

Subscribe to RSS
DOI: 10.1055/s-0045-1805055
Pulmonary Embolism and Posterior Circulation Infarcts Following Position Change from Prone to Supine during Cervical Spine Surgery: A Case Report
Authors


Abstract
Acute massive pulmonary embolism (PE) is a lethal condition unless promptly detected and managed. Diagnosing and managing massive PE during the perioperative period can be challenging due to overlapping clinical signs with other complications. This case report highlights the challenges of diagnosing and managing a massive PE in a patient with morbid obesity who underwent instrumentation of the cervical spine at multiple levels and developed cardiac arrest while turning the patient supine from the prone position. With the help of focused cardiac ultrasound, we suspected PE, which was later confirmed on imaging. Postoperative brain imaging also confirmed the presence of multiple embolic infarcts in the occipital and cerebellar hemispheres.
Keywords
pulmonary embolism - prone position - cervical vertebral fusion - vertebral artery insufficiency - posterior circulation brain infarctionIntroduction
Pulmonary embolism (PE) is the third most prevalent cardiovascular condition following myocardial infarction and stroke.[1] The outcome of a massive intraoperative PE is often fatal, and its diagnosis and management, especially in the perioperative period, can be extremely challenging.[2] A high degree of clinical suspicion, presence of risk factors, thorough evaluation, and point-of-care imaging are essential in diagnosing and managing PE. We present a case of sudden cardiac arrest caused by a massive PE after turning a patient from prone to supine following cervical spine surgery. The patient was later found to have multiple embolic infarcts in the posterior circulation, affecting the occipital lobes and cerebellar hemispheres.
Case Report
A 46-year-old male, American Society Anesthesiologist (ASA) physical class III with hypertension and obesity (BMI 40 kg/m2), was admitted for cervical spine surgery due to progressive myelopathy secondary to ossified posterior longitudinal ligament (C2–D3 vertebral levels). The patient could walk with support and perform daily activities. The patient had obstructive sleep apnea (OSA) with a STOP-BANG score of 5, and was advised to use continuous positive airway pressure (CPAP) during the night. Preoperative assessments, including routine blood investigations, 2D echocardiography, and pulmonary function tests were normal with no history of deep vein thrombosis (DVT) or clotting disorders.
The patient underwent posterior decompression and fusion of the C2–D3 vertebrae with motor evoked potential (MEP) monitoring. Anesthesia was induced, and the trachea was intubated with an 8.0-mm flexometallic endotracheal tube. Anesthesia was maintained with propofol (3–5 mg/kg/h) targeted to keep a bispectral index (BIS) of 45 to 55, fentanyl (0.5 µg/kg/h), and dexmedetomidine (0.2–0.5 µg/kg/h) to facilitate MEP monitoring. Intermittent pneumatic pumps were applied to both legs as per the institutional protocol. During the 10-hours surgery, intraoperative vitals were stable except for reduced urine output (total intraoperative urine output = 350 mL). Urine output did not improve despite ruling out mechanical obstruction and administering fluid challenges and diuretics. Blood loss was 1,200 mL, replaced with 2 units of packed red blood cells.
Due to OSA and prolonged prone surgery, elective postoperative ventilation was planned. The patient was turned supine, and the flexometallic tube was exchanged for a polyvinyl chloride endotracheal tube in one attempt. In next few minutes, the patient developed nonspecific arrhythmias, followed by bradycardia, hypotension, and asystole.
Cardiopulmonary resuscitation (CPR) was initiated, and return of spontaneous circulation was achieved after three cycles of CPR. A central line was placed, and inotropes (noradrenaline and adrenaline) were started.
A cardiology consultation and focused cardiac ultrasound (FOCUS) revealed normal right atrium (RA) and right ventricle (RV) size, hypercontractility of the left heart, and no thrombus. The patient had the end-tidal CO2 (EtCO2) of 20 to 24 mm Hg, while ABG revealed a pH of 6.86, PaCO2 of 85.4 mm Hg, PaO2 of 124 mm Hg, lactate of 9.6 mmol/L, and HCO3 − of 9.7 mmol/L. The patient was transferred to the intensive care unit (ICU). Despite improvement in oxygen saturation and blood pressure, his EtCO2 remained low (∼18–24 mm Hg). In the ICU, PaCO2 increased to even higher values of approximately 110 to 120 mm Hg, while EtCO2 remained in the range of 18 to 24 mm Hg. A persistently high PaCO2–EtCO2 gradient (∼90 mm Hg) raised a strong suspicion for PE.
A repeat FOCUS in the ICU showed dilated RA/RV and paradoxical septal motion, suggesting PE. A computed tomography pulmonary angiogram (CTPA) confirmed a saddle embolism in the main pulmonary artery extending into the right and left pulmonary arteries ([Fig. 1]). The risk-to-benefit ratio of administering unfractionated heparin was discussed with the surgical team. Given the life-threatening nature of the condition, intravenous unfractionated heparin 5,000 IU was administered, followed by embolectomy in the interventional suite (∼6 h later).

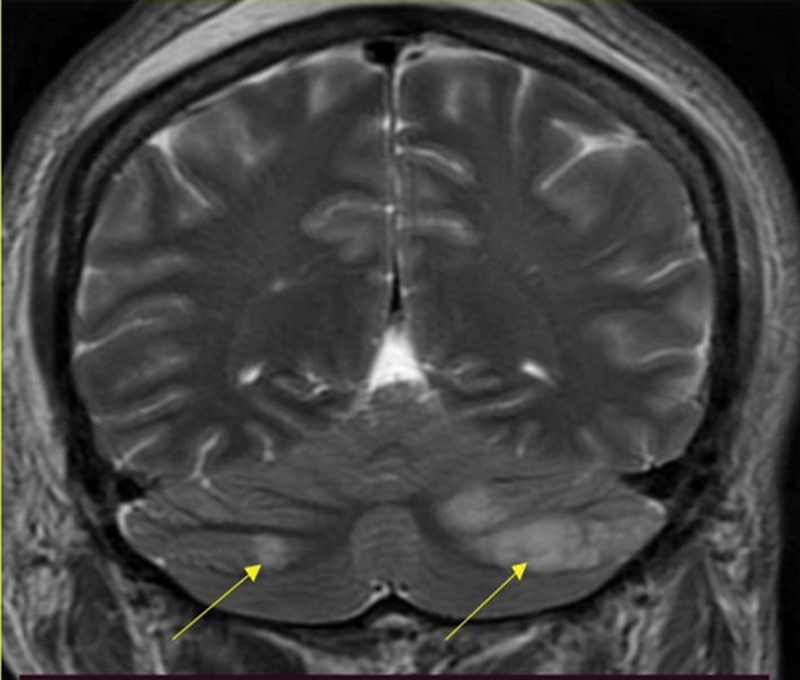
Postembolectomy, the patient's urine output improved, and hemodynamics stabilized. However, the patient's consciousness remained impaired (Glasgow coma scale [GCS] of E1VTM1) with sluggish reaction in bilateral pupils. Brain MRI revealed multiple embolic infarcts in the occipital and cerebellar hemispheres (left > right), as well as left vertebral artery thrombosis ([Fig. 2]). Doppler ultrasound of the lower limbs showed no evidence of DVT.
The patient remained in the ICU for 10 days, during which his GCS improved to E4VTM3 (tracheostomy). After 40 days, the patient was discharged with a GCS of E4VTM3 on oral anticoagulant. At present (6 months after surgery), the patient has improved to E4VTM6 with 2/5 power in all four limbs.
Discussion
This case underscores the diagnostic challenges of massive PE during cervical spine surgery in the prone position, with risk factors including obesity, OSA, reduced mobility, prolonged prone positioning, and blood transfusion.
Obesity is associated with venous stasis, chronic inflammation, and hypercoagulability, increasing PE risk.[3] OSA predisposes patients to higher risk of DVT and PE (3.50- to 3.97-fold higher).[4] Blood transfusion can disrupt coagulation, enhance inflammatory cascades, and alter red cell properties, further increasing thrombotic risk.[5]
The prone position exacerbates venous stasis by hindering lower extremity venous return and compressing iliac vessels, promoting thrombus formation.[6] We hypothesize that the clot formed in this position and migrated upon supine repositioning as vessel compression was relieved.
Diagnosing PE intraoperatively or immediate in postoperative period is particularly challenging due to overlapping clinical features with other conditions, such as myocardial infarction or hypovolemia. In this case, the sudden bradycardia, hypotension, and asystole after repositioning suggested a cardiovascular event.
Despite hemodynamic stabilization, the patient developed significant neurological complications, with brain MRI showing embolic infarcts in the occipital and cerebellar hemispheres. A thrombus located in the V4 segment of the left vertebral artery can contribute to quadriparesis due to lateral cord infarction (involving the posterior inferior cerebellar artery).[7] Vertebral artery injuries (0.8–1.4%) are rare but recognized complications of cervical spine surgery, especially during vertebral drilling and instrumentation.[7] These injuries can lead to arterial rupture, dissection, pseudoaneurysm, or thrombosis, resulting in bleeding, hypotension, or posterior circulation infarction.[8]
This case highlights the critical need for thorough preoperative risk assessment, prehabilitation (such as weight reduction and CPAP therapy),[9] and early thromboprophylaxis in high-risk patients. Strategies like minimizing operative time, staging procedures, and optimizing positioning to minimize venous stasis can reduce thrombotic risk. Vigilant perioperative monitoring, along with prompt point-of-care imaging, ensures early detection and management of complications. Additionally, vertebral artery injury led to adverse neurological outcomes, highlighting the importance of vigilant monitoring, meticulous surgical technique, and prompt intervention to improve patient outcomes.
Conflict of Interest
None declared.
-
References
- 1 Pharo GH, Andonakakis A, Chandrasekaren K, Amron G, Levitt JD. Survival from catastrophic intraoperative pulmonary embolism. Anesth Analg 1995; 81 (01) 188-190
- 2 Sharma J, Walia HS, Jaswal S, Goyal A. Diagnosis and management of intra-operative pulmonary embolism under general anaesthesia in a peripheral tertiary care centre with limited resources. Indian J Anaesth 2022; 66 (Suppl. 02) S131-S132
- 3 Hotoleanu C. Association between obesity and venous thromboembolism. Med Pharm Rep 2020; 93 (02) 162-168
- 4 Peng YH, Liao WC, Chung WS. et al. Association between obstructive sleep apnea and deep vein thrombosis / pulmonary embolism: a population-based retrospective cohort study. Thromb Res 2014; 134 (02) 340-345
- 5 Hovav T, Yedgar S, Manny N, Barshtein G. Alteration of red cell aggregability and shape during blood storage. Transfusion 1999; 39 (03) 277-281
- 6 Gebhard CE, Zellweger N, Gebhard C. et al. Prone positioning as a potential risk factor for deep vein thrombosis in covid-19 patients: a hypothesis generating observation. J Clin Med 2021; 11 (01) 103
- 7 Yi HJ. Epidemiology and management of iatrogenic vertebral artery injury associated with cervical spine surgery. Korean J Neurotrauma 2022; 18 (01) 34-44
- 8 Yee TJ, Swong K, Park P. Complications of anterior cervical spine surgery: a systematic review of the literature. J Spine Surg 2020; 6 (01) 302-322
- 9 Vasu TS, Grewal R, Doghramji K. Obstructive sleep apnea syndrome and perioperative complications: a systematic review of the literature. J Clin Sleep Med 2012; 8 (02) 199-207
Address for correspondence
Publication History
Article published online:
29 April 2025
© 2025. The Author(s). This is an open access article published by Thieme under the terms of the Creative Commons Attribution License, permitting unrestricted use, distribution, and reproduction so long as the original work is properly cited. (https://creativecommons.org/licenses/by/4.0/)
Thieme Medical and Scientific Publishers Pvt. Ltd.
A-12, 2nd Floor, Sector 2, Noida-201301 UP, India
-
References
- 1 Pharo GH, Andonakakis A, Chandrasekaren K, Amron G, Levitt JD. Survival from catastrophic intraoperative pulmonary embolism. Anesth Analg 1995; 81 (01) 188-190
- 2 Sharma J, Walia HS, Jaswal S, Goyal A. Diagnosis and management of intra-operative pulmonary embolism under general anaesthesia in a peripheral tertiary care centre with limited resources. Indian J Anaesth 2022; 66 (Suppl. 02) S131-S132
- 3 Hotoleanu C. Association between obesity and venous thromboembolism. Med Pharm Rep 2020; 93 (02) 162-168
- 4 Peng YH, Liao WC, Chung WS. et al. Association between obstructive sleep apnea and deep vein thrombosis / pulmonary embolism: a population-based retrospective cohort study. Thromb Res 2014; 134 (02) 340-345
- 5 Hovav T, Yedgar S, Manny N, Barshtein G. Alteration of red cell aggregability and shape during blood storage. Transfusion 1999; 39 (03) 277-281
- 6 Gebhard CE, Zellweger N, Gebhard C. et al. Prone positioning as a potential risk factor for deep vein thrombosis in covid-19 patients: a hypothesis generating observation. J Clin Med 2021; 11 (01) 103
- 7 Yi HJ. Epidemiology and management of iatrogenic vertebral artery injury associated with cervical spine surgery. Korean J Neurotrauma 2022; 18 (01) 34-44
- 8 Yee TJ, Swong K, Park P. Complications of anterior cervical spine surgery: a systematic review of the literature. J Spine Surg 2020; 6 (01) 302-322
- 9 Vasu TS, Grewal R, Doghramji K. Obstructive sleep apnea syndrome and perioperative complications: a systematic review of the literature. J Clin Sleep Med 2012; 8 (02) 199-207