

Subscribe to RSS
DOI: 10.1055/s-0045-1806813
Ultrasound-guided continuous radiofrequency ablation of the proximal greater occipital nerve is effective in refractory occipital neuralgia: a retrospective cohort study
Authors

Abstract
Background
Pain in occipital neuralgia (ON) originates from the upper cervical nerves converging with the trigeminal complex. Greater occipital nerve (GON) blocks and radiofrequency treatments can be used in refractory ON.
Objective
To assess the efficacy of ultrasound-guided proximal greater occipital nerve (PGON) continous radiofrequency ablation (CRFA) in ON throughout 1 year.
Methods
We analyzed data from medical records and headache diaries. Before the intervention and 1, 3, 6, and 12 months after the intervention, at each appointment we evaluated the headache intensity through the 11-point Numeric Rating Scale (NRS-11), the headache disability, through the Six-Item Headache Impact Test (HIT-6), as well as the headache days per month. Treatment efficacy was determined by NRS-11 score < 4 at 12 months.
Results
A total of 18 patients were analyzed. The mean initial NRS-11 score was of 8.78 ± 0.732. At least 50% of pain reduction was noted in all patients at 6 months, and in 66% patients at 12 months. The frequency of attacks was correlated to poor response (r = 0.598; p = 0.009). The efficacy of the diagnostic block was correlated to successful response (r = -0.789; p = 0.001). For the categorical variables, the electric shock pain was associated with NRS-11 score ≥ 4 (p = 0.041), and lancinating pain was associated with NRS-11 score < 4 at 12 months (p = 0.031).
Conclusion
Ultrasound-guided PGON CRFA in refractory ON significantly reduced pain for up to 1 year. The initial frequency of attacks, electric shock like pain, and reduced response to diagnostic block were associated with reduced response.
Keywords
Neuralgia - Headache - Radiofrequency Ablation - Nerve Block - Ultrasonography, Interventional - Pain Measurement - Treatment OutcomeINTRODUCTION
Occipital neuralgia (ON) is a unilateral or bilateral paroxysmal shooting or stabbing pain that occurs in the posterior region of the scalp and is characterized by the distribution of the greater occipital nerve (GON), the lesser occipital nerve (LON), or the third occipital nerve (TON).[1] Tenderness over the affected nerve and occasionally decreased sensation or dysesthesia in the affected area are common symptoms of the disease.[2] It often causes severe pain that impairs function and quality of life.[3] Most cases of ON are idiopathic and have no clearly-defined anatomical cause.[2] Initially, conservative treatment approaches such as medication and physiotherapy are often used. If conservative measures fail to alleviate ON, interventional treatments are available.[3] [4]
Radiofrequency ablation (RFA) has been shown to be effective in ON in previous studies.[4] Three RFA techniques have been used to treat ON, including continuous radiofrequency ablation (CRFA), pulsed radiofrequency (PRF) and cooled RFA.[4] However, the mechanism of action of the three RFA techniques is different, so their effectiveness in the treatment of ON may vary. In PRF, radio waves are delivered to the nerve in a pulsed sequence and at temperatures lower than 42°C.[4]
Researchers have investigated the use of PRF for the treatment of ON. The GON PRF has led to a significant improvement in pain scores and quality of life, as well as a reduction in the use of pain medication. However, its effectiveness only lasted for a short period.[5] [6] [7] [8] [9] [10] Continous RFA differs slightly from PRF in that it destroys tissue at a temperature higher than 42°C and interrupts pain by causing Wallerian degeneration. The pain interruption is longer and stronger than with PRF. However, side effects such as hyperesthesia, dysesthesia, and deafferentation pain have been observed more often than with PRF.[11] Cooled RFA is a relatively new technique developed to enlarge the lesion.[4]
As the GON is a purely sensory nerve, CRFA could be an alternative treatment option for ON with longer duration and more efficient than PRF.[4] A few studies[11] [12] [13] [14] have been published in the literature on the effectiveness of CRFA for ON under fluoroscopic control at the cervical 2 dorsal root ganglion (C2 DRG; defined as very proximal) or the external prominence (defined as distal), but these studies reported terrible side effects.
Ultrasound (US) could be used safely to determine the proximal GON (PGON) between the semispinalis capitis muscle and the obliquus inferior muscle at the level of C2.[15] Therefore, here, GON block might be more effective and safer. In the past, US-guided PGON block for chronic migraine, ON, and cervicogenic headache was considered more effective than distal GON (DGON) block performed at the external prominence.[16] [17] [18] In patients with chronic migraine, US-guided PRF of the PGON has already shown promise.[19] However, no study was found on the efficacy of US-guided CRFA of the PGON for ON.
Our hypothesis is that CRFA of the PGON might provide to ON patients a longer and more efficient treatment compared to previous studies, with fewer side effects. The main goal of the present study was to evaluate the efficacy of US-guided CRFA of the PGON in refractory ON throughout 1 year. The secondary aim was to determine the parameters related to treatment efficacy, which was defined by NRS score < 4 at 12 months follow-up.[20]
METHODS
Standard protocol approval and patient consent
In accordance with the Declaration of Helsinki, the institutional Ethics Committee approved the current retrospective cohort study (reference number/date 2024-446/22.05.2024), with ClinicalTrials.gov Protocol Registration and Results System (PRS) NCT06458179. Informed consent was obtained from all participants.
Study design and participants
Inclusion criteria
Between January 1, 2022, and April 30, 2023, all patients with primary unilateral ON who underwent US-guided diagnostic occipital nerve block and subsequent CRFA of the PGON in the Department of Pain Medicine and who were followed up for at least 1 year were identified and included.
Exclusion citeria
Patients who were unable to communicate, lacked documentation, or had inadequate follow-up were excluded. Patients were also excluded if they had received a new pain medication during the follow-up period that would have affected the assessment of their outcomes. Patients with bilateral ON, secondary ON (such as, cervical radiculopathy, infection, tumor, vascular compression of the nerve, musculoskeletal conditions such as C1-2 osteoarthritis etc.), other primary headaches, dermatitis or skin infections, and pacemakers were also excluded from the study.
Diagnosis
A diagnosis of ON was made based on the clinical history and neurological examination (including the Tinel test). A differential diagnosis of secondary ON was also made based on the results of hormonal and biochemical tests and imaging studies of the brain and cervical spine, such as X-rays or magnetic resonance imaging (MRI) scans, if needed. In total,3 patients had undergone brain and cervical spine MRI: 1 had cervical and 3-disc pathology, on MRI and were excluded from the study; the scans of the other 2 patients were within normal ranges.
In total, 22 out of the 34 patients with primary ON received PGON CRFA therapy. We only analyzed 18 of these patients because 4 of them were excluded because they did did not return for follow-up: 2 patients did not come to the sixth monthly visit, 1 patient moved to a different city in the third month, and 1 patient did not come for a check-up after 12 months. None of these patients complained of any side effects during the follow-up. However, as they were unable to complete the 12-month follow-up, we excluded them from the analysis. [Figure 1] shows the flow chart of the study.

Medical treatment and intervention
Patients who did not respond to drug therapy received a diagnostic block (duloxetine 60 mg/day, pregabalin 300 mg/day, or carbamazepine 800 mg/day) and postural training against muscle tension for at least 3 months. If the response to the diagnostic block was higher than 50%, we initiated CRFA at the next visit.
In our routine outpatient pain medicine practice, we used a US machine with a 13 MHz to 5 MHz linear probe (Voluson E6, GE Healthcare, Chicago, IL, United States) to perform the diagnostic block and CRFA of the PGON without anesthesia in the operating room. During the diagnostic block, a 3-mL injection of bupivacaine 0.025% (Buvasin 0.5%, VEM İlaç, Istanbul, Republic of Türkiye) was administered. The block was considered successful if it could be maintained with more than 50% of relief for at least 1 hour. After 1 week of successful block, CRFA was performed.
Continous RFA was performed with a radiofrequency (RF) device (TOP Lesion Generator, model TLG-10, TOP Corporation, Tokyo, Japan) under US guidance in the operating room. The patient was monitored for vital signs in the prone position with the head slightly flexed. After disinfection, the probe was inserted transversely into the neck. After the occipital protuberance was visualized, the probe was pushed down to find the bifid spinous process of C2. The probe was lateralized (toward the affected side) to identify the semispinalis capitis muscle and the obliquus capitis inferior muscle ([Figure 2A]). In this position, the GON was placed between the muscles. A 21-G 5-mm RF needle with an active tip and a length of 60 mm (SC-K; TOP Neuropole, TOP Corporation) was used to treat the nerve from medial to lateral under ultrasound. ([Figure 2B]). Sensory stimulation was administered at 50 Hz for 1 ms to determine the location of the nerve after accurate placement of the needle tip. A voltage lower than 0.5 V was required to elicit paresthesia, pain or irritation in the nerve distribution during sensory stimulation. In addition, a motor stimulus was applied at 2 Hz for 1 ms and up to 2 V to check that no fasciculations were present. After negative aspiration of blood or fluid, 1 mL of 2% lidocaine was injected with the RF cannulas to relieve procedural pain. Continuous RFA was performed at a temperature of 60°C for 90 s. Immediately after the procedure, 2 mg of dexamethasone were injected into each lesion site to minimize the risk of neuritis. All adverse events after the procedure were documented for each subject.

Outcome measures and follow-up
At the initial examination, the patient's demographic data and headache symptoms were thoroughly examined. In accordance with the recommendation of the Turkish National Headache and Pain Research Association, patients were asked to keep a headache diary for the duration of treatment and all subsequent appointments. Headache intensity, headache disability, and the number of headache days per month, as well as the use of non-steroidal anti-inflammatory drugs (NSAIDs), were determined from the diaries and discussed with the patient at each session.
The intensity of the headaches was measured at each appointment (before the intervention, and 1, 3, 6, and 12 months after the intervention) using the 11-point Numeric Rating Scale (NRS-11), a 1-dimensional scale that measures pain intensity in adults. The participant is asked to choose a number that best reflects the intensity of pain: 0 = no pain; 1 to 3 mild pain; 4 to 7 moderate pain; and 8 to 10 severe pain (with 10 indicating the worst pain imaginable). Treatment efficacy was defined as no pain or mild pain with NRS-11 score < 4 in the first year.[20]
Headache disability was assessed at each appointment using the Six-Item Headache Impact Test (HIT-6). The final score on the HIT-6 ranges from 36 to 78 points: minimal influence (≤ 49 points); considerable impact (50–55 points); significant impact (56–59 points); and severe impact (≥ 60 points).The Turkish version of the scale was previously validated with a Cronbach's alpha of 0.87.[21]
The primary and secondary endpoints were analyzed from the medical records and headache diaries with the data previously described.
Statistical analysis
The statistical analyses were performed using the IBM SPSS Statistics for Windows (IBM Corp., Armonk, NY, United States), software, version 25.0. The percentages show the numerical values of the categorical variable, and the mean and standard deviation (SD) values for the continuous variables provide the statistical representation. For data with normal distribution, we used the Student's t-test to compare two groups, and analysis of variance (ANOVA) to compare three or more groups. For data that was not normally-distributed, the Mann-Whitney U-test was used. For the analysis of the categorical variables, the Chi-squared (χ2) test or the Fisher's exact test were used. Correlations involving variables influencing the NRS-11 score at 12 months were analyzed using the Pearson correlation coefficient. Statistical significance was defined as p < 0.05.
RESULTS
We analyzed 18 patients, 13 (72.2%) of whom were female subjects. [Table 1] provides an overview of the patient characteristics.
[Table 1] also provides the details of the ON findings. Overall, ON had a mean duration of 8.28 ± 3.707 years. Pain was consistently paroxysmal in all patients, with a mean duration of 68.89 ± 62.18 minutes per attack. The mean number of attacks was of 11.94 ± 7.033 per day, and the mean for the attack days per month was of 12.11 ± 4.497. The mean initial NRS-11 score ws of 8.78 ± 0.732. The diagnostic block yielded the following efficacy percentages: 100% efficacy −2 patients (11.1%); 85 to 99% efficacy – 8 patients (44.4%); 76 to 84% efficacy – 3 patients (16.7%); and 55 to 75% efficacy – 5 patients (27.8%). The prophylactic agents administered were as follows: carbamazepine 800 mg/day (18 patients; 100%), pregabalin 300 mg/day (16 subjects; 88.9%), and duloxetine 60 mg/day (12 patients; 66.7%).
The number of attacks, the use of NSAIDs for acute treatment per month, and the change within the scores on the NRS-11 and HIT-6 as a function of time are illustrated in [Table 2]. The scores assessed during the appointments were lower than those at baseline. The relationship between time and the NRS-11 score was statistically significant (p = 0.001). The HIT-6 score (p = 0.001), the number of attacks (p = 0.001), and the monthly intake of NSAIDs (p = 0.001) also decreased after treatment at all appointments compared to baseline. At 12 months, 7 patients (38.9%) were taking no prophylaxis, 6 patients (33.3%), carbamazepine 400 mg/day, 4 patients (22.2%), duloxetine 30 mg/day, and 1 patient (5.6%), pregabalin 150 mg/day.
Abbreviations: HIT-6, 6-Item Headache Impact Test; NRS-11, 11-Point Numeric Rating Scale; NSAIDs, nonsteroidal antiinflammatory drugs.
Notes: Anova test was used. Data are expressed as mean ± standard deviation (minimum–maximum) values; * statistically significant.
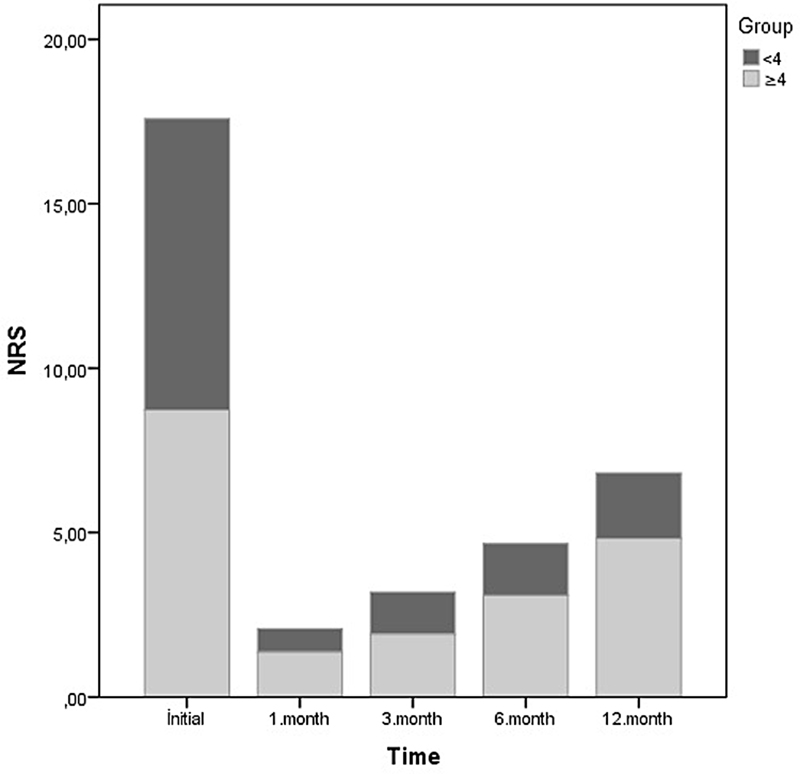
As previously mentioned, treatment efficacy was defined as NRS-11 score < 4 at 12 months. [Table 3] shows treatment efficacy by month. The number of patients with NRS-11 score < 4 was of 18 (100%) at the first and third months, 14 (77.8%) at the sixth month, and 7 (38.9%) at 12 months. [Figure 3] shows the mean NRS-11 scores for the group with NRS-11 score < 4 and the group with NRS-11 score ≥ 4 at 12 months. Pain reduction of at least 50% from baseline to the first, third, and sixth months was of 100%, and of 66% at month 12.
Abbreviations: BMI, body mass index; NRS-11, 11-Point Numeric Rating Scale.
Note: The Pearson's correlation coefficient was used in this analysis.
[Table 3] shows the correlated factors influencing the NRS-11 score at month 12. With an increasing frequency of attacks per month, the correlation with the NRS-11 score also increased (r = 0.598; p = 0.009). The NRS-11 score decreased inversely as the percentage of effectiveness of the diagnostic block increased (r = -0.789; p = 0.001). For the categorical variables, electroshock pain was associated with an NRS-11 score ≥ 4 at 12 months (p = 0.041). Lancinating pain was associated with an NRS-11 score < 4 at 12 months (p = 0.031) ([Table 4]).
Abbreviation: NRS-11, 11-Point Numeric Rating Scale.
Notes: The Chi-squared test or the Fisher's exact test was used in this analysis; * statistically significant.
In total, 2 patients experienced complications or side effects. One of them reported that hypoesthesia persisted for 2 months, which was located in the posterior region of the scalp, where the treated GON was distributed. The hypoesthesia disappeared on its own in the third month. One patient reported dizziness and ataxia in the first week after CRFA. At that time, the neuroimaging and neurologic examinations were normal. The symptoms disappeared coincidentally in the second week. The rest of the patients did not experience any side effects after the procedure.
DISCUSSION
As the authors hypothesized that US-guided CRFA of the PGON might be effective in the long term with fewer side effects, the findings of the current study support the hypothesis. The study highlights the benefits of CRFA targeting the PGON in ON patients, demonstrating both long-term efficacy and minimal, temporary side effects.
Pain reduction showed promising results: 100% of patients scored < 4 on the NRS-11 in the first and third months, 77.8%, by the sixth month, and 38.9%, by the twelfth month. Furthermore, at the 6-month mark, the percentage of patients who achieved a 50% or greater reduction in NRS-11 scores was of 100% (18), and by the twelfth month, it was of 66.7%. A successful treatment response correlated with effective diagnostic block and lower frequency of attacks. Differences emerged between patients with NRS-11 scores < 4 and those with scores ≥ 4, with electroshock-like pain more common in those with higher scores and lancinating pain more frequent in those with lower scores. Only 2 patients experienced temporary complications, both of whom recovered quickly.
The pain in ON likely originates from the upper cervical nerves due to convergence between upper cervical segment afferents and the trigeminal complex.[22] Consequently, GON block and RF are the cornerstone of ON treatment.[23] [24] [25]
Studies[5] [6] [7] [8] [9] [10] on PRF of the DGON with anatomical landmark-guidance have shown significant improvement in pain and quality of life. Choi et al.[7] found PRF more effective than steroid injections for pain reduction in a 6-month double-blinded study. In ON patients, PRF treatments have also been shown to improve sleep, mood, and daily functioning.[14]
Only 3 previous studies[12] [13] [14] have evaluated CRFA's effectiveness in ON. Hoffman et al.[12] reported a 76.3% success rate with DGON RFA using anatomical landmarks over six months. Finiels and Batifol[13] showed a success rate of 89.4% when treating ON with bilateral DGON and C2 DRG CRF under fluoroscopy.[13] In a retrospective observational study of fluoroscopy-guided C2 DRG CRF, Hamer and Purath[14] reported that 35% of the patients experienced complete pain relief, while 70% expreinced at least 80% of pain relief over an average of 22.35 weeks.
In the current study, CRFA targeted the PGON, which is located between the obliquus capitis inferior and semispinalis capitis muscles at C2, a site considered safer and more accessible than that of the DGON. This position enables US guidance, reducing the risks associated with fluoroscopy.[15] [16] [17] [18] Up to 90% of the cases[22] show compression of the GON by surrounding structures, such as the inferior oblique capitis and semispinal capitis muscles or the occipital artery. Successful treatments with US-guided PGON blocks have been documented, although fewer studies have addressed PGON PRF in ON.[15] [16] [23] [24] [25] [26] Guner and Eyigor[19] reported improvements in depression, migraine symptoms, and sleep disturbances in chronic migraine patients treated with US-guided PGON PRF.
Compared to the PRF and CRFA outcomes in the literature, in the present study, we observed greater effectiveness and longer-lasting pain relief. Here, success was defined as an NRS-11 score < 4, with baseline scores ranging from 8 to 10. By month 12, the scores ranged from 1 to 6. While a 50% of pain reduction compared to baseline was achieved in 100% (18 patients) of the cases in months 1 through 6, this rate was of 66% at 12 months, showing substantial long-term efficacy. However, we could not definitively determine whether PRF or CRF of the PGON is more beneficial under US guidance. Further research is needed to compare the effectiveness of US-guided PRF and CRFA of the PGON.
In the current study, we also observed fewer and less severe complications compared to previous studies, likely due to factors such as US guidance, dexamethasone administration, and precise targeting of the PGON.[11] While complications like hemiplegia and severe neuropathic pain have been reported[13] with C2 DRG CRFA at 70°C, the present study used a CRFA temperature of 60°C to avoid nerve damage while effectively managing pain. In previous studies[25] on trigeminal neuralgia, it was known that temperatures > 65°C destroy the nerve fibers, which, in turn, can lead to severe complications, such as blindness, deafness, ptosis, and permanent facial nerve palsy. As the current was the first study on US-guided PGON CRFA, the temperature was chosen carefully to ensure pain relief and reduce complications. Future research could explore temperature variations to further optimize CRFA outcomes and minimize complications in ON treatments.
STRENGTHS AND LIMITATIONS
The present study has several notable strengths. It is the first study on the efficacy of US-guided PGON CRFA. The 1-year follow-up and the use of validated instruments such as the HIT-6 enabled an effective evaluation of the long-term outcomes. However, there are also limitations, and the most important limitation one is the retrospective design, with a small sample size and no control group. Additionally, there is the inability to assess sample size or do post-hoc power analysis. In addition, ON can affect various aspects of a patient's quality of life, such as mood, mobility, and sleep, but no data on quality of life or disability were collected in the current study. Psychological factors that may influence the effectiveness of treatments for chronic pain were only assessed using medical records, without detailed examinations. Larger, prospective, controlled studies are needed to better understand the factors that predict the success of CRFA treatment in ON.
In conclusion, the present study showed that US-guided CRFA of the PGON significantly reduces pain in patients with refractory ON up to 1 year after the procedure. The initial attack frequency, electric shock-like pain, and reduced response to diagnostic block were associated with reduced response. These results suggest that CRFA of the PGON is promising. However, before it becomes widely accepted, further scientific studies and randomized controlled trials are needed.
Conflict of Interest
The authors have no conflict of interest to declare.
Authors' Contributions
SAT: conceptualization, formal analysis, investigation, methodology, validation, writing – original draft, and writing – review & editing; EC: data curation, project administration, resources, software, and writing – review & editing; and SA: formal analysis, methodology, supervision, validation, and writing – review & editing.
Data Availability Statement
Data and materials are available from the corresponding author upon reasonable request and are subject to ethical review.
Editor-in-Chief: Hélio A. G. Teive.
Associate Editor: Mário Fernando Prieto Peres.
-
References
- 1 Headache Classification Committee of the International Headache Society. International Classification of Headache Disorders. 3rd ed. (beta version). Cephalalgia 2013; 33: 629-808
- 2 Choi I, Jeon SR. Neuralgias of the Head: Occipital Neuralgia. J Korean Med Sci 2016; 31 (04) 479-488
- 3 Swanson D, Guedry R, Boudreaux M. et al. An Update on the Diagnosis, Treatment, and Management of Occipital Neuralgia. J Craniofac Surg 2022; 33 (03) 779-783
- 4 Urits I, Schwartz RH, Patel P. et al. A Review of the Recent Findings in Minimally Invasive Treatment Options for the Management of Occipital Neuralgia. Neurol Ther 2020; 9 (02) 229-241
- 5 Manolitsis N, Elahi F. Pulsed radiofrequency for occipital neuralgia. Pain Physician 2014; 17 (06) E709-E717
- 6 Vanelderen P, Rouwette T, De Vooght P. et al. Pulsed radiofrequency for the treatment of occipital neuralgia: a prospective study with 6 months of follow-up. Reg Anesth Pain Med 2010; 35 (02) 148-151
- 7 Choi HJ, Oh IH, Choi SK, Lim YJ. Clinical outcomes of pulsed radiofrequency neuromodulation for the treatment of occipital neuralgia. J Korean Neurosurg Soc 2012; 51 (05) 281-285
- 8 Huang JH, Galvagno Jr SM, Hameed M. et al. Occipital nerve pulsed radiofrequency treatment: a multi-center study evaluating predictors of outcome. Pain Med 2012; 13 (04) 489-497
- 9 Navani A, Mahajan G, Kreis P, Fishman SM. A case of pulsed radiofrequency lesioning for occipital neuralgia. Pain Med 2006; 7 (05) 453-456
- 10 Cohen SP, Peterlin BL, Fulton L. et al. Randomized, double-blind, comparative-effectiveness study comparing pulsed radiofrequency to steroid injections for occipital neuralgia or migraine with occipital nerve tenderness. Pain 2015; 156 (12) 2585-2594
- 11 Orhurhu V, Sidharthan S, Roberts J. et al. Radiofrequency Ablation for Craniofacial Pain Syndromes. Phys Med Rehabil Clin N Am 2021; 32 (04) 601-645
- 12 Hoffman LM, Abd-Elsayed A, Burroughs TJ, Sachdeva H. Treatment of Occipital Neuralgia by Thermal Radiofrequency Ablation. Ochsner J 2018; 18 (03) 209-214
- 13 Finiels PJ, Batifol D. The treatment of occipital neuralgia: Review of 111 cases. Neurochirurgie 2016; 62 (05) 233-240
- 14 Hamer JF, Purath TA. Response of cervicogenic headaches and occipital neuralgia to radiofrequency ablation of the C2 dorsal root ganglion and/or third occipital nerve. Headache 2014; 54 (03) 500-510
- 15 Narouze S. Occipital Neuralgia Diagnosis and Treatment: The Role of Ultrasound. Headache 2016; 56 (04) 801-807
- 16 Kaga M. First Case of Occipital Neuralgia Treated by Fascial Hydrodissection. Am J Case Rep 2022; 23: e936475
- 17 Skinner C, Kumar S. Ultrasound-Guided Occipital Nerve Block for Treatment of Atypical Occipital Neuralgia. Cureus 2021; 13 (10) e18584
- 18 Kissoon NR, O'Brien TG, Bendel MA. et al. Comparative Effectiveness of Landmark-guided Greater Occipital Nerve (GON) Block at the Superior Nuchal Line Versus Ultrasound-guided GON Block at the Level of C2: A Randomized Clinical Trial (RCT). Clin J Pain 2022; 38 (04) 271-278
- 19 Guner D, Eyigor C. Efficacy of ultrasound-guided greater occipital nerve pulsed radiofrequency therapy in chronic refractory migraine. Acta Neurol Belg 2023; 123 (01) 191-198
- 20 Krebs EE, Carey TS, Weinberger M. Accuracy of the pain numeric rating scale as a screening test in primary care. J Gen Intern Med 2007; 22 (10) 1453-1458
- 21 Dikmen PY, Bozdağ M, Güneş M. et al. Reliability and Validity of Turkish Version of Headache Impact Test (HIT-6) in Patients with Migraine. Noro Psikiyatri Arsivi 2020; 58 (04) 300-307
- 22 Saglam L, Gayretli O, Coskun O, Kale A. Morphological features of the greater occipital nerve and its possible importance for interventional procedures. J Anat 2024; 244 (02) 312-324
- 23 Jain E, Tram JK, Owens MA. et al. Radiofrequency ablation for headache pain: an updated systematic review. Ann Palliat Med 2024; 13 (04) 948-962
- 24 Orhurhu V, Huang L, Quispe RC. et al. Use of Radiofrequency Ablation for the Management of Headache: A Systematic Review. Pain Physician 2021; 24 (07) E973-E987
- 25 Oliveira K, Dhondt N, Englesakis M, Goel A, Hoydonckx Y. Pulsed Radiofrequency Neuromodulation of the Greater Occipital Nerve for the Treatment of Headache Disorders in Adults: A Systematic Review. Can J Pain 2024; 8 (01) 2355571
- 26 Wu H, Zhou J, Chen J, Gu Y, Shi L, Ni H. Therapeutic efficacy and safety of radiofrequency ablation for the treatment of trigeminal neuralgia: a systematic review and meta-analysis. J Pain Res 2019; 12: 423-441
Address for correspondence
Publication History
Received: 31 October 2024
Accepted: 25 January 2025
Article published online:
02 April 2025
© 2025. The Author(s). This is an open access article published by Thieme under the terms of the Creative Commons Attribution 4.0 International License, permitting copying and reproduction so long as the original work is given appropriate credit (https://creativecommons.org/licenses/by/4.0/)
Thieme Revinter Publicações Ltda.
Rua Rego Freitas, 175, loja 1, República, São Paulo, SP, CEP 01220-010, Brazil
Suna Aşkın Turan, Şenay Aydın, Ezgi Can. Ultrasound-guided continuous radiofrequency ablation of the proximal greater occipital nerve is effective in refractory occipital neuralgia: a retrospective cohort study. Arq Neuropsiquiatr 2025; 83: s00451806813.
DOI: 10.1055/s-0045-1806813
-
References
- 1 Headache Classification Committee of the International Headache Society. International Classification of Headache Disorders. 3rd ed. (beta version). Cephalalgia 2013; 33: 629-808
- 2 Choi I, Jeon SR. Neuralgias of the Head: Occipital Neuralgia. J Korean Med Sci 2016; 31 (04) 479-488
- 3 Swanson D, Guedry R, Boudreaux M. et al. An Update on the Diagnosis, Treatment, and Management of Occipital Neuralgia. J Craniofac Surg 2022; 33 (03) 779-783
- 4 Urits I, Schwartz RH, Patel P. et al. A Review of the Recent Findings in Minimally Invasive Treatment Options for the Management of Occipital Neuralgia. Neurol Ther 2020; 9 (02) 229-241
- 5 Manolitsis N, Elahi F. Pulsed radiofrequency for occipital neuralgia. Pain Physician 2014; 17 (06) E709-E717
- 6 Vanelderen P, Rouwette T, De Vooght P. et al. Pulsed radiofrequency for the treatment of occipital neuralgia: a prospective study with 6 months of follow-up. Reg Anesth Pain Med 2010; 35 (02) 148-151
- 7 Choi HJ, Oh IH, Choi SK, Lim YJ. Clinical outcomes of pulsed radiofrequency neuromodulation for the treatment of occipital neuralgia. J Korean Neurosurg Soc 2012; 51 (05) 281-285
- 8 Huang JH, Galvagno Jr SM, Hameed M. et al. Occipital nerve pulsed radiofrequency treatment: a multi-center study evaluating predictors of outcome. Pain Med 2012; 13 (04) 489-497
- 9 Navani A, Mahajan G, Kreis P, Fishman SM. A case of pulsed radiofrequency lesioning for occipital neuralgia. Pain Med 2006; 7 (05) 453-456
- 10 Cohen SP, Peterlin BL, Fulton L. et al. Randomized, double-blind, comparative-effectiveness study comparing pulsed radiofrequency to steroid injections for occipital neuralgia or migraine with occipital nerve tenderness. Pain 2015; 156 (12) 2585-2594
- 11 Orhurhu V, Sidharthan S, Roberts J. et al. Radiofrequency Ablation for Craniofacial Pain Syndromes. Phys Med Rehabil Clin N Am 2021; 32 (04) 601-645
- 12 Hoffman LM, Abd-Elsayed A, Burroughs TJ, Sachdeva H. Treatment of Occipital Neuralgia by Thermal Radiofrequency Ablation. Ochsner J 2018; 18 (03) 209-214
- 13 Finiels PJ, Batifol D. The treatment of occipital neuralgia: Review of 111 cases. Neurochirurgie 2016; 62 (05) 233-240
- 14 Hamer JF, Purath TA. Response of cervicogenic headaches and occipital neuralgia to radiofrequency ablation of the C2 dorsal root ganglion and/or third occipital nerve. Headache 2014; 54 (03) 500-510
- 15 Narouze S. Occipital Neuralgia Diagnosis and Treatment: The Role of Ultrasound. Headache 2016; 56 (04) 801-807
- 16 Kaga M. First Case of Occipital Neuralgia Treated by Fascial Hydrodissection. Am J Case Rep 2022; 23: e936475
- 17 Skinner C, Kumar S. Ultrasound-Guided Occipital Nerve Block for Treatment of Atypical Occipital Neuralgia. Cureus 2021; 13 (10) e18584
- 18 Kissoon NR, O'Brien TG, Bendel MA. et al. Comparative Effectiveness of Landmark-guided Greater Occipital Nerve (GON) Block at the Superior Nuchal Line Versus Ultrasound-guided GON Block at the Level of C2: A Randomized Clinical Trial (RCT). Clin J Pain 2022; 38 (04) 271-278
- 19 Guner D, Eyigor C. Efficacy of ultrasound-guided greater occipital nerve pulsed radiofrequency therapy in chronic refractory migraine. Acta Neurol Belg 2023; 123 (01) 191-198
- 20 Krebs EE, Carey TS, Weinberger M. Accuracy of the pain numeric rating scale as a screening test in primary care. J Gen Intern Med 2007; 22 (10) 1453-1458
- 21 Dikmen PY, Bozdağ M, Güneş M. et al. Reliability and Validity of Turkish Version of Headache Impact Test (HIT-6) in Patients with Migraine. Noro Psikiyatri Arsivi 2020; 58 (04) 300-307
- 22 Saglam L, Gayretli O, Coskun O, Kale A. Morphological features of the greater occipital nerve and its possible importance for interventional procedures. J Anat 2024; 244 (02) 312-324
- 23 Jain E, Tram JK, Owens MA. et al. Radiofrequency ablation for headache pain: an updated systematic review. Ann Palliat Med 2024; 13 (04) 948-962
- 24 Orhurhu V, Huang L, Quispe RC. et al. Use of Radiofrequency Ablation for the Management of Headache: A Systematic Review. Pain Physician 2021; 24 (07) E973-E987
- 25 Oliveira K, Dhondt N, Englesakis M, Goel A, Hoydonckx Y. Pulsed Radiofrequency Neuromodulation of the Greater Occipital Nerve for the Treatment of Headache Disorders in Adults: A Systematic Review. Can J Pain 2024; 8 (01) 2355571
- 26 Wu H, Zhou J, Chen J, Gu Y, Shi L, Ni H. Therapeutic efficacy and safety of radiofrequency ablation for the treatment of trigeminal neuralgia: a systematic review and meta-analysis. J Pain Res 2019; 12: 423-441