Subscribe to RSS
DOI: 10.1055/s-0045-1804494
Calcaneo-Stop: An Effective Surgical Technique to Correct Symptomatic Flexible Flatfoot in Children
Article in several languages: português | EnglishAuthors
Financial Support The authors declare that they did not receive financial support from agencies in the public, private or non-profit sectors to conduct the present study.

Abstract
Objective Flexible juvenile valgus flatfoot is a prevalent condition that typically resolves spontaneously but requires surgical treatment if associated with discomfort, pain, and physical limitation. However, certain surgical procedures are associated with higher morbidity, as they involve osteotomies and arthrodesis. In this context, extra-articular talocalcaneal arthroereisis is an option, because it is a cost-effective, low-morbidity, and efficient method of treatment. The aim of the present study is to report the outcomes of the treatment of flexible juvenile valgus flatfoot using the calcaneo-stop technique.
Methods Pre-adolescent patients with severe or symptomatic flexible juvenile valgus flatfoot were surgically treated using the calcaneo-stop technique (talocalcaneal arthroereisis). The outcomes were evaluated clinically and radiographically, assessing Meary angles, talonavicular coverage, talus-metatarsal alignment, Moreau-Costa-Bertani angle, calcaneal pitch, and the percentage of talus head coverage by the navicular.
Results A total of 23 individuals (44 feet) were evaluated and operated on, with ages ranging from 7 to 13 years (mean: 11) and a mean follow-up of 28 months. There was marked improvement or disappearance of symptoms in 90% of the patients. The complication rate was of 13.6%, primarily associated with localized pain at the surgical site. All radiographic parameters improved significantly (p < 0.001), with values approaching normality in most cases.
Conclusion Improvements in both clinical and radiographic parameters suggest that talocalcaneal arthroereisis corrects deformities with a low complication rate.
Introduction
Flexible flatfoot is characterized by the absence of or significant reduction in the medial longitudinal arch, associated with an increased valgus of the ankle during weight bearing. It is a common condition in children, but it is self-limiting and has a strong tendency for spontaneous regression.[1] However, a minority of individuals may experience complete failure in the development of the medial plantar arch, resulting in permanent flatfoot throughout life. In adulthood, if the condition is severe, there may be functional limitations, pain, and an increased risk of developing osteoarthritis.[2]
In the juvenile age group, flatfoot can be associated with symptoms such as fatigue after usual efforts, cramps, pain, and discomfort when attempting to fit the unconventional foot shape into standard footwear.[3] These complaints tend to be exacerbated with excess weight, ligament laxity, or Achilles tendon shortening.[4]
Conservative interventions, such as the use of insoles, despite their widespread use, lack scientific evidence supporting their effectiveness.[5] [6] As a result, several surgical procedures have been developed to correct symptomatic flexible flatfoot in immature individuals. These techniques can be grouped into soft-tissue procedures,[7] osteotomies,[8] [9] [10] or localized arthrodesis.[4] Approaches that exclusively target musculotendinous and ligamentous structures provide temporary corrective effects due to tissue compliance. Osteotomies yield favorable outcomes, but they require longer periods of immobilization and recovery. Arthrodesis has limited indications, as it requires joint destruction to achieve correction.[11]
Another surgical option is arthroereisis (from the Greek arthroereisis, in which arthros means joint, and ereisis, the action of supporting or sustaining). These procedures aim to preserve the joint providing mechanical stabilization without limiting functional movements. They are interesting for their potential in correcting and preventing severe deformities.[12] When applied to flatfoot, such techniques show simplicity, efficiency, low morbidity, and prompt recovery, making them suitable for young and healthy patients.[13]
The origins of arthroereisis in the foot can be attributed to Grice,[14] in 1952, who devised an extra-articular arthrodesis procedure by inserting a bone graft into the tarsal sinus, attempting to correct valgus deformities in children affected by poliomyelitis sequelae. In 1990, Crawford et al.[12] employed temporary metal staples in the subtalar joint to correct valgus feet in individuals with spastic cerebral palsy. The primary objective was to restore the medial plantar arch by partially restricting subtalar joint motion, rather than completely blocking it. Later, the arthroereisis effect was achieved through the insertion of implants into the tarsal sinus, or by blocking excessive calcaneal eversion using a screw placed laterally to the tarsal sinus, under the lateral process of the talus.[15]
Subtalar implants within the tarsal sinus were initially introduced in 1977, utilizing a silicone elastomer block to maintain the optimal position of the joint.[16] Since then, a wide variety of implants have been developed for this purpose, encompassing various shapes such as plugs, spacers, cones, screws, and cylinders. The materials include elastomer, polyethylene, titanium, and bioabsorbable poly-L-lactic acid.[3]
According to De Pellegrin,[15] the insertion of an extra-articular screw into the calcaneus, adjacent to the lateral process of the talus, was initially described by Álvarez[17] to achieve the effect of arthroereisis, and later modified by Pisani.[18] The technique temporarily blocks excessive pronation of the subtalar joint, enabling the lateral column to grow and occupy the space without pressure.
Currently, this technique is widely used in Europe.[13] [15] [18] [19] [20] In Brazil, arthroereisis with a screw in the calcaneus remains, to some extent, unfamiliar to most of the orthopedists, and the publications are on the treatment of neuropathic flatfoot.[21]
The objectives of the present study were to analyze the results of correcting severe symptomatic flexible valgus flatfoot in the preadolescent age group using the calcaneo-stop technique, and to contribute to a wider dissemination of this method.
Materials and Methods
The current retrospective study was designed to evaluate the outcomes of the surgical treatment in preadolescent patients with symptomatic flexible valgus flatfoot. The study was approved by the institutional Ethics Committee (CAAE: 77119524.8.0000.5440). The sample included individuals of both sexes presenting severe, flexible, idiopathic valgus flatfoot submitted to the calcaneo-stop technique at our institution. The flexibility of the foot was assessed based on reversibility of the deformity with and without weight bearing, the tiptoe standing test ([Fig. 1]), and on the result of the Jack test.

Data were collected from medical records, and the assessment included the resolution of the symptoms, the satisfaction of the patients and their families, as well as pre- and postoperative radiographic parameters. The study included cases with complete documentation and informed consent, involving surgeries performed between 2017 and 2022, with an average follow up of 28 months (range: 12-65). We excluded cases of lower limb mechanical axis deviation, concurrent foot deformities or stiffness, prior foot surgery or fractures, or underlying local or systemic diseases (Down syndrome, Ehlers-Danlos syndrome, etc.).
Operative Procedure
Under anesthesia, with the knee extended, the foot was forced into dorsiflexion to assess the degree of heel valgus and to check for associated equinus. Palpation was used to identify the sinus tarsi, and a skin incision measuring approximately 2.0 cm in length was made over it ([Fig. 2A]). Careful blunt dissection was performed to expose the fat pad and the short extensor muscle, ensuring the sensory branch of the fibular nerve remained undamaged. Under fluoroscopy, the foot was forced into supination, enabling the identification and exposure of the flat surface in the lateral region of the calcaneus, serving as the entry point to the sinus tarsi. A Kirschner wire (K wire) with 2.0 mm in diameter was perpendicularly inserted into the calcaneus bone surface, outside of the sinus tarsi, and its position was confirmed using fluoroscopy ([Fig. 2B]). Subsequently, the K wire was removed, but the hindfoot was maintained in varus position. The entry point of the wire was identified, the hole was enlarged using a 3.2-mm drill bit, and a partially threaded 6.5-mm cancellous stainless-steel screw (DePuy Synthes, Raynham, MA, United States) with 30 to 40 mm in length was inserted ([Fig. 2C,D]). The depth of the screw was adjusted to ensure its head was positioned beneath the lateral process of the talus, thereby correcting the malalignment in valgus of the hindfoot. If under- or overcorrection occurred, the screw was respectively advanced or retracted until the desired alignment was achieved. In certain cases, alternative implants, such as those of 7.0-mm cannulated cortical screws (DePuy Synthes), or fully-threaded screws were used. It should be noted that the available literature does not indicate any significant impact of these implant variations on the outcomes of the procedure. If residual equinus was present, a Hoke-type lengthening of the Achilles tendon was carried out, followed by the application of a long leg plaster cast splint.

Postoperative Care
Postoperatively, all patients were immobilized for 7 days, after which weight bearing was gradually reintroduced. In cases requiring equinus correction, patients wore a walking cast for an additional two weeks before transitioning to regular footwear.
A standardized physiotherapy protocol was not implemented, nor was the use of orthotics or modified footwear recommended. Around three weeks after surgery, once the scars had fully healed, the patients were advised to gradually resume physical activities and sports, provided postoperative pain had subsided.
Clinical Evaluation
The patient's medical record was accessed to compare the pre- and postoperative findings. Complications resulting from the surgical procedure, along with symptoms observed postoperatively that were not present preoperatively, were taken into consideration, such as pain, discomfort, and esthetic improvement.[22]
Radiographic Evaluation
The pre and the latest postoperative images were evaluated in anteroposterior and lateral views, under weight bearing. The following angles and measurements were assessed: Meary's, calcaneal pitch, Moreau-Costa-Bertani's, alignment between the long axis of the talus with the first metatarsal, talonavicular angular coverage, and talonavicular percentual coverage.[23] [24] [Fig. 3] shows the angles used, how to trace them, and their normal ranges. All collected data were grouped and presented in [Table 1].
|
Identification |
Age |
Follow-up |
Calcaneal pitch |
Talonavicular angle coverage |
Talonavicular percentual coverage |
Meary's angle |
Talus-first metatarsal angle |
Moreau-Costa-Bertani's angle |
Pain |
Complications |
|||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
(years) |
(month) |
Pre |
Post |
Pre |
Post |
Pre |
Post |
Pre |
Post |
Pre |
Post |
Pre |
Post |
Pre |
Post |
||
|
F1 |
9 |
20 |
4.5 |
11.8 |
45.6 |
22.4 |
50.6 |
24.8 |
-32.6 |
-5.5 |
25.3 |
2.7 |
159 |
140.8 |
Yes |
No |
No |
|
F2 |
9 |
20 |
7.7 |
14 |
44.8 |
21.8 |
47.7 |
24.2 |
-23 |
-5.6 |
14.3 |
7.4 |
148.2 |
135.3 |
Yes |
No |
No |
|
F3 |
13 |
34 |
6 |
16.7 |
36.6 |
16.5 |
40.6 |
18.3 |
-24 |
-13.7 |
12.4 |
3.4 |
142.4 |
132.4 |
SIM |
No |
No |
|
F4 |
13 |
28 |
8.6 |
17.3 |
23.9 |
11.6 |
26.5 |
12.8 |
-22 |
-8.6 |
13.3 |
1.4 |
142.8 |
127.8 |
Yes |
No |
No |
|
F5 |
9 |
34 |
2 |
4 |
56.1 |
24.7 |
62.3 |
27.4 |
-18.1 |
1.7 |
18.6 |
9.7 |
143.4 |
135 |
Yes |
No |
No |
|
F6 |
9 |
34 |
-4 |
1.5 |
45.9 |
25 |
51 |
27.7 |
-18 |
-4.6 |
20.3 |
1.2 |
147.6 |
135.8 |
Yes |
No |
No |
|
F7 |
11 |
40 |
2.6 |
10.5 |
45.8 |
18.7 |
50.8 |
20.7 |
-17.2 |
-0.8 |
17.1 |
5.5 |
146.1 |
133.1 |
Yes |
No |
Chronic pain |
|
F8 |
11 |
40 |
1 |
8.7 |
44.1 |
15.1 |
49 |
16.7 |
-22 |
-1.5 |
16.4 |
5 |
141.6 |
134.9 |
Yes |
Yes |
Chronic pain |
|
F9 |
12 |
30 |
0.5 |
4.3 |
41.3 |
1 |
45.8 |
1.1 |
-17.8 |
-12.8 |
16.8 |
5.2 |
144.2 |
134 |
Yes |
No |
No |
|
F10 |
12 |
30 |
0.5 |
6 |
50.4 |
23.3 |
56 |
25.8 |
-23.2 |
-9.8 |
36.1 |
17.3 |
151.5 |
135.3 |
Yes |
No |
No |
|
F11 |
12 |
37 |
10.5 |
13.8 |
16 |
11.3 |
17.7 |
12.5 |
-6.7 |
6.3 |
25 |
14.3 |
130.3 |
115.6 |
Yes |
No |
No |
|
F12 |
12 |
37 |
10.8 |
12.1 |
39.5 |
16.8 |
43.8 |
18.6 |
-14.6 |
1.6 |
36.2 |
19 |
134.7 |
119.5 |
Yes |
No |
No |
|
F13 |
11 |
21 |
6.3 |
9.5 |
39 |
21.5 |
43.3 |
23.8 |
-30.6 |
-12.5 |
23.5 |
3 |
151.7 |
142.5 |
Yes |
No |
No |
|
F14 |
11 |
21 |
9 |
7.8 |
11.9 |
9.8 |
13.2 |
10.8 |
-12.5 |
-7.7 |
6 |
7.8 |
141.6 |
137.7 |
Yes |
No |
No |
|
F15 |
11 |
39 |
11 |
18 |
40.2 |
1.1 |
44.6 |
1.2 |
-10.7 |
13.3 |
24.1 |
6.5 |
138.7 |
118.6 |
Yes |
No |
No |
|
F16 |
11 |
39 |
11.6 |
18.4 |
42.9 |
2.3 |
47.6 |
2.5 |
-12.5 |
-3.5 |
29.4 |
3.5 |
140 |
127 |
Yes |
No |
No |
|
F17 |
12 |
17 |
4.7 |
5.1 |
32.9 |
20.2 |
36.5 |
22.4 |
-22.1 |
-13.5 |
12 |
12.7 |
152.6 |
144.2 |
Yes |
No |
Undercorrection |
|
F18 |
12 |
17 |
3.3 |
9.6 |
43 |
27.6 |
47.7 |
30.6 |
-28 |
-4.5 |
25.5 |
1.9 |
153.4 |
131.2 |
Yes |
No |
No |
|
F19 |
11 |
47 |
9.6 |
15 |
38.8 |
12.8 |
43.1 |
14.3 |
-19 |
-5.3 |
19.2 |
9.3 |
151.2 |
129.5 |
Yes |
No |
No |
|
F20 |
11 |
47 |
6.5 |
16.8 |
32 |
11.9 |
35.5 |
13.2 |
-19.7 |
-2 |
22.4 |
12.9 |
148.1 |
129.9 |
Yes |
No |
No |
|
F21 |
9 |
65 |
3.9 |
17.3 |
42.8 |
15.5 |
47.5 |
17.2 |
-20.6 |
-4.4 |
16.8 |
8.6 |
144.8 |
130.4 |
Yes |
No |
No |
|
F22 |
9 |
65 |
3.3 |
13.3 |
46.9 |
22.7 |
52.1 |
25.2 |
-30 |
-7.1 |
20.1 |
8.1 |
158 |
137.2 |
Yes |
No |
No |
|
F23 |
9 |
6 |
3.6 |
7.9 |
26 |
20.4 |
28.8 |
22.6 |
-22.4 |
-12.2 |
4.4 |
2.3 |
148.4 |
141 |
Yes |
Yes |
Chronic pain |
|
F24 |
16 |
33 |
10.1 |
12.2 |
35.6 |
31.7 |
39.5 |
35.2 |
-9.5 |
-6 |
14.8 |
13 |
131.4 |
132 |
Yes |
No |
No |
|
F25 |
16 |
33 |
8.1 |
14.1 |
30.1 |
24.8 |
33.4 |
27.5 |
-14.6 |
-5.2 |
16 |
11 |
136.9 |
128.1 |
Yes |
No |
No |
|
F26 |
11 |
32 |
7.9 |
15.6 |
41.6 |
15.1 |
46.2 |
16.7 |
-18.7 |
-5.7 |
13.6 |
1.1 |
142.9 |
137.6 |
Yes |
No |
No |
|
F27 |
11 |
32 |
10.6 |
14.8 |
39.6 |
6.9 |
44 |
7.6 |
-13.4 |
-6.5 |
13.5 |
1.6 |
140.3 |
137.4 |
Yes |
No |
No |
|
F28 |
7 |
11 |
7 |
12.7 |
41.6 |
7.1 |
46.2 |
7.8 |
-9.5 |
10.6 |
12.5 |
9.2 |
140.9 |
124.6 |
Yes |
No |
No |
|
F29 |
7 |
11 |
6.7 |
8.2 |
33.8 |
4.5 |
37.5 |
5 |
-10.5 |
10.1 |
14.1 |
14.4 |
138.7 |
128 |
Yes |
No |
No |
|
F30 |
13 |
26 |
13.4 |
20.1 |
32.5 |
12.1 |
36.1 |
13.4 |
-12.9 |
4.8 |
36.6 |
16 |
134.8 |
121.8 |
Yes |
No |
No |
|
F31 |
13 |
26 |
19.3 |
20.6 |
36.4 |
16.6 |
40.4 |
18.4 |
-11.4 |
4.1 |
35.3 |
12.7 |
124.7 |
117.2 |
Yes |
No |
No |
|
F32 |
10 |
6 |
9.7 |
16.2 |
26.4 |
14.7 |
29.3 |
16.3 |
-9.6 |
0.8 |
13.7 |
11.2 |
133.5 |
122.1 |
Yes |
No |
No |
|
F33 |
10 |
6 |
14.4 |
17.3 |
20.8 |
2.3 |
23.1 |
2.5 |
-10.1 |
1.5 |
10.2 |
5 |
127.6 |
118 |
Yes |
No |
No |
|
F34 |
11 |
47 |
5.7 |
8.1 |
27.7 |
23.4 |
30.7 |
26 |
-17.7 |
3.5 |
16 |
11.8 |
142.2 |
128.7 |
Yes |
No |
No |
|
F35 |
11 |
47 |
7.1 |
8.7 |
23.8 |
18 |
26.4 |
20 |
-18.7 |
3.9 |
14 |
7 |
143.8 |
127.1 |
Yes |
No |
No |
|
F36 |
13 |
20 |
10.4 |
17.4 |
25.2 |
9.9 |
28 |
11 |
-11.2 |
-1 |
4.2 |
4.7 |
133.2 |
119.1 |
Yes |
No |
No |
|
F37 |
13 |
20 |
11.8 |
18.2 |
25.8 |
15.5 |
28.6 |
17.2 |
-13.6 |
-2.5 |
3.2 |
0.1 |
136.8 |
124.3 |
Yes |
No |
No |
|
F38 |
12 |
12 |
3 |
12.7 |
43 |
23.9 |
47.7 |
26.5 |
-24 |
-3.5 |
22 |
9.8 |
158 |
126.5 |
Yes |
No |
No |
|
F40 |
14 |
12 |
4.3 |
7.5 |
32.1 |
4.4 |
35.6 |
4.8 |
-21.7 |
-14.3 |
19.1 |
6.8 |
154.2 |
147.5 |
Yes |
No |
Undercorrection |
|
F41 |
14 |
12 |
5.5 |
11.1 |
36.7 |
5 |
40.7 |
5.5 |
-19.2 |
-10.4 |
23.2 |
9.8 |
150.1 |
143.2 |
Yes |
No |
Undercorrection |
|
F42 |
7 |
26 |
3.3 |
9.2 |
42 |
16.2 |
46.6 |
18 |
-13.3 |
-7.1 |
14.4 |
4.4 |
144.3 |
134.4 |
Yes |
No |
No |
|
F43 |
7 |
26 |
4.1 |
10.1 |
40.7 |
13.3 |
45.2 |
14.7 |
-11.9 |
-6.6 |
13.2 |
3.9 |
142.1 |
129.1 |
Yes |
No |
No |
|
F44 |
12 |
34 |
2.2 |
16.4 |
41.2 |
20.2 |
45.7 |
22.4 |
-23.1 |
-9.4 |
16.8 |
4.4 |
151.1 |
139.1 |
Yes |
No |
No |

Statistical Analysis
The Shapiro-Wilk test was used to evaluate the normality of the sample distribution and determine a parametric distribution, with statistical significance set at p < 0.05. The paired t-test was used to assess the significance of the surgical intervention and improvement in radiological outcomes, with p set at < 0.001. Analyses were conducted using the RStudio Desktop Pro (Posit, PBC, Boston, MA, United States) software, version 2023.03.0.
Results
A total of 23 patients (44 feet), aged between 7 and 13 (mean: 11) years, were considered eligible for the study. The minimum follow-up was 12 months, and the maximum was 5 years (65 months), with a mean of 28 months.
The clinical outcomes were satisfactory, addressing both esthetic concerns and alleviating pain. In total, 90% of the patients reported improvement or complete resolution of symptoms and pain relief compared to their preoperative condition. The rate of complications was of 13.6%, and they occurred in 6 cases: 3 with chronic pain at the surgical site, and 3 with incomplete correction of the deformity. In two cases, the pain was resolved with local corticosteroid injections, while, in the other case, the screw was removed, resulting in reduced pain – though not fully resolved. Implant removal was not necessary for the other patients. There were no occurrences of infection, wound healing issues, or implant breakage. All radiographic parameters exhibited significant postoperative improvement ([Fig. 4]).

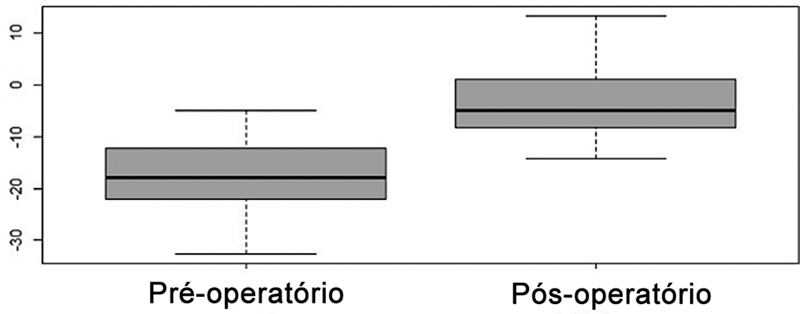
The calcaneal pitch showed a significant increase of 87%, with a preoperative mean value of 6.61° (standard deviation [SD]: 0.65°) and a postoperative value of 12.41° (SD: 0.60°) ([Fig. 5]). The talonavicular coverage exhibited a significant improvement, of 136%, as evidenced by the t-test (p < 0.001). The final mean values of 15.43° (SD: ± 1.15°) remained slightly higher than the reference values ([Fig. 6]). The Meary's angle showed a strong correlation in the t-test (p < 000.1) ([Fig. 7]), with a significant improvement of 383%, in the talonavicular alignment of the sagittal axis. However, the mean final value of -3.64° (SD: ± 1.01°) was still not within the normal range.



The alignment of the long axis of the talus with the first metatarsal in the coronal plane showed improvement of 141%, a significant difference in the t-test (p < 0.001) ([Fig. 8]). The mean preoperative value was of 18.12° (SD: ± 1.22°) and, postoperatively, it was of 7.5° (SD: ± 0.78°).

The Moreau-Costa-Bertani's angle showed improvement in the measured parameters (p < 0.001). Although the values did not reach normality, with a preoperative mean of 143.8° (SD: ± 1.22°) and a postoperative mean of and 131.21° (SD: ± 1.19°), an improvement of 9% in the formation of the plantar arch was observed ([Fig. 9]). The talonavicular coverage percentage showed significant improvement of 38% as evidenced by the t-test analysis (p < 0.001). The preoperative mean value of 59.7% (SD: ± 1.54%) increased to 82.8% (SD: ± 1.28%), with a significant improvement in the relationship between the hindfoot and midfoot ([Fig. 10]).


Discussion
In the present case series, the treatment of the severe idiopathic pediatric flatfoot using the calcaneo-stop technique demonstrated effective correction of the deformity with minimal complications. The surgical procedure is technically straightforward and yields positive clinical and radiographic outcomes.
Although the exact cause of flatfoot remains a topic of debate,[7] [25] if left untreated, it can lead to functional limitations in adulthood. Progressive subluxation and excessive loading of the triple joint complex and the spring ligament may occur, ultimately leading to late articular degeneration. This overloading is clinically responsible for fatigue, pain, and mechanical insufficiency.
The extra-articular technique known as calcaneo-stop involves the insertion of a screw into the calcaneus, effectively blocking excessive talus-calcaneus pronation and subsequent subluxations.[17] Moreover, research[15] [26] [27] suggests that, besides joint restriction, proprioceptive mechanisms influence gait kinetics. Unlike osteotomies, which immediately alter joint relationships and load distribution, arthroereisis induces an early correction of the deformities, followed by a late gradual three-dimensional articular reorganization over several months, leading to articular remodeling.
Lateral column lengthening osteotomies and medialization of the calcaneus are accepted treatments for symptomatic flexible flatfoot in the immature foot, with reported satisfactory results of approximately 90%.[8] [9] [10] However, these procedures are more invasive, require longer recovery time, and impose activity restrictions for weeks. In contrast, arthroereisis results in a fast rehabilitation, enabling the patient to walk shortly after surgery.[13] [17] [27] [28] Nevertheless, in the present series, 42% of the patients underwent Achilles tendon lengthening and required plaster immobilization for up to 21 days. For the remaining patients, weight bearing was allowed on the seventh postoperative day. Conversely, some authors[15] do not routinely release the triceps surae, even in the presence of equinus, arguing that the postoperative equinus can be reversed with physiotherapy.
While clinico-radiographic dissociation exists, we employed angular parameters to evaluate and enhance the objectivity and reproducibility of the results. Nonetheless, these variables may not directly correlate with the symptoms and severity of the foot. Moreover, establishing the most significant signals for the diagnosis and determining the precise threshold to define a foot as a flat remains challenging. The relevance of radiographic measures and flatfoot diagnosis is still under debate.[23]
Our radiographic assessments revealed improvement in hindfoot and midfoot parameters over a mean follow-up period of 28 months, which is consistent with the findings of previous studies.[19] [27] [28] The clinical outcomes were deemed satisfactory, with 90% of the patients reporting no pain. The complication rate was 13.6%, but they were minor complications, primarily attributed to pain that showed improvement following analgesic treatment. Our data and complication rates are similar to those reported in other studies.[19] [20] [27]
Determining the optimal time for implant removal without compromising correction remains uncertain in the calcaneo-stop technique. Some authors[11] [29] suggest removal after 2 years, during which joint remodeling and proprioceptive reflex incorporation occur. However, establishing a removal protocol in the present study was challenging due to high hospital service demands. As a result, most of the patients retained the implant for up to 5 years without experiencing overcorrection, pain, or breakage. The radiographic images showed no evidence of any impression on the talus secondary to prolonged contact at the implant interface. However, we did not precisely evaluate this parameter due to limited symptoms.
The current study has limitations, including a restricted sample size. Moreover, we faced challenges in quantifying the subjective and variable nature of pain and discomfort in a pediatric population and in establishing a correlation between the radiographic parameters and the clinical findings of the flatfoot.
Overall, our impression is that the calcaneo-stop technique seems to be an adequate option to treat symptomatic flexible flatfoot in juvenile patients, according to major studies.[30] [31] It offers potential correction of the initial deformity and consistent improvement in clinical and radiographic parameters. Furthermore, the technique can be reversed through screw removal if necessary, and it does not compromise the use of other techniques in cases of failure. There are still questions regarding joint remodeling and possible long-term repercussions; however, the technique seems promising.
Conflito de Interesses
Os autores não têm conflito de interesses a declarar.
Work developed at the Departament of Orthopedics and Anesthesiology, Hospital das Clínicas, Faculdade de Medicina de Ribeirão Preto, Universidade de São Paulo, Ribeirão Preto, SP, Brazil.
-
Referências
- 1 Volpon JB. Footprint analysis during the growth period. J Pediatr Orthop 1994; 14 (01) 83-85
- 2 Vulcano E, Maccario C, Myerson MS. How to approach the pediatric flatfoot. World J Orthop 2016; 7 (01) 1-7
- 3 Needleman RL. Current topic review: subtalar arthroereisis for the correction of flexible flatfoot. Foot Ankle Int 2005; 26 (04) 336-346
- 4 Mosca VS. Flexible flatfoot in children and adolescents. J Child Orthop 2010; 4 (02) 107-121
- 5 Whitford D, Esterman A. A randomized controlled trial of two types of in-shoe orthoses in children with flexible excess pronation of the feet. Foot Ankle Int 2007; 28 (06) 715-723
- 6 Molina-García C, Banwell G, Rodríguez-Blanque R. et al. Efficacy of Plantar Orthoses in Paediatric Flexible Flatfoot: A Five-Year Systematic Review. Children (Basel) 2023; 10 (02) 371
- 7 Jones BS. Flat foot. A preliminary report of an operation for severe cases. J Bone Joint Surg Br 1975; 57 (03) 279-282
- 8 Evans D. Calcaneo-valgus deformity. J Bone Joint Surg Br 1975; 57 (03) 270-278
- 9 Koutsogiannis E. Treatment of mobile flat foot by displacement osteotomy of the calcaneus. J Bone Joint Surg Br 1971; 53 (01) 96-100
- 10 Mosca VS. Calcaneal lengthening for valgus deformity of the hindfoot. Results in children who had severe, symptomatic flatfoot and skewfoot. J Bone Joint Surg Am 1995; 77 (04) 500-512
- 11 LeLièvre J. Current concepts and correction in the valgus foot. Clin Orthop Relat Res 1970; 70 (70) 43-55
- 12 Crawford AH, Kucharzyk D, Roy DR, Bilbo J. Subtalar stabilization of the planovalgus foot by staple arthroereisis in young children who have neuromuscular problems. J Bone Joint Surg Am 1990; 72 (06) 840-845
- 13 Jerosch J, Schunck J, Abdel-Aziz H. The stop screw technique–a simple and reliable method in treating flexible flatfoot in children. Foot Ankle Surg 2009; 15 (04) 174-178
- 14 Grice DS. An extra-articular arthrodesis of the subastragalar joint for correction of paralytic flat feet in children. J Bone Joint Surg Am 1952; 34 A (04) 927-940 , passim
- 15 De Pellegrin M. Die subtalare Schrauben-Arthrorise beim kindlichen Plattfuss. Orthopade 2005; 34 (09) 941-953 , quiz 954
- 16 Subotnick SI. The subtalar joint lateral extra-articular arthroereisis: a follow-up report. J Am Podiatry Assoc 1977; 67 (03) 157-171
- 17 Álvarez R. Calcáneo-Stop: Técnica Personal Para El Tratamiento Quirúrgico Del Pie Plano Del Niño y Del Adolescente Joven. In: Epeldelgui T. ed. Pie plano y anomalias del antepie. Madrid, Spain: Madrid Vicente; 1995: 174-177
- 18 Pisani G. Trattato Di Chirurgia Del Piede. 2nd ed. Torino: Minerva Medica; 1993
- 19 Costa FP, Costa G, Carvalho MS, Moura AM, Pinto R, Torres J. Long-Term Outcomes of the Calcâneo-Stop Procedure in the Treatment of Flexible Flatfoot in Children: A Retrospective Study. Acta Med Port 2017; 30 (7-8): 541-545
- 20 Pavone V, Vescio A, Di Silvestri CA, Andreacchio A, Sessa G, Testa G. Outcomes of the Calcâneo-Stop procedure for the treatment of juvenile flatfoot in young athletes. J Child Orthop 2018; 12 (06) 582-589
- 21 Fucs PMMB, Svartman C, Kertzman P, Kubasara A, Bussolaro F, Rosseti F. Tratamento do pé plano-valgo espástico pela artrorrise de Pisani. Rev Bras Ortop 1997; 32 (02) 145-152
- 22 Paley D. Problems, obstacles, and complications of limb lengthening by the Ilizarov technique. Clin Orthop Relat Res 1990; (250) 81-104
- 23 Benedetti MG, Berti L, Straudi S, Ceccarelli F, Giannini S. Clinicoradiographic assessment of flexible flatfoot in children. J Am Podiatr Med Assoc 2010; 100 (06) 463-471
- 24 Davids JR, Gibson TW, Pugh LI. Quantitative segmental analysis of weight-bearing radiographs of the foot and ankle for children: normal alignment. J Pediatr Orthop 2005; 25 (06) 769-776
- 25 Basmajian JV, Stecko G. The Role of Muscles in Arch Support of the foot. J Bone Joint Surg Am 1963; 45: 1184-1190
- 26 Christensen JC, Campbell N, DiNucci K. Closed kinetic chain tarsal mechanics of subtalar joint arthroereisis. J Am Podiatr Med Assoc 1996; 86 (10) 467-473
- 27 Roth S, Sestan B, Tudor A, Ostojic Z, Sasso A, Durbesic A. Minimally invasive Calcâneo-Stop method for idiopathic, flexible pes planovalgus in children. Foot Ankle Int 2007; 28 (09) 991-995
- 28 Pavone V, Costarella L, Testa G, Conte G, Riccioli M, Sessa G. Calcâneo-Stop procedure in the treatment of the juvenile symptomatic flatfoot. J Foot Ankle Surg 2013; 52 (04) 444-447
- 29 Carranza-Bencano A, Duque-Gimeno V, Gomez-Arroyo JA, Zurita-Gutierrez M. Giannini's prosthesis in the treatment of juvenile flatfoot. J Foot Ankle Surg 2000; 6 (01) 11-17
- 30 De Pellegrin M, Moharamzadeh D. Subtalar Arthroereisis for Surgical Treatment of Flexible Flatfoot. Foot Ankle Clin 2021; 26 (04) 765-805
- 31 Smith C, Zaidi R, Bhamra J, Bridgens A, Wek C, Kokkinakis M. Subtalar arthroereisis for the treatment of the symptomatic paediatric flexible pes planus: a systematic review. EFORT Open Rev 2021; 6 (02) 118-129
Endereço para correspondência
Publication History
Received: 30 March 2024
Accepted: 06 November 2024
Article published online:
11 April 2025
© 2025. The Author(s). This is an open access article published by Thieme under the terms of the Creative Commons Attribution 4.0 International License, permitting copying and reproduction so long as the original work is given appropriate credit (https://creativecommons.org/licenses/by/4.0/)
Thieme Revinter Publicações Ltda.
Rua Rego Freitas, 175, loja 1, República, São Paulo, SP, CEP 01220-010, Brazil
Leonardo Lima de Almeida, Paulo Henrique Bortolin, Diego Polizello, Leonardo Rigobello Bataglion, José Batista Volpon. Calcâneo-stop: Uma técnica cirúrgica eficaz para a correção do pé plano valgo flexível sintomático em crianças. Rev Bras Ortop (Sao Paulo) 2025; 60: s00451804494.
DOI: 10.1055/s-0045-1804494
-
Referências
- 1 Volpon JB. Footprint analysis during the growth period. J Pediatr Orthop 1994; 14 (01) 83-85
- 2 Vulcano E, Maccario C, Myerson MS. How to approach the pediatric flatfoot. World J Orthop 2016; 7 (01) 1-7
- 3 Needleman RL. Current topic review: subtalar arthroereisis for the correction of flexible flatfoot. Foot Ankle Int 2005; 26 (04) 336-346
- 4 Mosca VS. Flexible flatfoot in children and adolescents. J Child Orthop 2010; 4 (02) 107-121
- 5 Whitford D, Esterman A. A randomized controlled trial of two types of in-shoe orthoses in children with flexible excess pronation of the feet. Foot Ankle Int 2007; 28 (06) 715-723
- 6 Molina-García C, Banwell G, Rodríguez-Blanque R. et al. Efficacy of Plantar Orthoses in Paediatric Flexible Flatfoot: A Five-Year Systematic Review. Children (Basel) 2023; 10 (02) 371
- 7 Jones BS. Flat foot. A preliminary report of an operation for severe cases. J Bone Joint Surg Br 1975; 57 (03) 279-282
- 8 Evans D. Calcaneo-valgus deformity. J Bone Joint Surg Br 1975; 57 (03) 270-278
- 9 Koutsogiannis E. Treatment of mobile flat foot by displacement osteotomy of the calcaneus. J Bone Joint Surg Br 1971; 53 (01) 96-100
- 10 Mosca VS. Calcaneal lengthening for valgus deformity of the hindfoot. Results in children who had severe, symptomatic flatfoot and skewfoot. J Bone Joint Surg Am 1995; 77 (04) 500-512
- 11 LeLièvre J. Current concepts and correction in the valgus foot. Clin Orthop Relat Res 1970; 70 (70) 43-55
- 12 Crawford AH, Kucharzyk D, Roy DR, Bilbo J. Subtalar stabilization of the planovalgus foot by staple arthroereisis in young children who have neuromuscular problems. J Bone Joint Surg Am 1990; 72 (06) 840-845
- 13 Jerosch J, Schunck J, Abdel-Aziz H. The stop screw technique–a simple and reliable method in treating flexible flatfoot in children. Foot Ankle Surg 2009; 15 (04) 174-178
- 14 Grice DS. An extra-articular arthrodesis of the subastragalar joint for correction of paralytic flat feet in children. J Bone Joint Surg Am 1952; 34 A (04) 927-940 , passim
- 15 De Pellegrin M. Die subtalare Schrauben-Arthrorise beim kindlichen Plattfuss. Orthopade 2005; 34 (09) 941-953 , quiz 954
- 16 Subotnick SI. The subtalar joint lateral extra-articular arthroereisis: a follow-up report. J Am Podiatry Assoc 1977; 67 (03) 157-171
- 17 Álvarez R. Calcáneo-Stop: Técnica Personal Para El Tratamiento Quirúrgico Del Pie Plano Del Niño y Del Adolescente Joven. In: Epeldelgui T. ed. Pie plano y anomalias del antepie. Madrid, Spain: Madrid Vicente; 1995: 174-177
- 18 Pisani G. Trattato Di Chirurgia Del Piede. 2nd ed. Torino: Minerva Medica; 1993
- 19 Costa FP, Costa G, Carvalho MS, Moura AM, Pinto R, Torres J. Long-Term Outcomes of the Calcâneo-Stop Procedure in the Treatment of Flexible Flatfoot in Children: A Retrospective Study. Acta Med Port 2017; 30 (7-8): 541-545
- 20 Pavone V, Vescio A, Di Silvestri CA, Andreacchio A, Sessa G, Testa G. Outcomes of the Calcâneo-Stop procedure for the treatment of juvenile flatfoot in young athletes. J Child Orthop 2018; 12 (06) 582-589
- 21 Fucs PMMB, Svartman C, Kertzman P, Kubasara A, Bussolaro F, Rosseti F. Tratamento do pé plano-valgo espástico pela artrorrise de Pisani. Rev Bras Ortop 1997; 32 (02) 145-152
- 22 Paley D. Problems, obstacles, and complications of limb lengthening by the Ilizarov technique. Clin Orthop Relat Res 1990; (250) 81-104
- 23 Benedetti MG, Berti L, Straudi S, Ceccarelli F, Giannini S. Clinicoradiographic assessment of flexible flatfoot in children. J Am Podiatr Med Assoc 2010; 100 (06) 463-471
- 24 Davids JR, Gibson TW, Pugh LI. Quantitative segmental analysis of weight-bearing radiographs of the foot and ankle for children: normal alignment. J Pediatr Orthop 2005; 25 (06) 769-776
- 25 Basmajian JV, Stecko G. The Role of Muscles in Arch Support of the foot. J Bone Joint Surg Am 1963; 45: 1184-1190
- 26 Christensen JC, Campbell N, DiNucci K. Closed kinetic chain tarsal mechanics of subtalar joint arthroereisis. J Am Podiatr Med Assoc 1996; 86 (10) 467-473
- 27 Roth S, Sestan B, Tudor A, Ostojic Z, Sasso A, Durbesic A. Minimally invasive Calcâneo-Stop method for idiopathic, flexible pes planovalgus in children. Foot Ankle Int 2007; 28 (09) 991-995
- 28 Pavone V, Costarella L, Testa G, Conte G, Riccioli M, Sessa G. Calcâneo-Stop procedure in the treatment of the juvenile symptomatic flatfoot. J Foot Ankle Surg 2013; 52 (04) 444-447
- 29 Carranza-Bencano A, Duque-Gimeno V, Gomez-Arroyo JA, Zurita-Gutierrez M. Giannini's prosthesis in the treatment of juvenile flatfoot. J Foot Ankle Surg 2000; 6 (01) 11-17
- 30 De Pellegrin M, Moharamzadeh D. Subtalar Arthroereisis for Surgical Treatment of Flexible Flatfoot. Foot Ankle Clin 2021; 26 (04) 765-805
- 31 Smith C, Zaidi R, Bhamra J, Bridgens A, Wek C, Kokkinakis M. Subtalar arthroereisis for the treatment of the symptomatic paediatric flexible pes planus: a systematic review. EFORT Open Rev 2021; 6 (02) 118-129