaches a score of 2.
At 15 months post-intervention, the wrist and finger extensors are at 4, and the thumb and finger flexor at 2. No motor activity is detected in the triceps.
The patient is very satisfied with the results and surgery on the contralateral limb is proposed and accepted, in which the triple nerve transfer will be added to the tendon transfer from the posterior deltoid to the triceps to achieve elbow extension.
Discussion
The recovery of arm and hand function in a quadriplegic patient is the highest priority above the function of walking, sphincter control, or the sexual sphere.[3] For 49% of patients, recovery of the hand is essential compared to those who prefer to recover another function, which stands at 13%.[3]
When cervical injuries are above C5, tendon options are practically non-existent and therefore cannot be performed. Taking advantage of the experience accumulated in surgery of the peripheral nerve and brachial plexus, nerve transfer surgery has been applied in these patients to give function to the hand and arm. Although it seems like a promising process, few quality studies support this treatment, although there is increasing acceptance of this.
The problem of delimiting which nerves can be used for the transfer is something that is being worked on, with the use of nerve conduction studies.[4]
Timing, patient selection, and long-term clinical outcomes remain unclear. There are even indications that when there are difficulties in evaluating whether an injury is of the upper or lower motor neuron, or there is a combination of both, the nerve transfer should be performed within 12 months after the injury.[5]
The challenge lies in determining which nerves are viable for transfer. In our case, surface electromyography was used to assess the presence of denervation, aiding in preoperative planning. Intraoperative direct stimulation was then employed to evaluate the response of the recipient muscle. In this patient, the transfer from the brachialis to the anterior interosseous nerve was the first to show function, followed by the transfer from the supinator to the posterior interosseous nerve. However, the transfer from the teres minor branch to the triceps remains uncertain.
This makes us propose two things: try to refine preoperative planning further by applying other electrodiagnostic studies, such as nerve conduction studies, looking at the compound muscle action potential, since the electromyogram in long-standing spinal cord injury can be distorted and the results not be completely reliable.[6] And on the other hand, associating tendon transfer with the nerve transfer, in cases where it is possible, such as providing extensor function to the triceps, in which apart from performing the nerve transfer of the axillary branch for the teres minor to the triceps, associating the posterior deltoid tendon transfer to triceps, in the attempt to ensure this function, there are already references of this possibility.[4]
The option of combining tendon and nerve transfers is a solution that is being increasingly considered. Not only in “reinforcement” situations[4], as would be our case, but also in which a tendon transfer could be used to perform a movement and add a nervous movement to achieve other movements and complement the function of the hand, adapting the tendon transfer to the degree and distribution of reinnervation achieved.[7]
Conclusion
Nerve transposition is a technique that can offer therapeutic options within surgical treatment that tendon transposition cannot provide, and it may even enhance the effectiveness of tendon transfers.
It is essential to continue with follow-up and the comprehensive treatment we are providing.
Conflicto de Intereses
No existe conflicto de intereses por parte de los autores indicados. Lidia Ledesma Galey, José Manuel Méndez López.
Han participado en la concepción y diseño, así como el análisis de los datos del trabajo
Han participado en la redacción del texto y en las posibles revisiones de este
Se ha aprobado la versión que se presenta para ser publicada.
-
Bibliografia
- 1 Javeed S, Dibble CF, Greenberg JK. et al. Upper Limb Nerve Transfer Surgery in Patients With Tetraplegia. JAMA Netw Open 2022; 5 (11) e2243890
- 2 Fox IK, Novak CB, Kahn LC, Mackinnon SE, Ruvinskaya R, Juknis N. Using nerve transfer to restore prehension and grasp 12 years following spinal cord injury: a case report. Spinal Cord Ser Cases 2018; 4: 37
- 3 Anderson KD. Targeting recovery: priorities of the spinal cord-injured population. J Neurotrauma 2004; 21 (10) 1371-1383
- 4 Biondi M, Zucchini M, Bigazzi P, Falcone G, Pfanner S, Del Popolo G. Combined nerve and tendon transfer to restore elbow extension in tetraplegic patients: surgical technique and case report. Spinal Cord Ser Cases 2020; 6 (01) 31
- 5 Svantesson E, Berg J, Bunketorp L. et al. Combination of nerve and tendon transfers offer good prospects for hand function in patients with cervical spinal cord injury. Lakartidningen 2022; •••: 119
- 6 Hill EJR, El-Haj M, Giles JA, Fox IK. Using electrodiagnostics to define injury patterns amenable to nerve transfer surgery in tetraplegia: an illustrative case report. Spinal Cord Ser Cases 2020; 6 (01) 78
- 7 Fridén J, Lieber RL. Reach out and grasp the opportunity: reconstructive hand surgery in tetraplegia. J Hand Surg Eur Vol 2019; 44 (04) 343-353
Address for correspondence
Publication History
Received: 17 November 2023
Accepted: 07 October 2024
Article published online:
23 December 2024
© 2024. SECMA Foundation. This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/)
Thieme Revinter Publicações Ltda.
Rua do Matoso 170, Rio de Janeiro, RJ, CEP 20270-135, Brazil
-
Bibliografia
- 1 Javeed S, Dibble CF, Greenberg JK. et al. Upper Limb Nerve Transfer Surgery in Patients With Tetraplegia. JAMA Netw Open 2022; 5 (11) e2243890
- 2 Fox IK, Novak CB, Kahn LC, Mackinnon SE, Ruvinskaya R, Juknis N. Using nerve transfer to restore prehension and grasp 12 years following spinal cord injury: a case report. Spinal Cord Ser Cases 2018; 4: 37
- 3 Anderson KD. Targeting recovery: priorities of the spinal cord-injured population. J Neurotrauma 2004; 21 (10) 1371-1383
- 4 Biondi M, Zucchini M, Bigazzi P, Falcone G, Pfanner S, Del Popolo G. Combined nerve and tendon transfer to restore elbow extension in tetraplegic patients: surgical technique and case report. Spinal Cord Ser Cases 2020; 6 (01) 31
- 5 Svantesson E, Berg J, Bunketorp L. et al. Combination of nerve and tendon transfers offer good prospects for hand function in patients with cervical spinal cord injury. Lakartidningen 2022; •••: 119
- 6 Hill EJR, El-Haj M, Giles JA, Fox IK. Using electrodiagnostics to define injury patterns amenable to nerve transfer surgery in tetraplegia: an illustrative case report. Spinal Cord Ser Cases 2020; 6 (01) 78
- 7 Fridén J, Lieber RL. Reach out and grasp the opportunity: reconstructive hand surgery in tetraplegia. J Hand Surg Eur Vol 2019; 44 (04) 343-353


