
Subscribe to RSS
DOI: 10.1055/s-0044-1793921
Treatment of Sagittal Plane Instability of the Proximal Interphalangeal Joint: Ultrasound-Guided Volar Plate Scarification Technique
Article in several languages: español | English
Abstract
Introduction Laxity in the volar plate of the proximal interphalangeal joint can result in sagittal plane instability due to its incompetence, accompanied by digital hyperextension with dorsal subluxation, loss of functionality, and pain.
Objectives Present a series of cases of patients with sagittal instability of the volar plate of the proximal interphalangeal plate treated with a minimally invasive surgical technique and evaluate the short and medium-term results.
Material and Methods Patients treated with a minimally invasive surgical technique involving ultrasound-guided scarification of the volar plate for the treatment of laxity in the proximal interphalangeal joint that leads to hyperextension deformity. This technique has been used in five patients in a prospective study with a one-year follow-up, where the percutaneous technique is followed by a splinting and joint rehabilitation protocol.
Results Positive outcomes demonstrating improved joint stability, reduced pain, and enhanced function with a rate of resolution of the proximal interphalangeal joint hyperextension and blockage in a 100%, and improvement in the Quick-DASH and Mayo Wrist Score.
Conclusions The results have demonstrated that it is a safe method with good outcomes for patients with sagittal plane instability associated with volar plate laxity.
Introduction
The initial descriptions of proximal interphalangeal (PIP) joint instability by Kaplan[1] and Bunnell[2] provided foundational insights into the mechanisms and anatomical structures involved in these injuries. Kaplan linked hyperextension deformities of the PIP joint to damage in the volar joint capsule, while Bunnell highlighted the importance of the “volar” ligament in maintaining joint stability. Furthermore, a comprehensive case series from Moellar in 1974 contributed to a better understanding of the various injuries and incompetence associated with the volar plate (VP).[3]
Joint instability can result from different factors, such as a rupture of the VP, collateral ligament tears, or fractures near the middle phalanx's base.[4] These causes can be categorized as extrinsic (resulting from excessive force pulling at the middle phalanx level), intrinsic (due to muscle contracture), or articular (involving VP laxity, inflammatory arthritis, or traumatic injuries).[5]
Occasionally, the lack of diagnosis or inadequate treatment can result in chronic instability in the sagittal plane with PIP hyperextension,[5] [6] [7] giving rise to a spectrum of complications. These potential complications encompass functional impairment, pain, and discomfort. These clinical manifestations indicate the need for surgical treatment to provide stability and preserve joint function.[8] [9]
Surgical treatment options described in the literature include capsulodesis of the volar plate, reinsertion with suture anchors, and tenodesis techniques for stabilization.[10] All of them involve short- and medium-term follow-ups, varying results, and specific indications and complications, such as loss of strength and decreased range of motion.
By promptly addressing this condition we aim to restore joint stability, enhance function, alleviate discomfort, and most importantly to minimize the risk of complications, thus optimizing the patient's overall quality of life.
Within the context of this study, we present a series of cases involving patients who experienced sagittal plane instability of the PIP joint. These cases were treated using a minimally invasive, ultrasound-guided surgical technique which entailed percutaneous scarification of the volar plate. Short and medium-term clinical outcomes were evaluated and are reported herein.
Material and Methods
A prospective study was conducted involving five patients aged between 18 and 38 diagnosed with sagittal plane instability of the proximal interphalangeal (PIP) joint, attributed to volar plate (VP) incompetence. Inclusion criteria included patients with congenital laxity and hyperextension beyond 0°, while individuals with traumatic or acquired laxities, including those with rheumatic conditions, were excluded from the study.
These patients underwent a novel surgical intervention, with a minimum follow-up period of ten months (averaging twelve months) established for assessment. The procedure was performed during a scheduled clinic visit with the patient seated and conscious, under digital anesthesia. It involved ultrasound-guided percutaneous scarification of the PIP joint's VP using a 23G intramuscular needle (1.2 mm diameter). The needle was advanced parallel to the transducer for accurate monitoring and protection of the neurovascular bundle, passing below it horizontally. The needle tip remained consistently visible throughout the procedure. Following the intervention, the patient's finger was splinted with a thermoplastic dorsal splint set at a 30° flexion angle for the PIP joint, allowing immediate postoperative full finger flexion.
To evaluate outcomes, PIP hyperextension was measured with a goniometer, and the hyperextension block was assessed through a physical examination. Pain levels were recorded using a Visual Analog Scale (VAS), ranging from 0 (no pain) to 10 (most severe pain). Functional outcomes were assessed using the Quick Disabilities of the Arm, Shoulder, and Hand (Quick-DASH) and the Mayo Wrist Score (MWS). Grip strength was evaluated with a dynamometer, and the range of motion in flexion and extension was recorded in degrees. Evaluations and questionnaires were administered to assess and compare outcomes between the affected and unaffected hands on the day of the procedure, before any intervention, and at postoperative weeks 6, 12, 24, and 54.
Surgical Technique:
Before ensuring asepsis and antisepsis, we administered 2cc of lidocaine into the dorsal areas of the radial and ulnar collateral branches at the MCP joint of the affected finger ([Fig. 1]).

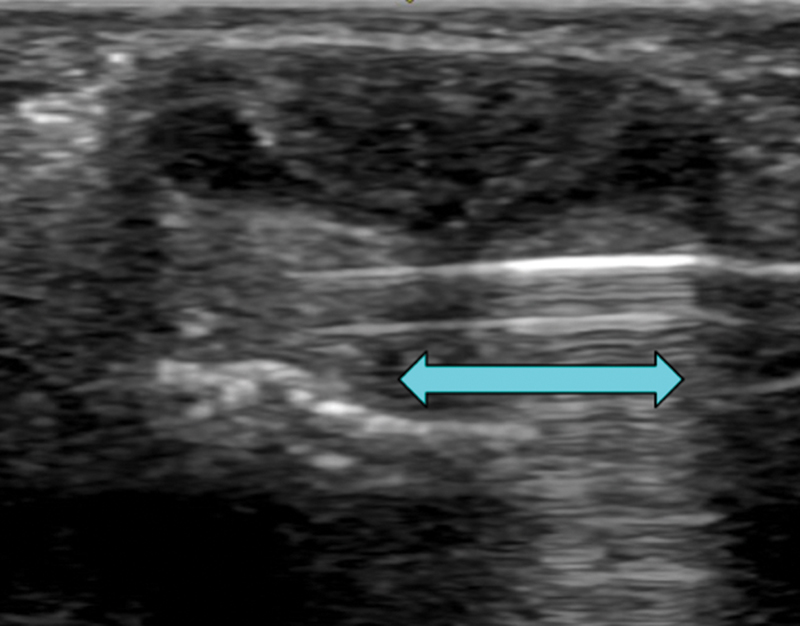
Using a linear transducer with a frequency of 10-25Hz, we performed a volar ultrasound scan in the long axis to assess the condition of the flexor tendons and to identify the proximal and distal boundaries of the VP ([Fig. 2a]). In the short axis we identified the radial and ulnar collateral neurovascular bundles to prevent injury during the procedure ([Fig. 2b]).

While keeping the VP in view on the short axis, we introduced a 23G intramuscular needle (1.2 mm diameter) under ultrasound guidance, targeting the proximal part of the volar plate near the proximal phalanx insertion. The needle was advanced parallel to the transducer for precise monitoring and protection of the neurovascular bundle, passing below it horizontally. The needle tip was consistently visible throughout the procedure. ([Fig. 3a] and [3b]).

From this position, we performed short and controlled forward and backward movements as well as lateral sweeps to conduct the percutaneous scarification of the VP ([Figs. 4] and [5]).

Technical Tips
In addition to continuous ultrasound monitoring, the needle tip should feel resistance against the bone cortex of the first phalanx. This action is referred to as “scarification.”
The procedure is dynamic, with ongoing ultrasound monitoring in both the longitudinal and transverse axes. Scarification of the VP typically takes about 5 to 7 minutes, including the application of anesthesia and waiting for its effect, and can be completed within 12 to 15 minutes. Following scarification, we verify the condition of the flexor tendons and the neurovascular bundle in both ultrasound axes. Subsequently, we splint the finger with a thermoplastic splint set at a 30° flexion angle for the PIP joint with an extension block while permitting full flexion of the finger.
Splinting
Proper placement of the post-treatment splint is crucial for the treatment's success and is done before the procedure. Initially, we protect the finger with a retrograde spiral bandage using cohesive bandage ([Fig. 6]). Then, we customize the thermoplastic material for each patient using Orfit colors NS with a thickness of 2mm, configuring it dorsally and at a 30° flexion angle for PIP joint and 0° for distal interphalangeal (DIP) joint ([Fig. 7]). The splint is adjustable with Velcro and allows for maximum flexion of the metacarpophalangeal (MP), PIP, and DIP joints while preventing PIP extension beyond −30°. After the procedure, the splint is worn continuously for six weeks but can be removed for hygiene and wound care while maintaining a flexed position ([Fig. 8]).



Rehabilitation Protocol
To enhance the PIP joint's stability and prevent deficits, we implement isometric muscle strengthening exercises for the superficial finger flexors, involving two sets of 25 repetitions twice daily. PIP flexion is maintained at 90°, and a rubber band is used for resistance ([Fig. 9]). This physiotherapy protocol should be followed throughout the rehabilitation process.

Results
Four women and one man were included, with an average age of 26 years. All five deformities were due to intrinsic laxity (congenital incompetence). No patient had digital sensory alterations or tendon injuries. The rate of resolution of PIP hyperextension was 100% at 6, 12, 24, and 54 weeks. The rate of resolution of hyperextension block was 100% at 6, 12, 24, and 54 weeks. Pain decreased after the procedure, and patients experienced improvements in both the Quick-DASH and Mayo Wrist Score (MMWS). Grip strength increased by 31% after the procedure. The range of motion in flexion of the treated finger did not show significant changes compared to preoperative measurements. The range of motion in the extension of the PIP treated showed significant changes compared to preoperative measurements (mean extension deficit of 7°, range -15° to 0°). In the final follow-up, there were no differences between the treated and untreated (healthy) hands in terms of digital joint balance or grip.
Discussion
This novel technique guided by ultrasound generates a controlled lesion to the VP and creates a guided scar that enhances the flexion of the PIP limiting its hyperextension and leading to fewer complications compared to open technique procedures. The VP scarification's resolution was 100%, without surgical site complications, and considerably lower costs. No need for hospital admission was necessary due to an ambulatory treatment managed in a routine clinic visit, without risk of major complications using only local anesthesia.
Traditionally, instability of the PIP is surgically treated with open techniques, with reinsertion of the volar plate being the most common.[11] [12] [13] [14] Zaidenberg et al in 2022 treated 16 patients with a volar capsulodesis technique, and a two-year follow-up yielded satisfactory results. Main limitans were an 85% grip strength compared to the contralateral side and a residual flexion contracture (residual flexion contracture was 10° in 13 patients and more than 10° in 3 cases).[15] In another study, Ahmed et al presented a case report of a patient treated with a reconstruction of the oblique retinacular ligament, with a 5-year follow-up where a resolution of instability was achieved, although with similar results as the volar capsulodesis technique, this one display significant loss of strength and decreased range of motion compared to the contralateral side.[16]
In another study, a series of cases treated with the modified Thompson-Littler technique is presented. Satisfactory results were obtained without the loss of flexion and recurrence of subluxation of the finger. This method enabled the correction of both dorsal and lateral instability of the PIP joint through an extended incision.[17] Nevertheless, greater comorbidity arouses with dorsal incision, risk of contractures, and split of tendon mechanisms with a possibility of lag extension. A closer postoperative follow-up is necessary for the identification of short- and medium-term complications.
All the techniques above demonstrated satisfactory results in certain aspects. However, compared to our minimally invasive technique, these alternatives required a more extensive surgical procedure with anesthesia and surgical risks and higher monetary costs. The hospitalization time was considerably longer, and they needed more frequent follow-ups for the treatment of operative wounds and a more exhaustive rehabilitation protocol, still without achieving better results compared to the contralateral side.
This study sheds light on a minimally invasive surgical technique aimed at addressing sagittal instability of the PIP joint achieving highly successful PIP stability and finger ROM results, with 100% resolution and no significant result differences compared with the contralateral (healthy) hand.
In orthopedic surgery, ultrasound-guided techniques are widely used, one example of its use is a successful repair of the Achilles tendon, being this intervention successful we wanted to recreate similar treatment techniques in hand surgery, as there is an increasing trend in the use of ultrasound-guided techniques due to its ability to provide real-time imaging for better visualization of soft tissues, nerves, blood vessels, and other structures.[18] This approach is valuable for various procedures, including joint injections (MP, PIP, DIP), and tendon sheath injections (for trigger fingers, tenosynovitis) with minimized potential complications, and improved therapeutic effects. It is also useful for nerve blocks, cyst aspirations, and soft tissue biopsies.
The use of ultrasound guidance in hand surgery offers several advantages, including improved accuracy, reduced complications, and enhanced patient outcomes. Surgeons can visualize anatomical structures in real time, thereby increasing the safety and efficacy of various procedures. However, surgeons must undergo proper training and gain experience in ultrasound-guided techniques to maximize the benefits of this procedure. To date, no similar treatment options are described in the literature for the resolution of sagittal instability of the PIP or other soft tissue problems in the stability of the finger joints.
Our study has limitations, including the short follow-up period and a small number of patients which does not allow for a more extensive case analysis to observe how the technique performs in other populations. Despite being a small study, it creates the opportunity to develop a long-term study with a broader population opening pathways to innovation in the treatment of PIP instability. This approach holds promise for improving the quality of life for individuals with chronic PIP joint instability, potentially preventing long-term joint degeneration and associated complications. Long-term follow-up studies will be valuable to confirm the durability and sustainability of these positive outcomes and may help validate the effectiveness of this technique and its applicability in a broader patient population.
Conclusion
In conclusion, there are promising results for the treatment of sagittal instability of the PIP joint using a minimally invasive ultrasound-guided technique, minimizing risks to adjacent structures. This approach simplifies the treatment, avoiding surgical approaches, infection risks, and operative anesthetic risks, with a shorter hospital stay and minimal follow-up for wound care. The rehabilitation protocol ismore comfortable for the patient, yielding positive long-term results with a preserved range of motion and strength compared to the contralateral side.
Conflictos de intereses
Ninguno.
-
Bibliografía
- 1 Kaplan EB. Extension deformities of the proximal inter- phalangeal joints of the fingers. J Bone Joint Surg Am 1939; 18: 781-783
- 2 Bunnell S. Surgery of the Hand, ed. 2. Philadelphia: 1948. JB Lippincott Co;
- 3 Moller JT. Lesions of the volar fibrocartilago in finger joints. A 2-year material. Acta Orthop Scand 1974; 45 (05) 673-682
- 4 Bowers WH. The proximal interphalangeal joint volar plate. II: a clinical study of hyperextension injury. J Hand Surg Am 1981; 6 (01) 77-81
- 5 McKeon KE, Lee DH. Posttraumatic Boutonnière and Swan Neck Deformities. J Am Acad Orthop Surg 2015; 23 (10) 623-632
- 6 Carlo J, Dell PC, Matthias R, Wright TW. Collateral Ligament Reconstruction of the Proximal Interphalangeal Joint. J Hand Surg Am 2016; 41 (01) 129-132
- 7 Lane R, Nallamothu SV. Swan-Neck Deformity. In: StatPearls. Treasure Island (FL): StatPearls Publishing; June 26, 2023
- 8 Smith GC, Amirfeyz R. The flexible swan neck deformity in rheumatoid arthritis. J Hand Surg Am 2013; 38 (07) 1405-1407
- 9 García Bernal FJ, Nevado Sánchez E. Tratamiento de la inestabilidad en plano sagital de la articulación interfalángica proximal mediante reparación de la placa volar. Revista Iberoamericana de Cirugía de la Mano 2022; 50 (01) e64-e68
- 10 Lee SK. Modern tendon repair techniques. Hand Clin 2012; 28 (04) 565-570
- 11 Thompson JS, Littler JW, Upton J. The spiral oblique retinacular ligament (SORL). J Hand Surg Am 1978; 3 (05) 482-487
- 12 van der Giesen FJ, Nelissen RG, van Lankveld WJ. et al. Swan neck deformities in rheumatoid arthritis: a qualitative study on the patients' perspectives on hand function problems and finger splints. Musculoskeletal Care 2010; 8 (04) 179-188
- 13 Catalano III LW, Skarparis AC, Glickel SZ. et al. Treatment of chronic, traumatic hyperextension deformities of the proximal interphalangeal joint with flexor digitorum superficialis tenodesis. J Hand Surg Am 2003; 28 (03) 448-452
- 14 Ko JH, Kalainov DM, Hsu LP, Fang RC, Mastey RD. Double lateral band transfer for treatment of traumatic hyperextension instability of the proximal interphalangeal joint: a report of two cases. Hand (N Y) 2012; 7 (01) 108-113
- 15 Zaidenberg E, Saba JS, Rellan I, Cesca FJ, Pastrana M, Zaidenberg CR. Volar Capsulodesis With Early Active Motion for the Treatment of Chronic Proximal Interphalangeal Joint Hyperextension Deformity. J Hand Surg Am 2023; 48 (12) 1275.e1-1275.e6
- 16 Ahmed HA, Goldie BS. Proximal interphalangeal joint instability: a dynamic technique for stabilization. J Hand Surg [Br] 2002; 27 (04) 354-355
- 17 Matsuo T, Suzuki T, Kimura H, Iwamoto T. Modified Thompson-Littler Method for Chronic Instability of the Proximal Interphalangeal Joint: A Report of Two Cases. J Hand Surg Asian Pac Vol 2023; 28 (01) 125-128
- 18 Paczesny Ł, Zabrzyński J, Domżalski M. et al. Mini-Invasive, Ultrasound Guided Repair of the Achilles Tendon Rupture-A Pilot Study. J Clin Med 2021; 10 (11) 2370
Address for correspondence
Publication History
Received: 12 February 2024
Accepted: 07 October 2024
Article published online:
23 December 2024
© 2024. SECMA Foundation. This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/)
Thieme Revinter Publicações Ltda.
Rua do Matoso 170, Rio de Janeiro, RJ, CEP 20270-135, Brazil
-
Bibliografía
- 1 Kaplan EB. Extension deformities of the proximal inter- phalangeal joints of the fingers. J Bone Joint Surg Am 1939; 18: 781-783
- 2 Bunnell S. Surgery of the Hand, ed. 2. Philadelphia: 1948. JB Lippincott Co;
- 3 Moller JT. Lesions of the volar fibrocartilago in finger joints. A 2-year material. Acta Orthop Scand 1974; 45 (05) 673-682
- 4 Bowers WH. The proximal interphalangeal joint volar plate. II: a clinical study of hyperextension injury. J Hand Surg Am 1981; 6 (01) 77-81
- 5 McKeon KE, Lee DH. Posttraumatic Boutonnière and Swan Neck Deformities. J Am Acad Orthop Surg 2015; 23 (10) 623-632
- 6 Carlo J, Dell PC, Matthias R, Wright TW. Collateral Ligament Reconstruction of the Proximal Interphalangeal Joint. J Hand Surg Am 2016; 41 (01) 129-132
- 7 Lane R, Nallamothu SV. Swan-Neck Deformity. In: StatPearls. Treasure Island (FL): StatPearls Publishing; June 26, 2023
- 8 Smith GC, Amirfeyz R. The flexible swan neck deformity in rheumatoid arthritis. J Hand Surg Am 2013; 38 (07) 1405-1407
- 9 García Bernal FJ, Nevado Sánchez E. Tratamiento de la inestabilidad en plano sagital de la articulación interfalángica proximal mediante reparación de la placa volar. Revista Iberoamericana de Cirugía de la Mano 2022; 50 (01) e64-e68
- 10 Lee SK. Modern tendon repair techniques. Hand Clin 2012; 28 (04) 565-570
- 11 Thompson JS, Littler JW, Upton J. The spiral oblique retinacular ligament (SORL). J Hand Surg Am 1978; 3 (05) 482-487
- 12 van der Giesen FJ, Nelissen RG, van Lankveld WJ. et al. Swan neck deformities in rheumatoid arthritis: a qualitative study on the patients' perspectives on hand function problems and finger splints. Musculoskeletal Care 2010; 8 (04) 179-188
- 13 Catalano III LW, Skarparis AC, Glickel SZ. et al. Treatment of chronic, traumatic hyperextension deformities of the proximal interphalangeal joint with flexor digitorum superficialis tenodesis. J Hand Surg Am 2003; 28 (03) 448-452
- 14 Ko JH, Kalainov DM, Hsu LP, Fang RC, Mastey RD. Double lateral band transfer for treatment of traumatic hyperextension instability of the proximal interphalangeal joint: a report of two cases. Hand (N Y) 2012; 7 (01) 108-113
- 15 Zaidenberg E, Saba JS, Rellan I, Cesca FJ, Pastrana M, Zaidenberg CR. Volar Capsulodesis With Early Active Motion for the Treatment of Chronic Proximal Interphalangeal Joint Hyperextension Deformity. J Hand Surg Am 2023; 48 (12) 1275.e1-1275.e6
- 16 Ahmed HA, Goldie BS. Proximal interphalangeal joint instability: a dynamic technique for stabilization. J Hand Surg [Br] 2002; 27 (04) 354-355
- 17 Matsuo T, Suzuki T, Kimura H, Iwamoto T. Modified Thompson-Littler Method for Chronic Instability of the Proximal Interphalangeal Joint: A Report of Two Cases. J Hand Surg Asian Pac Vol 2023; 28 (01) 125-128
- 18 Paczesny Ł, Zabrzyński J, Domżalski M. et al. Mini-Invasive, Ultrasound Guided Repair of the Achilles Tendon Rupture-A Pilot Study. J Clin Med 2021; 10 (11) 2370








